Combining Life Cycle Assessment and Circularity Assessment to Analyze Environmental Impacts of the Medical Remanufacturing of Electrophysiology Catheters



Abstract
:1. Introduction
2. Methodology
2.1. Life Cycle Assessment
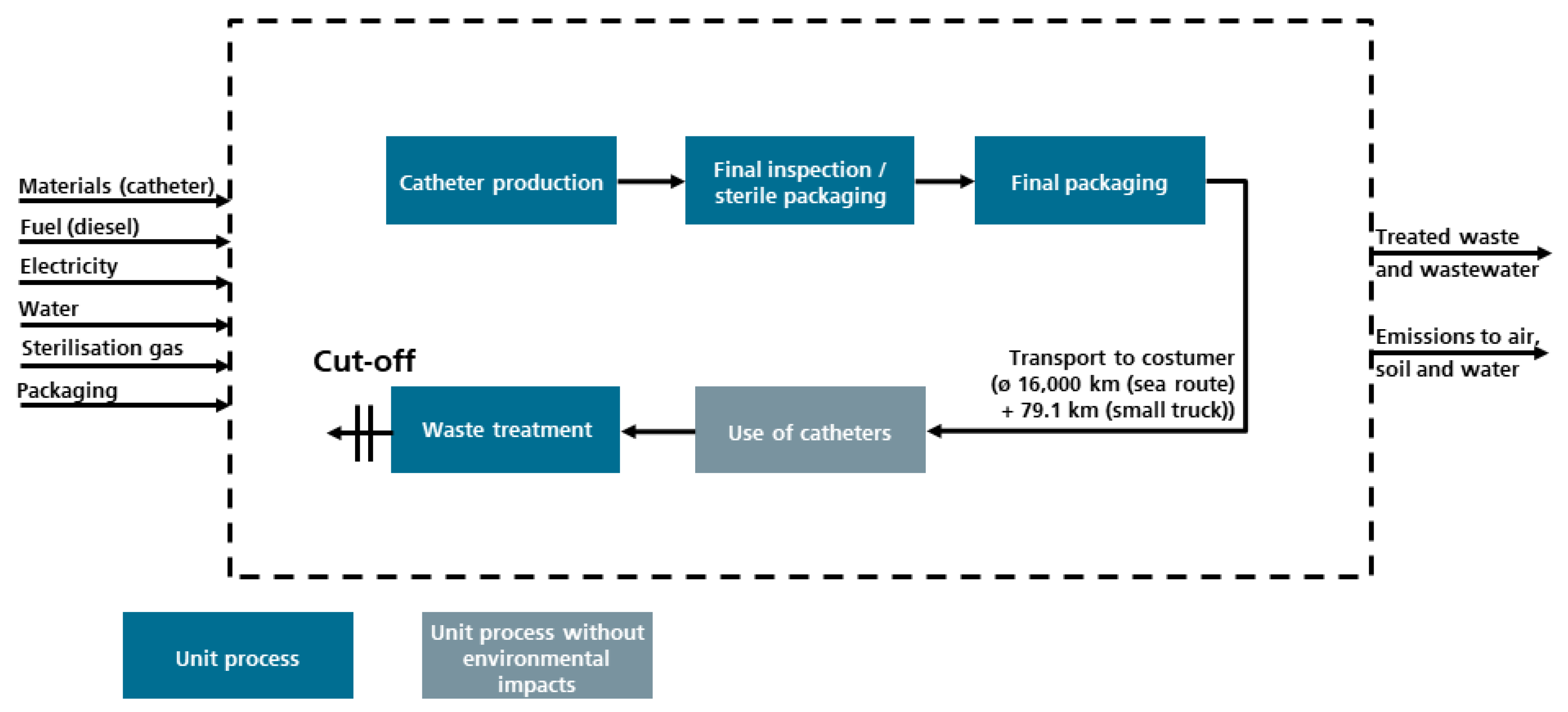
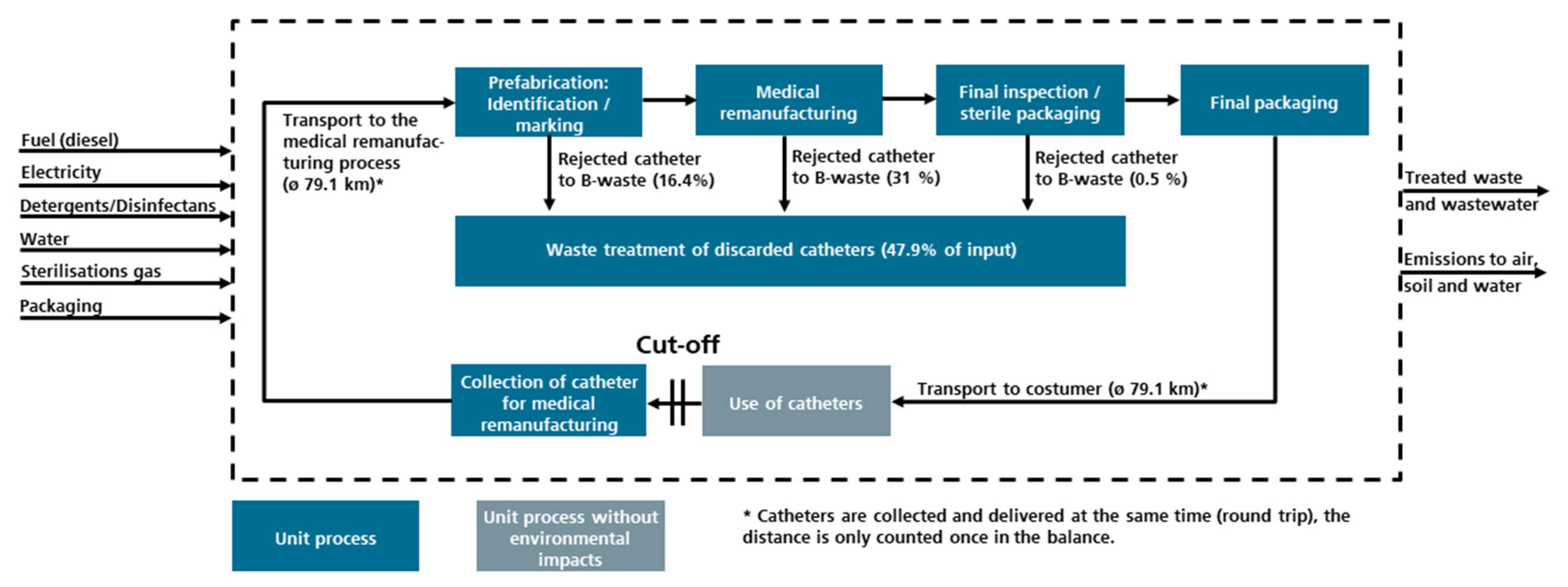
2.1.1. Goal and Scope of the Study
2.1.2. Life Cycle Inventory
2.1.3. Impact Assessment
