
An Inclusive Civil Society Dialogue for Successful Implementation of the EU HTA Regulation: Call to Action to Ensure Appropriate Involvement of Stakeholders and Collaborators

 , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. The EAA Convention Format: Public Session and Stakeholder-Centered Working Groups
2.2. Procedural Approach of the Working Groups
2.3. Plenary Session and Ranking
2.4. Data Handling and Analysis
3. Results
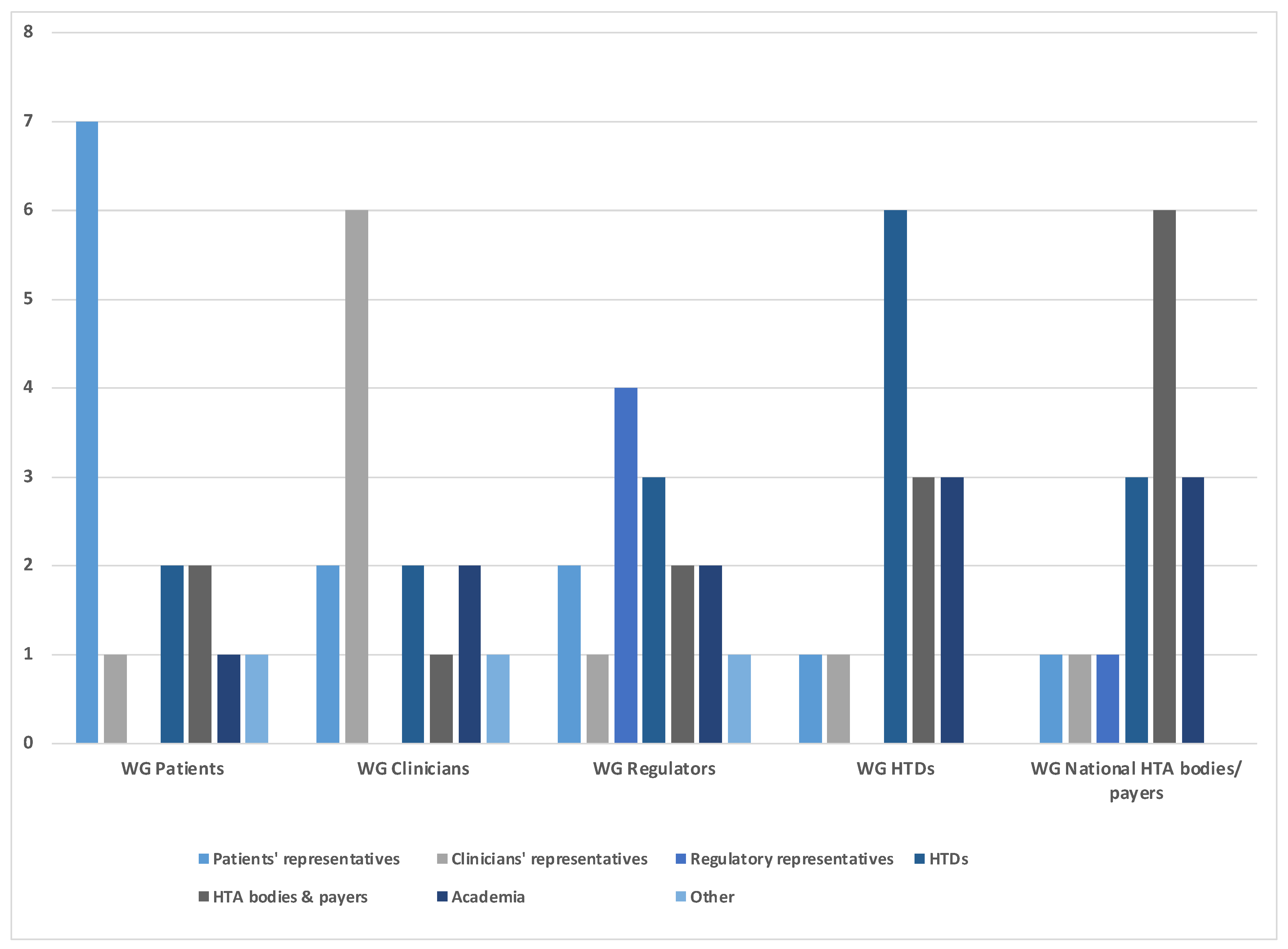
3.1. Stakeholder-Centered Working Groups at the EAA Convention
3.2. Characteristics of Role Profiles and Related Challenges
- Patients and patient representatives, as the end users of the health technology that is being assessed, should be considered equal-level stakeholders to be involved throughout the whole HTA process and advising on the medical and symptomatic context. Specific challenges identified for patients to fulfill this role include lack of resources/unreadiness, funding, management of conflicts of interest, educational needs, and inconsistent recognition of the value of patient input.
