
Bacterial Infection and Implant Loosening in Hip and Knee Arthroplasty: Evaluation of 209 Cases

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
3. Results
3.1. Clinical Data
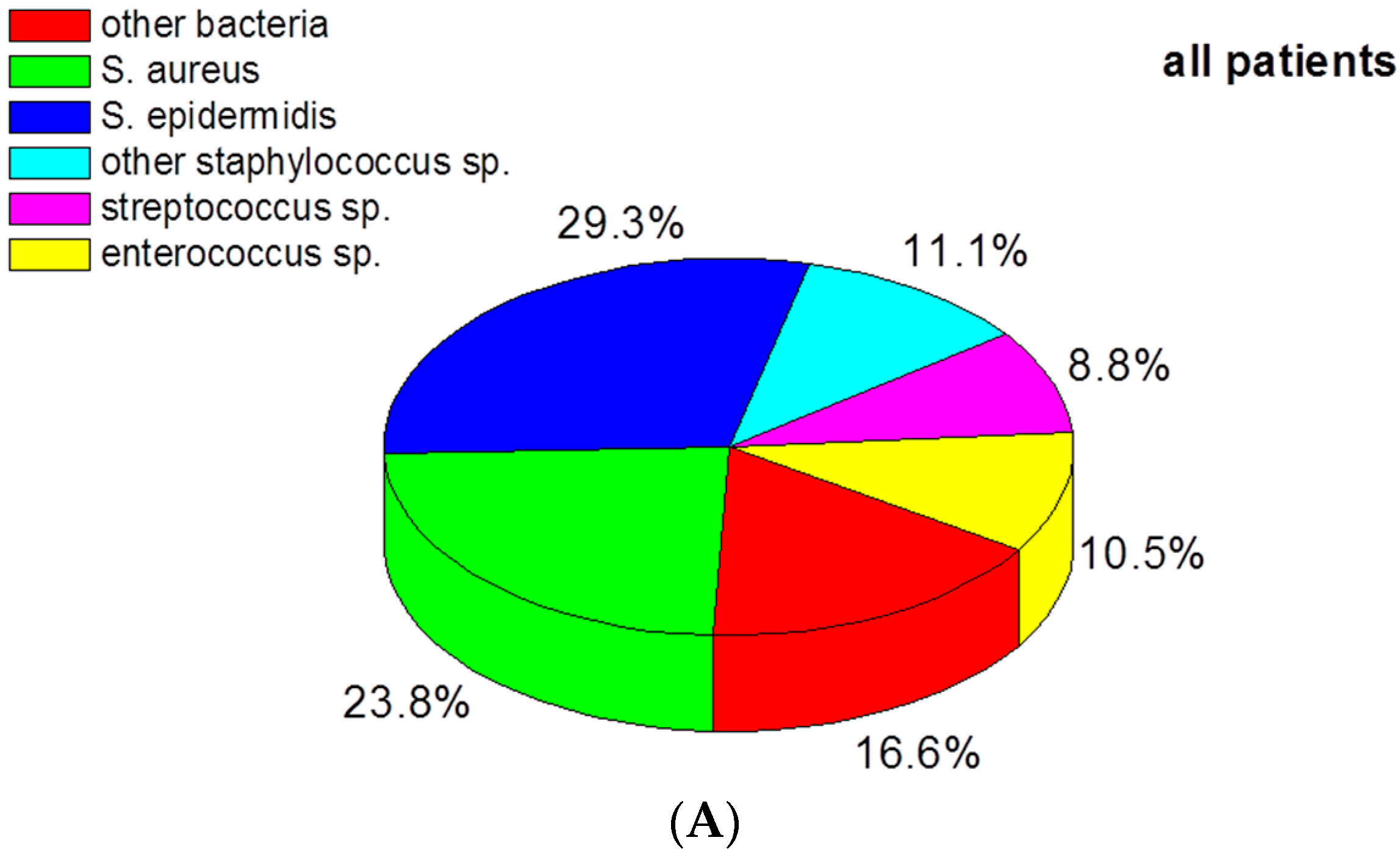
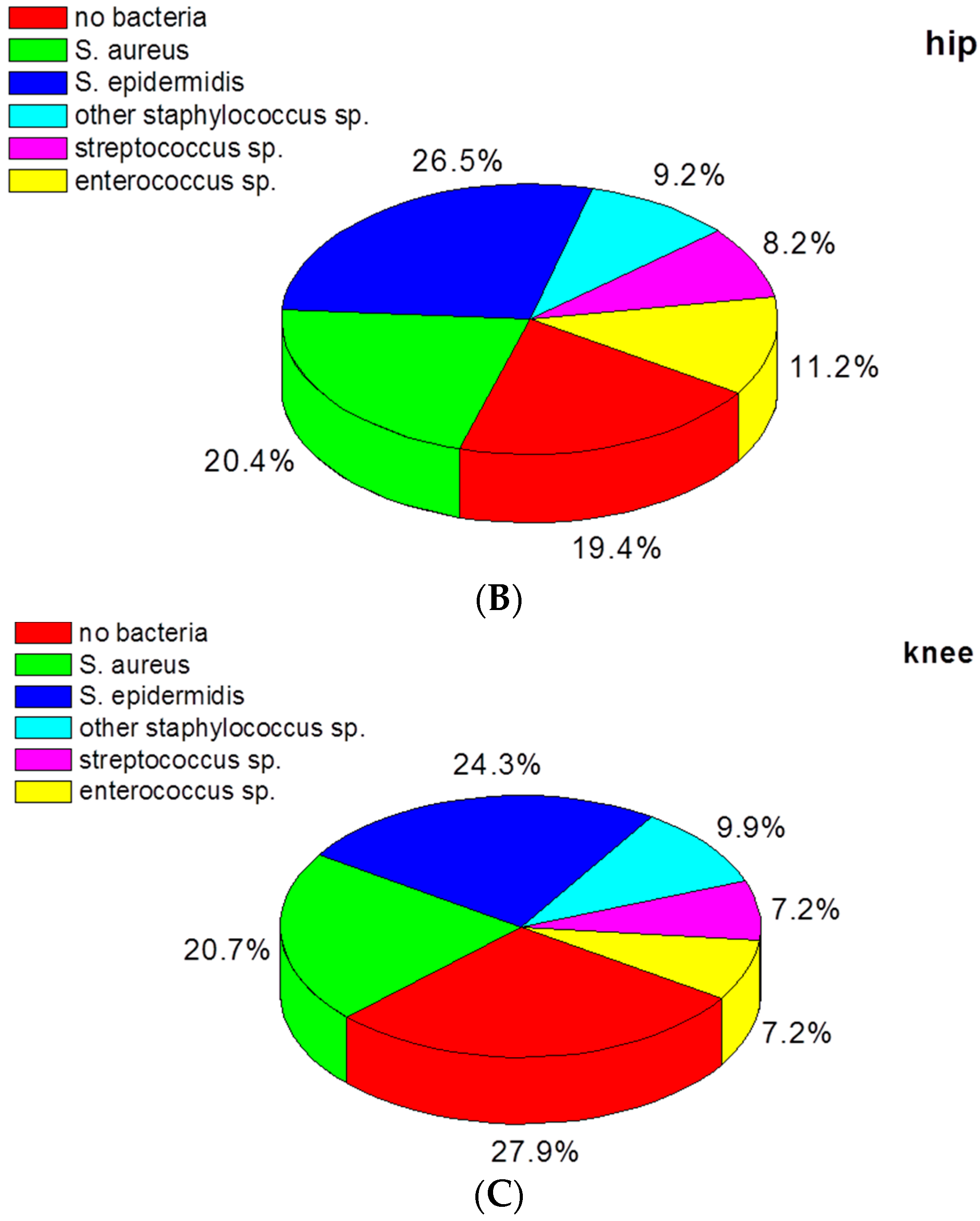
3.2. Bacteria Species in Infected Hip and Knee Prostheses
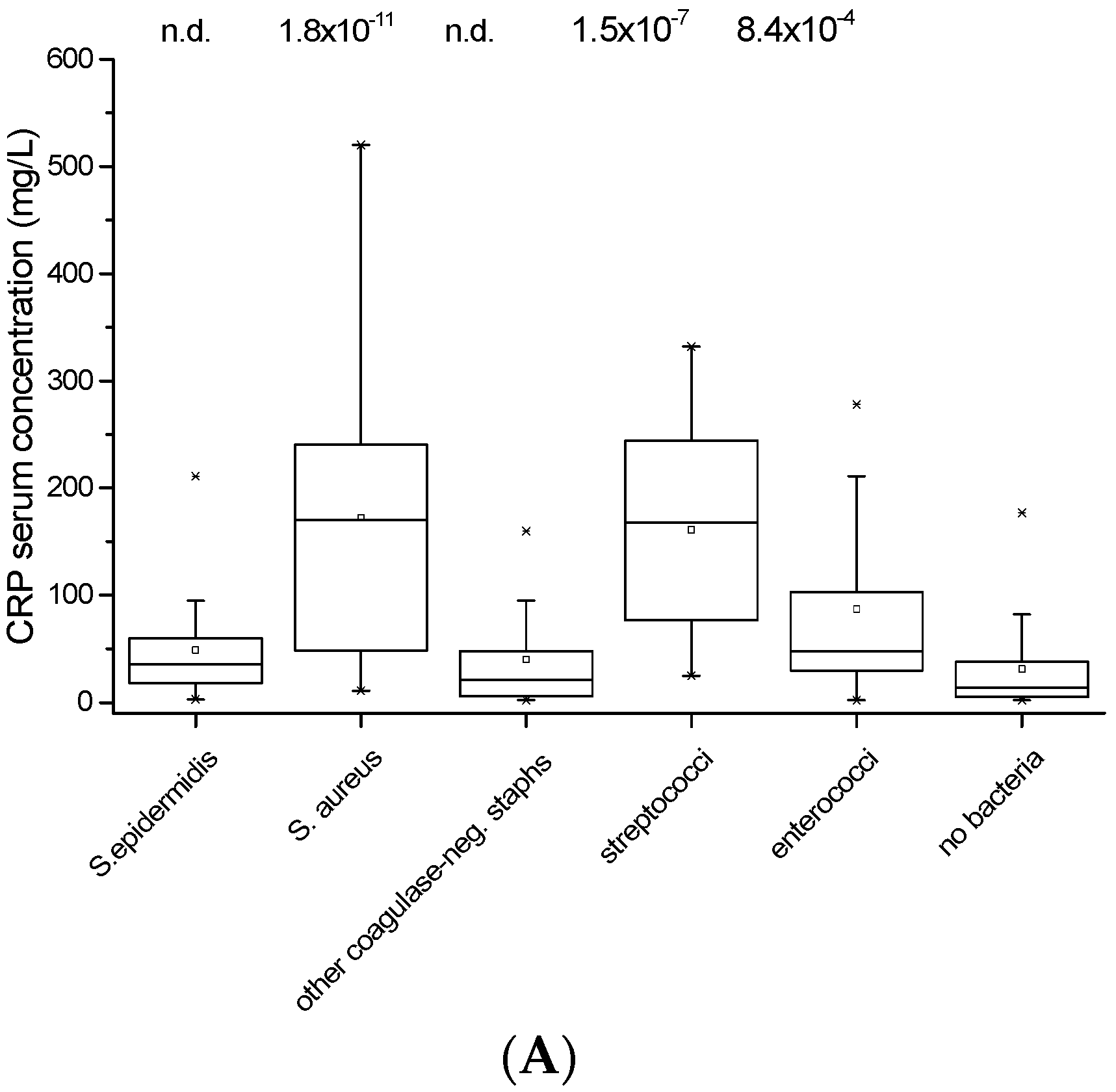
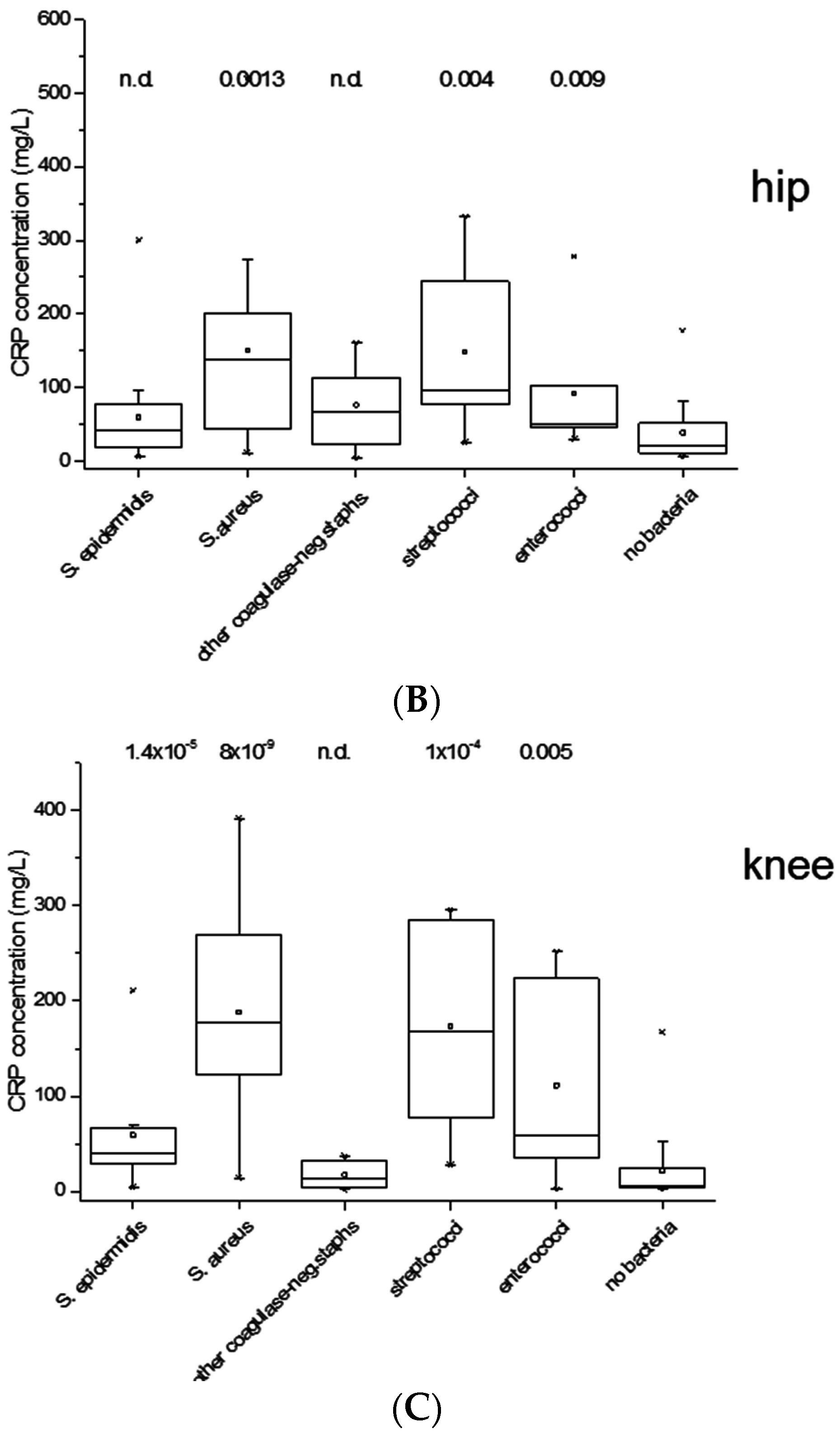
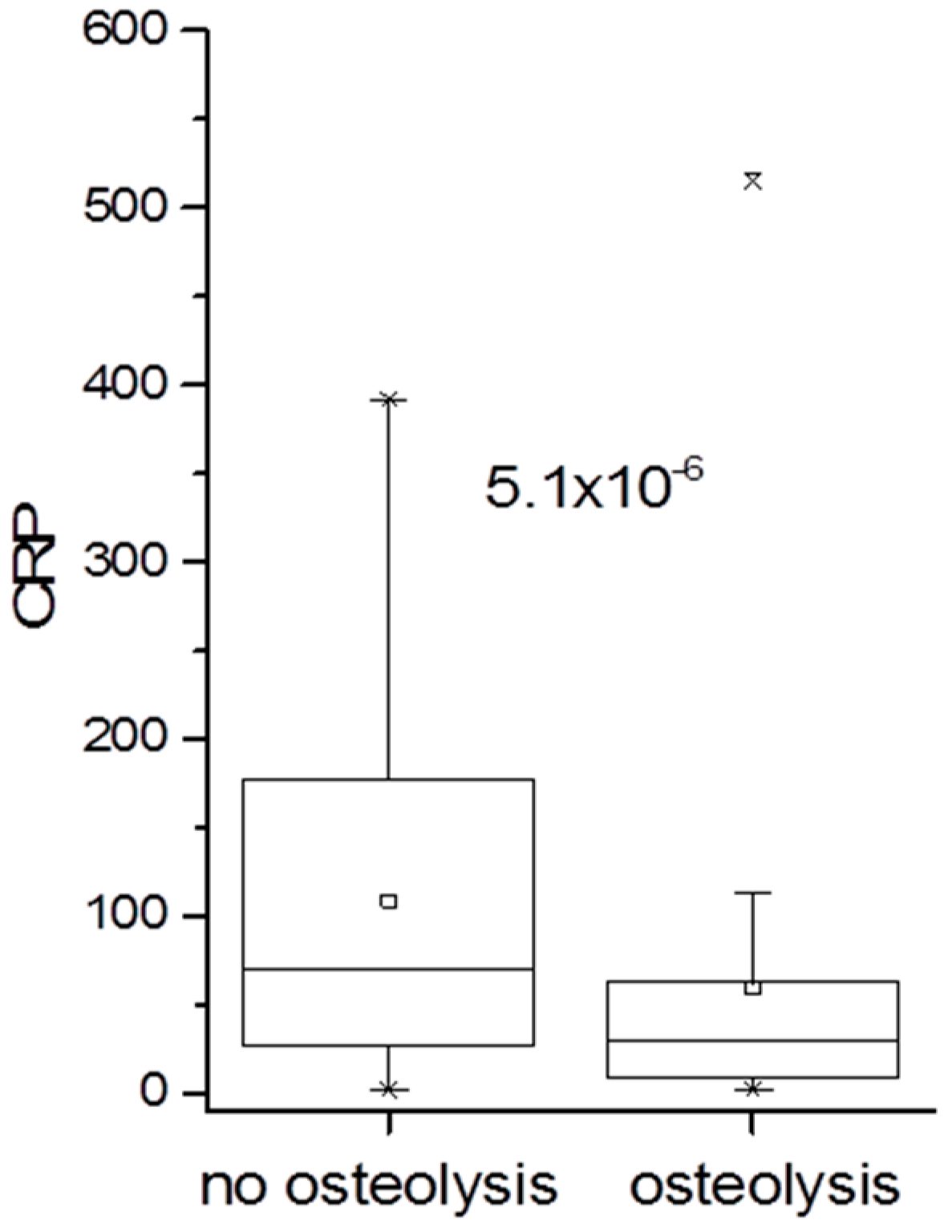
3.3. Association of CRP Concentration with Infection
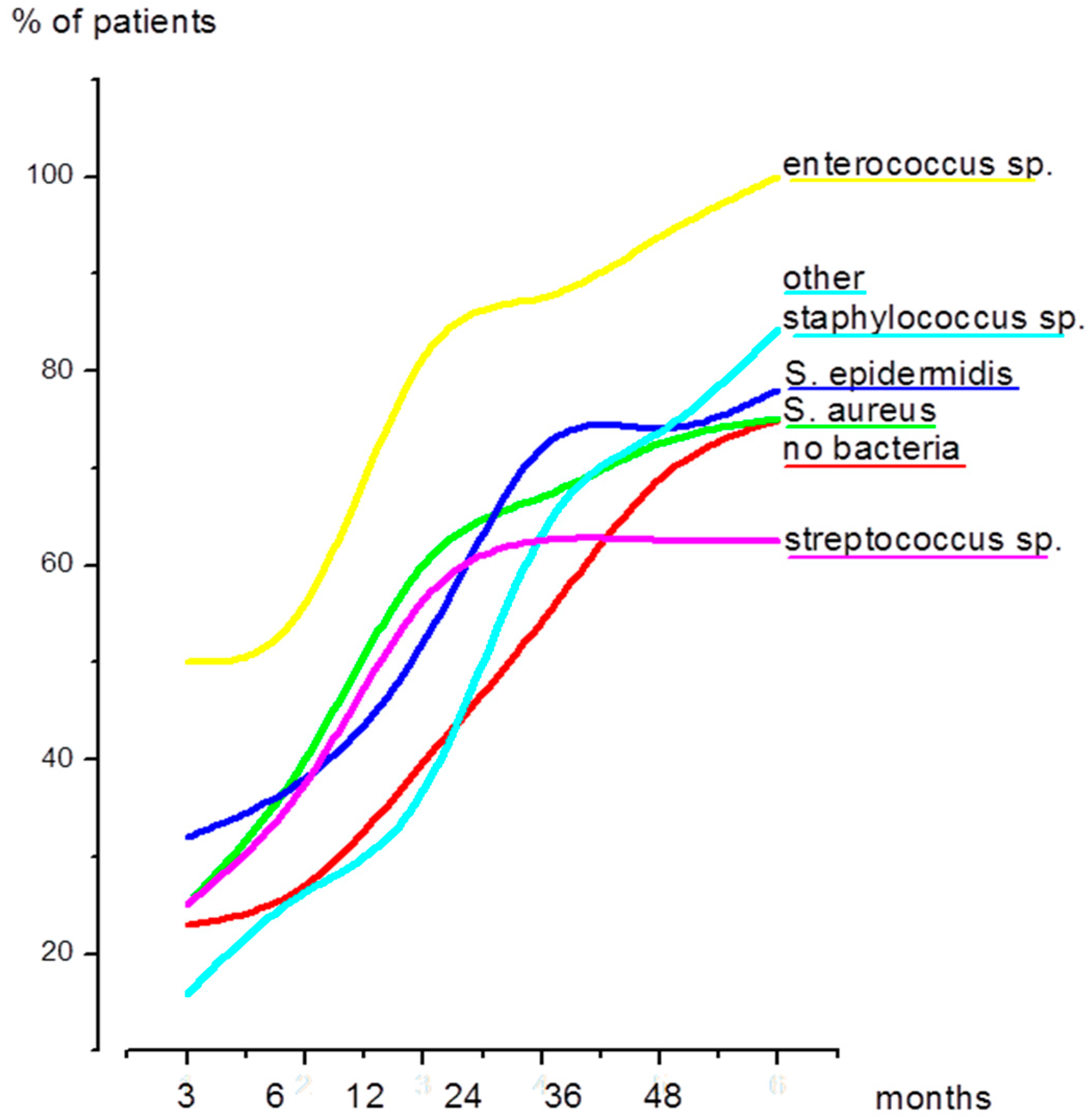
3.4. Time Elapsed Since the Primary Prosthetic Joint Replacement and Since the Last Surgical Intervention
3.5. Implant Loosening in Hip and Knee Prostheses
4. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Haenle, M.; Skripitz, C.; Mittelmeier, W.; Skripitz, R. Economic impact of infected total knee arthroplasty. Sci. World J. 2012, 2012, 196515–196521. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial biofilms: A common cause of persistent infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Laffer, R.R.; Graber, P.; Ochsner, P.E.; Zimmerli, W. Outcome of prosthetic knee-associated infection: Evaluation of 40 consecutive episodes at a single centre. Clin. Microbiol. Infect. 2006, 12, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Nickinson, R.S.; Board, T.N.; Gambhir, A.K.; Porter, M.L.; Kay, P.R. The microbiology of the infected knee arthroplasty. Int. Orthop. 2010, 34, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed]
