Spatial Equilibrium Allocation of Urban Large Public General Hospitals Based on the Welfare Maximization Principle: A Case Study of Nanjing, China


Abstract
:1. Introduction
2. Methodology and Materials
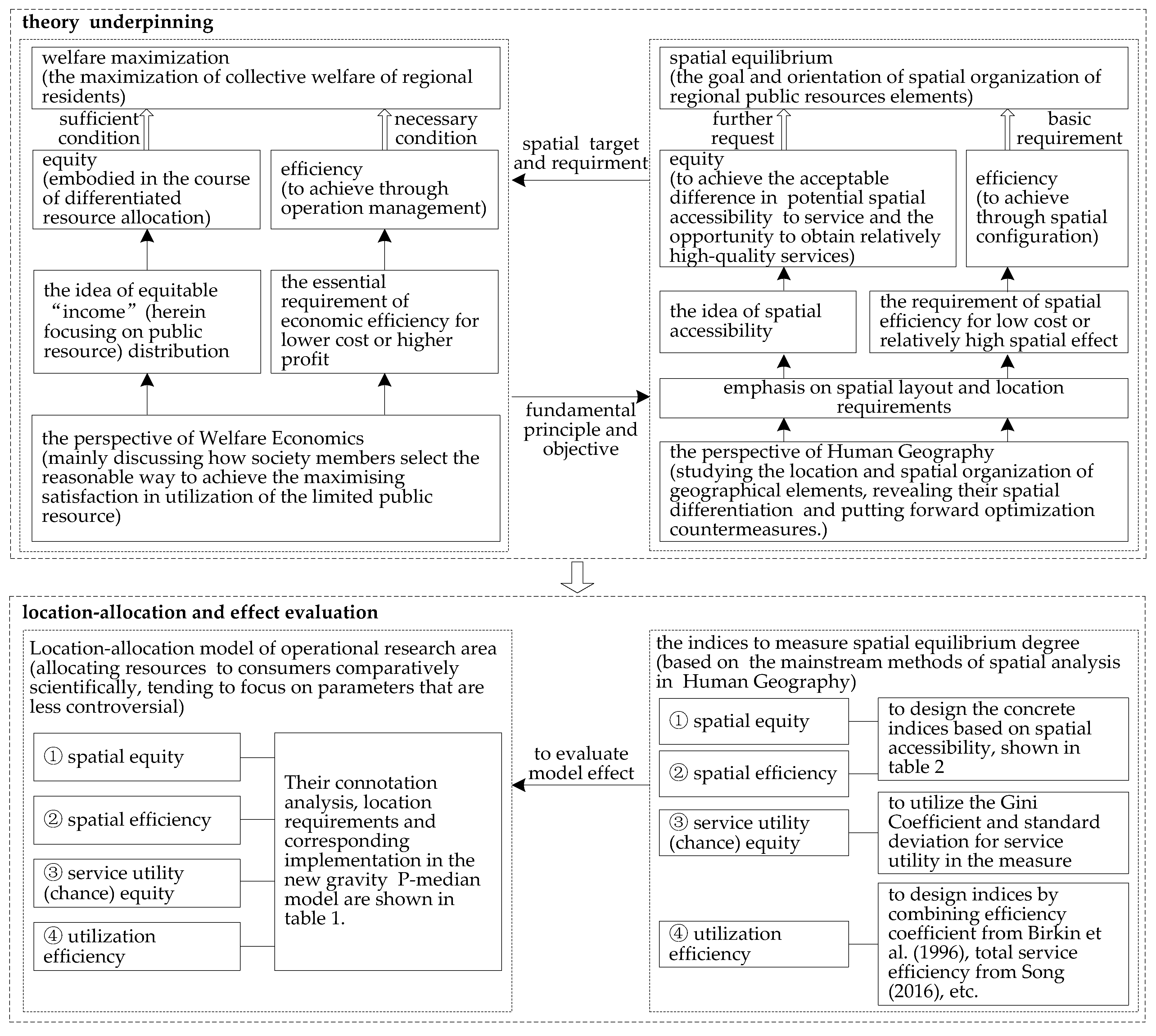
2.1. Spatial Allocation Goal of Urban General Hospitals—Spatial Equilibrium
2.2. The Construction Process and Mathematical Expression of the New Gravity P-Median Model
2.2.1. Probability Rule
2.2.2. The Construction Process of the New Gravity P-Median Model
- Z
- be the objective function;
- N
- of cardinality n, be the set of all numbers of alternative facility nodes or, N = {1, 2, …, n};
- M
- of cardinality m, be the set of demand points, M = {1, 2, …, m};
- N0
- be the set of non-negative integers;
- i
- be the index of the demand node;
- j
- be the index of the potential facility site;
- P
- be the amount of facilities located, and the set of facilities, j ∈ P;
- Wi
- be the demand quantity for demand point i;
- Dij
- be the travel cost between demand point i and facility j, which can be distance, time, expense, and the like;
- Ej
- be the demand population scale competition coefficient of a facility located at node j;
- K
- be the total scale of all facilities;
- β
- be the distance attenuation coefficient, in this study the distance function applies the power exponent form;
- Aij
- be the amount of potentially accessible service resources of the customers residing at demand point i served by the facility located at node j, which in this article refers to the general hospital j;
- Ai
- be the total amount of the potentially accessible service resources of demand point i patronizing all facilities in the study area;
- D0
- be the maximum travel cost between a demand point i and the corresponding adjacent facility;
- Qj
- be the capacity (scale) of each facility j, and, for general hospitals, it is usually characterized by the number of beds or personnel;
- Q0
- be the minimum scale of a single facility;
- Xj
- be the 0/1 decision variable, taking 1 to indicate that the location of j has one facility, and taking 0 to represent the opposite;
- Yij
- be 0/1 decision variable, taking 1 to indicate that the facility j can provide service for the demand point i, taking 0 to means the opposite.