- Clinicians and medical societies are key advisers for incorporating clinical expertise in the HTA process. This not only includes context of the disease and medical and/or scientific background, the actual bedside experience and expertise on treatment algorithms and standard of care, but also research and methodological expertise. To fulfill their role, capacity would need to be built up, educational efforts with a focus on methodological expertise are required, and conflicts of interest should be handled transparently.
- Regulators are collaborators rather than stakeholders in the evolving EU HTA process, having different although related remits than HTA bodies. Key challenges experienced in the regulatory/HTA collaboration include capacity constraints to conduct parallel scientific consultations, confidentiality arrangements (e.g., in the context of providing information to support HTA processes), and expert involvement across regulatory and HTA reviews in light of different conflict-of-interest rules.
- HTDs contribute the evidence package for the HTA assessment. A concern was raised pertaining to available slots for the JSC being scarce and HTDs appearing to be informed rather than consulted during the currently proposed JCA procedure. Further, the timelines within the process, as currently defined, are very short. Not allowing HTDs to provide key content feedback at the European level may hinder the opportunity to reduce duplicate work at the national level. Together, the long-term goal of simplifying and harmonizing the HTA process might be missed, especially when a multiplicity of PICO data requirements may create additional complexity.
3.3. Most Important Actions per Stakeholder/Collaborator Group
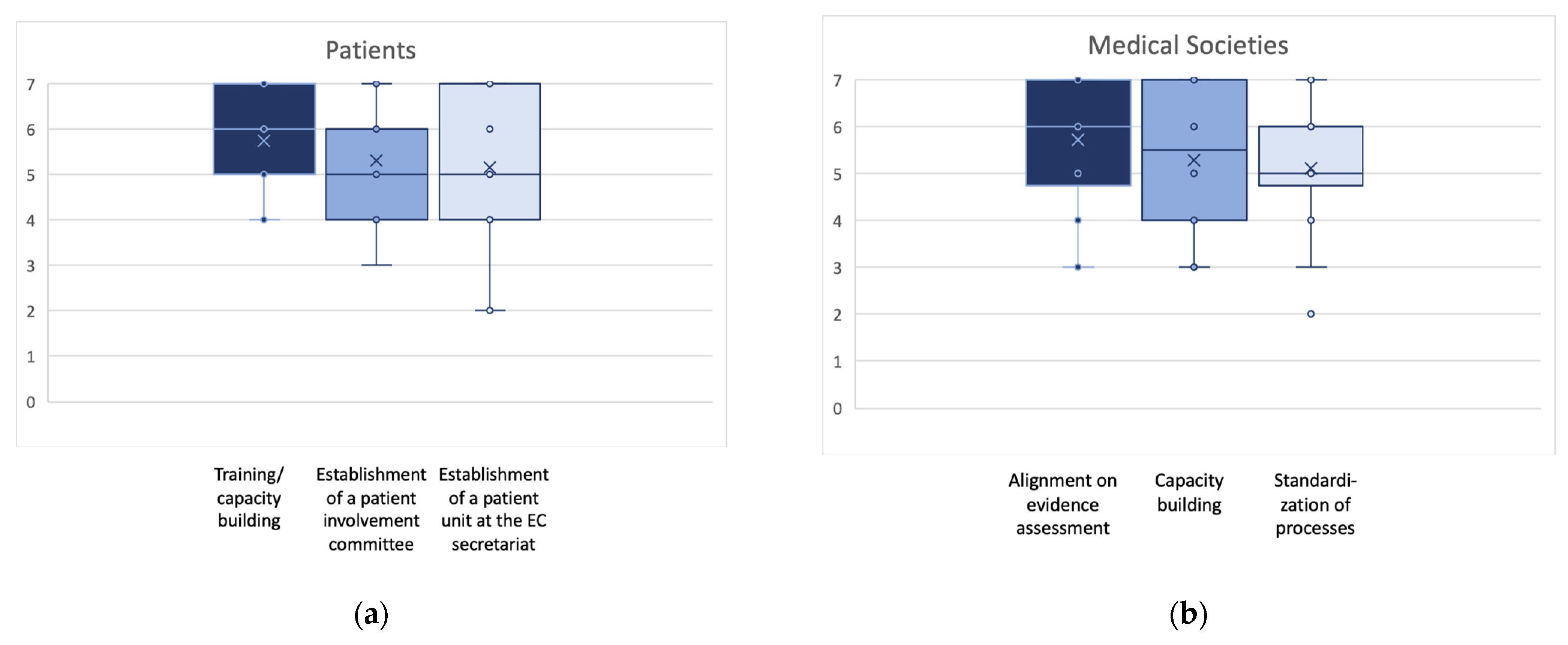
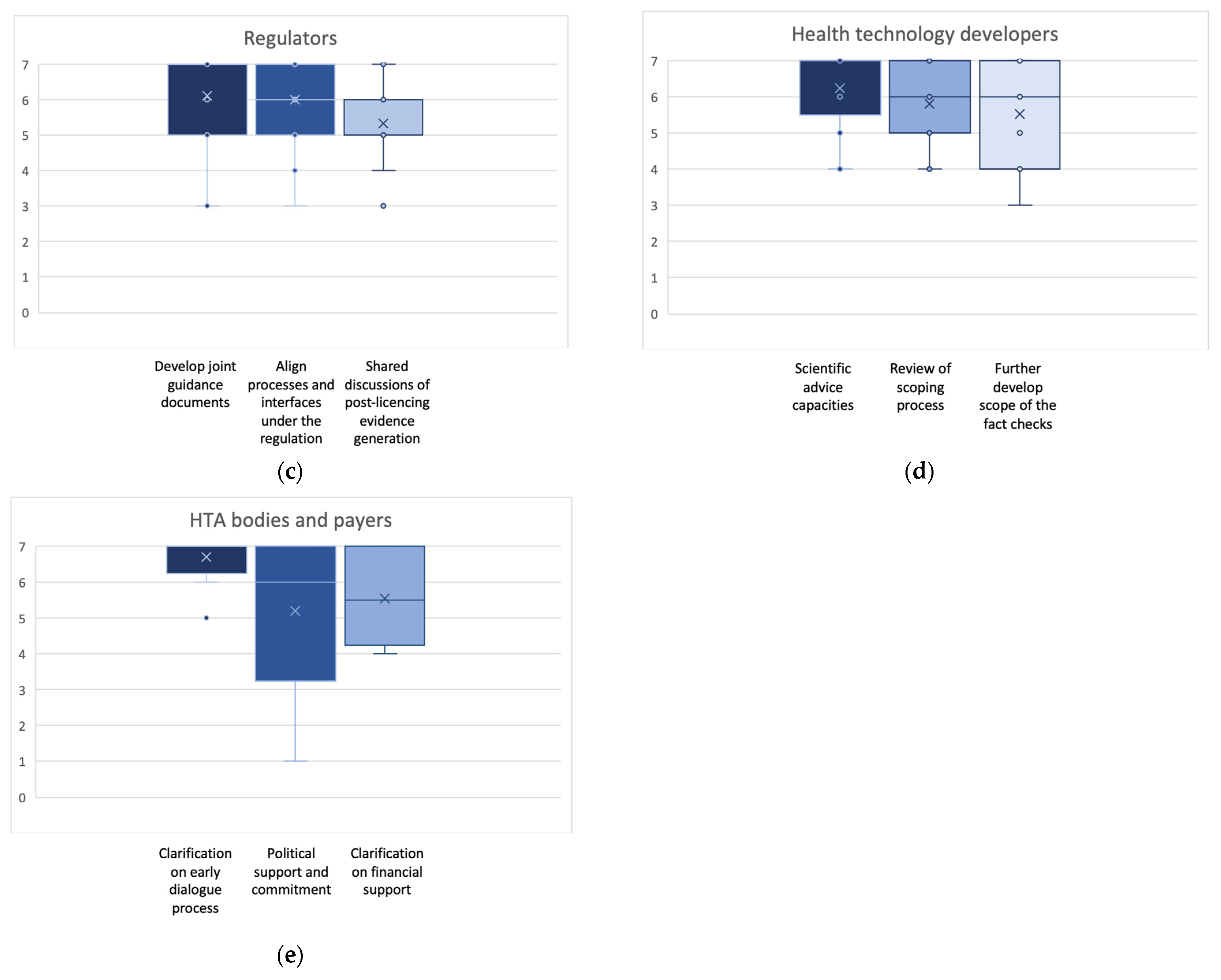
- Capacity-related actions and clarification on financial support were raised by patients’, clinicians’, regulatory, and national HTA bodies’ representatives. Furthermore, patients’ representatives asked for a structural base of involvement (the patient unit at the European Commission (EC) with the establishment of a patient involvement committee), and national HTA bodies’ representatives asked for clarity on political support and commitment.
- Process-related actions were raised by clinicians’ representatives (standardization of EU HTA processes), regulatory representatives (alignment of regulatory and HTA processes and interfaces; development of joint guidance documents between regulators and HTA), HTDs (review of the PICO scoping process; further development of the assessment report fact-checking process; availability of scientific advice at scale), and national HTA bodies’ representatives (clarification on the early dialogue process; clarification on designing and establishing the interface of national vs. EU-level processes).
- Methodological issues requiring action were raised by clinicians (alignment on evidence assessment), regulatory representatives (shared discussions on post-launch evidence generation (PLEG)), and HTD representatives (elements of PICO, including data requirements and harmonization).
