
The Changing Detection Rate of Respiratory Syncytial Virus in Adults in Western Australia between 2017 and 2023
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Location
2.2. Laboratory Data
2.3. Analysis
3. Results
3.1. RSV Seasonality in the Baseline Period between 2017 and 2019
3.2. SARS-CoV-2-Related Non-Pharmaceutical Interventions and RSV Seasonality
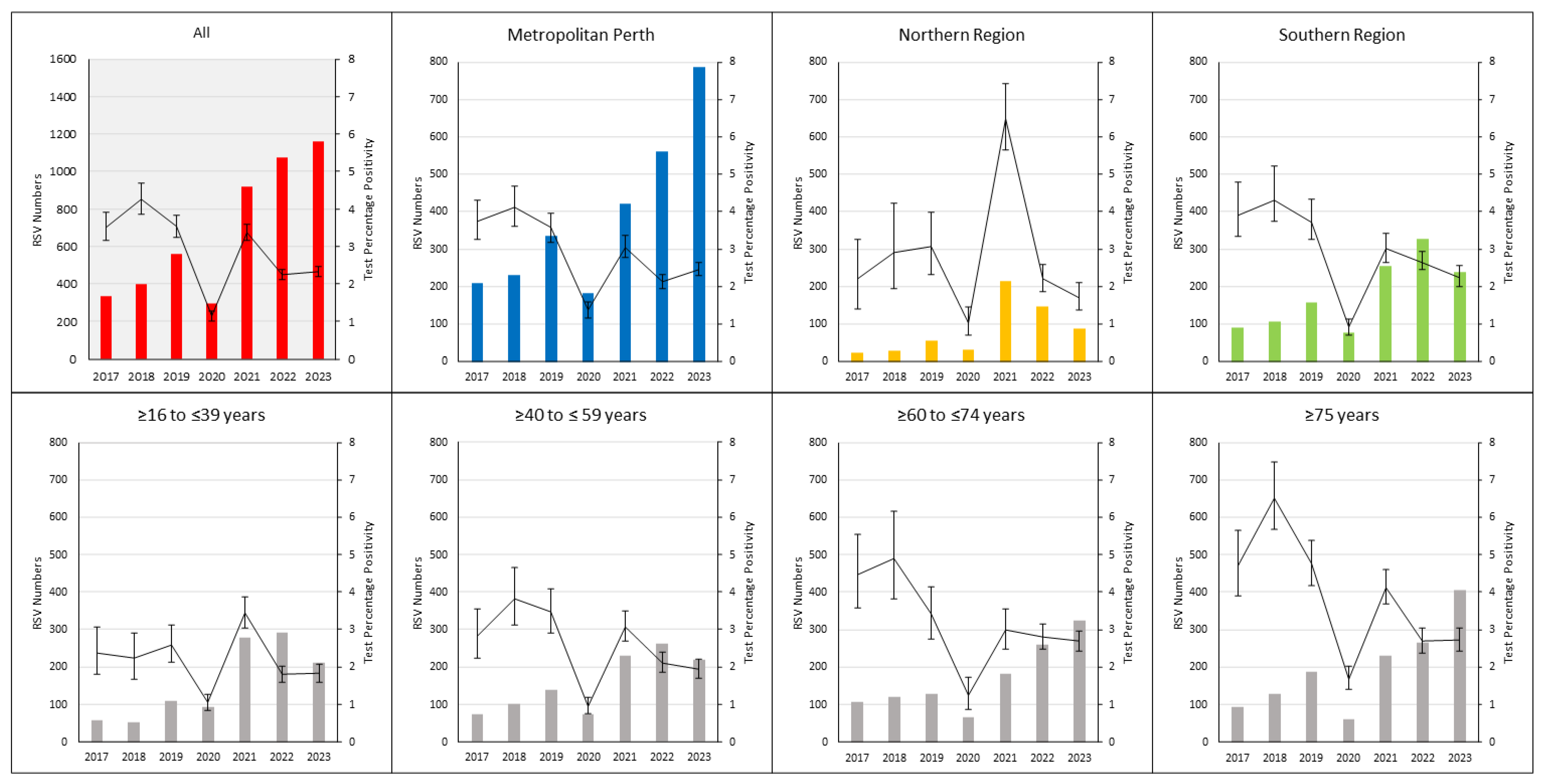
3.3. RSV Detection Rates per Year
3.4. Testing and Percentage Positivity
3.5. RSV Testing and Detections by Age Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen-Van-Tam, J.S.; O’Leary, M.; Martin, E.T.; Heijnen, E.; Callendret, B.; Fleischhackl, R.; Comeaux, C.; Tran, T.M.P.; Weber, K. Burden of respiratory syncytial virus infection in older and high-risk adults: A systematic review and meta-analysis of the evidence from developed countries. Eur. Respir. Rev. 2022, 31, 220105. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; Campbell, H.; Demont, C.; Nyawanda, B.O.; Chu, H.Y.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 222 (Suppl. S7), S577–S583. [Google Scholar] [CrossRef] [PubMed]
- Saravanos, G.L.; Sheel, M.; Homaira, N.; Dey, A.; Brown, E.; Wang, H.; Macartney, K.; Wood, N.J. Respiratory syncytial virus-associated hospitalisations in Australia, 2006–2015. Med. J. Aust. 2019, 210, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Mazur, N.I.; Terstappen, J.; Baral, R.; Bardají, A.; Beutels, P.; Buchholz, U.J.; Cohen, C.; Crowe, J.E.; Cutland, C.L.; Eckert, L. Respiratory syncytial virus prevention within reach: The vaccine and monoclonal antibody landscape. Lancet Infect. Dis. 2023, 23, e2–e21. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef]
- Foley, D.A.; Sikazwe, C.T.; Minney-Smith, C.A.; Ernst, T.; Moore, H.C.; Nicol, M.P.; Smith, D.W.; Levy, A.; Blyth, C.C. An Unusual Resurgence of Human Metapneumovirus in Western Australia Following the Reduction of Non-Pharmaceutical Interventions to Prevent SARS-CoV-2 Transmission. Viruses 2022, 14, 2135. [Google Scholar] [CrossRef]