2.3. Empirical Area and Data Preparation
2.3.1. Empirical Regional Introduction and Basic Data Acquisition
- (1)
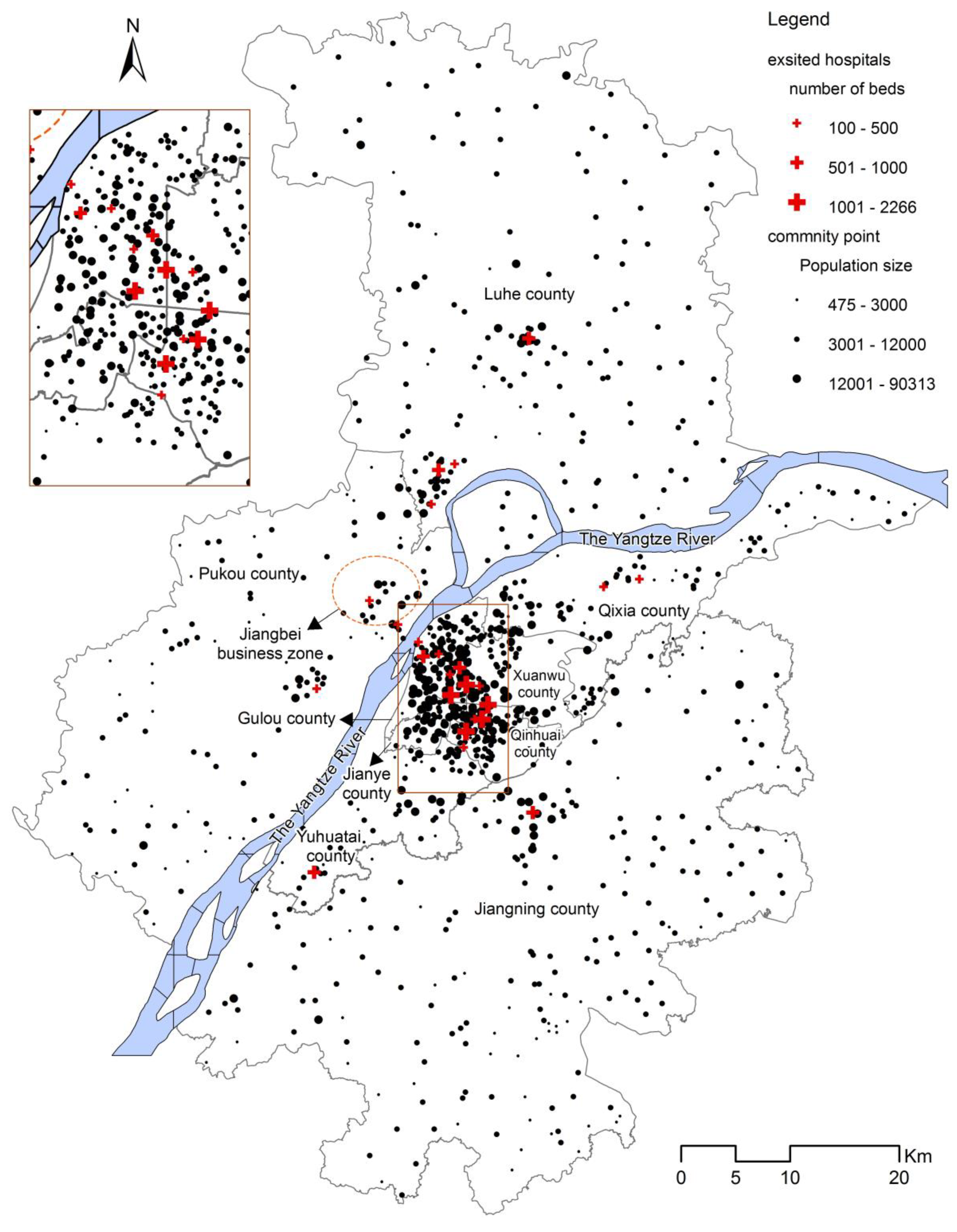
- Current facility locations and scales: By the end of 2013, there were 25 secondary and tertiary general hospitals and about 7,348,000 residents in the study area (Figure 3). They were mainly located in Gulou, Xuanwu, and Qinhuai District, all with dense populations. The bed number is selected to represent the hospital’s scale. Thus, the total beds of 25 hospitals amounted to 15,843, with an average number of beds per thousand people of approximately 2.16.
