1. Introduction
Respiratory diseases are amongst the leading causes of morbidity and mortality worldwide. Some of the most common include asthma, pneumonia, chronic obstructive pulmonary disease (COPD), acute respiratory distress syndrome (ARDS), tuberculosis (TB), and cystic fibrosis (CF). According to the WHO, in 2017, 544.9 million people worldwide had a chronic respiratory disease [
1]. Treatment can vary depending on severity; however, in most cases some form of respiratory support will be required to alleviate symptoms. The level of support can vary between invasive and non-invasive depending on the condition of the patient; it is delivered via endotracheal tube (ETT), tracheostomy tube (TT), mask, nasal cannula, or mouthpiece. High flow oxygen (HFO) therapy has become an increasingly implemented form of respiratory support as it can be used in both the hospital and homecare setting, improves patient oxygenation, reduces the work of breathing, and allows for concurrent delivery of aerosolised therapeutics for targeted treatment [
2,
3,
4,
5].
Numerous bench studies [
6,
7,
8,
9,
10] and clinical data sets [
11,
12,
13,
14,
15] have contributed to our understanding of the factors that influence aerosol drug delivery during HFO therapy. In a recent review paper of HFO therapy, Li et al. [
16] summarised the current state of the art knowledge in terms of the main factors influencing aerosol drug delivery. These include gas flow rate, gas density, dry versus humidified gas, gas type, delivery interface, position of the nebuliser in the circuit, nebuliser type, gas flow/patient’s inspiratory flow (GF/IF) ratio, open mouth versus closed mouth breathing, and control of aerosol generation during breathing. Of these, the authors concluded that GF/IF ratio, nebuliser type, and position in the circuit were the most important factors in maximising concurrent aerosol delivery. Vibrating mesh nebulisers (VMNs) were found to deliver the greatest quantities of aerosol; they should be placed at the inlet of the humidifier pot and GF/IF should be kept to 0.5 or lower. Bennett et al. had similar findings but concluded that the nebuliser should be placed at the exit of the humidifier pot in order to maximise the aerosol performance of a HFO therapy system [
17].
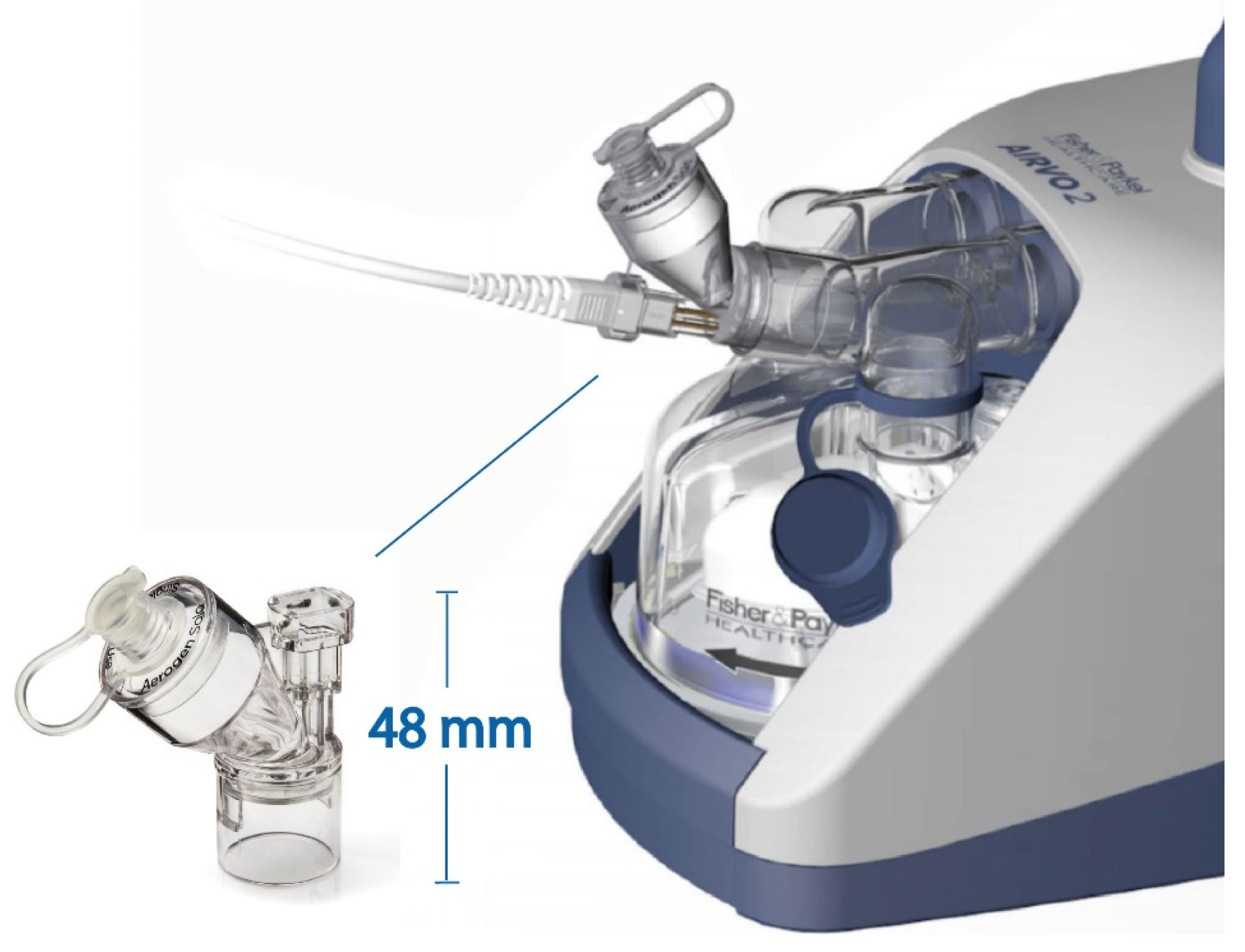
