
Colorectal Cancer: Disease Process, Current Treatment Options, and Future Perspectives
College of Pharmacy, Howard University, 2400 6th St NW, Washington, DC 20059, USA
*
Author to whom correspondence should be addressed.
Pharmaceutics 2023, 15(11), 2620; https://doi.org/10.3390/pharmaceutics15112620
Submission received: 21 September 2023
/
Revised: 28 October 2023
/
Accepted: 2 November 2023
/
Published: 12 November 2023
Abstract
:Colorectal cancer (CRC) is one of the deadliest malignancies in the US, ranking fourth after lung, prostate, and breast cancers, respectively, in general populations. It continues to be a menace, and the incidence has been projected to more than double by 2035, especially in underdeveloped countries. This review seeks to provide some insights into the disease progression, currently available treatment options and their challenges, and future perspectives. Searches were conducted in the PubMed search engine in the university’s online library. The keywords were “Colorectal Cancer” AND “disease process” OR “disease mechanisms” OR “Current Treatment” OR “Prospects”. Selection criteria were original articles published primarily during the period of 2013 through 2023. Abstracts, books and documents, and reviews/systematic reviews were filtered out. Of over 490 thousand articles returned, only about 800 met preliminary selection criteria, 200 were reviewed in detail, but 191 met final selection criteria. Fifty-one other articles were used due to cross-referencing. Although recently considered a disease of lifestyle, CRC incidence appears to be rising in countries with low, low–medium, and medium social demographic indices. CRC can affect all parts of the colon and rectum but is more fatal with poor disease outcomes when it is right-sided. The disease progression usually takes between 7–10 years and can be asymptomatic, making early detection and diagnosis difficult. The CRC tumor microenvironment is made up of different types of cells interacting with each other to promote the growth and proliferation of the tumor cells. Significant advancement has been made in the treatment of colorectal cancer. Notable approaches include surgery, chemotherapy, radiation therapy, and cryotherapy. Chemotherapy, including 5-fluorouracil, irinotecan, oxaliplatin, and leucovorin, plays a significant role in the management of CRC that has been diagnosed at advanced stages. Two classes of monoclonal antibody therapies have been approved by the FDA for the treatment of colorectal cancer: the vascular endothelial growth factor (VEGF) inhibitor, e.g., bevacizumab (Avastin®), and the epidermal growth factor receptor (EGFR) inhibitor, e.g., cetuximab (Erbitux®) and panitumumab (Verbitix®). However, many significant problems are still being experienced with these treatments, mainly off-target effects, toxic side effects, and the associated therapeutic failures of small molecular drugs and the rapid loss of efficacy of mAb therapies. Other novel delivery strategies continue to be investigated, including ligand-based targeting of CRC cells.
1. Introduction
Globally, colorectal cancer (CRC) is the third most commonly diagnosed cancer (with approximately 1.9 million cases) and the second most common cause of death (with approximately 0.9 million deaths worldwide) in 2020 [1]. Thus, colorectal cancer (CRC) accounts for about 10% of cancer cases and deaths, thus constituting a major component of the global cancer burden [2]. Although CRC is presently considered primarily a disease of Western society, a more rapid increase in incidence is being recorded in countries experiencing economic development with the associated changes in lifestyle and diet [3]. In addition, while the availability of screening services and improved treatment is considerably reducing CRC incidence and mortality in affluent countries [4], available screening programs and existing medical services are grossly inadequate [5] for timely diagnosis and treatment of cases that could arrest the escalating increase in incidence and death rates in the less affluent countries. A study by Liu et al. [2] showed that, when visualized at the social demographic index (SDI) level, the trend of age-adjusted death rate (AADR) increased in the low, low–middle, and middle SDI regions while it decreased in the high SDI region.
Despite the existence of effective screening techniques in high SDI regions that could reduce mortality rates, CRC continues to be a significant health threat [6]. In the US, CRC is presently the fourth most diagnosed but still the second most deadly after lung cancer [7]. It is projected that in 2023, there will be 153,020 new cases of colon cancer and 52,550 new cases of rectal cancer in the United States and that the global incidence of CRC will more than double by 2035, with the greatest increase in CRC burden and death expected in less developed countries [7,8]. The diversity of CRC diagnosis, prognosis, and survival is well established among the US population. CRC mortality is 36% higher among African-American men than among non-Hispanic white men and 34% higher among African-American women than among non-Hispanic white women [9,10,11].
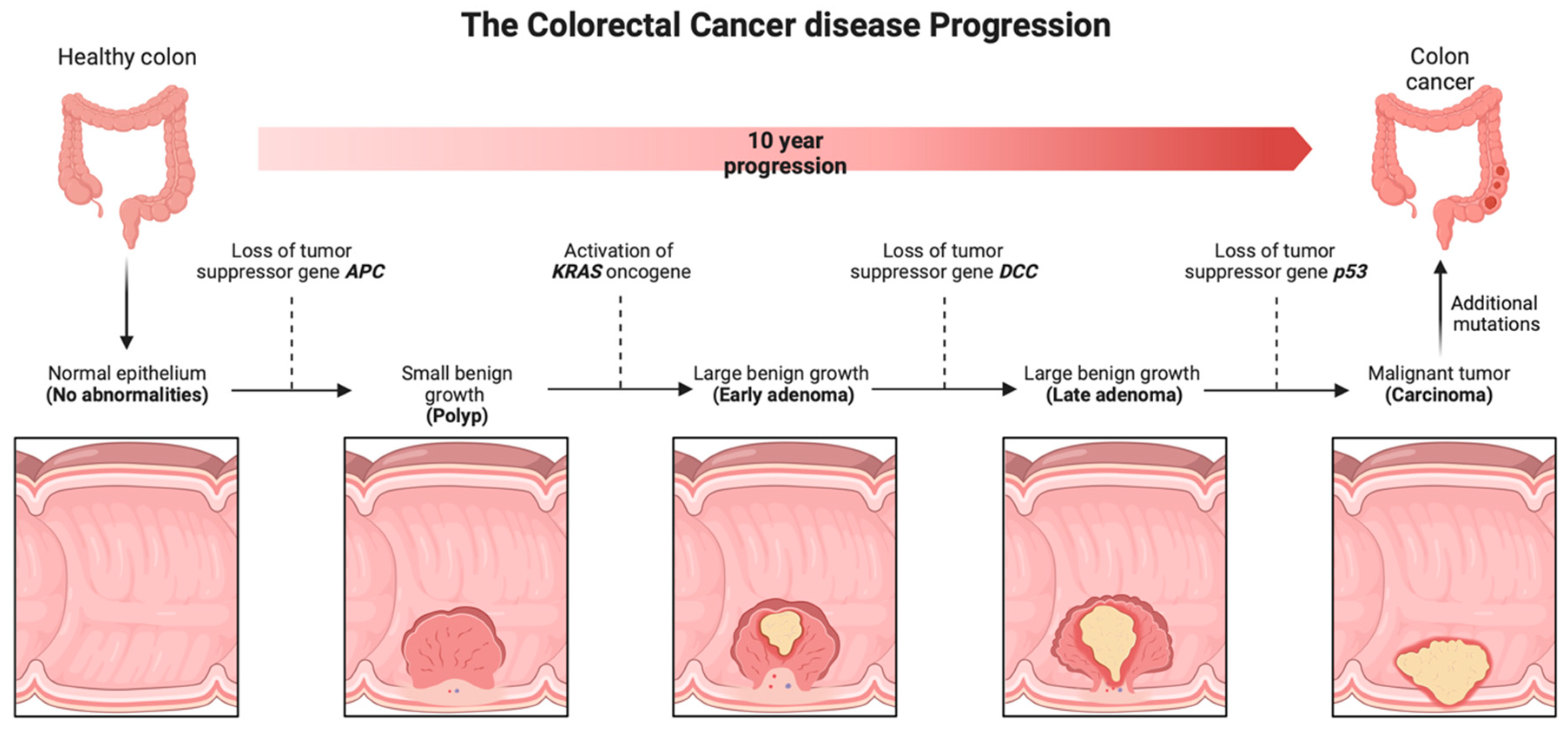
Histologically, adenocarcinoma is the most prevalent variant of colon cancer. Other histological types are scirrhous and neuroendocrine tumors [8]. Adenomatous polyposis coli (APC) is a CRC tumor suppressor gene found on the 5q21-q22 chromosome. APC is a colorectal cancer gene that is dysregulated at both the germline and somatic levels [12,13]. APC gene encodes a 310 kDa protein containing 2843 amino acids. About 75% of the coding sequence is located on exon 15, the most common region for both germline and somatic mutations of APC. APC’s germline mutations result in familial adenomatous polyposis (FAP), the major hereditary predisposition to CRC development [12,14]. On the other hand, somatic APC mutations are associated with more than 80% of sporadic colorectal tumors. Apart from CRC caused by CpG island methylator phenotype (CIMP) or mismatch repair hypermutable microsatellite instability (MSI) phenotype, alterations in the APC gene are the initiator of over 85% of sporadic colorectal cancers [13,14]. In addition, sporadic CRC cases, with no family history or inherited genomic alterations, comprise 60–65% of all CRC cases [15,16].
CRC arises from the epithelial cells lining the colon or rectum in the gastrointestinal tract due to abnormal growth of glandular epithelial cells [17]. The development of colorectal adenocarcinomas is caused by sequential genetic and epigenetic mutations in specific oncogenes in the epithelial cells of the gastrointestinal tract [18]. The normal epithelium forms into hyperproliferative mucosa and eventually forms a benign adenoma, which can then progress to carcinoma and metastasis over the course of about 10 years. This process occurs through various mechanisms, including microsatellite instability (MSI) and chromosomal instability (CIN) pathways [19].
In MSI, tumors are caused by the inactivation of one of the four mismatch repair (MMR)genes: MSH2, MLH1, MSH6, and PMS2. During normal DNA replication, these proficient MMR genes detect errors in DNA mismatches, and the MLH1 and/or PMS2 heterodimer helps remove these errors and form new, corrected DNA strands [20]. The human genome contains over 10,000 regions of short tandem repeat sequences called microsatellites, which are prone to replication errors and heavily rely on the MMR system for repair. Deficiency in the MMR system leads to a faster accumulation of genetic errors at these microsatellites, resulting in the formation of tumors [21]. In CIN, tumors are caused by mutations in genes that result in chromosomal aneuploidy, loss of heterozygosity, and structural chromosomal rearrangements. In addition to these karyotypic abnormalities, CIN tumors also have an accumulation of specific mutations in tumor suppressor genes and oncogenes that activate pathways crucial for the initiation and progression of CRC [22].
The most common biomarkers, which are overexpressed in the CRC cellular membrane, include the folate receptor (FR-α, 37.1%), epidermal growth factor receptor (EGFR, 32.8%), the carcinoembryonic antigen (CEA, 98.8%), and tumor-associated glycoprotein (TAG-72, 79%) [23]. A major biomarker that has been extensively reported to be overexpressed in CRC is the human transferrin receptor (hTfR). The human transferrin receptor (hTfR) is ubiquitous and overexpressed (>100 folds) in many cancers [24,25,26,27,28].
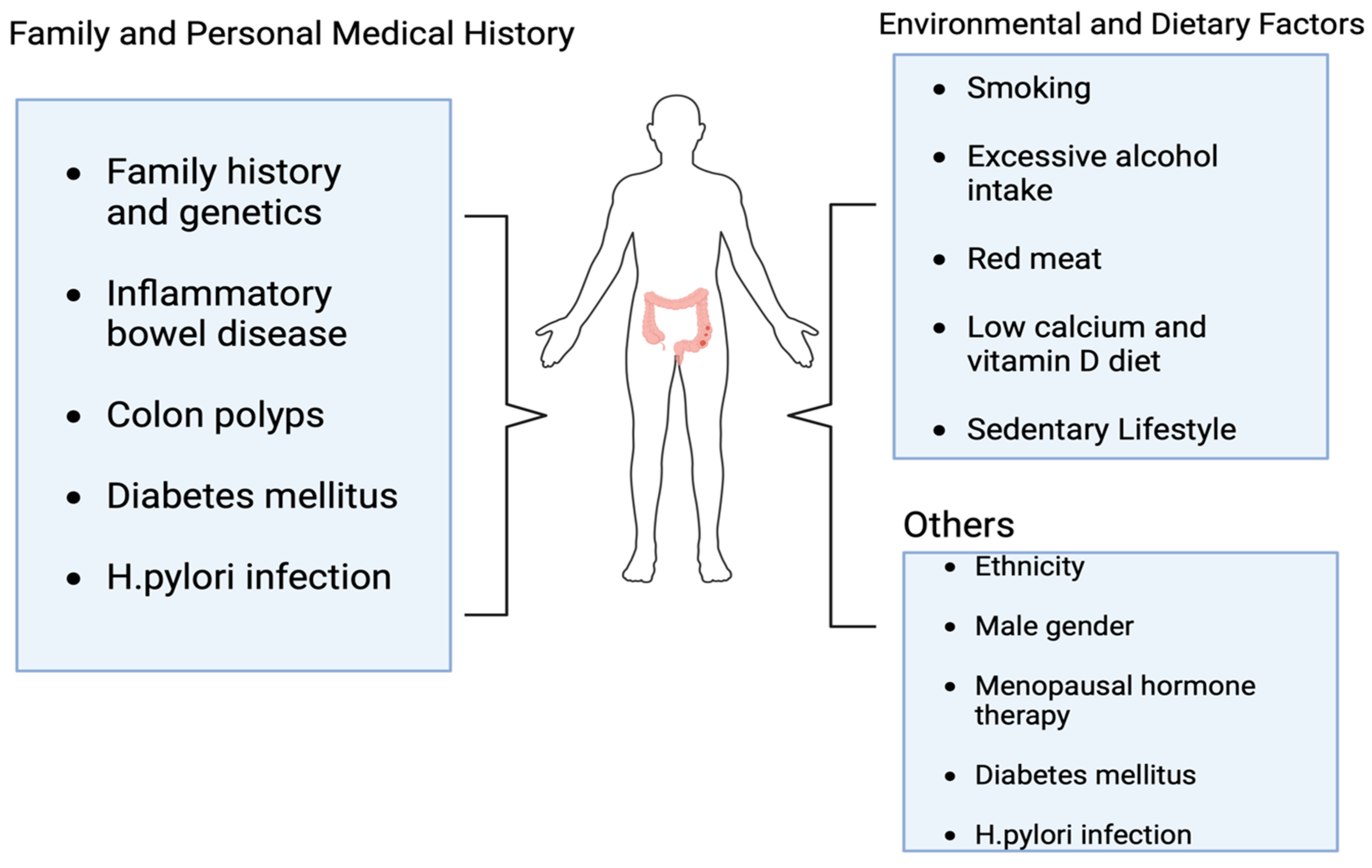
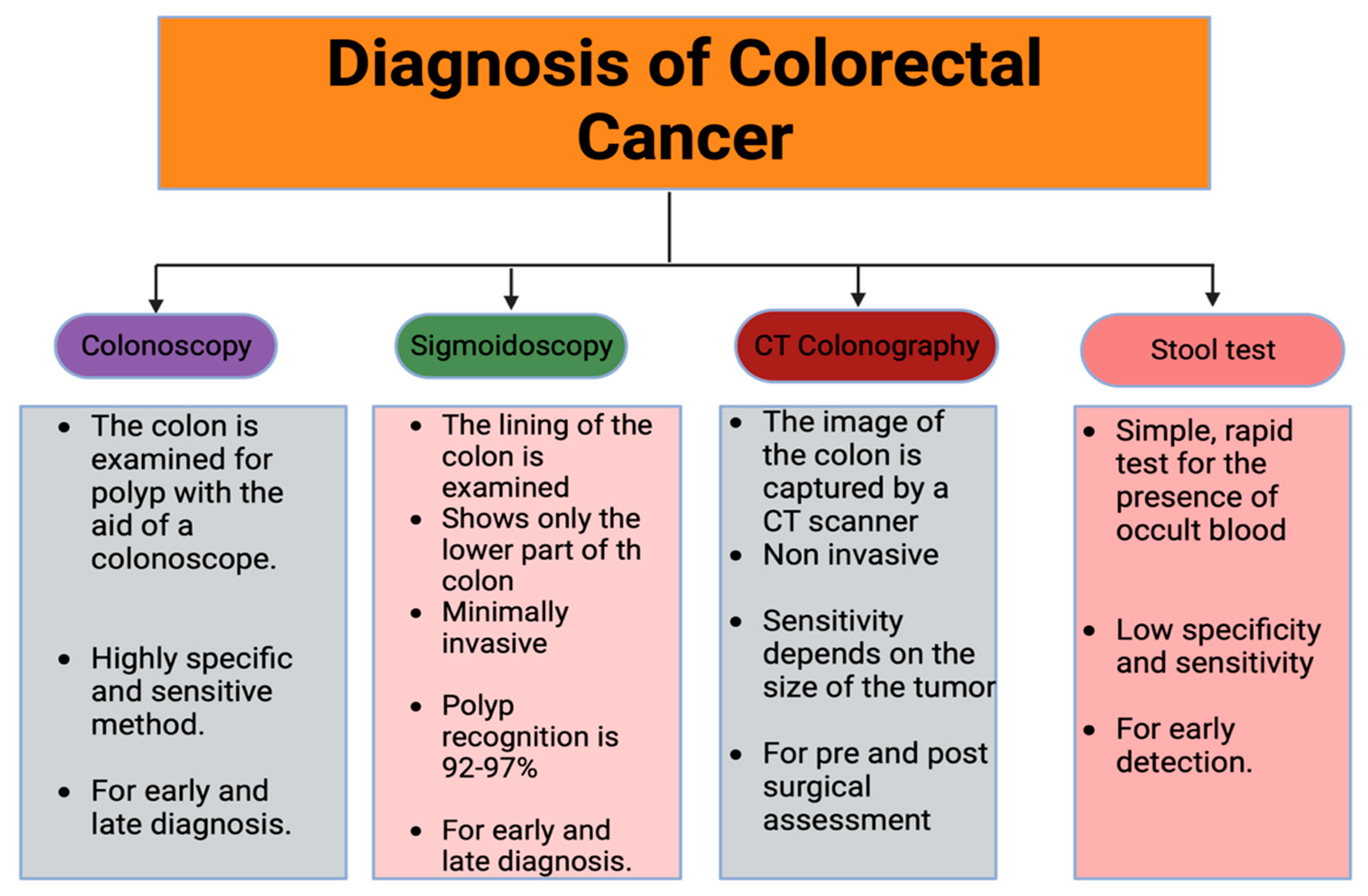
The most significant risk factor in the development of colorectal cancer is age, with adolescents and older individuals being more susceptible. Other risk factors include sedentary behaviors, Western-style diets, smoking, diabetes, obesity, and, most importantly, the occurrence of ulcerative colitis as a result of H. pylori infection (Figure 1) [29], which will be discussed later in this review. Although early-stage disease treatment yields the most favorable results, approximately half of the colorectal cancer patients are either diagnosed with metastatic disease, develop the advanced-stage disease later, or experience cancer recurrence within a few months [30]. For those with metastatic disease that cannot be treated through surgery, the prognosis is bleak, with a 5-year survival rate of roughly 14% [31,32]. The diagnosis of CRC is made using various methods and techniques with varying sensitivities (Figure 2). Studies have shown that individuals who undergo colonoscopy have a lower risk of developing CRC compared to those who do not get screened [33]. The effectiveness of sigmoidoscopy in reducing both the incidence and CRC-related death has been established, as well as the combination of sigmoidoscopy and stool testing, which are cost-effective approaches but, unfortunately, have not been well utilized in established guidelines [34,35].