- Nagakubo, Y.; Hirotsu, Y.; Maejima, M.; Shibusawa, M.; Hosaka, K.; Amemiya, K.; Sueki, H.; Hayakawa, M.; Mochizuki, H.; Tsutsui, T.; et al. Non-pharmaceutical interventions during the COVID-19 epidemic changed detection rates of other circulating respiratory pathogens in Japan. PLoS ONE 2022, 17, e0262874. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.S.; Cowling, B.J.; Peiris, J.S.M.; Chan, E.L.Y.; Wong, W.H.S.; Lee, K.P. Effects of Nonpharmaceutical COVID-19 Interventions on Pediatric Hospitalizations for Other Respiratory Virus Infections, Hong Kong. Emerg. Infect. Dis. 2022, 28, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Department of the Premier and Cabinet. Review of Western Australia’s COVID-19 Management and Response; The Government of Western Australia: West Perth, Australia, 2023.
- Eden, J.S.; Sikazwe, C.; Xie, R.; Deng, Y.M.; Sullivan, S.G.; Michie, A.; Levy, A.; Cutmore, E.; Blyth, C.C.; Britton, P.N.; et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat. Commun. 2022, 13, 2884. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Phuong, L.K.; Peplinski, J.; Lim, S.M.J.; Lee, W.H.; Keane, A.; Wong, J.W.S.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; et al. Examining the entire delayed respiratory syncytial virus season in Western Australia. Arch. Dis. Child. 2022, 107, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Minney-Smith, C.A.; Foley, D.A.; Sikazwe, C.T.; Levy, A.; Smith, D.W. The seasonality of respiratory syncytial virus in Western Australia prior to implementation of SARS-CoV-2 non-pharmaceutical interventions. Influenza Other Respir. Viruses 2023, 17, e13117. [Google Scholar] [CrossRef] [PubMed]
- Speers, D.J.; Moss, D.M.; Minney-Smith, C.; Levy, A.; Smith, D.W. Influenza and respiratory syncytial virus are the major respiratory viruses detected from prospective testing of pediatric and adult coronial autopsies. Influenza Other Respir. Viruses 2013, 7, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Epidemiological Surveillance Standards for Influenza; World Health Organization: Geneva, Switzerland, 2013.