While there are numerous different HFO therapy systems on the market, the most frequently encountered is the Airvo 2
TM manufactured by Fisher & Paykel. It can be used in both the critical and homecare environments and can deliver heated, humidified supplemental gas flows suitable for infant, paediatric, and adult patients. It is also one of the few HFO therapy system that has a bespoke nebuliser adapter. The Airvo Neb adapter, the output of a collaboration between Fisher & Paykel and Aerogen, was designed to maximise concurrent aerosol delivery. This adapter integrates the Aerogen Solo
TM VMN into the humidifier pot, where the aerosol is entrained into the heated, humidified gas flow exiting the pot. Although this system is frequently cited in the literature, there are conflicting reports on the levels of aerosol delivery at both system and patient level. For example, in studies that have used nasal cannulas, Li et al. [
7] reported inhaled doses (%) of 2.7–12%, Murphy et al. [
18] 1.37–15.72%, and Bennett et al. [
19] up to 28.95% in adults. In similar bench studies for paediatrics, Wang et al. [
20] measured tracheal doses (%) between 1.48–3.92%, Réminiac et al. [
21] 0.52–4.15%, and Bennett et al. [
19] up to 13.54%.
A useful feature of the Airvo2
TM system is its compatibility with tracheostomy tubes, which allows it to provide HFO to patients who have bypassed upper airways. Tracheostomy is commonly performed due to either pulmonary insufficiency or due to upper airway obstructions [
22]. Similar to HFO therapy via nasal cannula, there have been a number of in-vitro studies that examined means of optimising aerosol therapy delivered through a tracheostomy tube. Nebuliser type and circuit arrangement were found to significantly affect aerosol delivery [
10,
23,
24,
25,
26,
27]. The use of VMN incorporated via T-pieces rather than tracheostomy collars was the recommended option. However, there still exists a risk of accidental decannulation from the additional weight on the tracheostomy tube [
28]. The Airvo
2TM system, with its bespoke nebuliser adapter and tracheostomy interface, allows a direct connection of the system to the tracheostomy tube, eliminating the need for additional circuit components, potential decannulation, and unwanted dead space. To the best of the authors’ knowledge, neither in vitro nor in vivo data exist on the levels of aerosol delivery possible with this interface.