2. Search Method
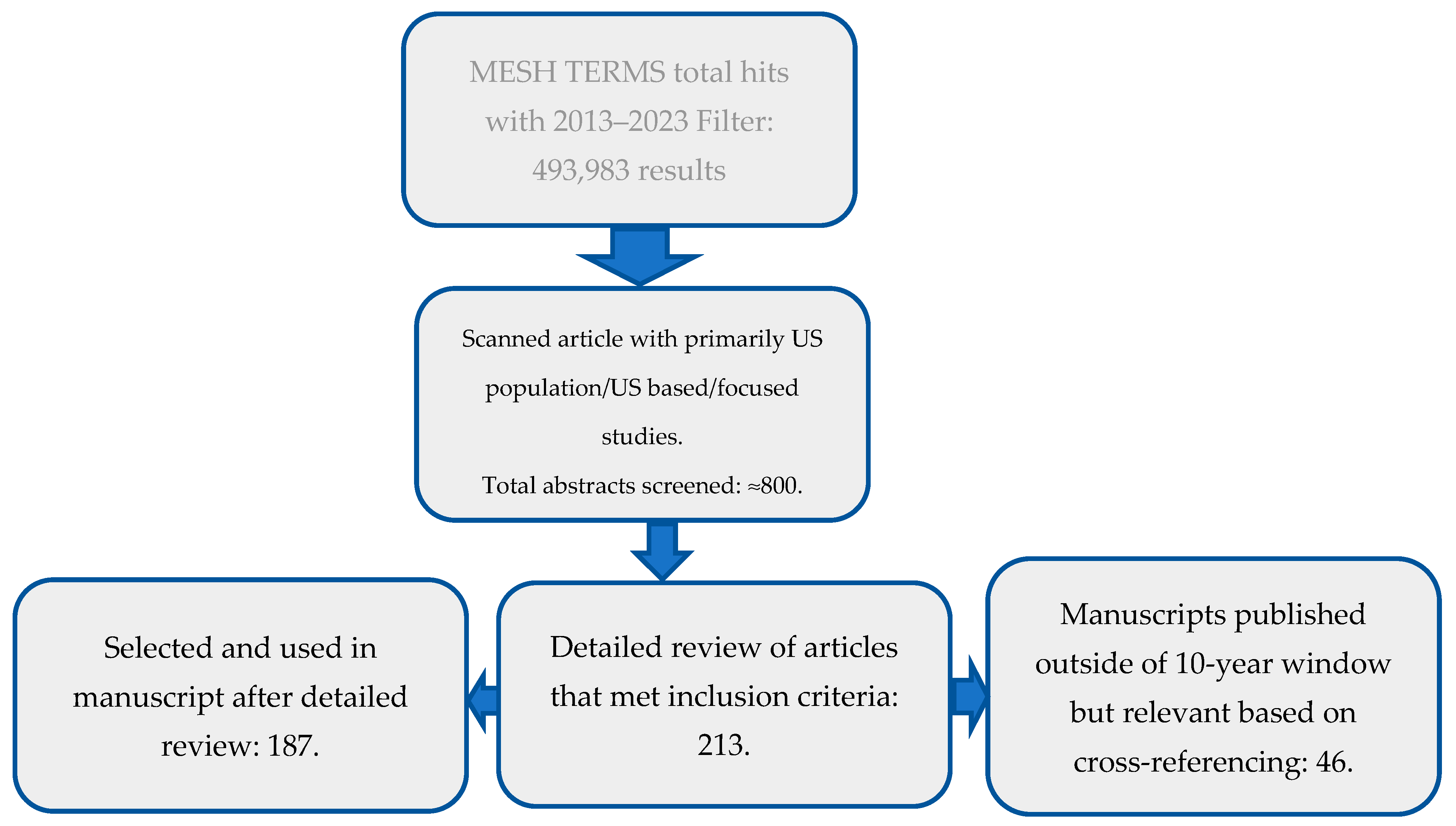
Searches were conducted electronically online, primarily in PubMed. The MESH words used for the search were (((((((((Colorectal Cancer) AND (disease process)) OR (disease mechanisms)) OR (Current Treatment)) OR (Prospects)) NOT (abstract)) NOT (books and documents)) NOT (review)) NOT (systematic review)). The result was filtered for the past 10 years (2013–2023). A total of 493,983 results were obtained. Article selection protocol is shown in Figure 3 below.
Additional searches were conducted in Google Scholar for any article that was found relevant due to the historical perspective of the study through citations in primary articles. Such articles have been included in order to avoid information gaps and to substantiate important claims by primary articles found in PubMed engine.
3. Results and Discussion
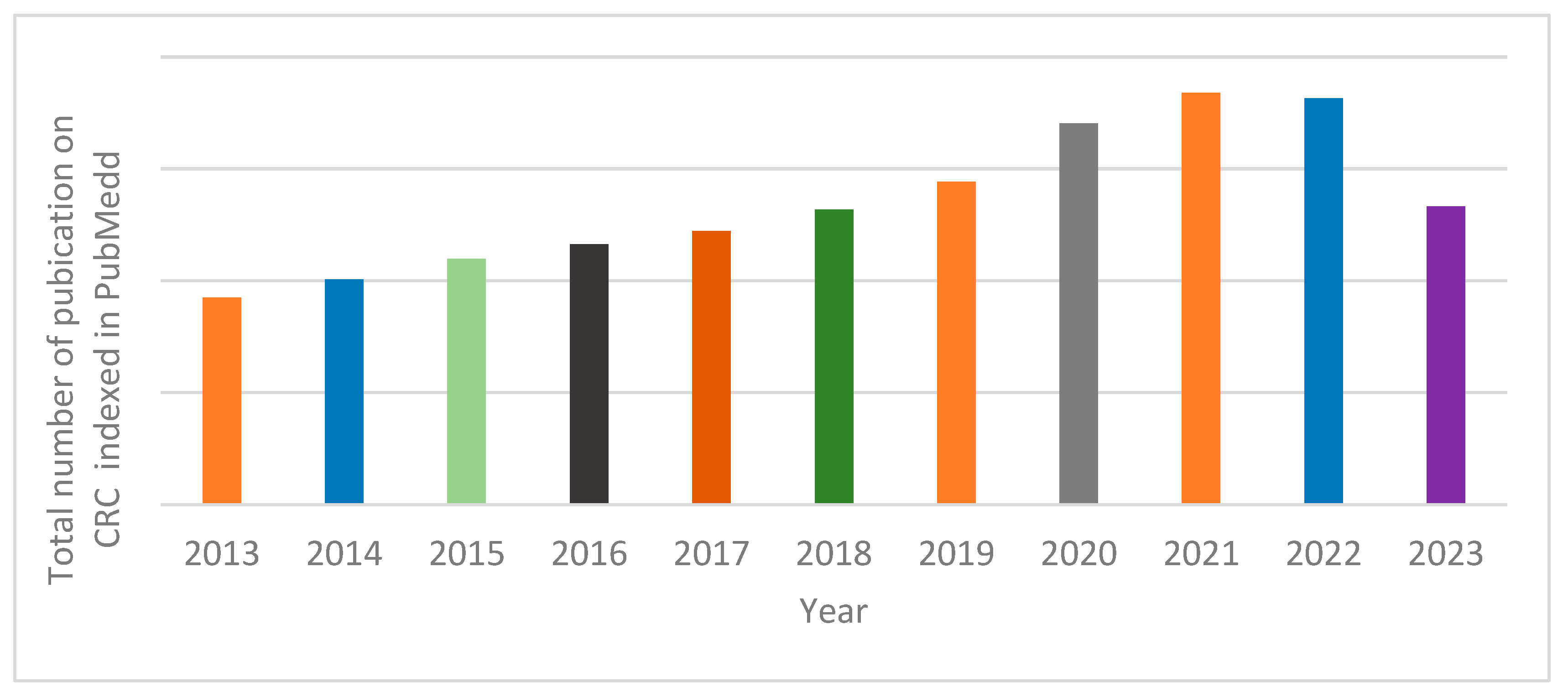
Figure 4 shows the distribution of published manuscripts on colorectal cancer based on the MESH terms used. An average of 54 thousand CRC-related manuscripts were published annually as retrieved by the MESH terms used. Annual number of published manuscripts on the subject of CRC rose steadily between 2013 and 2020. The highest number of annual publications was recorded in the year 2021.
3.1. The Colon and Peculiarities of Colorectal Cancer
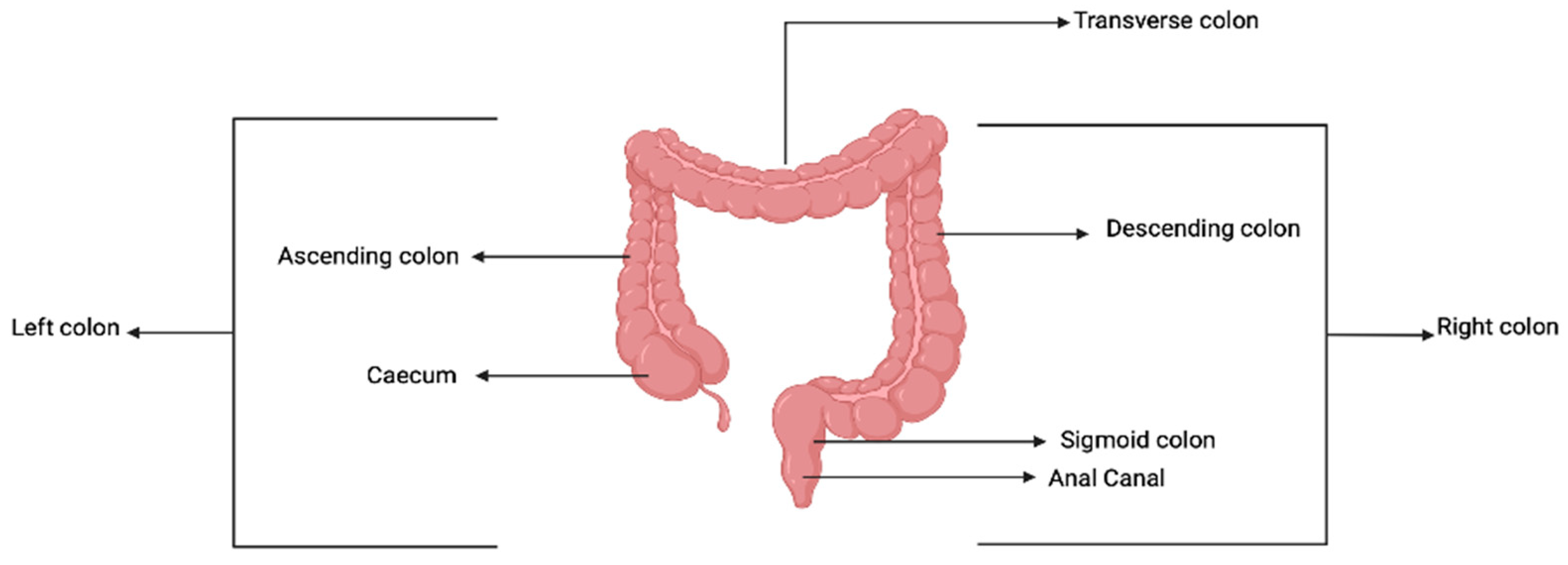
The colon is an important part of the gastrointestinal tract and is located in the abdomen, just below the stomach. It is about 150 cm long; the starting point is called the caecum, and the ending point is the anal verge. The colon is divided into four segments, namely: caecum and appendix vermiformis, colon segments which are divided into ascending, transverse descending colon, sigmoid colon, and anal canal. The first two segments are referred to as the left colon, and the last two are called the right colon. These segments have varying diameters; the caecum is the widest (7.5 cm), and the sigmoid colon is the narrowest (2.5 cm) [36]. In terms of embryology, the colon arises from the midgut and hindgut; the midgut gives rise to the transverse colon, ascending colon, and caecum, while the hindgut gives rise to descending colon, sigmoid colon, and anal canal. A description is shown in Figure 5.
The colon’s primary function is to extract water, nutrients, and electrolytes from partially digested food and to further process the remaining material to form stool. The stool is stored in the rectum and eventually expelled from the body through the anus [37].
3.2. CRC Development Processes
CRC can be categorized based on the location of the tumor within the colon and rectum. Right-sided colon cancers are found in the transverse colon, ascending colon, and caecum, while left-sided colon carcinomas are found in the transverse colon, descending colon, sigmoid colon, and anal canal [38,39]. Based on this categorization, the majority (about 63%) of diagnosed CRC is left-sided and mostly in younger patients [40,41].
Disease progression of colorectal cancer is shown in Figure 6. The symptoms and the prognosis of CRC have been shown by several studies to be associated with the location of the tumor [42,43]. Symptoms associated with left-side colorectal cancer include partial or total intestinal obstruction due to the narrow lumen of the colon on this side. As a result of the obstruction, symptoms such as constipation, nausea, abdominal distention, and abdominal pain are common. Right-sided CRC usually results in gross rectal bleeding, and the patient may present with iron-deficiency anemia [44]. Patients with right-sided CRC usually have a poor prognosis and are prone to metastasis compared to left-sided tumors [45,46]. The need for early diagnosis and search for more effective therapies is underscored by the fact that the majority of CRC (approx. 50%) are diagnosed at an advanced stage with resulting poor prognosis and high mortality [47].
The colorectal tumor microenvironment (TME) is characterized by multiple distinct cell types, primarily originating from the adjacent mesenchymal stroma and their interaction with tumor cells. The interactions between the tumor cells and neighboring stroma cells contribute to the growth and invasion of the tumor [48]. Tumor cells release various signals that transform the surrounding microenvironment into a pathological entity, which undergoes continuous changes throughout the progression of cancer. This transformed TME is believed to influence abnormal tissue functions and significantly contribute to the development of resistance to treatment [49]. The TME is made up of Cancer Associated Fibroblast (CAF), which represents the highest number of cells in the TME, immune cells such as myeloid cells, mast cells, dendritic cells, and tumor-associated macrophages (TAM) [50]. CAF produces and releases factors such as hepatocyte growth factor (HGF), epidermal growth factor (EGF), insulin-like growth factors 1 and 2 (IGF1 and IGF2), fibroblast growth factor 2 and 7 (FGF2 and FGF7), and vascular endothelial growth factor (VEGF). These factors have significant effects on processes such as inflammation, invasion, immune evasion, and angiogenesis, all of which contribute to the promotion of tumor growth [51,52]. CAF is associated with poor prognosis and is an important marker for predicting remission in patients [53].
3.3. H. pylori and Colorectal Cancer
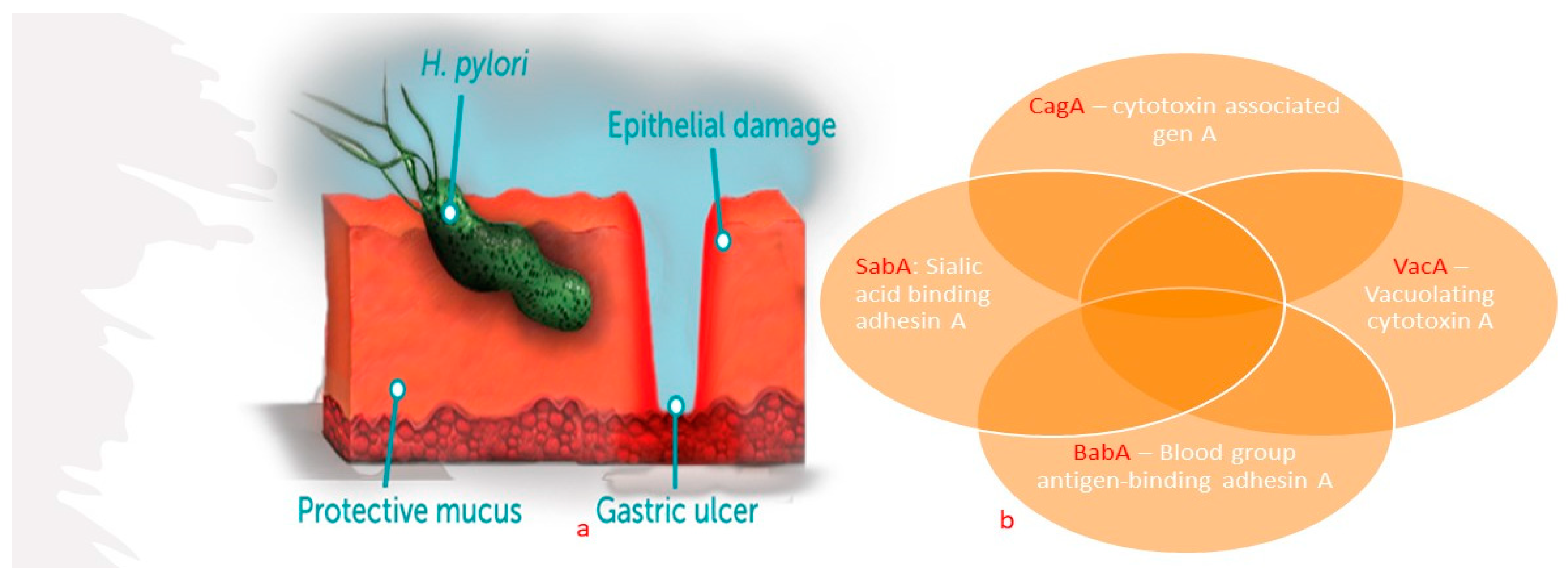
Discovered in 1982, Helicobacter pylori (H. pylori) has been characterized as a spiral-shaped microaerophilic Gram-negative bacillus [54,55]. Its global presence and putative modern and ancient migrations were mapped by Suerbauma and Achtmanb (2004) [56]. The spiral shape helps the cell traverse the sticky mucus lining to eventually lodge in the stomach muscle (Figure 7a), where it produces exotoxins that weaken the protective mucus layer of the stomach wall. Once established, H. pylori increases meal-stimulated gastrin levels, reduces gastric mucus production, and decreases duodenal mucosal bicarbonate secretion. All these mechanisms support its survival in the gastrointestinal tract, where it can live insidiously for many years.
Most carriers of H. pylori have been known to contract the organism in childhood, and it can last a lifetime if left untreated [55]. Its presence is often asymptomatic in the majority of people, and its symptoms are often masked by other git conditions. Major advances have been made in the diagnosis of H. pylori (Figure 8). Early manifestation of H. pylori pathogenicity includes acute or chronic gastritis or peptic ulceration. Zhao et al. [57] and Zuo et al. [58] reported an association between H. pylori infection and colorectal cancer from meta-analysis of the available literature and systematic reviews. The study by Zuo et al. [58] involved a systematic review and meta-analysis of the literature from forty-seven studies, comprising 12,146 cases of colorectal cancer and 55,811 control cases in populations from Asia, America, and Europe. It was concluded that H. pylori infection is modestly associated with a heightened risk of colorectal cancer.
Until very recently, the relationship between H. pylori infection and colorectal cancer continued to be the subject of conflicting reports [59,60,61] with divergent observations in different patient populations. Prevailing evidence strongly indicates that H. pylori infection poses a significant risk factor for the onset of colorectal cancer. Key virulence factors that heighten cancer development have been identified, including cytotoxin-associated gene A (CagA), sialic acid-binding adhesin A (SabA), blood group antigen-binding adhesin A (BabA), and vacuolating cytotoxin A (VacA) (Figure 7b) [55]. More recently, H. pylori has been recognized as a causative agent of gastric adenocarcinoma, mucosa-associated lymphoid tissue (MALT) lymphoma, and gastric non-Hodgkin’s lymphoma. In 1994, H. pylori was categorized by the World Health Organization (WHO) as a Class I Carcinogen [62,63], and in 2017, it was listed as a high priority drug-resistant bacterium [64,65].
Figure 8.
Diagnostic tests for H. pylori infection. Created with BioRender.com (A modification of original illustration by Cardos et al. [66]).
Figure 8.
Diagnostic tests for H. pylori infection. Created with BioRender.com (A modification of original illustration by Cardos et al. [66]).

4. Treatment of Colorectal Cancer
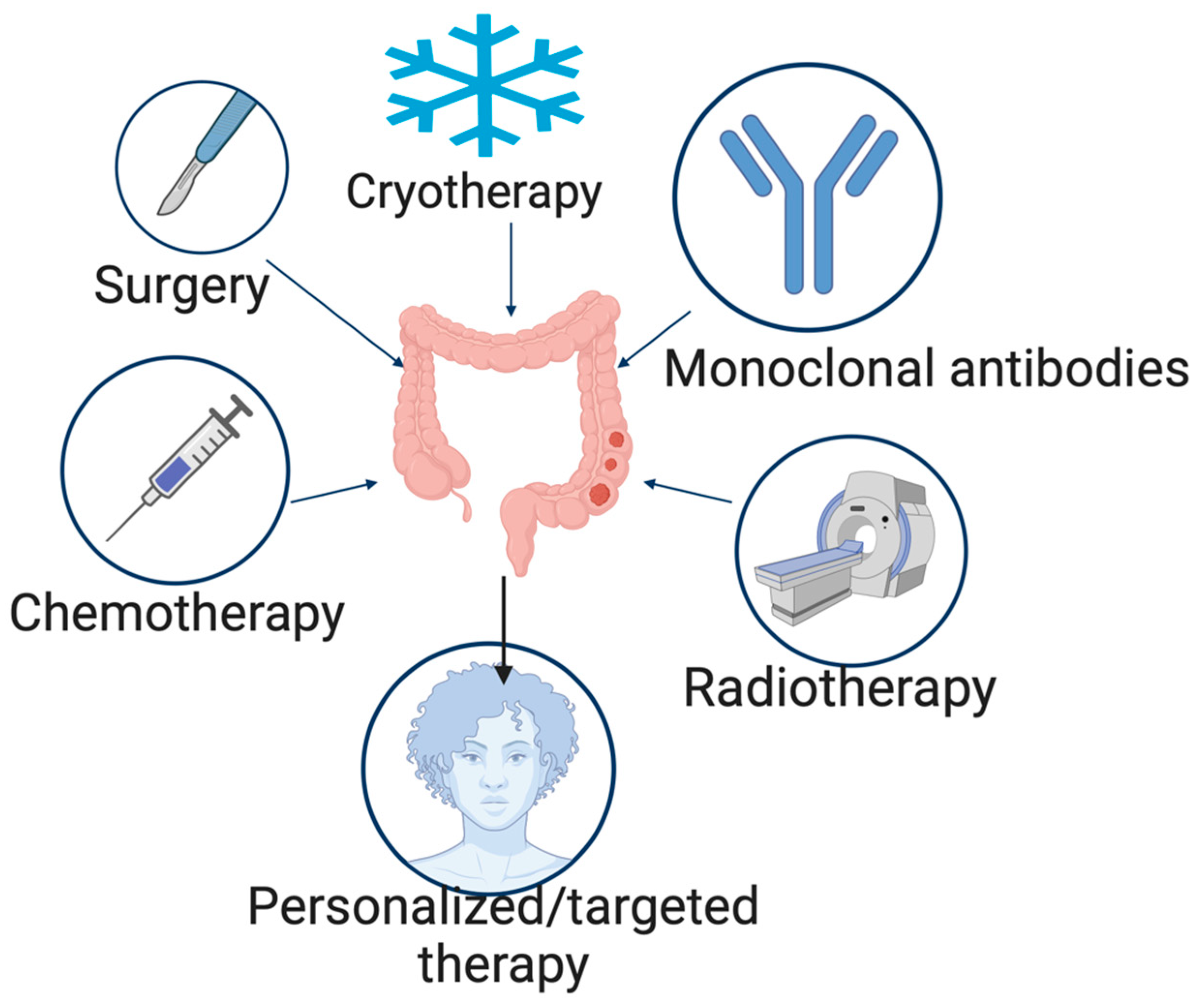
The treatment options for CRC include elimination of underlying infections, surgery, cryosurgery, chemotherapy, radiation therapy, and targeted therapy [67], with surgery being the main form of curative treatment and often supplemented with chemotherapy (Figure 9).