- (2)
- Determination of demand points: The 949 communities (villages) were selected as study units, and the administrative centers as demand points for all i.
- (3)
- Facility candidates: The candidate locations for all j consisted of 949 settlements and 25 current hospitals.
- (4)
- The travel time calculation under traffic network optimal path: The travel time Dij by car (bus and taxi) or subway was selected to measure the travel cost of residents to go to hospitals. The speed for each level road was determined by Technical Standard of Highway Engineering (JTG B01-2003) issued by Ministry of Communications of China in 2004. The main road network was supplemented by the 500 m × 500 m grid, to replace the lane (a street, often a narrow one with buildings on both sides), and the default speed for the roads that the grids represented was 10 km/h. The calculation of the shortest access time between hospitals (alternative points) and demand points was completed based on the optimal route in the ArcGIS Workstation or ArcView 3.3 software from American ESRI Company.
2.3.2. Determination of Key Constraints or Variables in the New Gravity P-Median Model
- (1)
- Facilities amount, P:The first step to decide where to locate the hospital is to determine the number, which is based on the current hospital allocation policy for preliminary judgment and, ultimately, can be determined by comparing the fairness and efficiency of different layout schemes. In this study, the hospital number is not taken as an object of inquiry. In fact, the determination of the number will require significant effort. We assumed that the number of secondary and tertiary general hospitals in the optimization was the same with the current layout, that is, P = 25.