- Climate change (determination of the GWI)
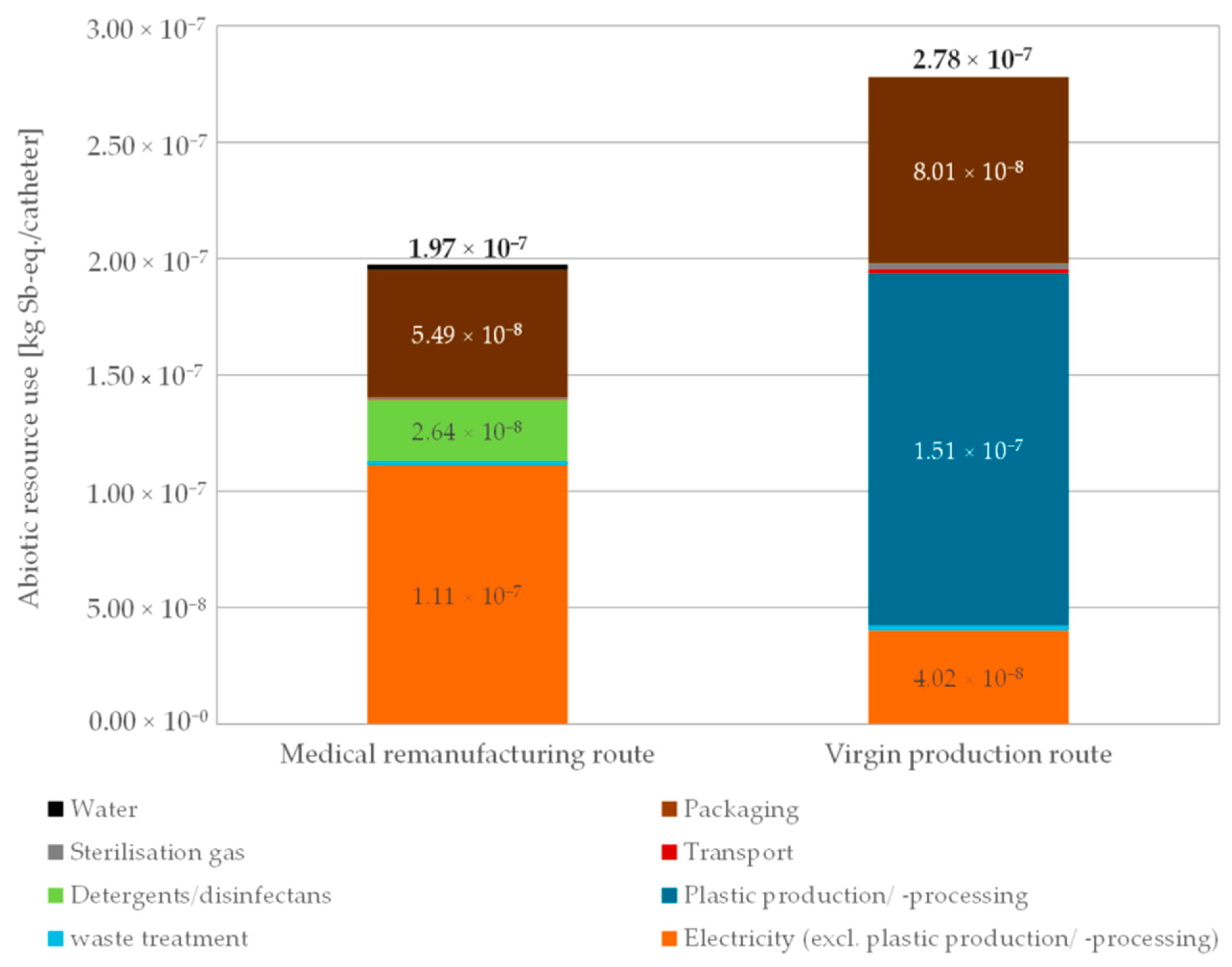
- Resource use, mineral and metals (determination of the abiotic resource use)
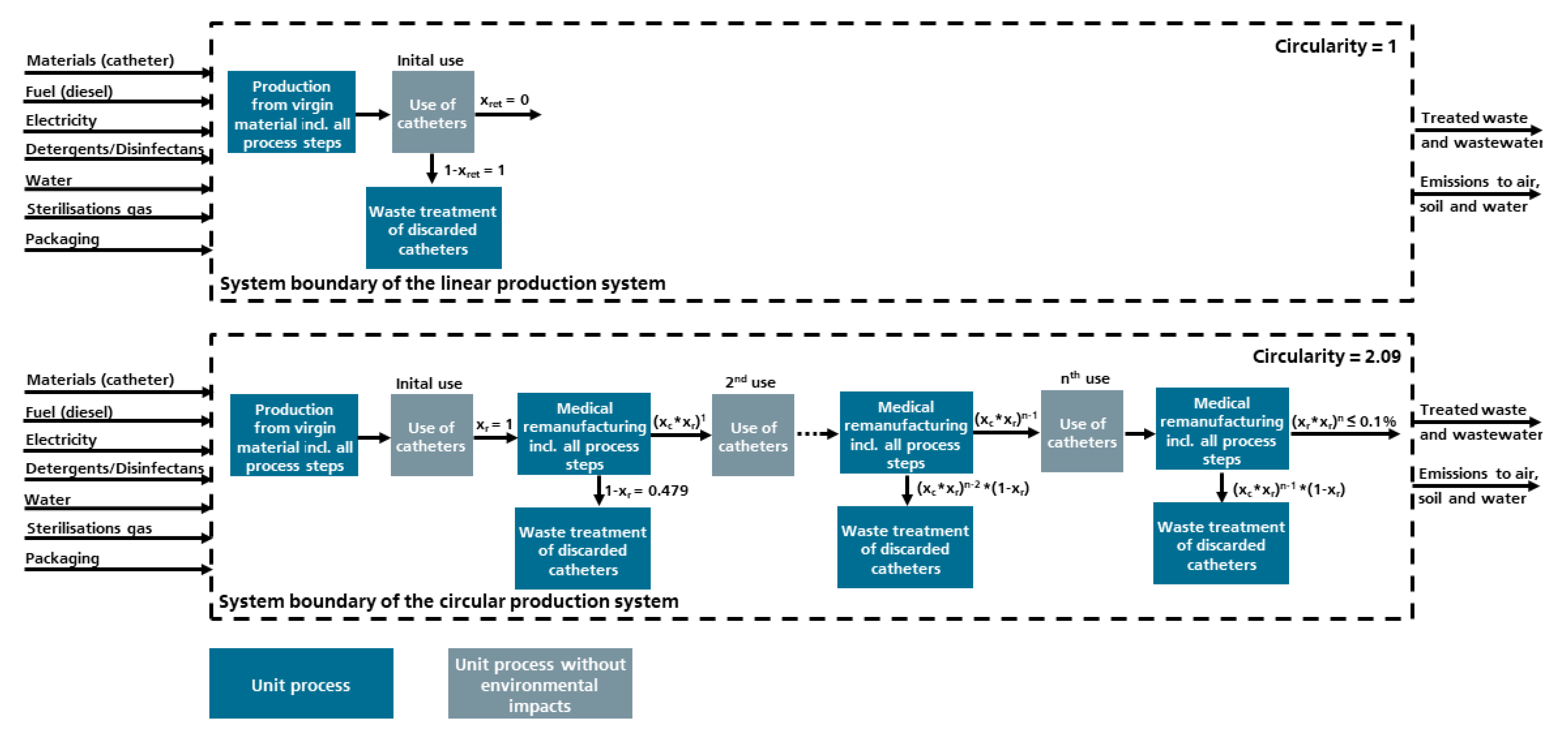