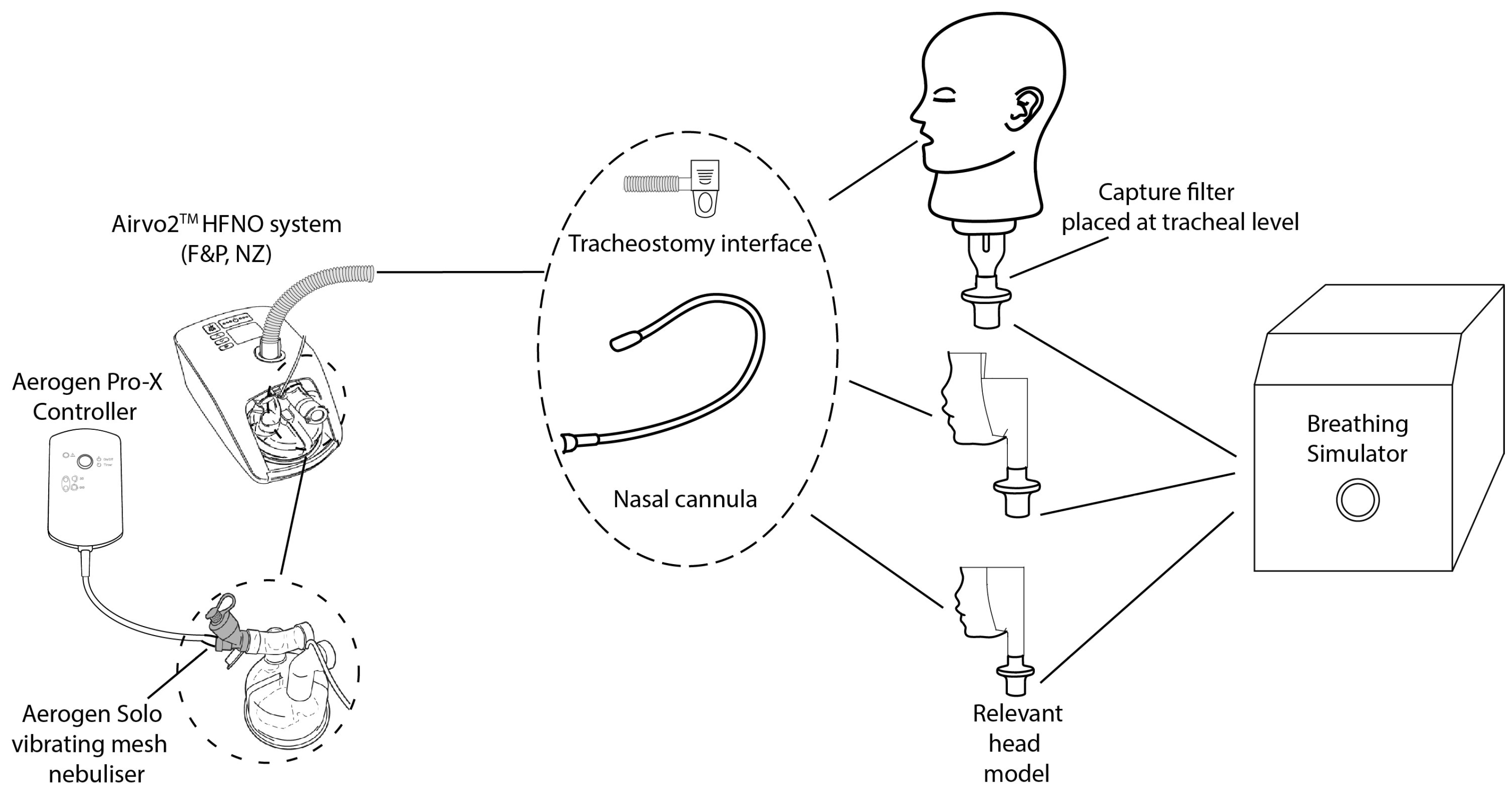
The objective of this study was to perform a comprehensive characterisation of the Airvo2TM HFO system delivering concurrent aerosol therapy with its recommended nebuliser, the Aerogen SoloTM. This includes both a system and simulated patient characterisation across a comprehensive suite of products, including the previously unreported tracheostomy interface, at the recommended operating ranges.
4. Discussion
In this study, we completed a full performance characterisation of the Airvo2TM HFO therapy system in combination with the Aerogen SoloTM VMN. Variations in the emitted dose (%), tracheal dose (%), MMAD, and GSD with changes in supplemental gas flow rate, interface, and nasal cannula size were documented across the infant, paediatric, and adult ranges, as well as breathing profiles.