- (2)
- The minimum facility scale, Q0:According to the current regulation on the minimum scale of secondary general hospitals, a bed number of 100 is the minimum scale of each facility.
- (3)
- The maximum travel cost, D0, among the costs of all demand points to the nearest hospitals:The D0 value was determined by the present accessibility situation and by questionnaires. The parents or other family members of elementary and middle school students completed about 400 questionnaires. In this survey, we sent out 600 questionnaires. The ideal travel time of the residents to the nearest hospital was determined to be 30 min.
- (4)
- The service capacity amount, K, of all facilities:The new model was discussed in a relatively static framework. The total service capacity of all facilities was set to be remain at 15,843 beds.
- (5)
- Attenuation coefficient, β:It was determined to be 2, based on the experimental comparison.
3. Results and Analysis
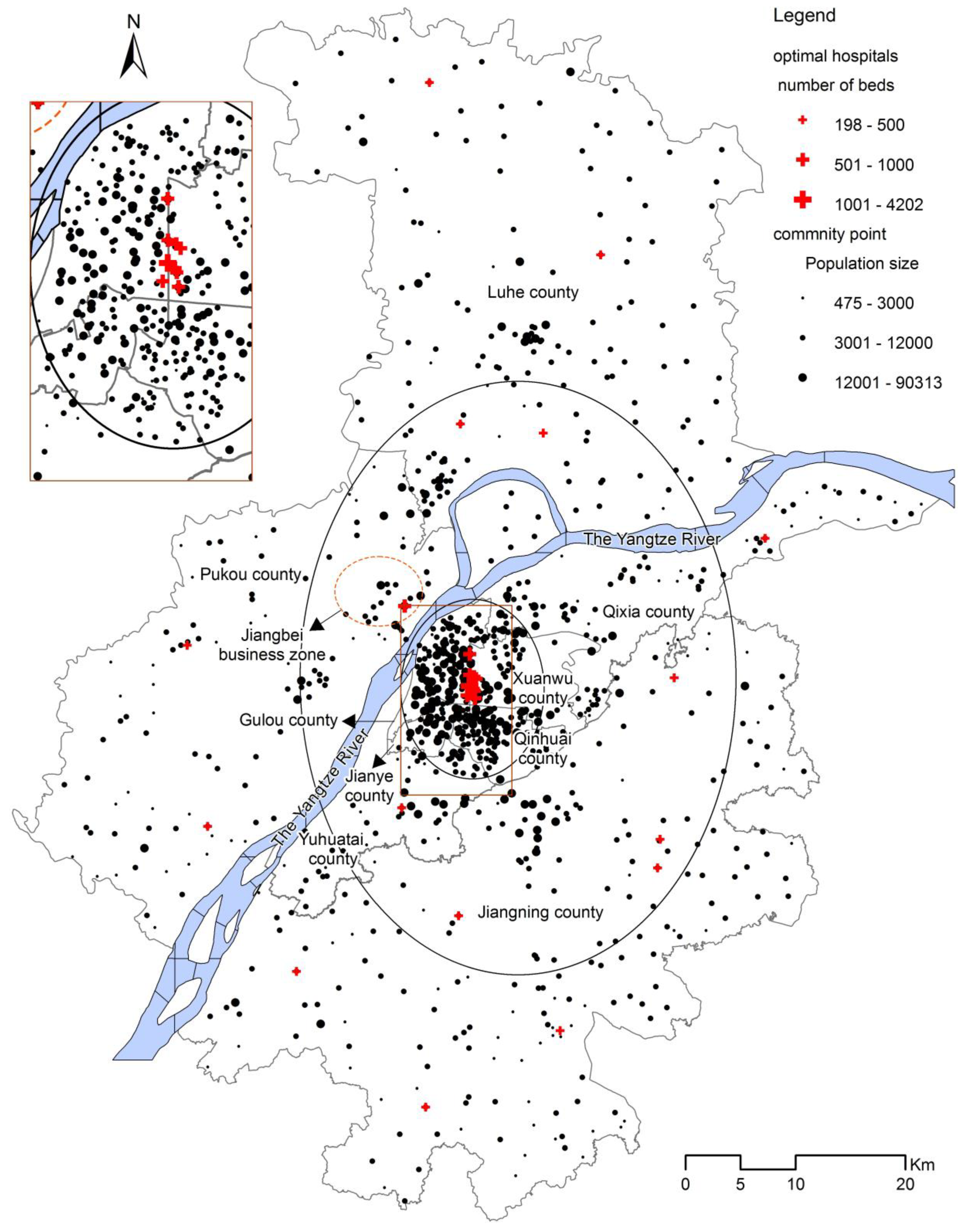
3.1. Spatial Distribution Description of Current and Suggested Hospitals Layouts
3.2. The Spatial Effect of Optimal Allocation
- (1)
- The new layout of the hospitals is relatively more convenient for residents, more fitting for the population distribution and traffic network layout. Moreover, the new location-allocation result is consistent with the three circles of population and transportation distribution.
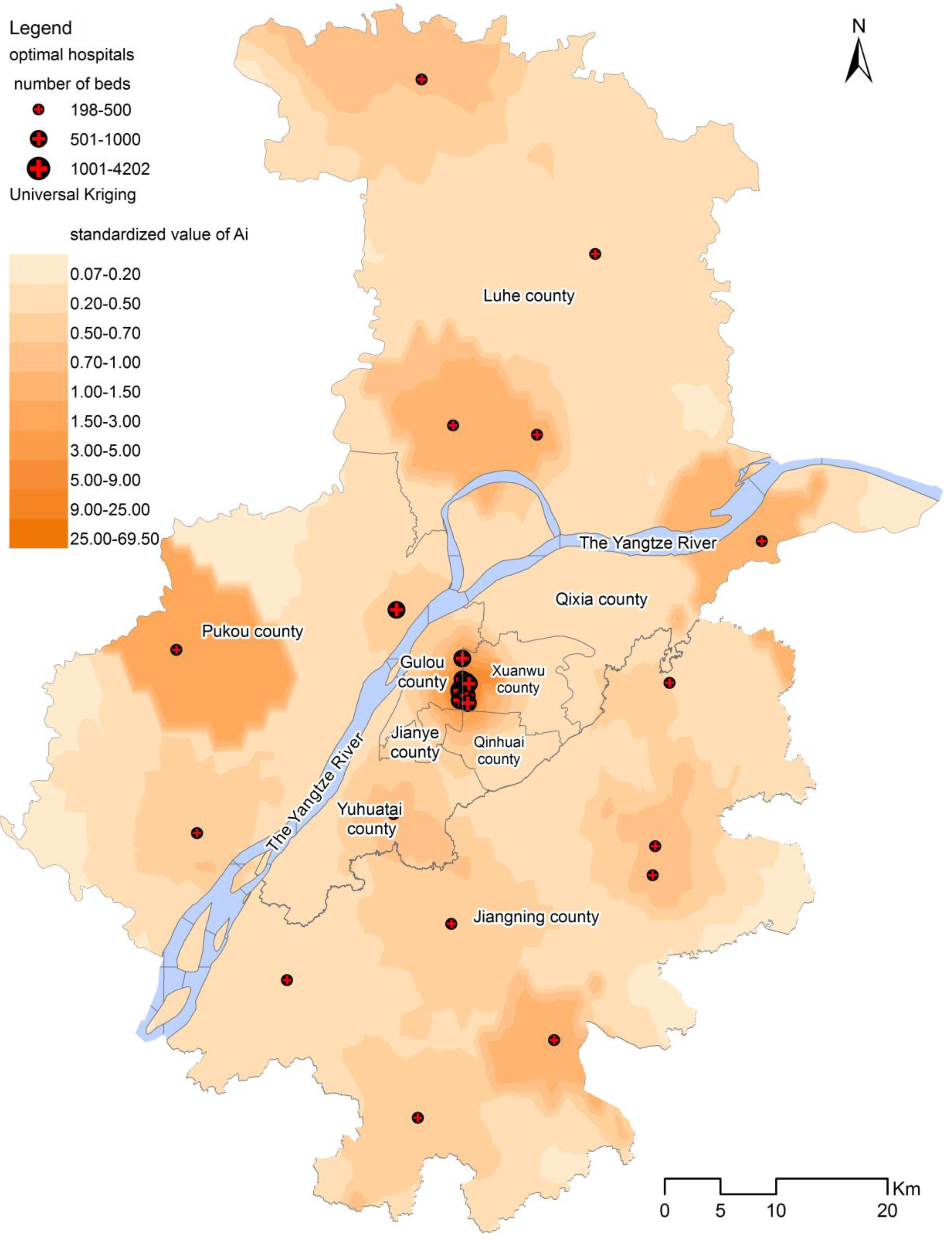
- (2)
- The utility fairness in accordance with the accessibility opportunity of the new layout is more prominent than the current situation, and the equity orientation is more striking.