4.1. Surgery
Surgery is the major treatment for colorectal cancer, especially where liver metastasis has occurred, and can be carried out using either the open or laparoscopic surgery technique [68]. Before proceeding with surgery, it is important to accurately determine the characteristics and extent of the tumor. Whenever feasible, it is recommended to obtain histological confirmation of the diagnosis, which may involve performing a colonoscopy if needed. This allows for a more precise understanding of the nature of the tumor and the stage of the disease, guiding the subsequent surgical approach [69]. The surgery involves the removal of the tumor and its surrounding mesentery, followed by the establishment of a primary connection between the remaining healthy sections.
The specific scope of the surgical removal is determined by factors such as the tumor’s position and the blood supply it receives [70]. As promising as surgery looks in the treatment of colorectal cancer, there are a lot of complications that arise post-surgery. These complications include but are not limited to infections, thrombosis, adhesion and small bowel obstruction, ileus, anastomotic leakage, and colonic ischemia. Some of these complications arise because of the complexities involved in the tumor removal process, the length of time it takes to conclude the removal, and the presence of other comorbidities [71].
In recent times, there has been an increase in the utilization of robotic surgery, which is less invasive. Robotic procedures provide distinct benefits compared to laparoscopic surgery. They enable an immersive three-dimensional (3D) visualization that enhances depth perception, thanks to the utilization of advanced imaging technology. The robotic system incorporates articulating wrists, allowing for enhanced dexterity and precision during surgical maneuvers. Moreover, the system eliminates the natural tremor that a surgeon may have, further enhancing accuracy. These advantages enable surgeons to perform more intricate and precise movements, enabling the completion of complex procedures [72].
4.2. Cryotherapy
Cryotherapy emerged as an adjunctive therapy for low rectal cancer during the 1970s. This therapeutic approach relies on the Joule–Thomson effect, which involves the ablation of tumors using low temperatures. Cryotherapy works by subjecting the tumor to extreme cold, leading to the destruction of cancer cells. It is considered a technique for tumor ablation based on the application of controlled low temperatures. Cryotherapy has been extensively utilized in the treatment of various tumors, particularly in the prostate, kidney, liver, and other solid organs [73]. However, there is limited information available regarding the application of cryoablation in patients with rectal cancers. In recent times, cryoablation has been considered a significant approach for treating patients with rectal cancers. This treatment method offers several advantages, including the preservation of the anus and protection of anal function. Additionally, cryoablation is considered a minimally invasive surgical procedure with low anesthesia requirements [74]. Several factors, such as the tumor site, tumor size, tumor stage, and lymph node metastasis, can influence the effectiveness of cryotherapy [75].
4.3. Radiation Therapy
The tumor stroma plays a crucial role in supporting tumor growth through various mechanisms, such as immunosuppressive cytokine secretion and metabolic alterations. It provides a complex network of cellular activities, such as preventing the physical contact of T cells and cancer cells, thereby facilitating tumor proliferation [76]. However, recent advancements in localized treatment, particularly radiation therapy, have enabled strategies to effectively target and eliminate tumor stromal tissue. Radiation therapy has the capability to induce immunogenic cell death, leading to the release of tumor antigens and promoting immune cell trafficking. This provides radiation therapy a unique advantage in counteracting the immune evasion mechanisms orchestrated by stromal cells within the tumor microenvironment [77].
While radiation therapy is not typically recommended as a routine treatment for colon cancer patients, it may have a role in specific situations. Radiation therapy may be considered for patients with locally advanced diseases that cannot be completely removed by surgery or are unlikely to achieve complete removal. Additionally, in cases of local recurrence, radiation therapy may also be utilized as a treatment option. It is important to note that the decision to use radiation therapy in these scenarios would be made on a case-by-case basis, considering the individual patient’s condition and factors such as tumor location and extent [78].
Intraoperative radiation therapy (IORT) is a valuable technique for increasing the radiation dose in patients with locally advanced primary and recurrent rectal cancer. It is typically combined with preoperative external beam radiation therapy (EBRT) and the administration of 5-fluorouracil (5-FU) or capecitabine. For patients with locally advanced primary or recurrent disease that can be completely removed through surgery, the potential benefits of dose escalation using IORT should be evaluated in prospective studies. This approach holds promise for improving treatment outcomes in these specific patient populations [79].
4.4. Chemotherapy
Chemotherapy involves the use of various drugs or combinations of drugs to slow down the rate of growth of cancer cells. However, conventional chemotherapy for colorectal cancer often leads to off-target effects resulting in unwanted side effects such as neutropenia, anemia, hand–foot syndrome, diarrhea, gastrointestinal toxicity, mucositis, nausea, vomiting, fatigue, hematologic disorders, and liver toxicity [80]. These side effects and the development of drug resistance mean that treatment outcomes to date have not been entirely satisfactory [81].
Chemotherapeutic agents typically work by destroying rapidly dividing cells or altering their growth. They can be administered individually or in combination and may be delivered intravenously to reach cancer cells throughout the body or targeted to specific areas affected by cancer [82].
Different chemotherapeutic agents work via different mechanisms, such as interfering with cell division and reproduction, inhibiting the molecules and nutrients required for cancer cell growth, inducing cell death (apoptosis), blocking the formation of new blood vessels that supply a tumor, cutting off its nutrients and prevention of DNA or RNA formation by mimicking nucleotides, known as antimetabolites, which are most effective during the S phase of the cell cycle [83].
Chemotherapeutic agents used in the treatment of CRC include 5-fluorouracil, irinotecan, oxaliplatin, and leucovorin. 5-fluorouracil (5-FU) has been widely used as a first-line treatment for cancer for many years, and it is thought to be particularly effective against colorectal cancer [84]. However, it has several significant drawbacks, including a short half-life, poor absorption due to the enzyme dihydropyrimidine dehydrogenase, and nonselective action against healthy cells in the gastrointestinal tract and bone marrow [85]. Researchers have developed a methacrylic-based copolymer-coated version of 5-FU to overcome its limitations by exploiting its pH-sensitive properties and hydrogel matrix [86]. Eudragit® P-4135F and Eudragit® RS100 are used to create microspheres for 5-FU [87].
Irinotecan (IRT) is a potent chemotherapy drug that targets an enzyme called Topo 1, which is present in many types of cells [88]. The drug works by killing rapidly dividing cells, including cancer cells, but it also affects non-tumor cells, such as blood cells, epithelial cells, and commensal bacteria [89]. As a result, treatment with IRT often causes side effects such as neutropenia, diarrhea, and gastrointestinal toxicities such as mucositis and liver injury, particularly non-alcoholic steatohepatitis [90]. These side effects can vary greatly among individuals depending on the severity of their condition [91].
In some published phase II clinical trials, irinotecan has been found to be effective in treating advanced colorectal cancer that did not respond to treatment with 5-fluorouracil (5-FU). Response rates in these trials were between 13 and 27%. Both a weekly regimen for 4 weeks followed by a 2-week rest and a once-every-3-week schedule produced similar response and survival rates. A biweekly regimen produced similar response rates but with similar side effects, such as delayed diarrhea, neutropenia, nausea, and vomiting. High-dose loperamide can help with the most common side effect of diarrhea. Irinotecan has also been studied as a single agent in newly diagnosed CRC and has shown response rates between 19 and 32% and a median survival time of around 12 months, similar to 5-FU and leucovorin. Two phase III studies have shown that irinotecan treatment improves survival compared to 5-FU infusion and provides the best supportive care in patients with 5-FU-refractory CRC. Current studies are focusing on using irinotecan in combination with other chemotherapy drugs, in combination with radiation therapy, and as adjuvant therapy for locally advanced CRC [88,92]. A combination therapy containing 5-fluorouracil and leucovorin has also been used in the treatment of CRC.
Leucovorin has been shown to enhance the effectiveness of fluorouracil in laboratory studies by increasing the inhibition of an enzyme called thymidylate synthase. This was first reported in clinical studies by Machover in 1982 [93]. A meta-analysis of various studies also showed that a combination of fluorouracil and leucovorin improved both the response rate of tumors and overall survival in patients with metastatic colorectal cancer (mCRC) compared to using fluorouracil alone [94]. Ibrahim et al. [95], showed that the development and optimization of nanoparticles containing a combination of 5-fluorouracil (5-FU) and leucovorin (LV) led to improved interactions with colon and colorectal cancer cells in laboratory experiments. In the in vitro experiments, the colon-targeted nanosystem prevented drug release in the gastrointestinal regions and increased its release in the colorectal sites, thereby improving the anti-cancer activity of the drug combination. The authors proposed that this approach could help in lowering the administered dosages of the anti-cancer drugs and, at the same time, enhancing therapeutic efficacy while minimizing associated toxic side effects for patients.
4.5. Monoclonal Antibodies
The advanced knowledge of the molecular basis of cancer development has given rise to the discovery and development of drugs that target specific molecular biomarkers, such as monoclonal antibodies [96]. Monoclonal antibodies have gained wide popularity in the treatment of colorectal cancer. They are targeted agents that bind to ligands or the extracellular compartments of receptors. As a result of this binding, several signal transduction pathways necessary for the thriving of cancer cells are inhibited [97]. There are two classes of monoclonal antibodies approved by the FDA for the treatment of colorectal cancer; they are the vascular endothelial growth factor (VEGF) inhibitor, e.g., bevacizumab (Avastin®), and the epidermal growth factor receptor (EGFR) inhibitor, e.g., cetuximab (Erbitux®) and panitumumab (Verbitix®).
Bevacizumab is a humanized monoclonal antibody, and it acts by binding to VEGF, thus preventing it from binding to the VEGF receptor, thereby halting the signal transduction pathway that gives rise to angiogenesis, proliferation, and migration of cancer cells [98]. Cetuximab, which is a chimeric immunoglobulin antibody, and panitumumab, a fully human immunoglobulin antibody, both act by binding competitively to the extracellular domain of the EGFR, thus preventing the binding of EGF, which is known to play a significant role in angiogenesis and proliferation of cancer cells [99]. In addition to being an EGFR inhibitor, cetuximab has been shown to inhibit the production of pro-angiogenic factors such as VEGF. These groups of drugs have been evaluated in several clinical trials either as monotherapy, in combination with chemotherapy, or in combination with each other.
4.6. Side Effects and Complications of CRC Treatments
Classical chemotherapeutic agents for CRC treatment are fluoropyrimidines intravenous 5-fluorouracil (i.v. 5-FU) or oral capecitabine in various combinations and schedules. Constipation, diarrhea, dyspepsia, mucositis, nausea, and vomiting are the most common gastrointestinal (GIT) adverse events of these classical chemotherapeutic agents. Incidence and severity of adverse drug effects associated with these agents often vary with the drug and the therapeutic schedules, including dose, route of administration, frequency, co-administration of other agents, and overall duration of treatment [100]. GIT toxicities are the most concerning, and they tend to impact the patients’ compliance with therapeutic regimens. Infused regimens of 5-FU and leucovorin (LV) have shown less toxicity than bolus regimens and therefore preferred by patients. Previous efforts in the search for ideal 5-FU led to the discovery of floxuridine and tegafur, two typical 5-FU derivatives with enhanced pharmacokinetics and pharmacological profiles resulting in improved absorption, higher selectivity, and bioactivity, metabolic stability, and lower toxicity [101]. The emergence of multi-drug resistant cancer cells makes combination therapy, with agents that target different cancer progression pathways, the hallmark of cancer treatment. However, the potential for adverse drug events and toxicities increases with a number of components in a regimen. Most common combination therapies employ irinotecan and oxaliplatin with 5-fluorouracil and novel drugs targeting epidermal growth factor receptor (EGFR, such as cetuximab and panitumumab) or vascular endothelial growth factor (VEGF, such as bevacizumab, aflibercept, regorafenib, and ramucirumab) [100,102]
In a randomized clinical trial on primary CRC tumor resection plus chemotherapy versus chemotherapy (mFOLFOX6 plus bevacizumab or CapeOX plus bevacizumab) alone for patients with asymptomatic, synchronous unresectable metastasis by Kanemitsu et al. [103], adverse events for treatment discontinuation were based on the severity of the events, whether patient declined treatment, adverse effect delayed medication for more than 28 days, necessitated subsequent dose reduction after the second reduction, or if the patient declined treatment due to AEs [103]. Chemotherapy’s AEs may also be confounded by tumor-associated complications of intestinal obstruction, perforation, fistulation, or hemorrhage [103]. The classical PK difference across ages may have implications for dose titration or drug product selection. However, Kim [102] concluded that elderly patients with stage 3 colon cancer can be treated with adjuvant chemotherapy comprising 5-fluorouracil-leucovorin or 5-FU capecitabine without significant differences in toxicity from younger patients. Further, combination chemotherapy appears to be safe in older patients with metastatic CRC, except that for frail or vulnerable elderly patients, a stop-and-go strategy or monotherapy may be more appropriate.
5. Colon-Specific Drug Delivery Systems
Despite the availability of highly potent chemotherapeutic agents used to treat CRC, their low specificity and off-target cellular interaction often produce a range of dose-limiting side effects [23]. Thus, targeting CRC is essential. Most orally administered drugs are small molecules because the physiological barriers of the GIT do not support large molecular weight peptides and protein absorption [104,105]. Fortunately, the location of CRC posits it for passive targeting of cytotoxic agents via enteric coating to the colon. One major concern had always been physiologic, enzymatic, and GIT motility barriers to protein and peptide delivery via the enteron. The recent development of synthetic techniques for making small, modifiable, and stable peptide ligands for targeting drug molecules on the surface of CRC cells has created an incredible opportunity for colon-specific delivery of small, cytotoxic molecules that are conjugated to target ligands [26,106,107].
There is growing interest in the development of new drug delivery systems that can deliver drugs at a controlled rate and target specific sites of action. Conventional dosage forms, including extended-release forms, are limited in their ability to meet these goals [108]. Also, the diversity of cancer cells and the intricate mechanisms involved in tumor development have made current chemotherapy treatments for colorectal cancer ineffective. The current therapies usually involve high doses of toxic drugs, which cause severe side effects and make patients discontinue therapy [109]. Therefore, it is crucial to develop targeted drug delivery methods that are more effective in fighting tumors and less harmful to the patient [110]. Colon-specific drug delivery systems are promising and have shown to be effective for directing treatment to the site of disease, reducing the dosage, and minimizing systemic effects [111]. Formulations for colonic delivery are also ideal for administering drugs that are polar, easily degraded chemically or enzymatically in the upper gastrointestinal tract, or are heavily metabolized by the liver, such as therapeutic proteins and peptides [110].
However, progress in this area has been hindered by instability in physiologic fluids, low specificity of targeting, and off-target cellular interaction with associated dose-limiting side effects.
5.1. Approaches for Colon-Specific Drug Delivery
5.1.1. PH Approach
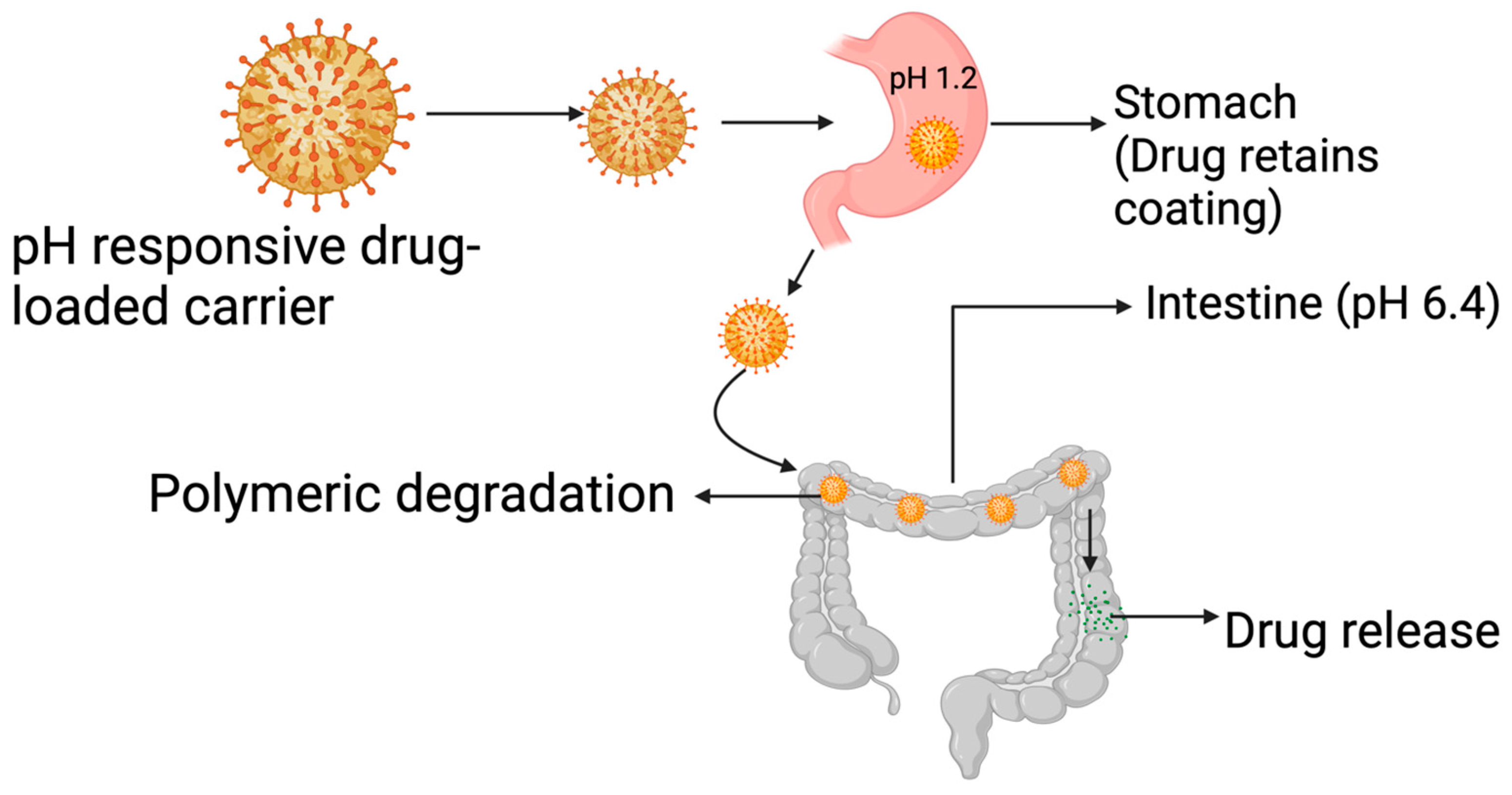
The pH approach to CRC drug delivery is illustrated in Figure 10. This approach takes advantage of the pH gradient present in the gastrointestinal tract, which becomes more alkaline as it moves from the stomach (pH 1.5–3.5) and small intestine (5.5–6.8) to the colon (6.4–7.0) [112]. By using polymers that dissolve at different pH levels and understanding their properties, drug delivery systems can be created to target specific areas [113]. pH-sensitive polymers such as cellulose acetate phthalates (CAP), hydroxypropyl methyl-cellulose phthalate (HPMCP) 50 and 55, and copolymers of methacrylic acid and methyl methacrylate, such as Eudragit® S 100, and Eudragit® L, have been widely used [114]. The most used pH-sensitive polymers are the copolymers of methacrylic acid and methyl methacrylate, especially Eudragit, because they have the added advantage of being mucoadhesive [115,116]. The broad usage of polymers in drug delivery has been due to their exceptional properties that have yet to be matched by any other material [117].
Using pH-sensitive polymers of methyl methacrylic acid, known as Eudragit R and S100, as a targeting technique for the colon is an effective method. This is because these polymers have a dissolution starting point that is like the pH of the colon, and they also have a number of benefits, such as reducing the impact of pH and decreasing the risk of high-dose dumping. Additionally, these polymers can improve the uptake and bioavailability of acid-labile drugs that are difficult to dissolve. Eudragit S100 specifically is known to inhibit drug release in the terminal ileum and increase the selective release of drugs in the colon [118,119].