- Stefansdottir, A.; Johansson, D.; Knutson, K.; Lidgren, L.; Robertsson, O. Microbiology of the infected knee arthroplasty: Report from the Swedish Knee Arthroplasty Register on 426 surgically revised cases. Scand. J. Infect. Dis. 2009, 41, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Woodford, N.; Livermore, D.M. Infections caused by Gram-positive bacteria: A review of the global challenge. J. Infect. 2009, 59 (Suppl. 1), S4–S16. [Google Scholar] [CrossRef]
- Guenther, F.; Stroh, P.; Wagner, C.; Obst, U.; Hansch, G.M. Phagocytosis of staphylococci biofilms by polymorphonuclear neutrophils: S. aureus and S. epidermidis differ with regard to their susceptibility towards the host defense. Int. J. Artif. Organs 2009, 32, 565–573. [Google Scholar] [PubMed]
- Meyle, E.; Stroh, P.; Gunther, F.; Hoppy-Tichy, T.; Wagner, C.; Hansch, G.M. Destruction of bacterial biofilms by polymorphonuclear neutrophils: Relative contribution of phagocytosis, DNA release, and degranulation. Int. J. Artif. Organs 2010, 33, 608–620. [Google Scholar] [PubMed]
- Dapunt, U.; Giese, T.; Lasitschka, F.; Lehner, B.; Ewerbeck, V.; Hansch, G.M. Osteoclast generation and cytokine profile at prosthetic interfaces: A study on tissue of patients with aseptic loosening or implant-associated infections. Eur. J. Inflamm. 2014, 12, 147–159. [Google Scholar]