- (3)
- The degree of spatial equilibrium can be significantly improved in the new layout by the measure with a series of indicators. From the effect of judgement, the indicator system tailored for spatial equilibrium assessment is relatively reliable and objective.
4. Discussion
4.1. The Discussion on the Deficiency of Model Solving
4.2. The Complexity of the Solution to the New Gravity P-Median Model
4.3. How to Combine the Ideal Results with Urban Planning and Construction?
5. Conclusions and Prospects
5.1. The Further Deepening of the Main Logical Framework, Ideas, and Feasibility of the Model
5.2. The Research Value of Equilibrium Allocation Based on the New Gravity P-Median Model
5.3. The Research Value Clarified from the Perspective of a Greater Board Research Scope
5.4. Deficiency and Prospect
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thisse, J.F.; Wildasin, D.E. Public facility location and urban spatial structure: Equilibrium and welfare analysis. J. Public Econ. 1992, 48, 83–118. [Google Scholar] [CrossRef]
- Alexiadis, S. Compatibility between equity and efficiency. In The Dilemma of Regional Policy; Palgrave Pivot: Cham, Switzerland, 2018; pp. 73–105. [Google Scholar]
- Ammari, F.; Ogawa, K.; Miyagi, T. Spatial interaction model in health-care facility location-allocation. Infrastruct. Plan. Rev. 2000, 17, 219–228. [Google Scholar] [CrossRef]
- Deverteuil, G. Reconsidering the legacy of urban public facility location theory in human geography. Prog. Hum. Geogr. 2000, 24, 47–69. [Google Scholar] [CrossRef]
- Song, Z.N. Competitive public facilities location decision: Concept, location selection principle and model construction. Sci. Geogr. Sin. 2016, 36, 1485–1494. [Google Scholar]
- Song, Z.N.; Yan, T.G.; Liu, T.; Huang, T. Anew gravity P-median model and empirical test in urban comprehensive hospital location decision making: Take Wuxi as an example. Prog. Geogr. 2016, 35, 420–430. [Google Scholar]
- Bennett, W.D. A location-allocation approach to health care facility location: A study of the undoctored population in Lansing, Michigan. Soc. Sci. Med. Part D 1981, 15, 305–312. [Google Scholar] [CrossRef]
- Phillips, D.R. Urban hospital location: London research series in geography no 4: Leslie Mayhew George Allen and Unwin, London. Cities 1986, 3, 357–358. [Google Scholar] [CrossRef]
- Scarpaci, J.L. Urban Hospital Location. Econ. Geogr. 1987, 63, 97–99. [Google Scholar] [CrossRef]
- Cho, C. An equity-efficiency trade-off model for the optimum location of medical care facilities. Socio-Econ. Plan. Sci. 1998, 32, 99–112. [Google Scholar] [CrossRef]
- Yasenovskiy, V.; Hodgson, J. Hierarchical location-allocation with spatial choice interaction modelling. Ann. Assoc. Am. Geogr. 2007, 97, 496–511. [Google Scholar] [CrossRef]
- Baray, J.; Cliquet, G. Optimizing locations through a maximum covering/p-median hierarchical model: Maternity hospitals in France. J. Bus. Res. 2013, 66, 127–132. [Google Scholar] [CrossRef]
- Guerriero, F.; Miglionico, G.; Olivito, F. Location and reorganization problems: The Calabrian health care system case. Eur. J. Oper. Res. 2016, 250, 939–954. [Google Scholar] [CrossRef]
- Marks, A.P.; Thrall, G.I.; Arno, M. Siting hospitals to provide cost-effective health care. Geo. Inf. Syst. 1992, 2, 58–66. [Google Scholar]
- Brown, L.; Barnett, J.R. Is the corporate transformation of hospitals creating a new hybrid health care space? A case study of the impact of co-location of public and private hospitals in Australia. Soc. Sci. Med. 2004, 58, 427–444. [Google Scholar] [CrossRef]
- Tulchinsky, T.H.; Varavikova, E.A. Chapter 12-planning and managing health systems. In The New Public Health, 3rd ed.; Tulchinsky, T.H., Varavikova, E.A., Bickford, J.D., Eds.; Academic Press: San Diego, CA, USA, 2014; pp. 613–641. [Google Scholar]
- Moscelli, G.; Siciliani, L.; Gutacker, N.; Gravelle, H. Location, quality and choice of hospital: Evidence from England 2002–2013. Reg. Sci. Urban Econ. 2016, 60, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Shortt, N.K.; Moore, A.J. Functional localities: An integrated spatial approach towards health care locality definition. GeoJournal 2006, 67, 27–40. [Google Scholar] [CrossRef]