Prajakta et al. [120] designed a pH-sensitive curcumin-loaded Eudragit S100 polymer for drug delivery to an HT-29 colorectal cancer cell line and observed a 2-fold inhibition of the cancer cells when compared to the use of curcumin as a free drug. The authors attributed the improved activity to improved cellular uptake of the drug-loaded polymer by the cancer cells. As promising as the pH approach may appear, a major setback has been the intraindividual variation in the GIT pH values and the lower colonic pH levels in individuals suffering from ulcerative colitis and Chron’s Disease [121]. Aside from the use of polymers, hydrogels have also been investigated for use in pH-specific colon drug delivery. In a study, Liu et al. [122] synthesized and characterized a novel pH-sensitive semi-interpenetrating polymer network (semi-IPN) hydrogels based on starch and poly-aspartic acid (PAsp). The 5-FU-loaded hydrogels had excellent drug release properties attributed to the hydrogels’ pH-sensitive properties, which posits them for application in the drug delivery platform for colon cancer management [122]. Stimuli-response hydrogels, carbon nano-onions, and functionalized carbon nano-onions designed for pH-triggered drug delivery [123,124,125] also hold great potential for facilitating targeted delivery of drugs to CRC cells.
5.1.2. Microbiota-Based Drug Delivery
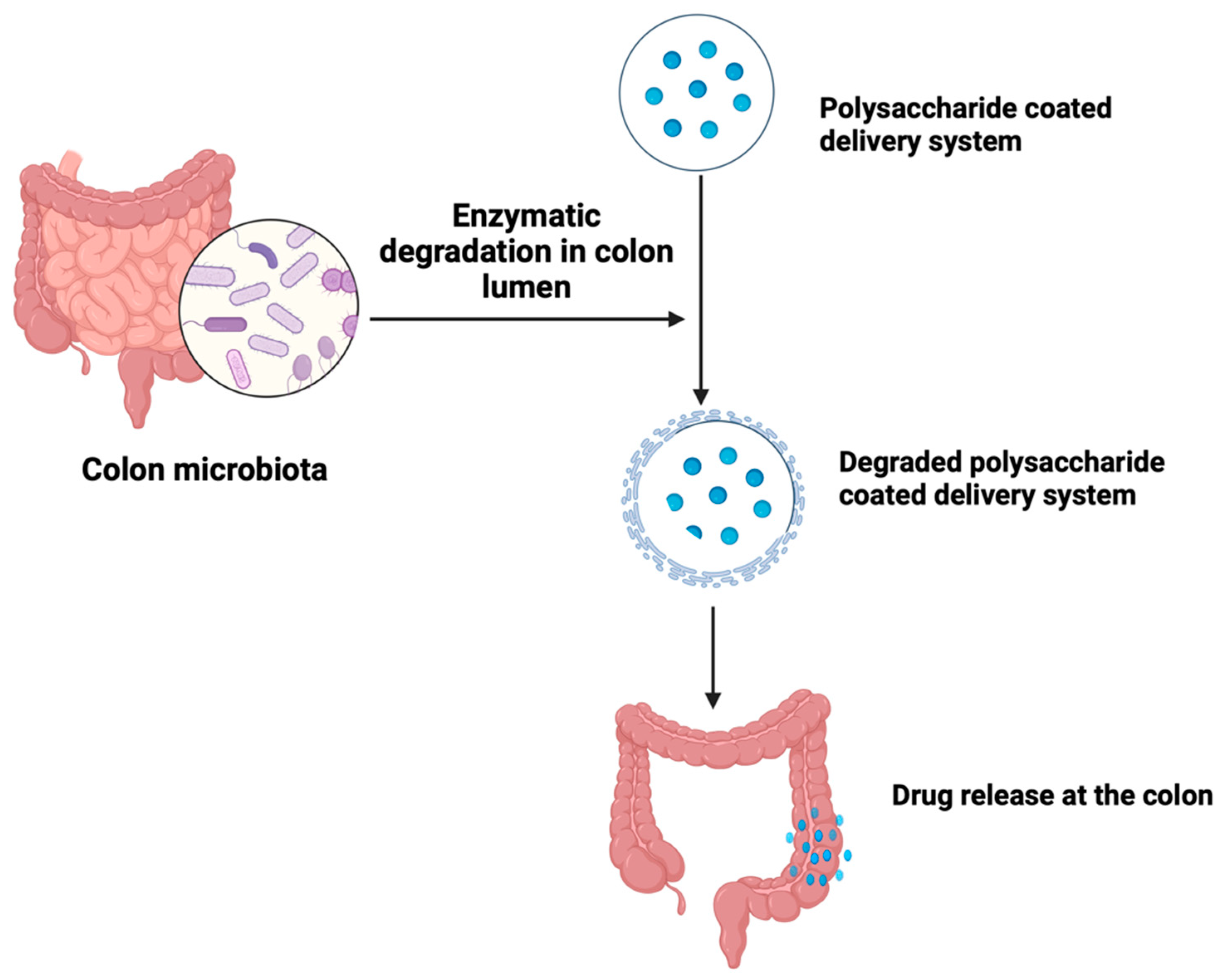
The human body is inhabited by a diverse range of microorganisms, including bacteria, archaea, viruses, fungi, protozoa, and helminths, collectively known as the human microbiota. These microorganisms are increasingly recognized as significant factors in human health and disease causation [126]. The colon harbors more than 400 variety of microorganisms, including aerobic species such as Escherichia coli and anaerobic species such as Clostridium spp. These bacteria possess multiple metabolizing enzymes that are both hydrolytic and reductive in nature [112]. Microbiota-activated delivery systems have been identified as a potential solution for colon-targeted drug delivery. It is a well-explored approach based on the ability of specific enzymes of colonic bacteria to degrade xenobiotics, polysaccharides, and polymers (Figure 11). Colonic bacteria enzymes such as azoreductases, glucuronidase, glycosidases, esterases, and amidases are responsible for the breakdown of drug-loaded polymers and polysaccharides.
Polysaccharides, such as pectin, guar gum, inulin, and chitosan, are utilized due to their ability to remain intact in the upper gastrointestinal tract while being susceptible to degradation by colonic microflora, thereby releasing the loaded drug [119]. The properties of the polysaccharides, such as drug release rate, stability, and mucoadhesion, can be enhanced by structural modification of the polysaccharides [127]. Mucoadhesion is particularly important because it promotes drug uptake by ensuring prolonged contact between the drug delivery system and the mucosal surface [128]. The use of combinations of polysaccharides also offers more advantages in terms of drug delivery rate. Zhu et al. [129] designed a colon-targeted drug delivery system utilizing a combination of 2 polysaccharides, porous starch, pectin, and chitosan. The drug, doxorubicin, was first loaded on the porous starch, which was then coated with pectin and chitosan solution. The result showed a 4-fold increase in the drug release rate from the porous starch–pectin–chitosan–doxorubicin combination when compared to pectin-doxorubicin.
Advantages of these polysaccharides include the presence of numerous modifiable functional groups, large-scale availability, relatively low cost, low toxicity and immunogenicity, high biocompatibility, and biodegradability [130,131]. Despite the beneficial attributes of polysaccharides in microbiota-based delivery, some drawbacks have limited its use, including a broad range of molecular weight due to the varying chemistry of polysaccharides [132], low solubility in a wide range of organic solvents and excessive aqueous solubility which leads to early drug release in the upper GI tract [133]. To address these challenges, especially that of premature release in the upper GI tract, polysaccharides-based systems can be formulated by combining polysaccharides with other polymers. For instance, water-insoluble polymers such as Eudragit RS and ethyl cellulose can be used in combination with different polysaccharides to achieve colon-specific drug delivery.
Although the rate and extent of drug release in polysaccharide-based microbiota-triggered systems is appropriate in terms of colon specificity, factors such as changes in microbiota due to disease conditions, enzymatic secretions, gut infections, and dietary habits cannot ensure the precise degradation of microbiota-triggered delivery systems and, as such, may not produce consistent and reliable and predictable drug delivery pattern [134].
5.1.3. Drug Conjugates
To treat colonic diseases with fewer toxic side effects, scientists are exploring drug conjugates that target specific receptors at disease sites through interaction between ligands on the carrier and expressed molecules on receptors [135]. Drug conjugates are compounds resulting from the chemical linkage between a drug and another molecule or compound.
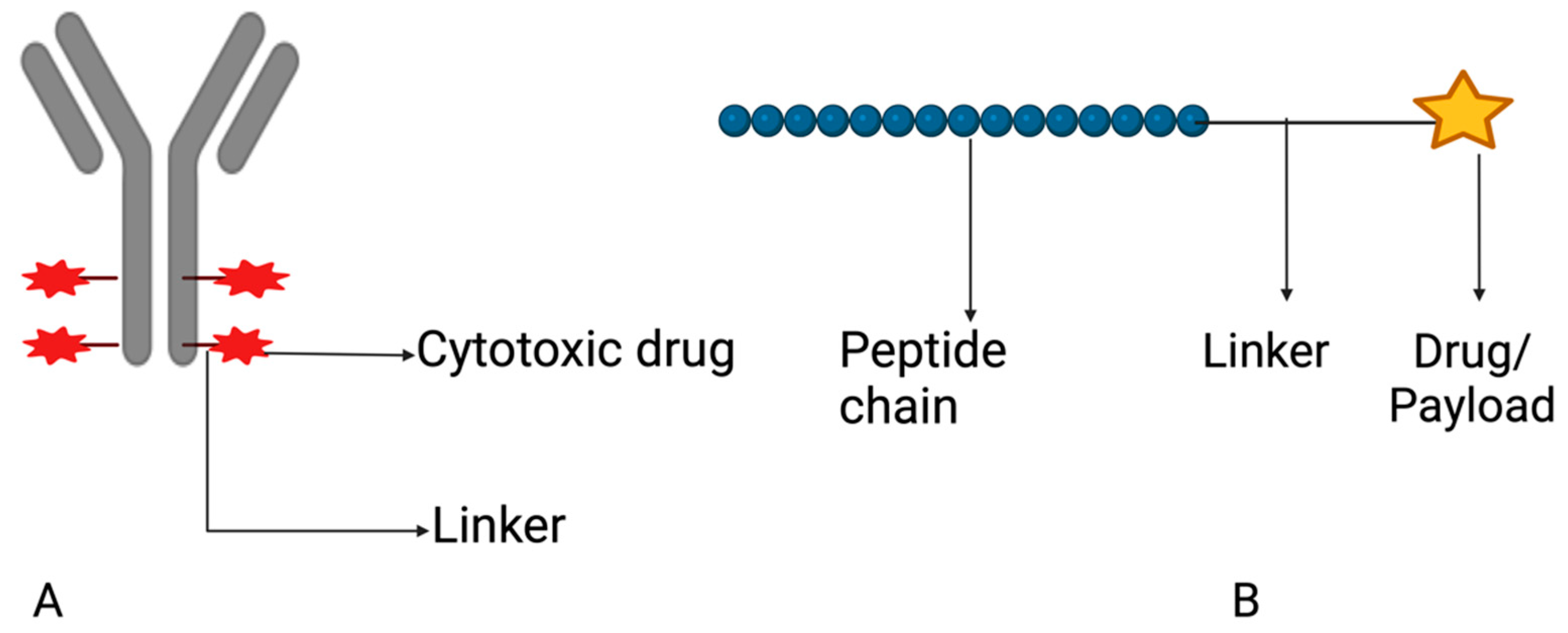
This coupling aims to amplify the therapeutic impact, augment selectivity, or enhance the pharmacokinetic characteristics of the drug (Alas et al., 2020) [136]. Different ligands, such as antibodies, peptides, folic acid, and hyaluronic acid, can be chosen based on their interaction with certain molecules that are expressed on receptors (Figure 12). Table 1 highlights several receptors that have been targeted in the delivery of drug conjugates for the treatment of colorectal cancer. Candelaria et al. (2021) [137] discussed the potential for transferrin receptor 1 (TfR1) targeting as direct anticancer agents. Since rapidly dividing cancer cells require an abundance of iron intake, TfR1, a type II transmembrane glycoprotein, is usually overexpressed in cancer cells. Thus, designing antibodies that could directly disrupt the TfR1-dependent cellular supply of iron or antibody–drug (oncology) conjugate that can be internalized by TfR1 receptor-mediated endocytosis are promising mechanisms for CRC treatment. Drug conjugate systems can also be combined with pH-sensitive systems for improved stability and specificity in the gastrointestinal tract (Tesauro et al., 2019) [138].
Peptides have attracted significant attention as possible ligands for targeted drug delivery due to their biocompatibility, cost-effectiveness, chemical diversity, and responsiveness to stimuli (Ghosh et al., 2018, Jiang et al., 2019) [139,140]. Due to their large binding interfaces with receptors, peptide ligands also have higher binding affinity and specificity than small molecule ligands. They are easily accessible through high-throughput screening and can be synthesized using automated devices, and any observed instability can be addressed by modifying the peptide sequences (Al-azzawi et al., 2019, Ren et al., 2016) [141,142]. Peptide-conjugated drug delivery systems are particularly promising for tumor-targeted delivery. For example, the TK peptide (TWYKIAFQRNRK) has a high affinity for integrin, which is upregulated in colon cancer cells and was conjugated to doxorubicin-loaded micelles for colon-specific delivery. The TK-conjugated micelles showed improved cytotoxicity and penetration in tumor spheroids, making TK a promising targeting ligand for colon-targeted therapy (Guo et al., 2019) [143]. Table 2 Illustrates examples of experimental drug conjugates in clinical trial.
Top-of-form nanoparticles specifically designed for the colon were modified with both amphipathic chitosan derivatives (ACS) and cell-penetrating peptides (CPP) to enhance the oral effectiveness of insulin. The ACS modification protects the CPP from degradation in the upper gastrointestinal tract and ensures colon-specific drug delivery. Once the nanoparticles reach the colon, the ACS on their surface degrades, and the exposed CPP allows for the drug to penetrate the colonic epithelium. In vitro and in vivo evaluations indicate that these ACS-CPP nanoparticles may be a promising method for improving the oral absorption of proteins and peptides in a colon-specific manner (Langel, 2019) [144].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Molecular targets and their ligands in colorectal cancer.
| Targets | Ligands | References |
|---|---|---|
| Carcinoembryonic antigen | Antibody | Tiernan et al., 2013 [145] |
| Folate receptor alpha (FRα) | Folic acid | Noe et al., 2022 [146] |
| Human epidermal growth factor 2 (HER-2) | Peptide | Suwaidan et al., 2022 [147] |
| Hyaluronic acid receptor | Hyaluronic acid | Mansoori et al., 2020 [148] |
| CD44 receptor | Hyaluronic acid | Tabasi et al., 2021 [149] |
Table 2.
Drug conjugates in clinical trial.
| Drug Conjugate | Target | Phase of Study | Clinical Trial Identifier | Sponsor |
|---|---|---|---|---|
| Disitamab vedotin and Tisleizumab | HER-2 | II | NCT05493683 | The First Affiliated Hospital with Nanjing Medical University (Nanjing, China) |
| M9140 | Carcinoembryonic antigen | I | NCT05464030 | EMD Serono Research & Development Institute, Inc. (Darmstadt, Germany) |
| CBP-1019 | Unknown | I, II | NCT05830097 | Coherent Biopharma (Hefei) Co., Ltd. (Hefei, China) |
| BDC-1001 (Nivolumab) | HER-2 | I, II | NCT04278144 | Bolt Biotherapeutics Inc. (Redwood City, CA, USA) |
| ELU001 | (FRα) | I, II | NCT05001282 | Elucida Oncology (Monmouth Junction, NJ, USA) |
| Datopotamab deruxtecan | Unknown | II | NCT05489211 | AstraZeneca (Minato City, Janpan) |
| SBT6050 (Cemiplimab) | HER-2 | I, IB | NCT04460456 | Silverback Therapeutics (Seattle, WA, USA) |
| TORL-3-600 | Unknown | I | NCT05948826 | TORL Biotherapeutics, LLC (Albuquerque, NM, USA) |
5.1.4. Vesicular Systems
Vesicular systems are a popular method for targeted delivery and improved outcomes. They are nanocarriers and have gained wide popularity due to their benefits, such as extending the half-life of drugs and evading uptake by reticuloendothelial systems (RES) (Kadam et al., 2012) [150]. Lipid-based vesicles have a wide range of uses in fields such as immunology, membrane biology, diagnostics, and genetic engineering. They can be used to model biological membranes and to transport and target active pharmaceutical ingredients (API) (Barani et al., 2020, Bagheri et al., 2014) [151,152]. A list of vesicular systems for drug delivery to colorectal cancer currently in clinical trial is shown in Table 3.
Liposomes
Liposomes are colloidal, spherical structures that form through the self-assembly of amphiphilic lipid molecules in a solution, such as phospholipids (Sebaaly et al., 2016) [153]. Liposomes have a size range of 30 nm to the micrometer scale, and their phospholipid bilayer is typically 4–5 nm thick. The liposomal membrane can consist of one or more lipid bilayers arranged around an internal aqueous core. The polar head groups are oriented towards both the inner and outer aqueous phases. This organized structure provides liposomes with a unique ability to load and transport molecules with various solubilities, such as hydrophilic molecules within the internal aqueous core, hydrophobic molecules within the lipid bilayer, and amphiphilic molecules at the interface between the water and lipid bilayer (Laouini et al., 2012) [154].
Liposomes have been used as a drug delivery carrier in a variety of disease conditions, especially cancer. There are several FDA-approved liposomes-based anticancer drugs, such as Doxil® (doxorubicin hydrochloride) used in the treatment of ovarian cancer and myeloid melanoma, Marqibo® (Vincristine sulfate) used in the treatment of leukemia and Onivyde® (irinotecan hydrochloride) used in the treatment of pancreatic adenocarcinoma (Liu et al., 2022) [155]. Liposomes are excellent drug carriers due to their remarkable properties, including the ability to shield the loaded drug from physiological degradation, prolong the drug’s half-life, and regulate of drug release rate (Niu et al., 2012, Wang et al., 2009) [156,157] and the ability to deliver chemotherapeutic agents to their site of action by active or passive targeting (Alavi, 2019) [158]. In colon-specific drug delivery, liposomes have been used as carriers to deliver the payload to tumor cells in the colon and to improve the efficacy and reduce side effects of existing chemotherapeutic agents, but most of the formulations are still in the experimental stage.
Khuntawee et al., 2021 [159] encapsulated cordycepin, a colon cancer drug candidate in liposomes, with the aim of overcoming the limitations of cordycepin, including poor stability and low water solubility. In vitro studies show that liposomal cordycepin inhibited the growth of the HT-29 colorectal cancer cell line, inducing apoptosis at a rate that was 2-fold greater than what was observed with free cordycepin. Xiong et al., 2017 [160] designed a mannosylated liposome loaded with paclitaxel for active targeting to mannose receptors, which are highly expressed in CT26 colon cancer cell lines. The result showed that there was increased cellular uptake of the mannosylated liposomes, and no toxicity or side effect was observed.
Niosomes
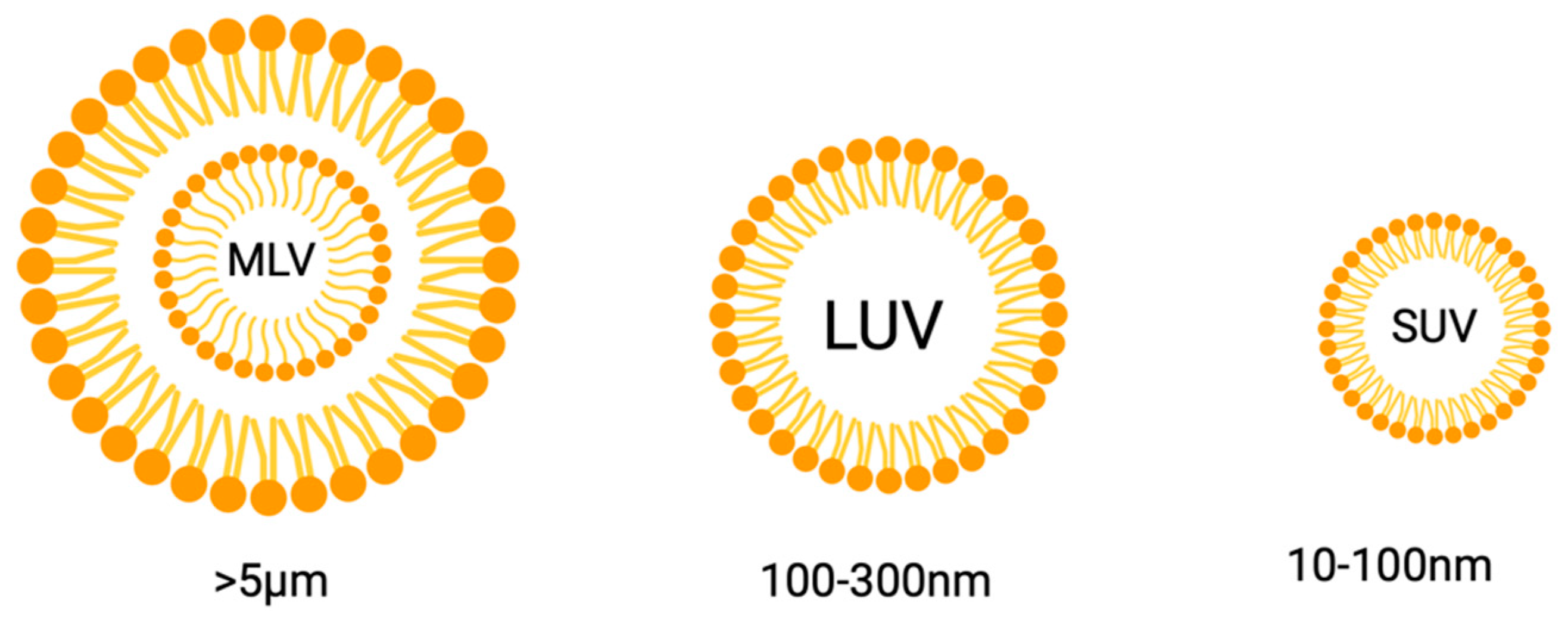
Nonionic surfactant vesicles (niosomes) are bilayer structures formed from the self-assembly of nonionic surfactants in an aqueous medium that requires external energy or heat to make the system stable (Yasamineh et al., 2022) [161]. The use was first reported in the cosmetic industries in the 1970s but has now gained wide popularity as an effective carrier for drugs to specific sites of action (Bagheri et al., 2014) [152]. Being bilayer vesicles, they are divided into unilamellar and multilamellar vesicles (Marianecci et al., 2014) [162]. Typically, niosomes fall within the sub-micron (colloidal) size range. Small unilamellar vesicles (SUVs) have particle sizes ranging from approximately 10 to 100 nm, while large unilamellar vesicles (LUVs) have sizes ranging from 100 to 3000 nm. Multi-lamellar vesicles (MLVs) are larger than 5 µm, and there have been a few reports of “giant” vesicles (>15 µm) as well (Figure 13) (Moghasemmi et al., 2014, Varshosaz et al., 2014) [163,164].