- Dapunt, U.; Maurer, S.; Giese, T.; Gaida, M.M.; Hansch, G.M. The macrophage inflammatory proteins MIP1 alpha (CCL3) and MIP2 alpha (CXCL2) in implant-associated osteomyelitis: Linking inflammation to bone degradation. Mediat. Inflamm. 2014, 2014, 728619–718629. [Google Scholar] [CrossRef] [PubMed]
- Dapunt, U.; Giese, T.; Maurer, S.; Stegmaier, S.; Prior, B.; Hansch, G.M.; Gaida, M.M. Neutrophil-derived MRP-14 is up-regulated in infectious osteomyelitis and stimulates osteoclast generation. J. Leukoc. Biol. 2015, 98, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Zimmerli, W. Clinical presentation and treatment of orthopaedic implant-associated infection. J. Intern. Med. 2014, 276, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-joint infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Morawietz, L.; Classen, R.A.; Schroder, J.H.; Dynybil, C.; Perka, C.; Skwara, A.; Neidel, J.; Gehrke, T.; Frommelt, L.; Hansen, T.; et al. Proposal for a histopathological consensus classification of the periprosthetic interface membrane. J. Clin. Pathol. 2006, 59, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Dale, H.; Fenstad, A.M.; Hallan, G.; Havelin, L.I.; Furnes, O.; Overgaard, S.; Pedersen, A.B.; Kärrholm, J.; Garellick, G.; Pulkkinen, P.; et al. Increasing risk of prosthetic joint infection after total hip arthroplasty. Acta Orthop. 