- Wu, C.; Lin, C.; Chen, H. Optimal selection of location for Taiwanese hospitals to ensure a competitive advantage by using the analytic hierarchy process and sensitivity analysis. Build. Environ. 2007, 42, 1431–1444. [Google Scholar] [CrossRef]
- Sinuany-Stern, Z.; Mehrez, A.; Tal, A.G.; Shemuel, B. The location of a hospital in a rural region: The case of the Negev. Locat. Sci. 1995, 3, 255–266. [Google Scholar] [CrossRef]
- Mestre, A.M.; Oliveira, M.D.; Barbosa-Póvoa, A.P. Location–allocation approaches for hospital network planning under uncertainty. Eur. J. Oper. Res. 2015, 240, 791–806. [Google Scholar] [CrossRef]
- Revelle, C.; Snyder, S. Integrated fire and ambulance sitting: A deterministic model. Socio-Econ. Plan. Sci. 1995, 29, 261–271. [Google Scholar] [CrossRef]
- Knight, V.A.; Harper, P.R.; Smith, L. Ambulance allocation for maximal survival with heterogeneous outcome measures. Omega 2012, 40, 918–926. [Google Scholar] [CrossRef]
- Salman, F.S.; Yücel, E. Emergency facility location under random network damage: Insights from the Istanbul case. Comput. Oper. Res. 2015, 62, 266–281. [Google Scholar] [CrossRef]
- Schweikhart, S.B.; Smith-Daniels, V.L. Location and service mix decisions for a managed health care network. Socio-Econ. Plan. Sci. 1993, 27, 289–302. [Google Scholar] [CrossRef]
- Zhang, W.; Cao, K.; Liu, S.; Huang, B. A multi-objective optimization approach for health-care facility location-allocation problems in highly developed cities such as Hong Kong. Comput. Environ. Urban Syst. 2016, 59, 220–230. [Google Scholar] [CrossRef]
- Marianov, V.; Serra, D.; New Trends in Public Facility Location Modeling. Economics Working Papers 2004. Available online: http://www.econ.upf.edu/docs/papers/downloads/755.pdf (accessed on 4 January 2010).
- Surhone, L.M.; Timpledon, M.T.; Marseken, S.F. Welfare Economics; Betascript Publishing: Whitefish, MT, USA, 2010. [Google Scholar]
- Chen, W. Economic Analysis of Spatial Equilibrium; Commercial Press: Beijing, China, 2008. [Google Scholar]
- Mirchandani, P.B.; Francis, R.L. Discrete Location Theory; John Wiley & Sons: New York, NY, USA, 1990. [Google Scholar]
- Marsh, M.T.; Schilling, D.A. Equity measurement in facility location analysis: A review and framework. Eur. J. Oper. Res. 1994, 74, 1–17. [Google Scholar] [CrossRef]
- Drezner, T. Location of casualty collection points. Environ. Plan. C Gov. Policy 2004, 22, 899–912. [Google Scholar] [CrossRef]
- Tsou, K.W.; Hung, Y.T.; Chang, Y.L. An accessibility-based integrated measure of relative spatial equity in urban public facilities. Cities 2005, 22, 424–435. [Google Scholar] [CrossRef]
- Drezner, T.; Drezner, Z. The gravity p-median model. Eur. J. Oper. Res. 2007, 179, 1239–1251. [Google Scholar] [CrossRef]
- Puerto, J.; Ricca, F.; Scozzari, A. Extensive facility location problems on networks with equity measures. Discret. Appl. Math. 2009, 157, 1069–1085. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Xie, Q.; Shi, S.; Ye, X.; Zhao, A. Regional maldistribution of China’s hospitals based on their structural system. Sustainability 2017, 9, 1046. [Google Scholar] [CrossRef]
- Wu, H.; Liu, L.; Yu, Y.; Peng, Z. Evaluation and planning of urban green space distribution based on mobile phone data and two-step floating catchment area method. Sustainability 2018, 10, 214. [Google Scholar] [CrossRef]
- Burkey, M.L.; Bhadury, J.; Eiselt, H.A. A location-based comparison of health care services in four U.S. states with efficiency and equity. Socio-Econ. Plan. Sci. 2012, 46, 157–163. [Google Scholar] [CrossRef]
- Cromley, E.; McLafferty, S. GIS and Public Health; The Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Rais, A.; Viana, A. Operations research in healthcare: A survey. Int. Trans. Oper. Res. 2010, 18, 1–31. [Google Scholar] [CrossRef]
- Huff, D.L. A programmed solution for approximating an optimum retail location. Land Econ. 1966, 42, 293–303. [Google Scholar] [CrossRef]