Niosomes are comparable to liposomes, but while liposomes contain phospholipids, niosomes are made from non-ionic surfactants like tweens and spans. Like other vesicular drug delivery systems, niosomes can entrap both hydrophilic and lipophilic drugs in either the aqueous layer or the lipid bilayer (Srinivas et al., 2010, Shakya et al., 2014) [165,166]. Niosomes are excellent drug carriers. Their advantage over other vesicular drug delivery systems includes ease of preparation, the ability to encapsulate a wide range of chemotherapeutic agents (Chen et al., 2019) [167], no need for covalent bonding of encapsulated payload, greater stability, and the ability to evade sequestration by the reticular endothelial systems and prolong circulation half-life (Witika et al., 2022) [168]. In terms of clearance, liposomes are more rapidly phagocytosed by cells of the RES and macrophages (El-Ridy et al., 2012) [169].
Several methods have been devised for niosomes preparation. Available methods of preparation include thin-film hydration (TFH), reverse-phase evaporation (RPE), evaporation/sonication (EVP/SON), and the ether injection method (EIM) (Umbarkar, 2021) [170]. The method used can have profound effects on the physicochemical properties of prepared niosomes. Ugorji et al., 2022 [171], prepared 5FU-loaded niosomes with either Tween 80 or Span 60 using the four methods mentioned above. The result showed that the TFH method produced the noisome with the smallest particle size (187 nm), while the EVP/SON produced the largest noisome with a particle size of 4476 nm. The particle size, polydispersity index, entrapment efficiency, and physical stability of the vesicles were influenced by the techniques used in their preparation. The thin-film hydration process produced smaller particle sizes and higher entrapment efficiency of 5FU than the other methods.
To evaluate the efficacy of 5FU-loaded noisome in colon cancer cell lines, Ugorji et al. (2022) [171] conducted a real-time cell assay, which is an in vitro cytotoxicity test against HCT-11 colon cancer cell lines. The result showed that compared to the pure drug and empty niosomes, the real-time cell assay indicated that the niosomes loaded with 5-fluorouracil induced more long-lasting cell death. Also, El-far et al., 2022 [172], designed oxaliplatin and paclitaxel-loaded noisome in a bid to assess the efficacy of the drug combination in HT-29 colorectal cancer cell lines. The result showed that as a distinctive nano micellar system, niosomes loaded with drugs can improve cellular absorption of drugs, leading to increased cytotoxicity and apoptosis of the cells. The drug-loaded noisome exhibited improved bioavailability and can be deemed as a promising alternative delivery system for these two anticancer drugs in the treatment of colorectal cancer.
Polymeric Nanoparticles
To surmount the associated challenges of poor specificities in most chemotherapeutic agents’ challenges, various substances such as polymeric nanoparticles and materials based on organometallic compounds and carbon have been employed as carrier systems for colorectal cancer treatment (Zhu et al., 2019; Rashmi et al., 2015) [129,173]. The emergence of nanotechnology has provided significant progress in the delivery of drugs to cancer cells. Although only a limited number of drugs in nanocarriers have made it through for clinical use, it is anticipated that nanocarriers will be a major delivery system to obtain the breakthrough formulation for the diagnosis and treatment of colorectal cancer in the foreseeable future.
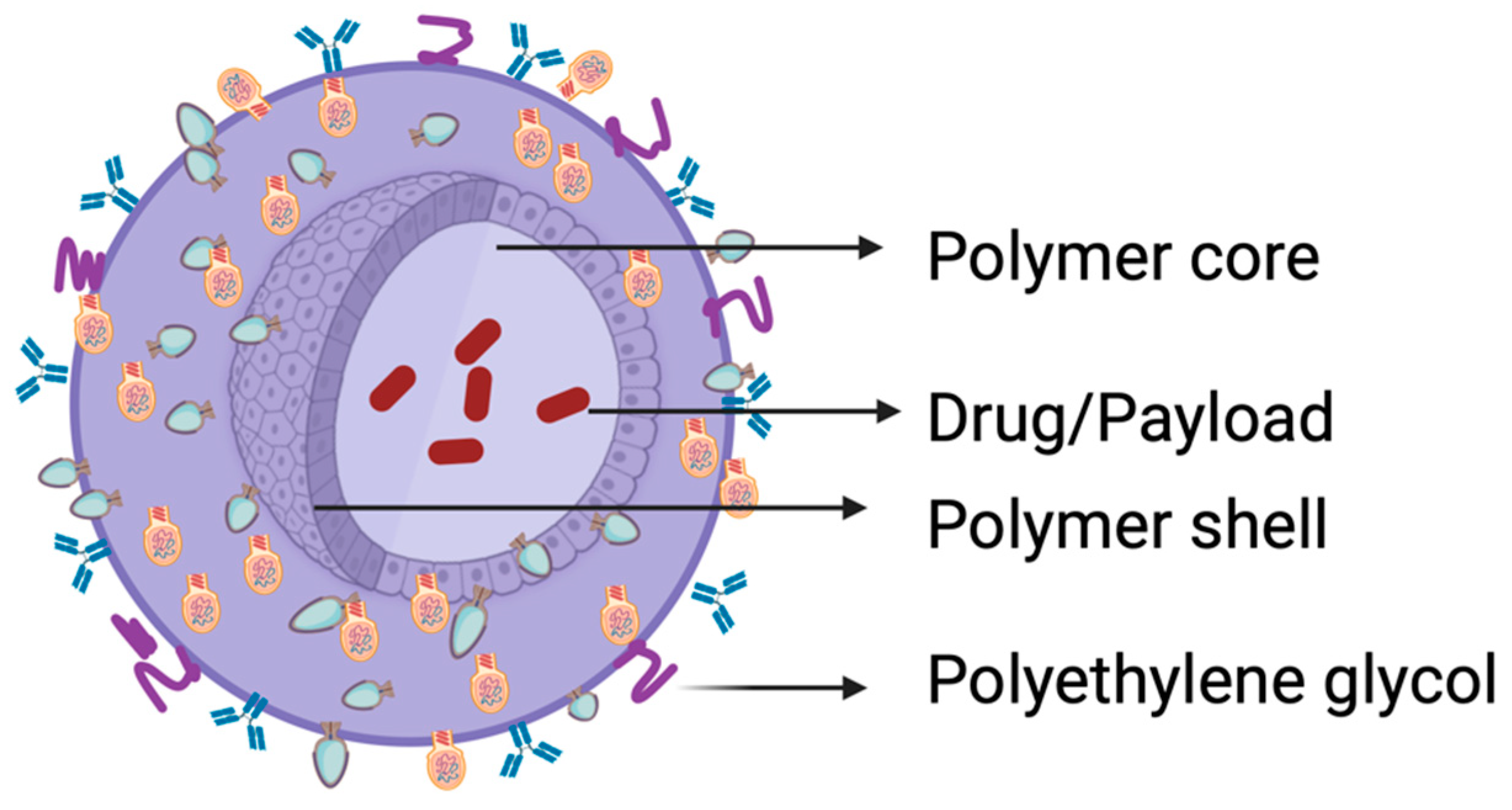
Polymeric nanoparticles provide the opportunity to encapsulate drugs with varying properties, protect the drugs from degrading enzymes, and possess numerous other benefits compared to larger molecular-weight drugs. Moreover, modifying their surface with targeting molecules enhances their adeptness in navigating the in vivo surroundings and prolongs the controlled discharge of the payload. Considering that conventional nanoparticles (NPs) can easily be taken up by cells of the RES, strategies such as surface modification of the nanocarriers have been employed to slow down or prevent RES sequestration on NPs. This is achieved by coating the surface of the nanocarrier with a hydrophilic polymer such as polyethylene glycol (PEG), which protects the surface charge of the nanocarrier (Figure 14), thus making it unrecognizable to the RES (Lampretch, 2015) [174]. The optimal size of nanoparticles is typically within the range of 10 nm–200 nm; this size and their stealth property (due to coating with PEG) confers on them the ability to intravasate the leaky vasculature of cancer cells through the enhanced permeability and retention (EPR) effect (Greish, 2010; Ejigah et al., 2022) [175,176]. More recently, stimuli-responsive nanoparticles (nano-onions) comprising poly 4-hydroxyphenyl methacrylate–carbon nanoparticles embedding γ-cyclodextrin, gelatin methacrylate or bovine serum albumin nanocomposite fibers were designed by Mamidi et al. (2020, 2021a,b) [123,124,125]. Ionic gelation, primed layer-by-layer self-assembly, and Forcespinning® technology were used as construction techniques. Controlled, pH-responsive release of model drugs (e.g., diclofenac, doxorubicin) was achieved.
Numerous polymers, including poly(lactide-co-glycolide) (PLGA), polylactide (PLA), polycaprolactone (PCL), poly(D,L-lactide), chitosan, and PLGA–polyethylene glycol (PEG), have been used to formulate nanocarriers to facilitate targeted delivery of chemotherapeutic agents to cancer cells. Among these, PLGA stands out as a highly suitable biodegradable polymer for drug delivery and biomaterial applications. This is attributed to its capability to undergo hydrolysis within the body, resulting in the formation of metabolite monomers—lactic acid and glycolic acid. As these monomers are naturally occurring and efficiently metabolized by the body, employing PLGA for medical purposes carries minimal risk of systemic toxicity (Prabhu et al., 2015) [173].
6. Prospects: Individualized Therapy and Drugs in Clinical Trials
The occurrence of colorectal cancer continues to increase, especially in young adults. The disease burden is higher in developing countries with no proper diagnostic techniques and equipment. Though there are currently available therapies, most of them come with various challenges, such as toxicity and severe complications. The outlook for effective treatment of colorectal cancer will be to individualize treatment, such that each patient is treated based on the peculiarities of their situation. Prognostic and predictive markers such as KRAS AND MSI can be used as the starting point for developing effective therapies. These new therapies can then be tested in clinical trials, even though only a few patients may qualify to participate.
Also, the combination of chemotherapeutic agents and monoclonal antibodies should be tested for their prospect in treating colon cancer. An example of such a combination was tested in a phase 3 randomized clinical trial by Tabernero et al., 2021 [177]. The study, with the clinical trial number NCT04737187, was tagged “SUNLIGHT”. It is a follow-up/confirmatory test on a previous study that reported the efficacy of the combination therapy, Trifluridine/tipiracil (FTD/TPI), and the monoclonal antibody, Bevacizumab (Bev) carried out by Prager et al. (2023) [178]. Study participants were randomized into two groups, with the first group receiving FTD/TPI+BEV while the other group received FTD/TPI. The primary outcome was overall survival, and the result showed that the combination of FTD/TPI and BEV produced an improvement in the overall survival, and the result was statistically significant when compared to the group that took FTD/TPI alone.
To compare the activity of FTD/TPI+BEV with the already approved fluoropyrimidine-irinotecan+ BEV, Kuboki et al. (2023) [179] conducted a randomized noninferiority trial. The experimental group received FTD/TPI+BEV, while the control group received fluoropyrimidine-irinoteacn+ BEV. The result showed that even though FTD/TPI+BEV did not demonstrate noninferiority over the control, the patients’ quality of life improved compared to the control. The result also showed that the combination could be a substitute for irinotecan-containing combination drugs, especially in patients who cannot tolerate irinotecan due to associated nonhematologic adverse effects. Thus, there is a prospect for improved efficacy and overall survival in the use of chemotherapeutic agents and monoclonal antibodies and should, therefore, be explored more.
Inhibitors of the vascular endothelial growth factor receptors (VEGFR), such as fruquitinib, are also being investigated, especially for colorectal cancers that have proven resistant to available chemotherapy. Dasari et al., 2023 [180], conducted a multi-centered randomized, double-blind phase 3 clinical trial tagged FRESCO 2 to examine the effectiveness of fruquitinib, which is a very potent and highly selective VEGFR inhibitor. The result showed that fruquitinib produced a significant overall survival in the patients when compared to the placebo, indicating that fruquitinib can be considered a treatment option for patients with refractory colorectal cancer. The analysis of the quality-of-life data is currently ongoing, and it is expected to further reinforce the clinical advantage of fruquitinib.
7. Impact of Circadian Rhythm on CRD Drug Delivery and Efficacy
Circadian clocks (CC), arising from the suprachiasmatic nucleus (SCN) and peripheral clocks, have been recognized in biological organisms for over three decades. CC serves as an adaptive method for organisms to respond to changes in their natural environment. Day and night alternations culminating in environmental light or other stimuli follow the laws of nature and induce the SCN to recognize the environmental changes and release signals to specific pathways for the activation of subordinate clocks that would produce corresponding adjustments to the 24 h period cycle (Shafi et al., 2019; Kinouchi and Sassone-Corsi, 2020) [181,182]. Recent studies suggest the potential regulatory effects of circadian clocks in various physiological processes that impact human health (Zhou et al., 2021) [183], including CRC.
An earlier study involving meta-analysis of individual data from three international phase III trials compared the outcome of chronomodulated therapies of 5-fluorouracil, leucovorin, and oxaliplatin administered in chronomodulated (chronoFLO) against conventional (CONV) infusions. A hazard ratio of 1.59 (1.30 to 1.75) for overall survival (p = 0.002) indicated that males lived significantly longer on chronomodulated chemotherapy than on conventional chemotherapy. Also, the sex versus schedule interaction effect provided a strong predictive factor for optimal treatment schedules. On the contrary, a systematic review and meta-analysis of data from six randomized controlled trials involving 1347 patients on chronomodulated chemotherapies generally did not show any advantages over conventional therapies with regard to overall survival, objective response rate, or toxicity (Brenner et al., 2014; Huang et al., 2016) [4,184]. Other recent studies have confirmed these observations but found a reduction in hematologic toxicity in the chronomodulated therapy group (Nassar et al., 2023) [185]. Kinouchi and Sassone-Corsi (2020) [182] concluded that an information gap still exists regarding the existence of a common core clock connection between cancer and pluripotent stem cells that may elucidate the impact of the circadian clock on critical stages of cellular differentiation. Despite the promising potential of chronomodulated administration of chemotherapeutics agents for optimizing treatment outcomes, this modality has not been widely implemented in many clinical situations.
8. Conclusions
As the scourge of colorectal cancer continues to ravage the human population, greater attention is being paid to its management, particularly due to recent changes in patient demography: CRC affects more people between the ages of 40 and 50, the productive capacity of most economies in many countries. The disease burden is more pronounced in underdeveloped countries with a lack of access to up-to-date equipment for early detection and diagnosis and inadequate clinical facilities for patient treatment. Although it is regarded as a lifestyle disease whose incidence is significantly impacted by a Westernized diet and sedentary way of life, a recent analysis of its social demographic context has shown more impact of its burden on low and medium SDI countries. While several treatment options exist for colorectal cancer, surgery and chemotherapy remain the mainstay of treatment despite the intractable disease remission and toxicity associated with these treatment strategies. The widespread availability of novel technologies for its monitoring, early diagnosis, and care will continue to support the fight against CRC. For example, elucidation of the genetic basis initiation, development, and progression of CRC has led to the introduction of biotechnology products that have had a significant impact on its treatment. Inhibitors of the vascular endothelial growth factor receptors (VEGFR) such as fruquitinib, trifluridine/tipiracil (FTD/TPI), and the monoclonal antibody (bevacizumab) have proven efficacious in the treatment of CRC cells that were previously resistant to available chemotherapies. Current understanding of the molecular basis of CRC and identification of specific cell surface receptors for peptide ligands will support the nanoparticle-based targeting of combination chemotherapeutic agents and/or monoclonal antibodies to the cells in ways that will minimize the off-target binding, enable high target specificity, and preserve normal cells. Preservation of normal cells will, in turn, lead to the abolition or reduction of adverse drug events, promote patient compliance, and produce an overall improvement in treatment outcomes.
Author Contributions
Conceptualization, A.S.A. and K.A.; methodology, A.S.A.; software, K.A. and A.S.A.; validation, A.S.A., S.K.A., K.A. and O.O.; formal analysis, K.A.; investigation, A.S.A. and K.A.; resources, A.S.A., S.K.A. and K.A.; data curation, K.A. and A.S.A.; writing—original draft preparation, K.A. and A.S.A.; writing—review and editing, A.S.A., K.A. and S.K.A.; visualization, A.S.A. and K.A.; supervision, A.S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the American Cancer Society Diversity in Cancer Research Institutional Development Grant (DICRIDG-21-074-01-DICRIDG) at Howard University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Xi, Y.; Xu, P. Global colorectal cancer burden in 2020 and projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, C.; Wang, Q.; Wu, K.; Sun, Z.; Tang, Z.; Zhang, B. Global, Regional, and National Burden of Colorectal Cancer and Attributable Risk Factors, from 1990 to 2019: Updated Results from the Global Burden of Disease Study 2019. Available online: https://www.researchsquare.com/article/rs-1478628/v1 (accessed on 23 October 2023).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. Available online: https://pubmed.ncbi.nlm.nih.gov/33538338/ (accessed on 23 October 2023). [CrossRef]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomized controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef]
- World Health Organization. WHO Report on Cancer: Setting Priorities, Investing Wisely and Providing Care for All. World Health Organization. Available online: https://www.who.int/publications-detail-redirect/9789240001299 (accessed on 17 August 2023).
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society (ACS). Cancer Facts & Figures; American Cancer Society: Atlanta, GA, USA, 2022; Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2022.html (accessed on 26 May 2023).
- Lebwohl, B.; Capiak, K.; Neugut, A.I.; Kastrinos, F. Risk of colorectal adenomas and advanced neoplasia in Hispanic, black and white patients undergoing screening colonoscopy. Aliment. Pharmacol. Ther. 2012, 35, 1467–1473. [Google Scholar] [CrossRef]
- Coughlin, S.S. Social determinants of colorectal cancer risk, stage, and survival: A systematic review. Int. J. Color. Dis. 2020, 35, 985–995. [Google Scholar] [CrossRef]
- Engin, O.; Kilinc, G.; Salimoglu, S. Trends, risk factors, and preventions in colorectal cancer. Colon. Polyps Color. Cancer 2020, 213–233. [Google Scholar] [CrossRef]
- Li, Y.; Lauriola, M.; Kim, D.; Francesconi, M.; D’Uva, G.; Shibata, D.; Malafa, M.P.; Yeatman, T.J.; Coppola, D.; Solmi, R.; et al. Adenomatous polyposis coli (APC) regulates MIR17-92 cluster through β-catenin pathway in colorectal cancer. Oncogene 2016, 35, 4558–4568. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Shay, J.W. Multiple roles of APC and its therapeutic implications in colorectal cancer. JNCI J. Natl. Cancer Inst. 2017, 109, djw332. [Google Scholar] [CrossRef]
- Zhou, J.J. MicroRNA regulation network in colorectal cancer metastasis. World J. Biol. Chem. 2014, 5, 301. [Google Scholar] [CrossRef]
- Tian, Y.; Kharazmi, E.; Sundquist, K.; Sundquist, J.; Brenner, H.; Fallah, M. Familial colorectal cancer risk in half siblings and siblings: Nationwide cohort study. BMJ 2019, 364, l803. [Google Scholar] [CrossRef]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.S.; Karuniawati, H.; Jairoun, A.A.; Urbi, Z.; Ooi, D.J.; John, A.; Hadi, M.A. Colorectal cancer: A review of carcinogenesis, global epidemiology, current challenges, risk factors, preventive and treatment strategies. Cancers 2022, 14, 1732. [Google Scholar] [CrossRef] [PubMed]
- Dulai, P.S.; Sandborn, W.J.; Gupta, S. Colorectal Cancer and Dysplasia in Inflammatory Bowel Disease: A Review of Disease Epidemiology, Pathophysiology, and Management Colorectal Cancer in Inflammatory Bowel Disease. Cancer Prev. Res. 2016, 9, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Pancione, M.; Remo, A.; Colantuoni, V. Genetic and epigenetic events generate multiple pathways in colorectal cancer progression. Pathol. Res. Int. 2012, 2012, 509348. [Google Scholar] [CrossRef]
- Ziapour, P.; Ataee, R.; Shadifar, M.; Vaillancourt, C.; Ahmadi, A.; Jafari-Sabet, M.; Ataee, A. New intracellular and molecular aspects in pathophysiology of colorectal cancer. Gastroenterol. Hepatol. Bed Bench 2011, 4, 43–52. [Google Scholar]
- Gupta, R.; Sinha, S.; Paul, R.N. The impact of microsatellite stability status in colorectal cancer. Curr. Probl. Cancer 2018, 42, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Bach, D.H.; Zhang, W.; Sood, A.K. Chromosomal instability in tumor initiation and development. Cancer Res. 2019, 79, 3995–4002. [Google Scholar] [CrossRef]
- Cisterna, B.A.; Kamaly, N.; Choi, W.I.; Tavakkoli, A.; Farokhzad, O.C.; Vilos, C. Targeted nanoparticles for colorectal cancer. Nanomedicine 2016, 11, 2443–2456. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Engler, J.A.; Collawn, J.F.; Moore, B.A. Receptor mediated uptake of peptides that bind the human transferrin receptor. Eur. J. Biochem. 2001, 268, 2004–2012. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Bickel, U. Transferrin receptor mediated brain uptake during ischemia and reperfusion. J. Pharm. Pharm. Sci. 2013, 16, 541. [Google Scholar] [CrossRef]
- Abegg, D.; Gasparini, G.; Hoch, D.G.; Shuster, A. Strained Cyclic Disulfides Enable Cellular Uptake by Reacting with the Transferrin Receptor. 2016. Available online: https://pubs.acs.org/doi/suppl/10.1021/jacs.6b09643/suppl_file/ja6b09643_si_001.pdf (accessed on 17 August 2023).