In a study examining the parameters affecting the performance of high flow nasal therapy systems providing concurrent aerosol therapy, Bennett et al. found that to maximise the aerosol dose emitted, the supplemental gas flow rate should be kept low, the aerosol droplet size should be kept small, and the nebuliser should be positioned immediately after the humidification chamber [
17]. Two of these factors, aerosol droplet size and nebuliser position, were kept constant throughout this study, while the nasal cannula size and supplemental gas flow rates were varied.
As expected and in line with the numerous published studies that have examined trans-nasal aerosol delivery via HFO in the literature, supplemental gas flow rate was found to have an inverse relationship with the emitted and tracheal doses (%), irrespective of cannula size in the adult range,
p ≤ 0.05 [
18,
33,
34]. Cannula size was found to have a significant impact on both the emitted and tracheal doses (%) at supplemental gas flow rates of 30 LPM and below. Greater emitted and tracheal doses (%) were measured when the OPT946 was used at each flow rate considered as shown in
Figure 4a,
Figure 5a, and
Tables S1 and S3 supplementary data, most likely due to the larger inner bore diameter of the OPT946 cannula, 6.0 mm ID versus 5.1 mm ID for the OPT944 and 4.2 mm ID for the OPT942. Smaller dimensions of the tubing and cannula components will hinder the exit of aerosol from the cannula during HFNO [
35]. Similar trends to those reported here have been documented previously in the literature with this and other HFO therapy systems [
4,
17,
18,
34,
35,
36].
The data generated using the paediatric cannulas and settings follows the same trends as the adult data and other HFNO therapy paediatric studies in the literature [
20,
21]; increases in supplemental gas flow rate result in decreases in emitted and tracheal doses (%), as shown in
Figure 4b and
Figure 5b. Increasing cannula size from 2.9 mm ID OPT318 to 3.3 mm ID OPT418 had no significant effect on the emitted dose (%) below 25 LPM,
p ≥ 0.05. However, at the lowest flow rate, 2 LPM, cannula size did have a significant effect on the tracheal dose (%),
supplementary data Table S4,
p ≤ 0.05. This is most likely due to losses in the head model. Interestingly, there were some key differences in the emitted and tracheal dose (%) data trends in the infant models OPT 316 and OPT416. While both decrease with increasing gas flow rate, 2–20 LPM, from 30.24–25.71% emitted and 8.11–4.45% tracheal OPT316 and from 31.64–25.46% emitted and 8.14–4.46% tracheal OPT416, both the emitted and tracheal doses (%) were significantly greater at 20 LPM than 11 LPM. In similar studies with the same infant head model SAINT, neither Wang et al. [
20] nor Réminiac et al. [
21] observed this phenomena. However, neither study extended the flow rate above 8 LPM. It is possible that at the higher gas flow rate, significant aerosol coalescence occurs and passes through the circuit to the collection filters. In a clinical setting, flows at this rate would most likely not be tolerated by the respective patient cohort and the findings here would serve to inform a clinical practice about reducing the gas flow rate during concurrent aerosol therapy in a HFNO therapy patient [
37].
The opposite trends were found in the infant models OPT316 and OPT416, where above 2 LPM cannula ID had no significant effect on the emitted dose (%),
p ≥ 0.05,
supplementary data Table S2, and had no significant effect on the tracheal dose (%),
p ≥ 0.05,
supplementary data Table S4. Given that the infant cannula OPT316 and OPT416 had the smallest ID nares, 2.5 mm and 2.9 mm, respectively, and the smaller airway passages in the head model, this result is unsurprising. A recent scintigraphy study in infants reported values of 4.5 ± 2.2% deposition at a flow rate of 2 LPM using the same VMN [
38]. The present study recorded values of 8.10 ± 0.85% with the OPT316 cannula and 8.14 ± 0.74% with the OPT416 cannula. The overestimation of our in vitro data is to be expected as the filters do not allow for the exhalation of aerosols that are not deposited.