2012, 83, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, J.V.; Gordon, M.; Wretenberg, P.; Karrholm, J.; Garellick, G. Validation of reoperations due to infection in the Swedish Hip Arthroplasty Register. BMC Musculoskelet. Disord. 2014, 15, 384. [Google Scholar] [CrossRef] [PubMed]
- Sektorenübergreifende Qualität im Gesundheitswesen. Available online: https://www.sqg.de/ergebnisse/leistungsbereiche/index.html (accessed on 5 July 2014).
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorli, L.; Fresco, G.; Fernández-Sampedro, M.; Dolores Del Toro, M.; Guío, L.; et al. Time trends in the aetiology of prosthetic joint infections: A multicentre cohort study. Clin. Microbiol. Infect. 2016, 22, 732.e1–732.e8. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Leone, S. Prosthetic joint infections: Microbiology, diagnosis, management and prevention. Int. J. Antimicrob. Agents 2008, 32, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Zimmerli, W. Diagnosis and treatment of infections associated with fracture-fixation devices. Injury 2006, 37 (Suppl. 2), S59–S66. [Google Scholar] [CrossRef] [PubMed]
- Von Eiff, C.; Peters, G.; Heilmann, C. Pathogenesis of infections due to coagulase-negative staphylococci. Lancet Infect. Dis. 2002, 2, 677–685. [Google Scholar] [CrossRef]