- Rapoport, S.M. Uptake and fate of iron: The transferrin receptor. In The Reticulocyte; CRC Press: Boca Raton, FL, USA, 2020; pp. 145–154. [Google Scholar] [CrossRef]
- Xue, X.; Kim, H. IDDF2022-ABS-0024 Transferrin Receptor-Mediated Iron Uptake Is Essential for Colon Tumorigenesis. Basic. Gastroenterol. 2022, 71, A32. Available online: https://gut.bmj.com/content/71/Suppl_2/A32.1 (accessed on 17 August 2023).
- Ren, J.; Zhang, P.; Li, Z.; Zhang, X.; Shen, D.; Chen, P.; Mao, C. Association of screening status, polygenic risk score and environmental risk factors with colorectal cancer incidence and mortality risks. Int. J. Cancer 2023, 152, 1778–1788. [Google Scholar] [CrossRef] [PubMed]
- Krul, M.F.; Elferink, M.A.G.; Kok, N.F.M.; Dekker, E.; Lansdorp-Vogelaar, I.; Meijer, G.A.; Nagtegaal, I.D.; Breekveldt, E.C.H.; Ruers, T.J.M.; van Leerdam, M.E.; et al. Initial impact of national CRC screening on incidence and advanced colorectal cancer. Clin. Gastroenterol. Hepatol. 2023, 21, 797–807. [Google Scholar] [CrossRef]
- Sharma, A.; Sharma, A.; Sharma, V.; Kumar, S.; Kumar, A.; Deo, S.; Pathy, S.; Shukla, N.K.; Pramanik, R.; Raina, V.; et al. Long-Term Survivors of Metastatic Colorectal Cancer: A Tertiary Care Centre Experience. South. Asian J. Cancer 2021, 10, 87–91. [Google Scholar] [CrossRef]
- Sharma, R. Global, regional, national burden of breast cancer in 185 countries: Evidence from Globocan 2018. Breast Cancer Res. Treat. 2021, 187, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Bretthauer, M.; Løberg, M.; Wieszczy, P.; Kalager, M.; Emilsson, L.; Garborg, K.; Kaminski, M.F. Effect of colonoscopy screening on risks of colorectal cancer and related death. N. Engl. J. Med. 2022, 387, 1547–1556. [Google Scholar] [CrossRef]
- Diedrich, L.; Brinkmann, M.; Dreier, M.; Rossol, S.; Schramm, W.; Krauth, C. Is there a place for sigmoidoscopy in colorectal cancer screening? A systematic review and critical appraisal of cost-effectiveness models. PLoS ONE 2023, 18, e0290353. [Google Scholar] [CrossRef]
- Imperiale, T.F.; Ransohoff, D.F. In adults, sigmoidoscopy screening invitation reduced CRC incidence and related mortality at 15 y. Ann. Intern. Med. 2023, 176, JC19. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, A.; Lee, Y.Y. Colon and pelvic floor anatomy and physiology. Clin. Basic. Neurogastroenterol. Motil. 2020, 113–126. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Camilleri, M. Physiology of the colon and its measurement. In Shackelford’s Surgery of the Alimentary Tract; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1676–1688. [Google Scholar]
- Iacopetta, B. Are there two sides to colorectal cancer? Int. J. Cancer 2002, 101, 403–408. [Google Scholar] [CrossRef]
- Gervaz, P.; Bucher, P.; Morel, P. Two colons-two cancers: Paradigm shift and clinical implications. J. Surg. Oncol. 2004, 88, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, K.; Santi, I.; Weires, M.; Thomsen, H.; Sundquist, J.; Bermejo, J.L. Tumor location and patient characteristics of colon and rectal adenocarcinomas in relation to survival and TNM classes. BMC Cancer 2010, 10, 688. [Google Scholar] [CrossRef]
- Price, T.J.; Beeke, C.; Ullah, S.; Padbury, R.; Maddern, G.; Roder, D.; Karapetis, C. Does the primary site of colorectal cancer impact outcomes for patients with metastatic disease? Cancer 2015, 12, 830–835. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Tejpar, S.; Gibbs, P.; Thiebach, L.; Lenz, H.J. Understanding the role of primary tumour localization in colorectal cancer treatment and outcomes. Eur. J. Cancer 2017, 84, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.K.; Shin, U.S.; Ki, Y.J.; Kim, Y.B.; Moon, S.M.; Sung, S.J. Is the location of the tumor another prognostic factor for patients with colon cancer? Ann. Coloproctol. 2017, 33, 210. [Google Scholar] [CrossRef]
- Cappell, M.S. From colonic polyps to colon cancer: Pathophysiology, clinical presentation, and diagnosis. Clin. Lab. Med. 2005, 25, 135–177. [Google Scholar] [CrossRef]
- Loupakis, F.; Yang, D.; Yau, L.; Feng, S.; Cremolini, C.; Zhang, W.; Lenz, H.J. Primary tumor location as a prognostic factor in metastatic colorectal cancer. JNCI J. Natl. Cancer Inst. 2015, 107, dju427. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.H.; Malietzis, G.; Askari, A.; Bernardo, D.; Al-Hassi, H.O.; Clark, S.K. Is right-sided colon cancer different to left-sided colorectal cancer? –a systematic review. Eur. J. Surg. Oncol. 2015, 41, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Hochster, H.; Shitara, K.; Mayer, R.; Ohtsu, A.; Falcone, A.; Tabernero, J. Pooled safety analysis from phase III studies of trifluridine/tipiracil in patients with metastatic gastric or gastroesophageal junction cancer and metastatic colorectal cancer. ESMO Open 2022, 7, 100633. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Quail, D.F.; Joyce, J.A. Microenvironmental regulation of tumor progression and metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef]
- Colangelo, T.; Polcaro, G.; Muccillo, L.; D’Agostino, G.; Rosato, V.; Ziccardi, P. Colantuoni, Friend or foe?: The tumor microenvironment dilemma in colorectal cancer. Biochim. Et. Biophys. Acta (BBA)-Rev. Cancer 2017, 1867, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Cirri, P.; Chiarugi, P. Cancer associated fibroblasts: The dark side of the coin. Am. J. Cancer Res. 2011, 1, 482. [Google Scholar] [PubMed]
- Hawinkels LJ, A.C.; Paauwe, M.; Verspaget, H.W.; Wiercinska, E.; Van Der Zon, J.M.; Van Der Ploeg, K.; Sier CF, M. Interaction with colon cancer cells hyperactivates TGF-β signaling in cancer-associated fibroblasts. Oncogene 2014, 33, 97–107. [Google Scholar] [CrossRef]
- Paulsson, J.; Micke, P. Prognostic relevance of cancer-associated fibroblasts in human cancer. In Seminars in Cancer Biology; Academic Press: Cambridge, MA, USA, 2014; Volume 25, pp. 61–68. [Google Scholar]
- Robinwarren, J. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983, 321, 1273–1275. [Google Scholar] [CrossRef]
- Chmiela, M.; Karwowska, Z.; Gonciarz, W.; Allushi, B.; Stączek, P. Host pathogen interactions in helicobacter pylori related gastric cancer. World J. Gastroenterol. 2017, 23, 1521. [Google Scholar] [CrossRef]
- Suerbauma, S.; Achtmanb, M. Helicobacter pylori: Recombination, population structure and human migrations. Int. J. Med. Microbiol. 2004, 294, 133–139. [Google Scholar] [CrossRef]
- Zhao, Y.S.; Wang, F.; Chang, D.; Han, B.; You, D.Y. Meta-analysis of different test indicators: Helicobacter pylori infection and the risk of colorectal cancer. Int. J. Color. Dis. 2008, 23, 875–882. [Google Scholar] [CrossRef]
- Zuo, Y.; Jing, Z.; Bie, M.; Xu, C.; Hao, X.; Wang, B. Association between Helicobacter pylori infection and the risk of colorectal cancer: A systematic review and meta-analysis. Medicine 2020, 99, 37. [Google Scholar] [CrossRef]
- Zhang, Y.; Hoffmeister, M.; Weck, M.N.; Chang-Claude, J.; Brenner, H. Helicobacter pylori infection and colorectal cancer risk: Evidence from a large population-based case-control study in Germany. Am. J. Epidemiol. 2012, 175, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Fernández de Larrea-Baz, N.; Michel, A.; Romero, B.; Pérez-Gómez, B.; Moreno, V.; Martín, V.; Dierssen-Sotos, T.; Jiménez-Moleón, J.J.; Castilla, J.; Tardón, A.; et al. Helicobacter pylori Antibody Reactivities and Colorectal Cancer Risk in a Case-control Study in Spain. Front. Microbiol. 2017, 8, 888. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.; Varga, M.G.; Blot, W.J.; Teras, L.; Visvanathan, K.; Le Marchand, L.; Epplein, M. Serologic response to Helicobacter pylori proteins associated with risk of colorectal cancer among diverse populations in the United States. Gastroenterology 2019, 156, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Sokic-Milutinovic, A.; Alempijevic, T.; Milosavljevic, T. Role of Helicobacter pylori infection in gastric carcinogenesis: Current knowledge and future directions. World J. Gastroenterol. 2015, 21, 11654. [Google Scholar] [CrossRef]
- Takahashi-Kanemitsu, A.; Knight, C.T.; Hatakeyama, M. Molecular anatomy and pathogenic actions of helicobacter pylori CagA that underpin gastric carcinogenesis. Cell. Mol. Immunol. 2019, 17, 50–63. [Google Scholar] [CrossRef]
- World Health Organization. WHO Publishes List of Bacteria for which New Antibiotics Are Urgently Needed. World Health Organization. Available online: https://www.who.int/news/item/27-02-2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed (accessed on 17 August 2023).
- Srisuphanunt, M.; Wilairatana, P.; Kooltheat, N.; Duangchan, T.; Katzenmeier, G.; Rose, J.B. Molecular mechanisms of antibiotic resistance and novel treatment strategies for helicobacter pylori infections. Trop. Med. Infect. Dis. 2023, 8, 163. [Google Scholar] [CrossRef]
- Cardos, A.I.; Maghiar, A.; Zaha, D.C.; Pop, O.; Fritea, L.; Miere, F.; Cavalu, S. Evolution of diagnostic methods for helicobacter pylori infections: From traditional tests to high technology, advanced sensitivity and discrimination tools. Diagnostics 2022, 12, 508. [Google Scholar] [CrossRef]
- Behranvand, N.; Nasri, F.; Zolfaghari Emameh, R.; Khani, P.; Hosseini, A.; Garssen, J.; Falak, R. Chemotherapy: A double-edged sword in cancer treatment. Cancer Immunol. Immunother. 2022, 71, 507–526. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Muro, K.; Ajioka, Y.; Hashiguchi, Y.; Ito, Y.; Saito, Y. Japanese Society for Cancer of the Colon and Rectum Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2018, 23, 1–34. [Google Scholar] [CrossRef]
- Dorudi, S.; Steele, R.J.; McArdle, C.S. Surgery for colorectal cancer. Br. Med. Bull. 2002, 64, 101–118. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.D.; Felder, S.I.; Bhama, A.R.; Hawkins, A.T.; Langenfeld, S.J.; Shaffer, V.O.; Paquette, I.M. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of colon cancer. Dis. Colon. Rectum 2022, 65, 148–177. [Google Scholar] [CrossRef] [PubMed]
- Pak, H.; Maghsoudi, L.H.; Soltanian, A.; Gholami, F. Surgical complications in colorectal cancer patients. Ann. Med. Surg. 2020, 55, 13–18. [Google Scholar] [CrossRef]
- Gomez Ruiz, M.; Lainez Escribano, M.; Cagigas Fernandez, C.; Cristobal Poch, L.; Santarrufina Martinez, S. Robotic surgery for colorectal cancer. Ann. Gastroenterol. Surg. 2020, 4, 646–651. [Google Scholar] [CrossRef]
- Theodorescu, D. Cancer cryotherapy: Evolution and biology. Rev. Urol. 2004, 6 (Suppl. S4), S9. [Google Scholar]
- Jiang, X.; Ji, Z.; Lei, X.; Liu, C.; Yuan, F. Suitable T stage for cryosurgery to spare the anus in patients with low rectal cancer. Cryobiology 2023, 111, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Bageacu, S.; Kaczmarek, D.; Lacroix, M.; Dubois, J.; Forest, J.; Porcheron, J. Cryosurgery for resectable and unresectable hepatic metastases from colorectal cancer. Eur. J. Surg. Oncol. 2007, 33, 590–596. [Google Scholar] [CrossRef]
- Joyce, J.A.; Fearon, D.T. T cell exclusion, immune privilege, and the tumor microenvironment. Science 2015, 348, 74–80. [Google Scholar] [CrossRef]
- Menon, H.; Ramapriyan, R.; Cushman, T.R.; Verma, V.; Kim, H.H.; Schoenhals, J.E.; Welsh, J.W. Role of radiation therapy in modulation of the tumor stroma and microenvironment. Front. Immunol. 2019, 10, 193. [Google Scholar] [CrossRef]
- Haddock, M.G. Intraoperative radiation therapy for colon and rectal cancers: A clinical review. Radiat. Oncol. 2017, 12, 11. [Google Scholar] [CrossRef]
- Potemin, S.; Kübler, J.; Uvarov, I.; Wenz, F.; Giordano, F. Intraoperative radiotherapy as an immediate adjuvant treatment of rectal cancer due to limited access to external-beam radiotherapy. Radiat. Oncol. 2020, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Tofthagen, C. Surviving chemotherapy for colon cancer and living with the consequences. J. Palliat. Med. 2010, 13, 1389–1391. [Google Scholar] [CrossRef] [PubMed]
- Ades, S. Adjuvant chemotherapy for colon cancer in the elderly: Moving from evidence to practice. Oncology 2009, 23, 162. [Google Scholar]
- Dickens, E.; Ahmed, S. Principles of cancer treatment by chemotherapy. Surgery 2018, 36, 134–138. [Google Scholar]
- Bhosle, J.; Hall, G. Principles of cancer treatment by chemotherapy. Surgery 2009, 27, 173–177. [Google Scholar]
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J. Benefits and drawbacks of the use of oral fluoropyrimidines as single-agent therapy in advanced colorectal cancer. Clin. Color. Cancer 2005, 5, S47–S50. [Google Scholar] [CrossRef] [PubMed]
- Ashwanikumar, N.; Kumar, N.A.; Nair, S.A.; Kumar, G.V. Methacrylic-based nanogels for the pH-sensitive delivery of 5-fluorouracil in the colon. Int. J. Nanomed. 2012, 7, 5769–5779. [Google Scholar]
- Dhawale, S.C.; Bankar, A.S.; Patro, M.N. Formulation and evaluation porous microspheres of 5-fluorouracil for colon targeting. Int. J. Pharm. Tech. Res. 2010, 2, 1112–1118. [Google Scholar]
- Bailly, C. Irinotecan: 25 years of cancer treatment. Pharmacol. Res. 2019, 148, 104398. [Google Scholar] [CrossRef]
- Bao, X.; Wu, J.; Kim, S.; LoRusso, P.; Li, J. Pharmacometabolomics reveals irinotecan mechanism of action in cancer patients. J. Clin. Pharmacol. 2019, 59, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Reyhanoglu, G.; Smith, T. Irinotecan in StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Miele, L.; Liguori, A.; Marrone, G.; Biolato, M.; Araneo, C.; Vaccaro, F.G.; Grieco, A. Fatty liver and drugs: The two sides of the same coin. Eur. Rev. Med. Pharmacol. Sci. 2017, 21 (Suppl. S1), 86–94. [Google Scholar] [PubMed]
- Milano, G.; Innocenti, F.; Minami, H. Liposomal irinotecan (Onivyde): Exemplifying the benefits of nanotherapeutic drugs. Cancer Sci. 2022, 113, 2224–2231. [Google Scholar] [CrossRef]
- Machover, D. Treatment of advanced colorectal and gastric adenocarcinomas with 5-FU combined with high-dose folinic acid: A pilot study. Cancer Treat. Rep. 1982, 66, 1803–1807. [Google Scholar]
- Thirion, P.; Michiels, S.; Pignon, J.P.; Buyse, M.; Braud, A.C.; Carlson, R.W.; O’Connell, M.; Sargent, P.; Piedbois, P. Meta-Analysis Group in Cancer Modulation of fluorouracil by leucovorin in patients with advanced colorectal cancer: An updated meta-analysis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 3766–3775. [Google Scholar] [CrossRef]
- Ibrahim, B.; Mady, O.Y.; Tambuwala, M.M.; Haggag, Y.A. pH-sensitive nanoparticles containing 5-fluorouracil and leucovorin as an improved anti-cancer option for colon cancer. Nanomedicine 2022, 17, 367–381. [Google Scholar] [CrossRef]
- Veronese, M.L.; O’Dwyer, P.J. Monoclonal antibodies in the treatment of colorectal cancer. Eur. J. Cancer 2004, 40, 1292–1301. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.J.; Cohen, R.B.; Meropol, N.J. Targeting signal transduction pathways in colorectal cancer—More than skin deep. J. Clin. Oncol. 2005, 23, 5374–5385. [Google Scholar] [CrossRef]
- Dvorak, H.F. Vascular permeability factor/vascular endothelial growth factor: A critical cytokine in tumor angiogenesis and a potential target for diagnosis and therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20, 4368–4380. [Google Scholar] [CrossRef]
- Grünwald, V.; Hidalgo, M. Developing inhibitors of the epidermal growth factor receptor for cancer treatment. J. Natl. Cancer Inst. 2003, 95, 851–867. [Google Scholar] [CrossRef]
- Aprile, G.; Rihawi, K.; De Carlo, E.; Sonis, S.T. Treatment-related gastrointestinal toxicities and advanced colorectal or pancreatic cancer: A critical update. World J. Gastroenterol. 2015, 21, 11793–11803. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Wang, C.; Wang, F.; Li, P.; Hu, Z.; Shan, Y.; Zhang, J. Development of 5-fluorouracil derivatives as anticancer agents. Curr. Med. Chem. 2011, 18, 4538–4556. [Google Scholar] [CrossRef]
- Kim, J.H. Chemotherapy for colorectal cancer in the elderly. World J. Gastroenterol. 2015, 21, 5158–5166. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shitara, K.; Mizusawa, J.; Hamaguchi, T.; Shida, D.; Komori, K.; Ikeda, S.; Ojima, H.; Ike, H.; Shiomi, A.; et al. Primary tumor resection plus chemotherapy versus chemotherapy alone for colorectal cancer patients with asymptomatic, synchronous unresectable metastases (JCOG1007; ipacs): A randomized clinical trial. J. Clin. Oncol. 2021, 39, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Huang, S.; Huang, G. Design and application of Oral Colon Administration System. J. Enzym. Inhib. Med. Chem. 2019, 34, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Otte, A.; Park, K. Evolution of drug delivery systems: From 1950 to 2020 and beyond. J. Control. Release 2022, 342, 53–65. [Google Scholar] [CrossRef]
- Williams, T.M.; Sable, R.; Singh, S.; Vicente, M.G.; Jois, S.D. Peptide ligands for targeting the extracellular domain of EGFR: Comparison between linear and cyclic peptides. Chem. Biol. Drug Des. 2017, 91, 605–619. [Google Scholar] [CrossRef]
- Islam, M.S.; Junod, S.L.; Zhang, S.; Buuh, Z.Y.; Guan, Y.; Zhao, M.; Kaneria, K.H.; Kafley, P.; Cohen, C.; Maloney, R.; et al. Unprotected peptide macrocyclization and stapling via a fluorine-thiol displacement reaction. Nat. Commun. 2022, 13, 350. [Google Scholar] [CrossRef]
- Laffleur, F.; Keckeis, V. Advances in drug delivery systems: Work in progress still needed? Int. J. Pharm. 2020, 590, 119912. [Google Scholar] [CrossRef]
- Bahrami, A.; Khazaei, M.; Hassanian, S.M.; ShahidSales, S.; Joudi-Mashhad, M.; Maftouh, M.; Jazayeri, M.H.; Parizade, M.R.; Ferns, G.A.; Avan, A. Targeting the tumor microenvironment as a potential therapeutic approach in colorectal cancer: Rational and progress. J. Cell. Physiol. 2018, 233, 2928–2936. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Bhatt, N.; Patel, K.R.; Patel, N.M.; Patel, M.R. Colon targeted drug delivery system: A review system. J. Pharm. Sci. Biosci. Res. 2011, 1, 37–49. [Google Scholar]
- Kumar, M.; Ali, A.; Kaldhone, P.; Shirode, A.; Kadam, V.J. Report on pharmaceutical approaches to colon targeted drug delivery systems. J. Pharm. Res. 2010, 3, 157–159. [Google Scholar]
- Amidon, S.; Brown, J.E.; Dave, V.S. Colon-targeted oral drug delivery systems: Design trends and approaches. AAPS Pharm. SciTech 2015, 16, 731–741. [Google Scholar] [CrossRef]
- Yoshida, T.; Lai, T.C.; Kwon, G.S.; Sako, K. pH-and ion-sensitive polymers for drug delivery. Expert. Opin. Drug Deliv. 2013, 10, 1497–1513. [Google Scholar] [CrossRef]
- Newton AM, J.; Prabakaran, L.; Jayaveera, K. Pectin-HPMC E15LV vs. pH sensitive polymer coating films for delayed drug delivery to colon: A comparison of two dissolution models to assess colonic targeting performance in-vitro. Int. J. Appl. Res. Nat. Prod. 2012, 5, 1–16. [Google Scholar]
- Englert, C.; Brendel, J.C.; Majdanski, T.C.; Yildirim, T.; Schubert, S.; Gottschaldt, M.; Windhab, N.; Schubert, U.S. Pharmapolymers in the 21st century: Synthetic polymers in drug delivery applications. Prog. Polym. Sci. 2018, 87, 107–164. [Google Scholar] [CrossRef]
- Naik, J.B.; Waghulde, M.R. Development of vildagliptin loaded Eudragit® microspheres by screening design: In vitro evaluation. J. Pharm. Investig. 2018, 48, 627–637. [Google Scholar] [CrossRef]
- Mahkam, M.; Abbaszad Rafi, A.; Mohammadzadeh Gheshlaghi, L. Preparation of novel pH-sensitive nanocomposites based on ionic-liquid modified montmorillonite for colon specific drug delivery system. Polym. Compos. 2016, 37, 182–187. [Google Scholar] [CrossRef]
- Lamprecht, A.; Yamamoto, H.; Takeuchi, H.; Kawashima, Y. Design of pH-sensitive microspheres for the colonic delivery of the immunosuppressive drug tacrolimus. Eur. J. Pharm. Biopharm. 2004, 58, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Kotla, N.G.; Rana, S.; Sivaraman, G.; Sunnapu, O.; Vemula, P.K.; Pandit, A.; Rochev, Y. Bioresponsive drug delivery systems in intestinal inflammation: State-of-the-art and future perspectives. Adv. Drug Deliv. Rev. 2019, 146, 248–266. [Google Scholar] [CrossRef]
- Prajakta, D.; Ratnesh, J.; Chandan, K.; Suresh, S.; Grace, S.; Meera, V.; Vandana, P. Curcumin-loaded pH-sensitive nanoparticles for the treatment of colon cancer. J. Biomed. Nanotechnol. 2009, 5, 445–455. [Google Scholar] [CrossRef]
- Naeem, M.; Awan, U.A.; Subhan, F.; Cao, J.; Hlaing, S.P.; Lee, J.; Yoo, J.W. Advances in colon-targeted nano-drug delivery systems: Challenges and solutions. Arch. Pharmacal. Res. 2020, 43, 153–169. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Gan, X.; Chen, Y. A novel pH-sensitive hydrogels for potential colon-specific drug delivery: Characterization and in vitro release studies. Starch-Stärke 2011, 63, 503–511. [Google Scholar] [CrossRef]
- Mamidi, N.; Velasco Delgadillo, R.; Gonzáles Ortiz, A.; Barrera, E.V. Carbon. nano-onions reinforced multilayered thin film system for stimuli-responsive drug release. Pharmaceutics 2020, 12, 1208. [Google Scholar] [CrossRef] [PubMed]
- Mamidi, N.; Velasco Delgadillo, R.M.; Barrera, E.V. Covalently Functionalized Carbon Nano-Onions Integrated Gelatin Methacryloyl Nanocomposite Hydrogel Containing γ-Cyclodextrin as Drug Carrier for High-Performance PH-Triggered Drug Release. Pharmaceutics 2021, 14, 291. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8064464/ (accessed on 14 August 2023).