- Training and educational actions were highlighted by patients’, clinicians’, and national HTA bodies’ representatives.
3.4. Prioritization of Actions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Directorate-General for Health and Food Safety. Overview. 2023. Available online: https://health.ec.europa.eu/health-technology-assessment/overview_en (accessed on 10 January 2024).
- World Health Organization. Health Technology Assessment. Available online: https://www.who.int/health-topics/health-technology-assessment#tab=tab_1. (accessed on 10 January 2024).
- Gozzo, L.; Paterson, K.; Wong, O.; Megerlin, F.; Geldmacher, J.; Popoli, P.; Jommi, C.; Fricke, F.-U.; De Solà-Morales, O.; Kamae, I.; et al. Towards a European harmonization of health technology assessment recommendations executive paper of European regulatory conference focused on the EU commission proposal to harmonize HTA. Front. Drug Saf. Regul. 2022, 2, 970661. [Google Scholar] [CrossRef]
- Drummond, M.; Tarricone, R.; Torbica, A. European union regulation of health technology assessment: What is required for it to succeed? Eur. J. Health Econ. 2022, 23, 913–915. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Health Technology Assessment: Commission Welcomes the Adoption of New Rules to Improve Access to Innovative Technologies 2021. Available online: https://ec.europa.eu/commission/presscorner/detail/en/IP_21_6771 (accessed on 10 January 2024).