- Daskin, M.S. Network and Discrete Location: Models, Algorithms, and Applications; John Wiley & Sons: New York, NY, USA, 1995. [Google Scholar]
- Owen, S.H.; Daskin, M.S. Strategic facility location: A review. Eur. J. Oper. Res. 1998, 111, 423–447. [Google Scholar] [CrossRef]
- Church, R.L.; ReVelle, C.S. Theoretical and computational links between the p-median, location set-covering, and the maximal covering location problem. Geogr. Anal. 1976, 8, 406–415. [Google Scholar] [CrossRef]
- Drezner, T.; Drezner, Z. Multiple facilities location in the plane using the gravity model. Geogr. Anal. 2006, 38, 391–406. [Google Scholar] [CrossRef]
- Carreras, M.; Serra, D. On optimal location with threshold requirements. Socio-Econ. Plan. Sci. 1999, 33, 91–103. [Google Scholar] [CrossRef]
- Wang, F.; Luo, W. Assessing spatial and non-spatial factors for healthcare access: Towards an integrated approach to defining health professional shortage areas. Health Place 2005, 11, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Birkin, M.; Clarke, G.; Clarke, M.; Wilson, A. Intelligent GIS: Location Decisions and Strategic Planning; Wiley: New York, USA, 1996; pp. 265–267. [Google Scholar]
- Tolle, K.M.; Tansley, D.S.W.; Hey, A.J.G. The fourth paradigm: Data-intensive scientific discovery. Proc. IEEE 2011, 99, 1334–1337. [Google Scholar] [CrossRef]
- Fotheringham, A.S.; O’Kelly, M.E. Spatial Interaction Models: Formulations and Applications; Kluwer Academic Publishers: Dordrecht, The Netherlands, 1989. [Google Scholar]
- Yamashita, J. Effects of spatial interaction on spatial structure: A case of day centre location in Malinti. Geogr. Rev. Jpn. 1993, 66, 156–172. [Google Scholar] [CrossRef]
- Drezner, T.; Drezner, Z. A note on applying the gravity rule to the airline hub problem. J. Reg. Sci. 2001, 41, 67–73. [Google Scholar] [CrossRef]
- Drezner, T.; Drezner, Z. The gravity multiple server location problem. Comput. Oper. Res. 2011, 38, 694–701. [Google Scholar] [CrossRef]
- Wan, B. Study on the Public Service Facility Location Problem. Ph.D. Thesis, Huazhong University of Science and Technology, Wuhan, China, 2012. [Google Scholar]
- Garey, M.R.; Johnson, D.S. Computers and Intractability: A Guide to the Theory of NP-Completeness; W.H. Freeman and Company: New York, NY, USA, 1979. [Google Scholar]
- White, A. Accessibility and public facility location. Econ. Geogr. 1979, 55, 18–35. [Google Scholar] [CrossRef]
- Murad, A. A GIS Application for modeling accessibility to health care centers in Jeddah, Saudi Arabia. In GIS for Health and the Environment; Springer: Berlin/Heidelberg, Germany, 2007; pp. 57–70. [Google Scholar]
- Revelle, C. Handbook of Regional & Urban Economics. In Urban Economics; Chapter 27 Urban public facility location; Mills, E.S., Ed.; Elsevier: Amsterdam, North-Holland, 1987; Volume 2, pp. 291–326. [Google Scholar]
- Smith, H.K.; Potts, C.N. Bicriteria efficiency/equity hierarchical location models for public service application. J. Oper. Res. Soc. 2013, 64, 500–512. [Google Scholar] [CrossRef]
- Hodgson, M.J. An hierarchical location-allocation model for primary health care delivery in a developing area. Soc. Sci. Med. 1988, 26, 153–161. [Google Scholar] [CrossRef]
- Chan, Y.; Mahan, J.M.; Chrissis, J.W.; Drake, D.A.; Wang, D. Hierarchical maximal-coverage location–allocation: Case of generalized search-and-rescue. Comput. Oper. Res. 2008, 35, 1886–1904. [Google Scholar] [CrossRef]
- Minde, J.M. Building a Framework for a Spatial Decision Support System for Co-Locating Public Facilities. Master’s Thesis, University of Iowa, Iowa City, IA, USA, 1997. [Google Scholar]
- Huang, R.B. Network Location Problems with Multiple Types of Facilities; Library and Archives Canada (Bibliothèque et Archives Canada): Ottawa, ON, Canada, 2006. [Google Scholar]
- Sikder, S.K.; Eanes, F.; Asmelash, H.B.; Kar, S.; Koetter, T. The contribution of energy-optimized urban planning to efficient resource use—A case study on residential settlement development in Dhaka City, Bangladesh. Sustainability 2016, 8, 119. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interpretation Perspective | Geography (Spatial) | Economics | |