- Grilc, E.; Prosenc Trilar, K.; Lajovic, J.; Socan, M. Determining the seasonality of respiratory syncytial virus in Slovenia. Influenza Other Respir. Viruses 2021, 15, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics Australian Demographic Statisitics. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Latestproducts/3101.0Main%20Features3Dec%202019?opendocument&tabname=Summary&prodno=3101.0&issue=Dec%202019&num=&view= (accessed on 1 February 2024).
- Htar, M.T.T.; Yerramalla, M.; Moïsi, J.; Swerdlow, D. The burden of respiratory syncytial virus in adults: A systematic review and meta-analysis. Epidemiol. Infect. 2020, 148, e48. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simoes, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef] [PubMed]
- Savic, M.; Penders, Y.; Shi, T.; Branche, A.; Pircon, J.Y. Respiratory syncytial virus disease burden in adults aged 60 years and older in high-income countries: A systematic literature review and meta-analysis. Influenza Other Respir. Viruses 2023, 17, e13031. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.; Blyth, C.C.; de Klerk, N.; Lee, W.H.; Borland, M.L.; Richmond, P.; Lim, F.J.; Fathima, P.; Moore, H.C. Geographical disparities in emergency department presentations for acute respiratory infections and risk factors for presenting: A population-based cohort study of Western Australian children. BMJ Open 2019, 9, e025360. [Google Scholar] [CrossRef] [PubMed]
- Paynter, S. Humidity and respiratory virus transmission in tropical and temperate settings. Epidemiol. Infect. 2015, 143, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Obando-Pacheco, P.; Justicia-Grande, A.J.; Rivero-Calle, I.; Rodriguez-Tenreiro, C.; Sly, P.; Ramilo, O.; Mejias, A.; Baraldi, E.; Papadopoulos, N.G.; Nair, H.; et al. Respiratory Syncytial Virus Seasonality: A Global Overview. J. Infect. Dis. 2018, 217, 1356–1364. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Seasons | 2017 | 2018 | 2019 | 2020/21 | 2021/22 | 2022 | 2023 |
|---|---|---|---|---|---|---|---|
| Timing | Week 19 to 44 | Week 12 to 42 | Week 17 to 42 | Week 44 to 15 | Week 32 to 8 | Week 31 to 46 | Week 22 to 43 |
| Duration (weeks) | 32 | 31 | 26 | 25 | 29 | 16 | 22 |
| Onset Date | 8 May 2017 | 19 Mar 2018 | 22 April 2019 | 26 October 2020 | 9 August 2021 | 1 August 2022 | 29 May 2023 |
| Offset Date | 5 November 2017 | 21 October 2018 | 20 October 2019 | 18 April 2021 | 27 February 2022 | 20 November 2022 | 29 October 2023 |
| Detections; n | 284 | 344 | 482 | 642 | 542 | 688 | 949 |
| Mean Detections/Week | 9 | 11 | 19 | 26 | 19 | 43 | 44 |
| Total Tests; n | 6424 | 6415 | 11,635 | 9654 | 17,687 | 14,221 | 23,146 |
| % Positive (95% CI) | 4.4 (3.9 to 5) | 5.4 (4.8 to 6) | 4.1 (3.8 to 4.5) | 6.7 (6.1 to 7.2) | 3.1 (2.8 to 3.3) | 4.8 (4.5 to 5.2) | 4.1 (3.8 to 4.4) |
| Year | 2017 | 2018 | 2019 | 2020 * | 2021 * | 2022 * | 2023 |