- Mamidi, N.; Delgadillo, R.M. Design, fabrication and drug release potential of dual stimuli-responsive composite hydrogel nanoparticle interfaces. Colloids Surf. B Biointerfaces 2021, 204, 1118–1119. [Google Scholar] [CrossRef]
- Garrett, W.S. The gut microbiota and colon cancer. Science 2019, 364, 1133–1135. [Google Scholar] [CrossRef]
- Shukla, R.K.; Tiwari, A. Carbohydrate polymers: Applications and recent advances in delivering drugs to the colon. Carbohydr. Polym. 2012, 88, 399–416. [Google Scholar] [CrossRef]
- Yadav, V.K.; Gupta, A.B.; Kumar, R.; Yadav, J.S.; Kumar, B. Mucoadhesive polymers: Means of improving the mucoadhesive properties of drug delivery system. J. Chem. Pharm. Res. 2010, 2, 418–432. [Google Scholar]
- Zhu, J.; Zhong, L.; Chen, W.; Song, Y.; Qian, Z.; Cao, X.; Chen, W. Preparation and characterization of pectin/chitosan beads containing porous starch embedded with doxorubicin hydrochloride: A novel and simple colon targeted drug delivery system. Food Hydrocoll. 2019, 95, 562–570. [Google Scholar] [CrossRef]
- Barclay, T.G.; Day, C.M.; Petrovsky, N.; Garg, S. Review of polysaccharide particle-based functional drug delivery. Carbohydr. Polym. 2019, 221, 94–112. [Google Scholar] [CrossRef]
- Meng, Q.; Zhong, S.; Xu, L.; Wang, J.; Zhang, Z.; Gao, Y.; Cui, X. Review on design strategies and considerations of polysaccharide-based smart drug delivery systems for cancer therapy. Carbohydr. Polym. 2022, 279, 119013. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.; Shukla, N.; Mahajan, S. Polysaccharides in colon specific drug delivery. J. Transl. Sci. 2015, 1, 3–11. [Google Scholar]
- Wen, Y.; Oh, J.K. Recent strategies to develop polysaccharide-based nanomaterials for biomedical applications. Macromol. Rapid Commun. 2014, 35, 1819–1832. [Google Scholar] [CrossRef] [PubMed]
- Prudhviraj, G.; Vaidya, Y.; Singh, S.K.; Yadav, A.K.; Kaur, P.; Gulati, M.; Gowthamarajan, K. Effect of co-administration of probiotics with polysaccharide-based colon targeted delivery systems to optimize site specific drug release. Eur. J. Pharm. Biopharm. 2015, 97, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Si, X.Y.; Merlin, D.; Xiao, B. Recent advances in orally administered cell-specific nanotherapeutics for inflammatory bowel disease. World J. Gastroenterol. 2016, 22, 7718. [Google Scholar] [CrossRef]
- Alas, M.; Saghaeidehkordi, A.; Kaur, K. Peptide–drug conjugates with different linkers for cancer therapy. J. Med. Chem. 2020, 64, 216–232. [Google Scholar] [CrossRef]
- Candelaria, P.V.; Leoh, L.S.; Penichet, M.L.; Daniels-Wells, T.R. Antibodies targeting the transferrin receptor 1 (tfr1) as direct anti-cancer agents. Front. Immunol. 2021, 12, 607692. [Google Scholar] [CrossRef]
- Tesauro, D.; Accardo, A.; Diaferia, C.; Milano, V.; Guillon, J.; Ronga, L.; Rossi, F. Peptide-based drug-delivery systems in biotechnological applications: Recent advances and perspectives. Molecules 2019, 24, 351. [Google Scholar] [CrossRef]
- Ghosh, D.; Peng, X.; Leal, J.; Mohanty, R.P. Peptides as drug delivery vehicles across biological barriers. J. Pharm. Investig. 2018, 48, 89–111. [Google Scholar] [CrossRef]
- Jiang, Z.; Guan, J.; Qian, J.; Zhan, C. Peptide ligand-mediated targeted drug delivery of nanomedicines. Biomater. Sci. 2019, 7, 461–471. [Google Scholar] [CrossRef]
- Al-azzawi, S.; Masheta, D. Designing a drug delivery system for improved tumor treatment and targeting by functionalization of a cell-penetrating peptide. J. Pharm. Investig. 2019, 49, 643–654. [Google Scholar] [CrossRef]
- Ren, Y.; Mu, Y.; Song, Y.; Xie, J.; Yu, H.; Gao, S.; Lu, W. A new peptide ligand for colon cancer targeted delivery of micelles. Drug Deliv. 2016, 23, 1763–1772. [Google Scholar] [CrossRef]
- Guo, F.; Ouyang, T.; Peng, T.; Zhang, X.; Xie, B.; Yang, X.; Zhong, H. Enhanced oral absorption of insulin using colon-specific nanoparticles co-modified with amphiphilic chitosan derivatives and cell-penetrating peptides. Biomater. Sci. 2019, 7, 1493–1506. [Google Scholar] [CrossRef] [PubMed]
- Langel, Ü. Methods for CPP functionalization. CPP Cell-Penetrating Pept. 2019, 83–156. [Google Scholar] [CrossRef]
- Tiernan, J.P.; Perry, S.L.; Verghese, E.T.; West, N.P.; Yeluri, S.; Jayne, D.G.; Hughes, T.A. Carcinoembryonic antigen is the preferred biomarker for in vivo colorectal cancer targeting. Br. J. Cancer 2013, 108, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Noe, O.; Ngo, N.; Lin, L.; Stanbery, L.; Creeden, J.F.; Hamouda, D.; Nemunaitis, J. Folate Receptor as a Biomarker and Therapeutic Target in Solid Tumors. Curr. Probl. Cancer 2022, 47, 100917. [Google Scholar]
- Suwaidan, A.A.; Lau, D.K.; Chau, I. HER2 targeted therapy in colorectal cancer: New horizons. Cancer Treat. Rev. 2022, 105, 102363. [Google Scholar] [CrossRef]
- Mansoori, B.; Mohammadi, A.; Abedi-Gaballu, F.; Abbaspour, S.; Ghasabi, M.; Yekta, R.; Baradaran, B. Hyaluronic acid-decorated liposomal nanoparticles for targeted delivery of 5-fluorouracil into HT-29 colorectal cancer cells. J. Cell. Physiol. 2020, 235, 6817–6830. [Google Scholar] [CrossRef]
- Tabasi, H.; Mosavian, M.H.; Sabouri, Z.; Khazaei, M.; Darroudi, M. pH-responsive and CD44-targeting by Fe3O4/MSNs-NH2 nanocarriers for oxaliplatin loading and colon cancer treatment. Inorg. Chem. Commun. 2021, 125, 108430. [Google Scholar] [CrossRef]
- Kadam, R.S.; Bourne, D.W.; Kompella, U.B. Nano-advantage in enhanced drug delivery with biodegradable nanoparticles: Contribution of reduced clearance. Drug Metab. Dispos. 2012, 40, 1380–1388. [Google Scholar] [CrossRef]
- Barani, M.; Mirzaei, M.; Torkzadeh-Mahani, M.; Lohrasbi-Nejad, A.; Nematollahi, M.H. A new formulation of hydrophobin-coated niosome as a drug carrier to cancer cells. Mater. Sci. Eng. 2020, 113, 110975. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, A.; Chu, B.S.; Yaakob, H. Niosomal drug delivery systems: Formulation, preparation and applications. World Appl. Sci. J. 2014, 32, 1671–1685. [Google Scholar]
- Sebaaly, C.; Greige-Gerges, H.; Stainmesse, S.; Fessi, H.; Charcosset, C. Effect of composition, hydrogenation of phospholipids and lyophilization on the characteristics of eugenol-loaded liposomes prepared by ethanol injection method. Food Biosci. 2016, 15, 1–10. [Google Scholar] [CrossRef]
- Laouini, A.; Jaafar-Maalej, C.; Limayem-Blouza, I.; Sfar, S.; Charcosset, C.; Fessi, H. Preparation, characterization and applications of liposomes: State of the art. J. Colloid. Sci. Biotechnol. 2012, 1, 147–168. [Google Scholar] [CrossRef]
- Liu, P.; Chen, G.; Zhang, J. A review of liposomes as a drug delivery system: Current status of approved products, regulatory environments, and future perspectives. Molecules 2022, 27, 1372. [Google Scholar] [CrossRef]
- Niu, M.; Lu, Y.; Hovgaard, L.; Guan, P.; Tan, Y.; Lian, R.; Qi, J.; Wu, W. Hypoglycemic activity and oral bioavailability of insulin-loaded liposomes containing bile salts in rats: The effect of cholate type, particle size and administered dose. Eur. J. Pharm. Biopharm. 2012, 81, 265–272. [Google Scholar] [CrossRef]
- Wang, N.; Wang, T.; Li, T.; Deng, Y. Modulation of the physicochemical state of interior agents to prepare controlled release liposomes. Colloids Surf. B Biointerfaces 2009, 69, 232–238. [Google Scholar] [CrossRef]
- Alavi, M.; Hamidi, M. Passive and active targeting in cancer therapy by liposomes and lipid nanoparticles. Drug Metab. Pers. Ther. 2019, 34, 20180032. [Google Scholar] [CrossRef]
- Khuntawee, W.; Amornloetwattana, R.; Vongsangnak, W.; Namdee, K.; Yata, T.; Karttunen, M.; Wong-Ekkabut, J. In silico and in vitro design of cordycepin encapsulation in liposomes for colon cancer treatment. RSC Adv. 2021, 11, 8475–8484. [Google Scholar] [CrossRef]
- Xiong, M.; Lei, Q.; You, X.; Gao, T.; Song, X.; Xia, Y.; Yu, L. Mannosylated liposomes improve therapeutic effects of paclitaxel in colon cancer models. J. Microencapsul. 2017, 34, 513–521. [Google Scholar] [CrossRef]
- Yasamineh, S.; Yasamineh, P.; Ghafouri Kalajahi, H.; Gholizadeh, O.; Yekanipour, Z.; Afkhami, H.; Eslami, M.; Hossein Kheirkhah, A.; Taghizadeh, M.; Yazdani, Y.; et al. A state-of-the-art review on the recent advances of niosomes as a targeted drug delivery system. Int. J. Pharm. 2022, 624, 121878. [Google Scholar] [CrossRef]
- Marianecci, C.; Di Marzio, L.; Rinaldi, F.; Celia, C.; Paolino, D.; Alhaique, F.; Carafa, M. Niosomes from 80s to present: The state of the art. Adv. Colloid Interface Sci. 2014, 205, 187–206. [Google Scholar] [CrossRef]
- Moghassemi, S.; Hadjizadeh, A. Nano-niosomes as nanoscale drug delivery systems: An illustrated review. J. Control. Release 2014, 185, 22–36. [Google Scholar] [CrossRef]
- Varshosaz, J.; Taymouri, S.; Pardakhty, A.; Asadi-Shekaari, M.; Babaee, A. Niosomes of ascorbic acid and α-tocopherol in the cerebral ischemia-reperfusion model in male rats. BioMed Res. Int. 2014, 2014, 816103. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, S.; Kumar, Y.A.; Hemanth, A.; Anitha, M. Preparation and evaluation of niosomes containing aceclofenac. Dig. J. Nanomater. Bios 2010, 5, 249–254. [Google Scholar]
- Shakya, V.; Bansal, B.K. Niosomes: A novel trend in drug delivery. Int. J. Res. Dev. Pharm. Life Sci. 2014, 3, 1036–1041. [Google Scholar]
- Chen, S.; Hanning, S.; Falconer, J.; Locke, M.; Wen, J. Recent advances in non-ionic surfactant vesicles (niosomes): Fabrication, characterization, pharmaceutical and cosmetic applications. Eur. J. Pharm. Biopharm. 2019, 144, 18–39. [Google Scholar] [CrossRef]
- Witika, B.A.; Bassey, K.E.; Demana, P.H.; Siwe-Noundou, X.; Poka, M.S. Current advances in specialised niosomal drug delivery: Manufacture, characterization and drug delivery applications. Int. J. Mol. Sci. 2022, 23, 9668. [Google Scholar] [CrossRef]
- El-Ridy, M.S.; Badawi, A.A.; Safar, M.M.; Mohsen, A.M. Niosomes as a novel pharmaceutical formulation encapsulating the hepatoprotective drug silymarin. Int. J. Pharm. Pharm. Sci. 2012, 4, 549–559. [Google Scholar]
- Umbarkar, M.G. Niosome as a novel pharmaceutical drug delivery: A brief review highlighting formulation, types, composition and application. Indian. J. Pharm. Educ. Res. 2021, 55, s11–s28. [Google Scholar] [CrossRef]
- Ugorji, O.L.; Umeh ON, C.; Agubata, C.O.; Adah, D.; Obitte, N.C.; Chukwu, A. The effect of noisome preparation methods in encapsulating 5-fluorouracil and real time cell assay against HCT-116 colon cancer cell line. Heliyon 2022, 8, e12369. [Google Scholar] [CrossRef]
- El-Far, S.W.; Abo El-Enin, H.A.; Abdou, E.M.; Nafea, O.E.; Abdelmonem, R. Targeting colorectal cancer cells with niosomes systems loaded with two anticancer drugs models; comparative in vitro and anticancer studies. Pharmaceuticals 2022, 15, 816. [Google Scholar] [CrossRef]
- Prabhu, R.H.; Patravale, V.B.; Joshi, M.D. Polymeric nanoparticles for targeted treatment in oncology: Current insights. Int. J. Nanomed. 2015, 10, 1001–1018. [Google Scholar] [CrossRef]
- Lamprecht, A. Nanomedicines in gastroenterology and hepatology. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 195–204. [Google Scholar] [CrossRef]
- Greish, K. Enhanced permeability and retention (EPR) effect for anticancer nanomedicine drug targeting. Cancer Nanotechnol. Methods Protoc. 2010, 624, 25–37. [Google Scholar]
- Ejigah, V.; Owoseni, O.; Bataille-Backer, P.; Ogundipe, O.D.; Fisusi, F.A.; Adesina, S.K. Approaches to improve macromolecule and nanoparticle accumulation in the tumor microenvironment by the enhanced permeability and retention effect. Polymers 2022, 14, 2601. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Taieb, J.; Prager, G.W.; Ciardiello, F.; Fakih, M.; Leger, C.; Fougeray, R.; Amellal, N.; van Cutsem, E. Trifluridine/tipiracil plus bevacizumab for third-line management of metastatic colorectal cancer: SUNLIGHT study design. Future Oncol. 2021, 17, 1977–1985. [Google Scholar] [CrossRef]
- Prager, G.W.; Taieb, J.; Fakih, M.; Ciardiello, F.; Van Cutsem, E.; Elez, E.; Tabernero, J. Trifluridine–tipiracil and bevacizumab in refractory metastatic colorectal cancer. N. Engl. J. Med. 2023, 388, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Kuboki, Y.; Terazawa, T.; Masuishi, T.; Nakamura, M.; Watanabe, J.; Ojima, H.; Makiyama, A.; Kotaka, M.; Hara, H.; Kagawa, Y.; et al. Trifluridine/tipiracil+ bevacizumab (BEV) vs. fluoropyrimidine-irinotecan+ BEV as second-line therapy for metastatic colorectal cancer: A randomised noninferiority trial. Br. J. Cancer 2023, 128, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Lonardi, S.; Garcia-Carbonero, R.; Elez, E.; Yoshino, T.; Sobrero, A.; Yao, J.; García-Alfonso, P.; Kocsis, J.; Cubillo Gracian, A.; et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (fresco-2): An International, multicentre, randomised, double-blind, phase 3 study. Lancet 2023, 402, 41–53. [Google Scholar] [CrossRef]
- Shafi, A.A.; Knudsen, K.E. Cancer and the circadian clock. Cancer Res. 2019, 79, 3806–3814. [Google Scholar] [CrossRef]
- Kinouchi, K.; Sassone-Corsi, P. Metabolic rivalry: Circadian homeostasis and tumorigenesis. Nat. Rev. Cancer 2020, 20, 645–661. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wang, J.; Zhang, X.; Tang, Q. New insights into cancer chronotherapies. Front. Pharmacol. 2021, 12, 741295. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yu, Q.; Liu, Y.; Zhu, Z.; Wang, L.; Wang, H.; Li, K. Efficacy and safety of chronomodulated chemotherapy for patients with metastatic colorectal cancer: A systematic review and meta-analysis. Asia-Pac. J. Clin. Oncol. 2016, 13, e171–e178. [Google Scholar] [CrossRef]
- Nassar, A.; Abdelhamid, A.; Ramsay, G.; Bekheit, M. Chronomodulated Administration of Chemotherapy in Advanced Colorectal Cancer: A Systematic Review and Meta-Analysis. Cureus 2023, 15, e36522. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Risk factors of CRC. Created with BioRender.com.