As noted in the introduction, to the best of the authors’ knowledge, there are neither in vivo nor in vitro studies that have detailed the aerosol delivery from the Airvo2
TM HFO therapy system where the bespoke nebuliser adapter and tracheostomy interface were used. Standard clinical practice incorporates a nebuliser into the respiratory circuit using a T-piece or tracheostomy collar. As such, there is no direct comparison possible between the data presented in this study with previous studies in the literature. Hence, the data presented in this study is the first to evaluate aerosol delivery via this means. Emitted and tracheal dose (%) data pertaining to the tracheostomy interface OPT970 follows the same trends as the nasal cannula data. Increases in supplemental gas rates cause a significant reduction in both the emitted and tracheal dose (%) measured. The emitted and tracheal doses (%) decrease from 9.38 ± 0.37% and 4.75 ± 0.53% at 10 LPM to 2.21 ± 0.31% and 0.40 ± 0.08% at 50 LPM. The low delivery efficiency compared to the nasal cannula—for example the OPT942 tracheal dose was 18.75 ± 0.83% at 10 LPM—is unsurprising given the design of the interface. The openings at the exit of the interface prior to the connection with the tracheostomy tube are a major source of aerosol loss. The use of a tracheostomy tube should result in a greater level of aerosol delivery as it bypasses the upper airways (naso/oropharynx and hypopharynx) where there is significant filtering and deposition of larger aerosol particles, increased resistance, and dead space [
24].
MMAD is considered to be the optimal laboratory-based method to predict possible aerosol distribution within the lungs. It is the diameter that is larger than 50% of the aerosolised droplets and smaller than the remaining 50%, based on mass. In general, particles < 5 µm in diameter are considered suitable for inhaled drug delivery, with larger diameter droplets preferring to deposit in the upper airways [
39,
40]. The aerosol droplet sizes exiting the range of interfaces was consistently lower than that produced by the nebuliser, 4.11 ± 0.06 µm,
Table 5 and
Table 6. As the supplemental gas flow rate increased, the aerosol droplet diameter decreased significantly across the range of nasal and tracheostomy adult interfaces tested. This reduction is most likely caused by inertial impaction of the larger diameter aerosol droplets within the HFO therapy system and the cannula; thus, only the smaller diameter aerosol droplets can successfully transit through to the exit of the interfaces. Furthermore, at flow rates > 30 LPM, cannula diameter had a significant effect on the diameter of the aerosol droplets,
p ≤ 0.05. These findings are consistent with those of both Bennett et al. [
17] and Bhashyam et al. [
41]. Cannula size had no significant effect on the aerosol droplet size exiting the paediatric and infant cannulas. Increases in supplemental gas flow and cannula diameter had no significant effect on the aerosol droplet size at the exit of the paediatric nares,
p ≥ 0.05. This is most likely due to the filtering effect of the small diameter nares limiting the emission of the larger diameter particles, e.g., OPT 318 has a 2.9 mm ID and OPT418 has an ID of 3.3 mm. Contrasting aerosol droplet size trends were found when using the infant sized nares; as supplemental gas flow increased from 2–20 LPM, the aerosol droplet size increased. This was also reported in studies performed by Perry et al. [
34] and Reminiac et al. [
21]. The infant nares OPT 316 and OPT 416 have smaller internal diameters of 2.5 mm ID OPT316 and 2.9 mm ID OPT416, respectively, and should, in theory, have the smallest aerosol droplet diameters exiting the nares, particularly at the higher flow rates. The increase in aerosol droplet diameter with increasing flow rate may occur due to increased levels of rained-out humidity that occur within the smaller tubing and nares which would artificially increase the droplet size measurements.
There are several limitations to this study. In line with international test standards, e.g., ISO27427 and the FDA guidance, tracheal doses (%) were assessed with breathing patterns associated with simulated healthy adults, infants, and paediatrics. However, recipients of HFO therapy would, most likely, not present with such breathing patterns. Breath pattern has been shown to affect the delivered dose, and as such, whilst this can be considered a gold standard data set describing the performance of the Airvo2 and Aerogen Solo combination, differences may be expected in the clinical setting. There are a number of different designs of nasal cannula in use in the critical and home care setting, including the asymmetrical nasal cannula. These new designs offer greater patient comfort and airway CO2 removal. However, there are few studies that have examined their effect on aerosol delivery. This study was completed using atmospheric air containing 21% oxygen. However, in certain clinical situations, blends are used to deliver a higher oxygen concentration. Studies are required to determine the effects, if any, of higher oxygen concentrations and other blended carrier gasses on aerosol delivery to different patient types and cohorts.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}