|---|---|---|---|---|---|---|---|
| Detections; n | 333 | 400 | 562 | 294 | 919 | 1077 | 1158 |
| Total Tests; n | 9475 | 9403 | 15,910 | 25,643 | 27,228 | 47,814 | 49,943 |
| % Positive (95% CI) | 3.5 (3.1 to 3.9) | 4.3 (3.8 to 4.7) | 3.5 (3.2 to 3.8) | 1.1 (1 to 1.3) | 3.4 (3.2 to 3.6) | 2.3 (2.1 to 2.4) | 2.3 (2.2 to 2.5) |
| Detection rate per year (95% CI) | Detection rate per year (95% CI) | Detection rate per year (95% CI) | Detection rate per year (95% CI) | Detection rate per year (95% CI) | Detection rate per year (95% CI) | Detection rate per year (95% CI) | |
| All | 16.3 (14.6 to 18.1) | 19.3 (17.5 to 21.3) | 26.7 (24.6 to 29) | 13.7 (12.2 to 15.3) | 42.2 (39.5 to 45) | 48.7 (45.9 to 51.7) | 50.7 (47.9 to 53.8) |
| By Region | |||||||
| Metropolitan Perth | 12.4 (10.7 to 14.2) | 13.7 (12 to 15.5) | 19.8 (17.8 to 22.1) | 10.8 (9.3 to 12.5) | 25 (22.6 to 27.5) | 33.2 (30.6 to 36.1) | 46.6 (43.4 to 49.9) |
| Northern Region | 35.2 (22.6 to 52.4) | 41.1 (27.3 to 59.4) | 82.2 (62.1 to 106.8) | 45.5 (30.9 to 64.6) | 314.2 (273.5 to 359.2) | 215.8 (182.3 to 253.6) | 127.7 (102.3 to 157.5) |
| Southern Region | 25.8 (20.8 to 31.6) | 29.7 (24.3 to 35.9) | 44.3 (37.6 to 51.7) | 21.3 (16.8 to 26.7) | 71.7 (63.2 to 81.1) | 91.9 (82.2 to 102.4) | 66.7 (58.5 to 75.7) |
| By Age Group | |||||||
| ≥16 to ≤39 years | 6.6 (5.0 to 8.5) | 6 (4.5 to 7.9) | 12.2 (10.0 to 14.7) | 10.4 (8.4 to 12.7) | 31.2 (27.6 to 35.1) | 32.5 (28.9 to 36.5) | 22.6 (19.6 to 25.8) |
| ≥40 to ≤59 years | 11.2 (8.8 to 14) | 14.9 (12.1 to 18.1) | 20.3 (17.1 to 24) | 10.6 (8.3 to 13.3) | 32.6 (28.5 to 37.1) | 36.6 (32.3 to 41.4) | 30.1 (26.2 to 34.3) |
| ≥60 to ≤74 years | 31.2 (25.5 to 37.7) | 33.4 (27.7 to 40.0) | 35 (29.2 to 41.5) | 16.8 (13.0 to 21.4) | 45.2 (38.9 to 52.3) | 63.7 (56.2 to 71.9) | 77.7 (69.5 to 86.7) |
| ≥75 years | 62.2 (50.2 to 76.2) | 81.6 (68 to 97.1) | 114.2 (98.3 to 131.8) | 36.1 (27.7 to 46.3) | 127.5 (111.6 to 145.1) | 138 (121.8 to 155.7) | 199.5 (180.5 to 220.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foley, D.A.; Minney-Smith, C.A.; Tjea, A.; Nicol, M.P.; Levy, A.; Moore, H.C.; Blyth, C.C. The Changing Detection Rate of Respiratory Syncytial Virus in Adults in Western Australia between 2017 and 2023. Viruses 2024, 16, 656. https://doi.org/10.3390/v16050656
Foley DA, Minney-Smith CA, Tjea A, Nicol MP, Levy A, Moore HC, Blyth CC. The Changing Detection Rate of Respiratory Syncytial Virus in Adults in Western Australia between 2017 and 2023. Viruses. 2024; 16(5):656. https://doi.org/10.3390/v16050656
Chicago/Turabian StyleFoley, David A., Cara A. Minney-Smith, Andrew Tjea, Mark P. Nicol, Avram Levy, Hannah C. Moore, and Christopher C. Blyth. 2024. "The Changing Detection Rate of Respiratory Syncytial Virus in Adults in Western Australia between 2017 and 2023" Viruses 16, no. 5: 656. https://doi.org/10.3390/v16050656