- The European Parliament and the Council of the European Union. Regulation (EU) 2021/2282 of the European Parliament and of the Council of 15 December 2021 on Health Technology Assessment and amending Directive 2011/24/EU2021 22.12.2021. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32021R2282&from=EN (accessed on 10 January 2024).
- Kristensen, F.B.; Mäkelä, M.; Neikter, S.A.; Rehnqvist, N.; Håheim, L.L.; Mørland, B.; Milne, R.; Nielsen, C.M.; Busse, R.; Lee-Robin, S.H.; et al. European network for health technology assessment, EUnetHTA: Planning, development, and implementation of a sustainable European network for health technology assessment. Int. J. Technol. Assess. Health Care 2009, 25 (Suppl. S2), 107–116. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, C.P.; Lauritsen, S.W.; Kristensen, F.B.; Bistrup, M.L.; Cecchetti, A.; Turk, E. Involving stakeholders and developing a policy for stakeholder involvement in the European network for Health Technology Assessment, EUnetHTA. Int. J. Technol. Assess. Health Care 2009, 25, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Julian, E.; Gianfrate, F.; Sola-Morales, O.; Mol, P.; Bergmann, J.F.; Salmonson, T.; Ruof, J. How can a joint European health technology assessment provide an ‘additional benefit’ over the current standard of national assessments? Insights generated from a multi-stakeholder survey in hematology/oncology. Health Econ. Rev. 2022, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Julian, E.; Pavlovic, M.; Sola-Morales, O.; Gianfrate, F.; Toumi, M.; Bucher, H.C.; Dierks, C.; Greiner, W.; Mol, P.; Bergmann, J.-F.; et al. Shaping a research agenda to ensure a successful European health technology assessment: Insights generated during the inaugural convention of the European access academy. Health Econ. Rev. 2022, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Cardone, A.; van Dyck, W.; Ermisch, M.; Gianfrate, F.; Hebborn, A.; Julian, E.; Pavlovic, M.; Peters, S.; Price, R.; Ruof, J.; et al. (Eds.) Europe’s Evolving HTA Regulation & It’s Relevance for ‘Beating Cancer’; EAA Convention Proceedings Volume 1; Copenhagen University: København, Denmark; The European Access Academy: Basel, Switzerland, 2022. [Google Scholar]
- Bernardini, R.; Berntgen, M.; Van De Casteele, M.; Desmet, T.; Dierks, C.; van Dyck, W.; Giuliani, R.; Goettsch, W.; Guardian, M.; Van Haesendonck, L.; et al. (Eds.) Stakeholder Involvement & Europe’s Evolving HTA Framework; EAA Convention; Vlerick Business School: Brussels, Belgium; The European Access Academy: Basel, Switzerland, 2022. [Google Scholar]
- Van Haesendonck, L.; Ruof, J.; Desmet, T.; Van Dyck, W.; Simoens, S.; Huys, I.; Giuliani, R.; Toumi, M.; Dierks, C.; Dierks, J.; et al. The role of stakeholder involvement in the evolving EU HTA process: Insights generated through the European Access Academy’s multi-stakeholder pre-convention questionnaire. J. Mark. Access Health Policy 2023, 11, 2217543. [Google Scholar] [CrossRef] [PubMed]
- Role 2023. Available online: https://dictionary.cambridge.org/dictionary/english/role (accessed on 10 January 2024).
- European Commission. Pharmaceutical Strategy for Europe 2020. Available online: https://health.ec.europa.eu/system/files/2021-02/pharma-strategy_report_en_0.pdf (accessed on 10 January 2024).