- Arciola, C.R.; Visai, L.; Testoni, F.; Arciola, S.; Campoccia, D.; Speziale, P.; Montanaro, L. Concise survey of Staphylococcus aureus virulence factors that promote adhesion and damage to peri-implant tissues. Int. J. Artif. Organs 2011, 34, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Campoccia, D.; Montanaro, L.; Arciola, C.R. The significance of infection related to orthopedic devices and issues of antibiotic resistance. Biomaterials 2006, 27, 2331–2339. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Murillo, O.; Iribarren, J.A.; Soriano, A.; Sanchez-Somolinos, M.; Baraia-Etxaburu, J.M.; Rico, A.; Palomino, J.; Rodríguez-Pardo, D.; Horcajada, J.P.; et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin. Infect. Dis. 2013, 56, 182–194. [Google Scholar] [CrossRef] [PubMed]
- El Helou, O.C.; Berbari, E.F.; Marculescu, C.E.; El Atrouni, W.I.; Razonable, R.R.; Steckelberg, J.M.; Hanssen, A.D.; Osmon, D.R. Outcome of enterococcal prosthetic joint infection: Is combination systemic therapy superior to monotherapy? Clin. Infect. Dis. 2008, 47, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Everts, R.J.; Chambers, S.T.; Murdoch, D.R.; Rothwell, A.G.; McKie, J. Successful antimicrobial therapy and implant retention for streptococcal infection of prosthetic joints. ANZ J. Surg. 2004, 74, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Berbari, E.F.; Marculescu, C.; Sia, I.; Lahr, B.D.; Hanssen, A.D.; Steckelberg, J.M.; Gullerud, R.; Osmon, D.R. Culture-negative prosthetic joint infection. Clin. Infect. Dis. 2007, 45, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Neut, D.; van Horn, J.R.; van Kooten, T.G.; van der Mei, H.C.; Busscher, H.J. Detection of biomaterial-associated infections in orthopaedic joint implants. Clin. Orthop. Relat. Res. 2003, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Dapunt, U.; Lehner, B.; Burckhardt, I.; Zimmermann, S.; Hansch, G.M.; Ewerbeck, V. Evaluation of implant sonication as a diagnostic tool in implant-associated infections. J. Appl. Biomater. Funct. Mater. 2014, 12, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Tunney, M.M.; Patrick, S.; Gorman, S.P.; Nixon, J.R.; Anderson, N.; Davis, R.I.; Hanna, D.; Ramage, G. Improved detection of infection in hip replacements. A currently underestimated problem. J. Bone Jt. Surg. Br. 1998, 80, 568–572. [Google Scholar] [CrossRef]
- Trampuz, A.; Piper, K.E.; Jacobson, M.J.; Hanssen, A.D.; Unni, K.K.; Osmon, D.R.; Mandrekar, J.N.; Cockerill, F.R.; Steckelberg, J.M.; Greenleaf, J.F.; et al. Sonication of removed hip and knee prostheses for diagnosis of infection. N. Engl. J. Med. 2007, 357, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Douiri, N.; Hansmann, Y.; Lefebvre, N.; Riegel, P.; Martin, M.; Baldeyrou, M.; Christmann, D.; Prevost, G.; Argemi, X. Staphylococcus lugdunensis: A virulent pathogen causing bone and joint infections. Clin. Microbiol. Infect. 