|---|---|---|---|
| Starting Point | |||
| Fairness: On the basis of public demand and individual considerations | fairness according to the travel convenience of dwellers | service utility equity (providing relatively high-level service, whose differentiation can be acceptable) | |
| Location-allocation requirement | to limit travel costs to nearby facilities | ① to set a minimum facility scale, ② to set an appropriate scale for each facility based on population distribution and the accessibility to all facilities | |
| The corresponding items in the following model of Section 2.2.2 | Equations (8)–(11) in step (2) | ① Equations (6) and (7) in step (4); ② Equations (4) and (5) in step (3) | |
| Efficiency: On the basis of the consideration of the governmental fiscal orientation and the integrity of the audience | The total travel cost to all facilities is minimized, and a larger proportion of inhabitants can conveniently reach the facilities | utilization efficiency, which is the efficiency of dwellers to utilize facilities based on scale attractiveness | |
| Location-allocation requirement | to minimize the total weighted travel cost | ① to set a minimum facility scale, ② to set an appropriate scale for each facility according to population distribution and traffic layout | |
| The corresponding items in the following model of Section 2.2.2 | Equation (1) in step (2) | ① Equations (6) and (7) in step (4); ② Equations (4) and (5) in step (3) | |
| The Contrast Indicator | The Current Layout | Optimal Layout | Ameliorated Degree (by %) | |
|---|---|---|---|---|
| Spatial equity | The maximum time from the demand points to the nearest hospitals (min) | 65.60 | 30.00 | 54 |
| The average travel time from the demand points to the nearest hospitals (min) | 17.25 | 11.99 | 30 | |
| Spatial efficiency | The residents covered quantity ratio within 30 min (%) | 87.33 | 100 | 13 |
| The weighted average travel time from all the demand points to hospitals (min) | 22.95 | 24.78 | – | |
| Service utility(chance) fairness | The Gini Coefficient of potentially accessible service resources amount of residents | 0.40 | 0.28 | 30 |
| The standard deviation of the service utility with the time factor (the population of each demand point potentially going for one facility by probability/time2× scale) | 2,547,941.34 | 945,443.17 | 63 | |
| The standard deviation of potentially accessible service resources amount of all demand points (Std of all Aij) | 1.13 | 0.96 | 15 | |
| Utilization efficiency | The average of potentially accessible service resources amount of all demand points (AVG of all Aij) (the number s of beds per 1000 people) | 0.07 | 0.08 | 14 |
| The average of each hospital service utility (to sum the population of each community potentially going for some facility by probability × hospital scale/hospital number, population size × the number of beds) | 260,482,453 | 297,479,205 | 14 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Z.; Yan, T.; Ge, Y. Spatial Equilibrium Allocation of Urban Large Public General Hospitals Based on the Welfare Maximization Principle: A Case Study of Nanjing, China. Sustainability 2018, 10, 3024. https://doi.org/10.3390/su10093024
Song Z, Yan T, Ge Y. Spatial Equilibrium Allocation of Urban Large Public General Hospitals Based on the Welfare Maximization Principle: A Case Study of Nanjing, China. Sustainability. 2018; 10(9):3024. https://doi.org/10.3390/su10093024
Chicago/Turabian StyleSong, Zhengna, Tinggan Yan, and Yunjian Ge. 2018. "Spatial Equilibrium Allocation of Urban Large Public General Hospitals Based on the Welfare Maximization Principle: A Case Study of Nanjing, China" Sustainability 10, no. 9: 3024. https://doi.org/10.3390/su10093024
APA StyleSong, Z., Yan, T., & Ge, Y. (2018). Spatial Equilibrium Allocation of Urban Large Public General Hospitals Based on the Welfare Maximization Principle: A Case Study of Nanjing, China. Sustainability, 10(9), 3024. https://doi.org/10.3390/su10093024