- Cavazza, M.; Jommi, C. Stakeholders involvement by HTA Organisations: Why is so different? Health Policy 2012, 105, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Wale, J.L.; Thomas, S.; Hamerlijnck, D.; Hollander, R. Patients and public are important stakeholders in health technology assessment but the level of involvement is low—A call to action. Res. Involv. Engagem. 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Vokó, Z.; Cheung, K.L.; Józwiak-Hagymásy, J.; Wolfenstetter, S.B.; Jones, T.; Muñoz, C.; Pokhrel, S. Similarities and Differences between Stakeholders’ Opinions on Using HTA Information Across Five European Countries; Gildeprint: Maastricht, The Netherlands, 2023. [Google Scholar]
- Mitchell, G.R.; Hartelius, E.J.; McCoy, D.; McTigue, K.M. Deliberative Stakeholder Engagement in Person-centered Health Research. Social Epistemol. 2022, 36, 21–42. [Google Scholar] [CrossRef]
- Oortwijn, W.; Husereau, D.; Abelson, J.; Barasa, E.; Bayani, D.; Canuto Santos, V.; Culyer, A.; Facey, K.; Grainger, D.; Kieslich, K.; et al. Designing and Implementing Deliberative Processes for Health Technology Assessment: A Good Practices Report of a Joint HTAi/ISPOR Task Force. Value Health 2022, 25, 869–886. [Google Scholar] [CrossRef] [PubMed]
- Stakeholders and Communication Division. Engagement Framework: EMA and Patients, Consumers and Their Organisations. EMA/649909/2021:[8 p.]. 2022. Available online: https://www.ema.europa.eu/en/documents/other/engagement-framework-european-medicines-agency-patients-consumers-their-organisations_en.pdf (accessed on 10 January 2024).
- Dierks, C.; Grimalauskas, A. Options of patient participation—A view of the legal framework. In Patients and Medical Societies: Additional Expertise for AMNOG; Interdisciplinary platform on benefit assessment; Staeck, F., van den Bergh, W., Eds.; Springer Medizin Verlag GmbH: Berlin, Germany, 2021; Volume 13, pp. 10–13. [Google Scholar]
- Schulz-Asche, K. The role of patients in the AMNOG procedure from the Green’s point of view. In Patients and Medical Societies: Additional Expertise for AMNOG; Interdisciplinary platform on benefit assessment; Staeck, F., van den Bergh, W., Eds.; Springer Medizin Verlag GmbH: Berlin, Germany, 2021; Volume 13, pp. 8–9. [Google Scholar]
- Danner, M. Patients in the early benefit assessment—A field report. In Patients and Medical Societies: Additional Expertise for AMNOG; Interdisciplinary platform on benefit assessment; Staeck, F., van den Bergh, W., Eds.; Springer Medizin Verlag GmbH: Berlin, Germany, 2021; Volume 13, pp. 14–17. [Google Scholar]
- Schlegl, E.; Ducournau, P.; Ruof, J. Different Weights of the Evidence-Based Medicine Triad in Regulatory, Health Technology Assessment, and Clinical Decision Making. Pharm. Med. 2017, 31, 213–216. [Google Scholar] [CrossRef] [PubMed]
- ESMO. ESMO-Magnitude of Clinical Benefit Scale 2023. Available online: https://www.esmo.org/guidelines/esmo-mcbs (accessed on 10 January 2024).