2016, 22, 747–748. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, S.; Selan, L.; Visai, L.; Pirini, V.; Campoccia, D.; Maso, A.; Speziale, P.; Montanaro, L.; Arciola, C.R. Staphylococcus lugdunensis, an aggressive coagulase-negative pathogen not to be underestimated. Int. J. Artif. Organs 2012, 35, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Arciola, C.R.; Hansch, G.M.; Visai, L.; Testoni, F.; Maurer, S.; Campoccia, D.; Selan, L.; Montanaro, L. Interactions of staphylococci with osteoblasts and phagocytes in the pathogenesis of implant-associated osteomyelitis. Int. J. Artif. Organs 2012, 35, 713–726. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Prosthetic Joint Infection | Hip | Knee |
|---|---|---|
| Number of patients | 98 | 111 |
| Age (years) | median 74 | median 69 |
| range: 18–91 | range: 27–91 | |
| IQR: 16.5 | IQR: 15 | |
| Gender | 52 female | 44 female |
| 46 male | 67 male | |
| elevated CRP serum concentration (reference value >5 mg/L) | 98% | 85% |
| Bacteria detected in tissue samples | 80.60% | 72.10% |
| Implant loosening | 59.80% | 44.6% * |
| Duration since primary prosthetic joint replacement (months) | median 48 | median 36 |
| range: 1–408 | range: 1–300 | |