Figure 1.
Risk factors of CRC. Created with BioRender.com.

Figure 2.
Diagnosis of CRC. Created with BioRender.com.
Figure 2.
Diagnosis of CRC. Created with BioRender.com.

Figure 3.
Reviewed articles selection protocol.
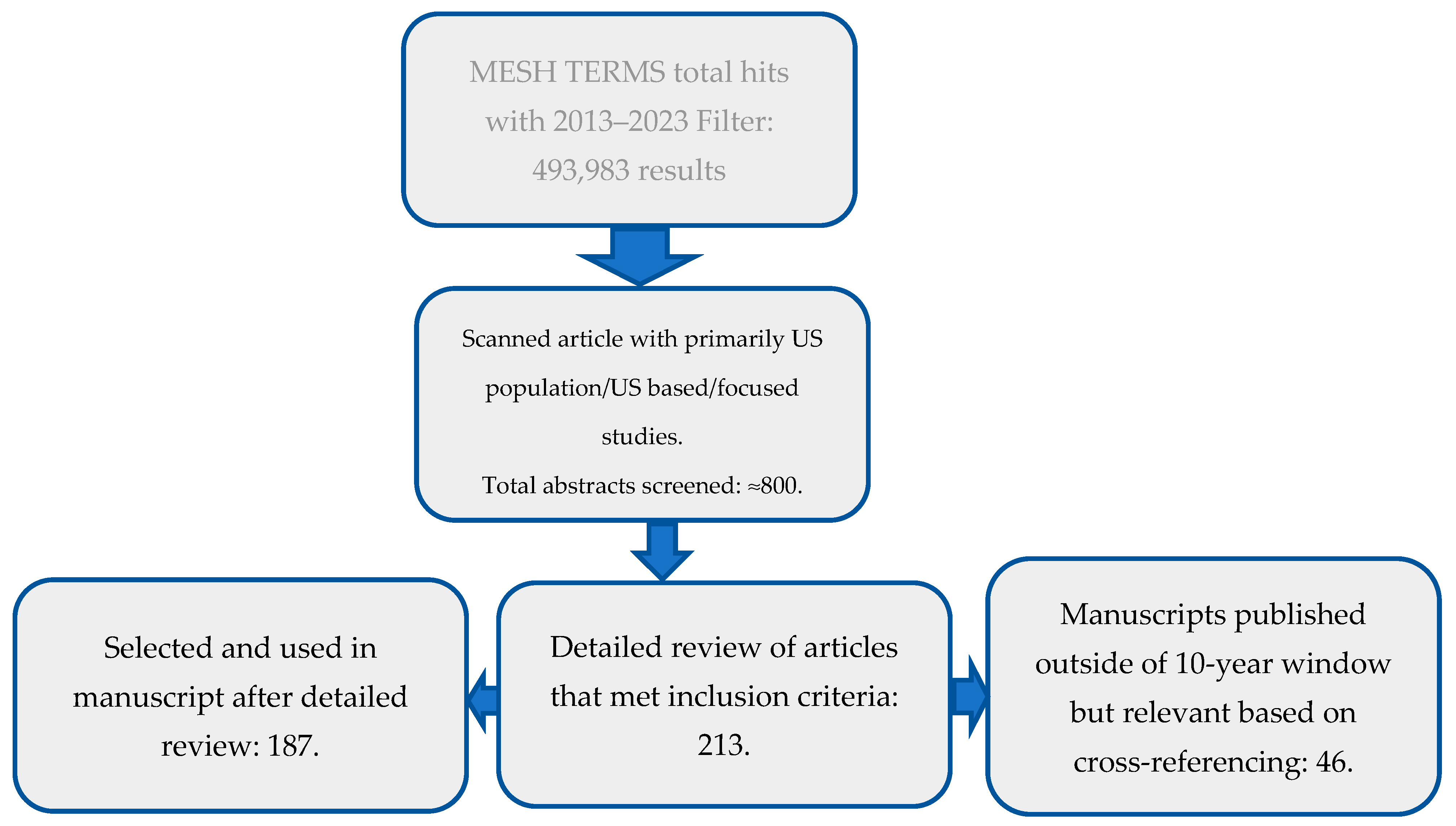
Figure 4.
Research articles returned by MESH words used in the primary search in PubMed.
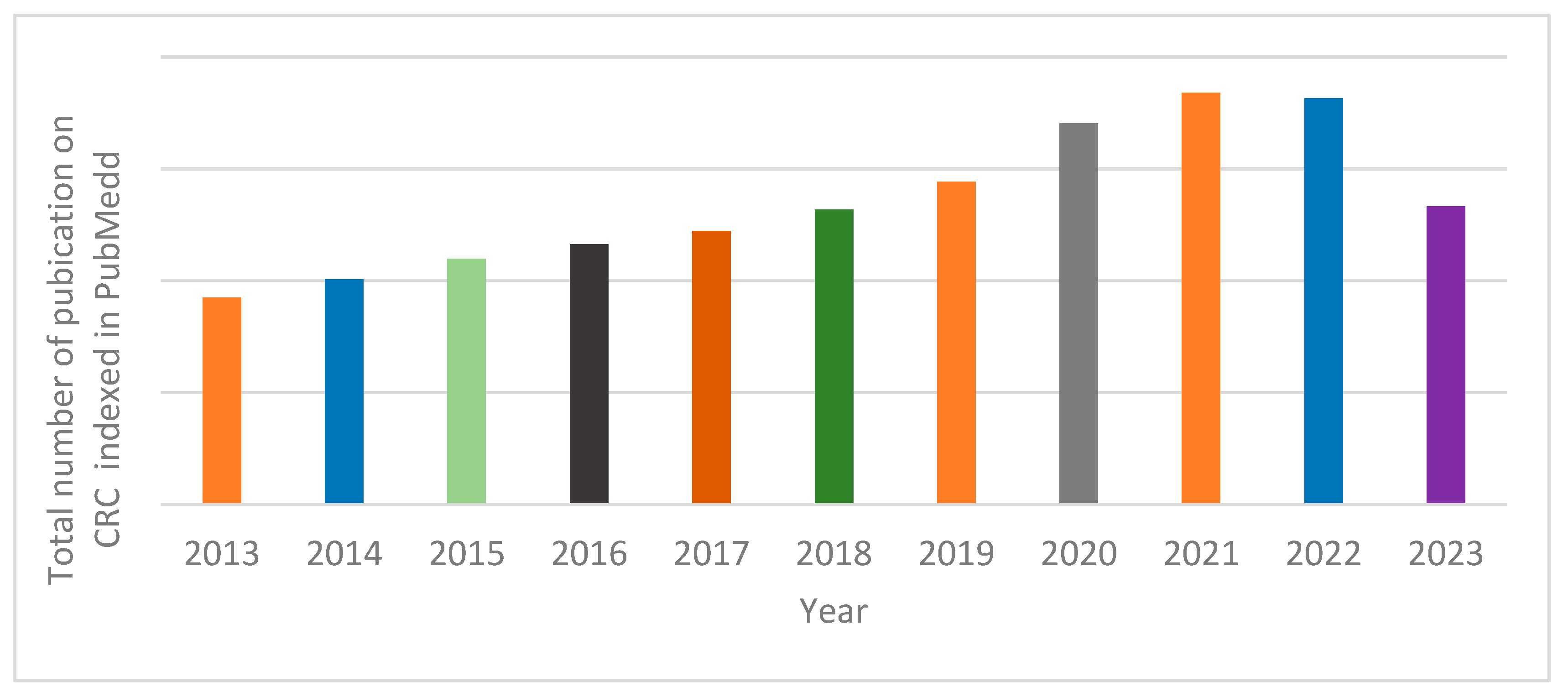
Figure 5.
Anatomical description of the colon. Created with BioRender.com.
Figure 5.
Anatomical description of the colon. Created with BioRender.com.
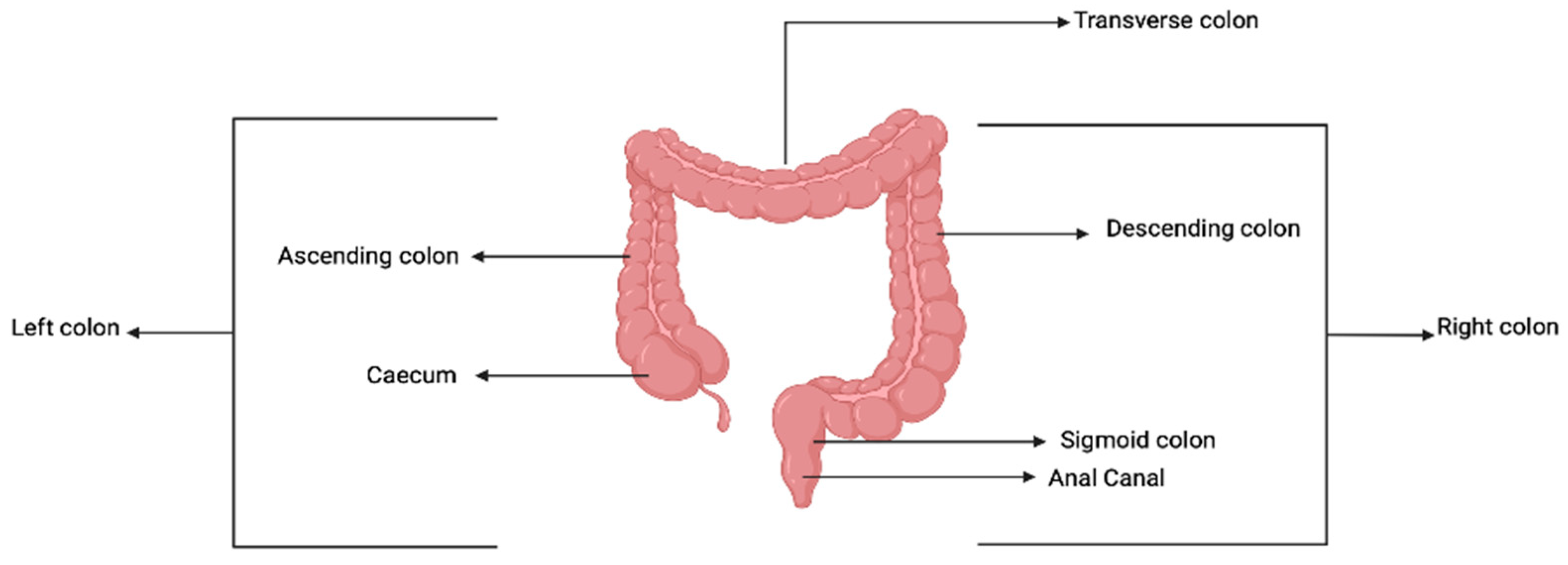
Figure 6.
Disease progression of colorectal cancer. Created using a template on BioRender.com.
Figure 6.
Disease progression of colorectal cancer. Created using a template on BioRender.com.

Figure 7.
(a) Illustrative location of H. pylori in gastric mucosal. (b) Virulence factors that heighten cancer development (Chmiela et al. [55]).
Figure 7.
(a) Illustrative location of H. pylori in gastric mucosal. (b) Virulence factors that heighten cancer development (Chmiela et al. [55]).

Figure 9.
Treatment strategies for CRC. Created with BioRender.com.
Figure 9.
Treatment strategies for CRC. Created with BioRender.com.

Figure 10.
The pH approach to CRC drug delivery. Created with BioRender.com.
Figure 10.
The pH approach to CRC drug delivery. Created with BioRender.com.

Figure 11.
A description of the microbiota-based drug delivery. Created with BioRender.com.
Figure 11.
A description of the microbiota-based drug delivery. Created with BioRender.com.
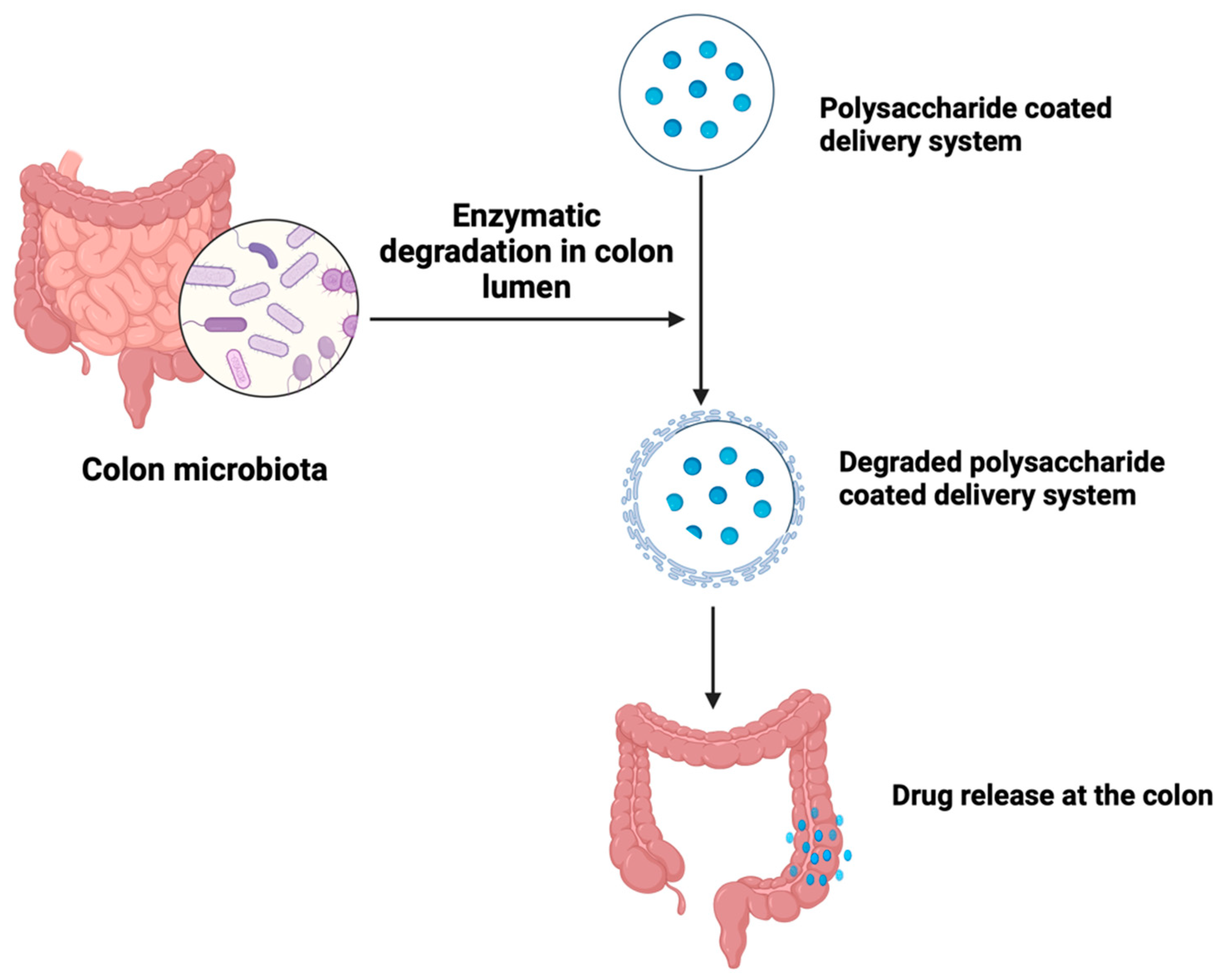
Figure 12.
A description of an antibody–drug conjugate (A) and peptide–drug conjugate (B). Created with BioRender.com.
Figure 12.
A description of an antibody–drug conjugate (A) and peptide–drug conjugate (B). Created with BioRender.com.
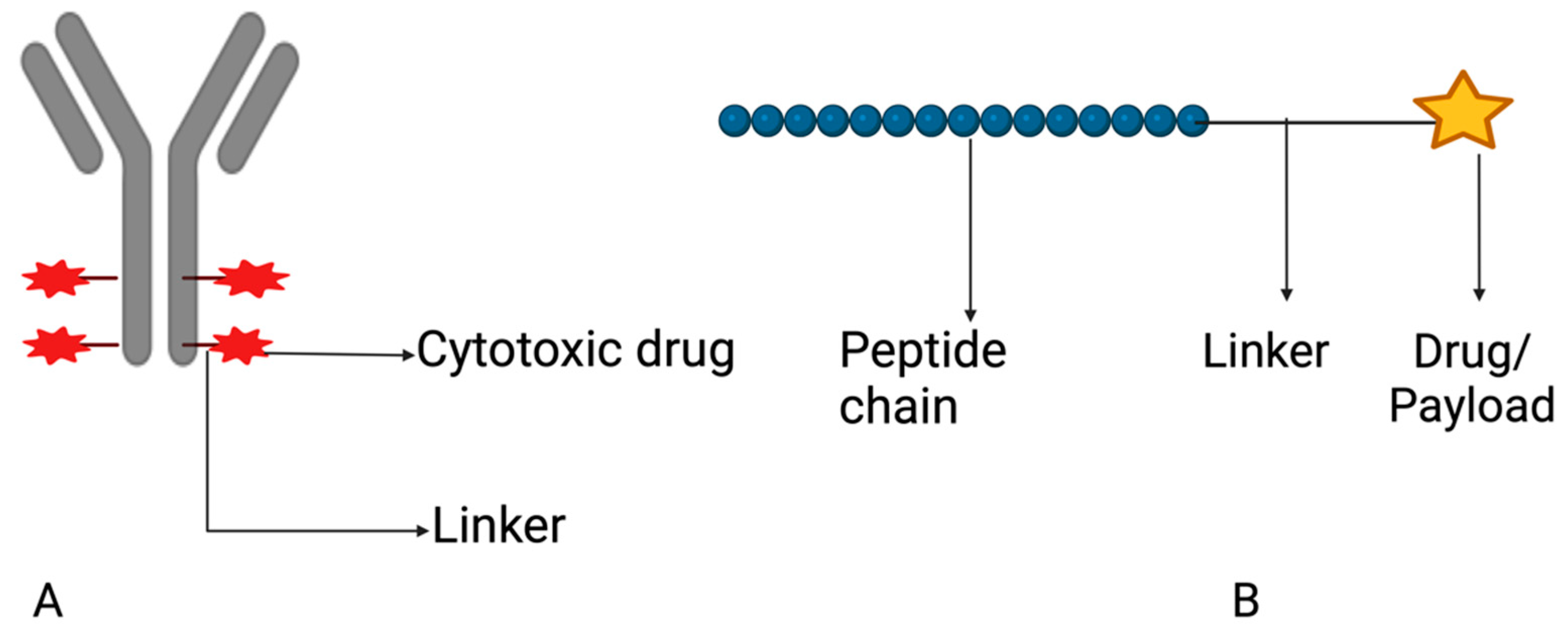
Figure 13.
Various possible sizes of niosomes. Created with BioRender.com.
Figure 13.
Various possible sizes of niosomes. Created with BioRender.com.

Figure 14.
A polymeric nanoparticle for drug delivery. Created with BioRender.com.
Figure 14.
A polymeric nanoparticle for drug delivery. Created with BioRender.com.

Table 3.
Drug-loaded vesicular system currently in clinical trial.
| Vesicular System | Payload | Phase of Study | Clinical Trial Identifier | Sponsor |
|---|---|---|---|---|
| Liposome | Irinotecan and Bevacizumab | I | NCT05854498 | University of Wisconsin (Madison, WI, USA) |
| Irinotecan-based FOLFIRI combined with Bevacizumab | II | NCT05969899 | Fudan University (Shanghai, China) | |
| Fluorouracil and Irinotecan and Leucovorin | I, II | NCT03337087 | Academic and Community Cancer Research United (Rochester, MN, USA) | |
| Polymeric nanoparticle | Cetuximab | I | NCT03774680 | Al-Azhar University (Cairo, Egypt) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Adebayo, A.S.; Agbaje, K.; Adesina, S.K.; Olajubutu, O. Colorectal Cancer: Disease Process, Current Treatment Options, and Future Perspectives. Pharmaceutics 2023, 15, 2620. https://doi.org/10.3390/pharmaceutics15112620
AMA Style
Adebayo AS, Agbaje K, Adesina SK, Olajubutu O. Colorectal Cancer: Disease Process, Current Treatment Options, and Future Perspectives. Pharmaceutics. 2023; 15(11):2620. https://doi.org/10.3390/pharmaceutics15112620
Chicago/Turabian StyleAdebayo, Amusa S., Kafilat Agbaje, Simeon K. Adesina, and Oluwabukunmi Olajubutu. 2023. "Colorectal Cancer: Disease Process, Current Treatment Options, and Future Perspectives" Pharmaceutics 15, no. 11: 2620. https://doi.org/10.3390/pharmaceutics15112620
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.