- Cherny, N.I.; Sullivan, R.; Dafni, U.; Kerst, J.M.; Sobrero, A.; Zielinski, C.; de Vries, E.G.E.; Piccart, M.J. A standardised, generic, validated approach to stratify the magnitude of clinical benefit that can be anticipated from anti-cancer therapies: The European Society for Medical Oncology Magnitude of Clinical Benefit Scale (ESMO-MCBS). Ann. Oncol. 2015, 26, 1547–1573. [Google Scholar] [CrossRef] [PubMed]
- Cherny, N.I.; Dafni, U.; Bogaerts, J.; Latino, N.J.; Pentheroudakis, G.; Douillard, J.Y.; Tabernero, J.; Zielinski, C.; Piccart, M.J.; de Vries, E.G.E. ESMO-Magnitude of Clinical Benefit Scale version 1.1. Ann. Oncol. 2017, 28, 2340–2366. [Google Scholar] [CrossRef] [PubMed]
- Kiesewetter, B.; Dafni, U.; de Vries, E.G.E.; Barriuso, J.; Curigliano, G.; González-Calle, V.; Galotti, M.; Gyawali, B.; Huntly, B.J.P.; Jäger, U.; et al. ESMO-Magnitude of Clinical Benefit Scale for haematological malignancies (ESMO-MCBS:H) version 1.0. Ann. Oncol. 2023, 34, 734–771. [Google Scholar] [CrossRef] [PubMed]
- Wörmann, B. Medical societies in the AMNOG procedure—A “non-quantifiable benefit”? In Patients and Medical Societies: Additional Expertise for AMNOG; Interdisciplinary platform on benefit, assessment; Staeck, F., van den Bergh, W., Eds.; Springer Medizin Verlag: Berlin, Germany, 2021; Volume 13, pp. 26–35. [Google Scholar]
- European Medicines Agency. European Collaboration between Regulators and Health Technology Assessment Bodies Joint Work Plan (2021–2023) between EMA and European HTA Bodies Facilitated through EUnetHTA212022; EMA/188201/2022:[7 p.]. Available online: https://www.ema.europa.eu/en/documents/work-programme/european-collaboration-between-regulators-health-technology-assessment-bodies-joint-work-plan-2021_en.pdf (accessed on 10 January 2024).
- Lobker, W.; Broich, K. Harmonised HTA Assessment: Experiences on the Way to Centralised Approval. European Benefit Assessment—Opportunities and Risks; Interdisciplinary platform on benefit assessment; Springer Medizin Verlag: Berlin, Germany, 2019; Volume 8, pp. 46–53. [Google Scholar]
- EFPIA. Joint Statement Pharmaceutical Industry Concerns over the Implementation of the EU HTA Regulation 2022. Available online: https://www.efpia.eu/news-events/the-efpia-view/statements-press-releases/joint-statement-pharmaceutical-industry-concerns-over-the-implementation-of-the-eu-hta-regulation/ (accessed on 10 January 2024).




{kind=link}
{kind=link}
{kind=link}
| Stakeholder/Collaborator | Role |
|---|---|
| Patients | Patients are independent “equal level” stakeholders that should be involved throughout the EU HTA process (i.e., not only in the content, such as specific input on a specific product), including governance, decision-making, dissemination, and advocacy. Involvement both on an EU and national level is important. |
| Clinicians | Clinicians are to be engaged as advisors adding expertise to the process by:
|
| Regulators | Regulatory and HTA bodies have different remits. Regulators collaborate with HTA bodies but are not stakeholders in the meaning of the EU HTA Regulation. Collaboration includes: Contribution throughout the implementation to
|
| HTDs | HTDs develop innovative medicines and provide evidence that allows HTA agencies to conduct a solid and unbiased assessment of the value of the innovation. While communication with HTA agencies to ensure the appropriateness of the submitted evidence is required, this is limited to ensure the independence of HTAs is maintained. Both on a generic methodological level (e.g., input into methodological guidelines) and an applied product-specific level, HTDs contribute scientific excellence throughout the process. HTDs support embedding the EU assessment reports into national appraisals and are addressing any remaining uncertainty. |
| National HTA bodies and payers | National Expertise Centers of Excellence have a dual role, both as drivers and producers of reports and as users of the EU HTA assessments. National Centers participate in designing and setting up the EU HTA organization and governance structure. They further participate in developing the operational guidelines and they review their internal organization and processes in order to avoid duplication of tasks already performed at the EU level. |