| IQR: 152 | IQR: 75 | |
| Duration since last surgical intervention (months) | median 12 | median 12 |
| range: 1–276 | range: 1–180 | |
| IQR: 47 | IQR: 32 |
| Bacteria Species | Hip | Knee |
|---|---|---|
| S. aureus | 48 | 28 |
| (IQR 198) | (IQR 72.5) | |
| S. epidermidis | 41 | 36 |
| (IQR 129.5) | (IQR 109.5) | |
| other Staphylococcus spp. | 33 | 38 |
| (IQR 83) | (IQR 55) | |
| Streptococcus spp. | 162 * | 61 |
| (IQR 197) | (IQR 64) | |
| Enterococcus spp. | 12 ** | 29 |
| (IQR 78) | (IQR 46) | |
| no bacteria | 72 | 54 |
| (IQR 154) | (IQR 84.5) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dapunt, U.; Radzuweit-Mihaljevic, S.; Lehner, B.; Haensch, G.M.; Ewerbeck, V. Bacterial Infection and Implant Loosening in Hip and Knee Arthroplasty: Evaluation of 209 Cases. Materials 2016, 9, 871. https://doi.org/10.3390/ma9110871
Dapunt U, Radzuweit-Mihaljevic S, Lehner B, Haensch GM, Ewerbeck V. Bacterial Infection and Implant Loosening in Hip and Knee Arthroplasty: Evaluation of 209 Cases. Materials. 2016; 9(11):871. https://doi.org/10.3390/ma9110871
Chicago/Turabian StyleDapunt, Ulrike, Stephanie Radzuweit-Mihaljevic, Burkhard Lehner, Gertrud Maria Haensch, and Volker Ewerbeck. 2016. "Bacterial Infection and Implant Loosening in Hip and Knee Arthroplasty: Evaluation of 209 Cases" Materials 9, no. 11: 871. https://doi.org/10.3390/ma9110871