| Stakeholder/Collaborator | Identified Activities |
|---|---|
| Patients | Training/capacity building and related funding for patient representatives Establish a patient involvement committee (may be part of the EU HTA Stakeholder Network) to define rules, procedures, templates, and methodology for patient input Establish a dedicated “patient unit” at the EC secretariat level |
| Clinicians | Alignment between clinical societies on evidence assessment for a consolidated position to achieve: Narrowing the gaps in methodologies, e.g., pertaining to required methods assessing rare diseases/small populations Management of uncertainty, e.g., context-dependent alignment on acceptable levels of uncertainty More dynamic adoption of new frameworks and methodologies, e.g., basket trials based on the clinical context Capacity building by medical societies: Create a pool of clinicians/societies for involvement in HTA on the EU level Societies to choose their fields and abilities Involve remuneration for consulting Standardization of processes for involvement of clinicians in HTA: Formalized integration of consultation, dialogue, and feedback processes Education on methodologies |
| Regulators | Develop joint guidance documents with HTA: Product specific Therapeutic area specific Methods Align processes and interfaces with HTA bodies under the regulation: Exchange of information in the context of JCA Considering sharing the right data at the right time Respecting remits Expert engagement Shared discussion with HTA bodies on PLEG: Condition-specific evidence generation (registries) Identification of requirements (product specific) Guidance to be developed to engage with other stakeholders Ensure sufficient regulatory capacities for: Early scientific consultation (PICO alignment) |
| HTDs | Rapid introduction of scientific advice within EU HTA at scale—resources, expertise, and agility to respond to the needs Review the scoping process within EU HTA to optimize input and insights from the different stakeholders, especially HTDs: Allow HTDs to propose elements of the PICOs Increase the utility of the process/reports to national HTA agencies Risk with status quo: PICOs not being fit for purpose Develop the scope of the fact-checking process further so that it increases the scientific credibility of the EU report, stakeholder trust, and utilization by national HTA agencies |
| National HTA bodies and payers | Develop joint guidance documents with regulators: Product specific Therapeutic area specific Methods Align processes and interfaces with regulators under the regulation: Exchange of information in the context of JCA Considering sharing the right data at the right time Respecting remits Expert engagement Shared discussion with regulators on PLEG: Condition-specific evidence generation (registries) Identification of requirements (product specific) Guidance to be developed to engage with other stakeholders Ensure sufficient national HTA capacities for: Early scientific consultation (PICO alignment) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Desmet, T.; Julian, E.; Van Dyck, W.; Huys, I.; Simoens, S.; Giuliani, R.; Toumi, M.; Dierks, C.; Dierks, J.; Cardone, A.; et al. An Inclusive Civil Society Dialogue for Successful Implementation of the EU HTA Regulation: Call to Action to Ensure Appropriate Involvement of Stakeholders and Collaborators. J. Mark. Access Health Policy 2024, 12, 21-34. https://doi.org/10.3390/jmahp12010004
Desmet T, Julian E, Van Dyck W, Huys I, Simoens S, Giuliani R, Toumi M, Dierks C, Dierks J, Cardone A, et al. An Inclusive Civil Society Dialogue for Successful Implementation of the EU HTA Regulation: Call to Action to Ensure Appropriate Involvement of Stakeholders and Collaborators. Journal of Market Access & Health Policy. 2024; 12(1):21-34. https://doi.org/10.3390/jmahp12010004
Chicago/Turabian StyleDesmet, Thomas, Elaine Julian, Walter Van Dyck, Isabelle Huys, Steven Simoens, Rosa Giuliani, Mondher Toumi, Christian Dierks, Juliana Dierks, Antonella Cardone, and et al. 2024. "An Inclusive Civil Society Dialogue for Successful Implementation of the EU HTA Regulation: Call to Action to Ensure Appropriate Involvement of Stakeholders and Collaborators" Journal of Market Access & Health Policy 12, no. 1: 21-34. https://doi.org/10.3390/jmahp12010004