2.2. Combining Circularity and Life Cycle Assessment
3. Results and Discussion
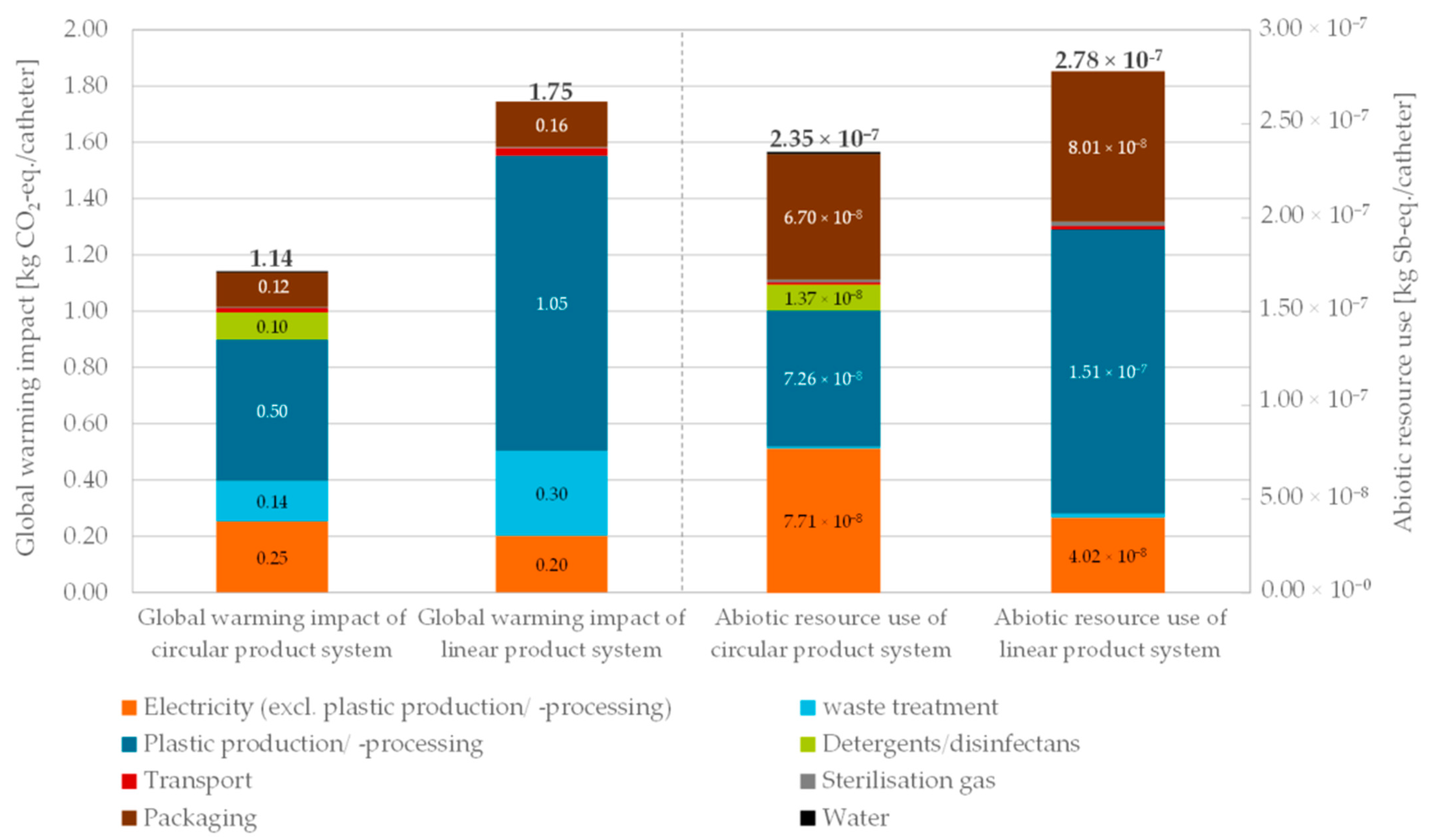
3.1. Environmental Impacts of the Medical Remanufacturing and Virgin Production Routes
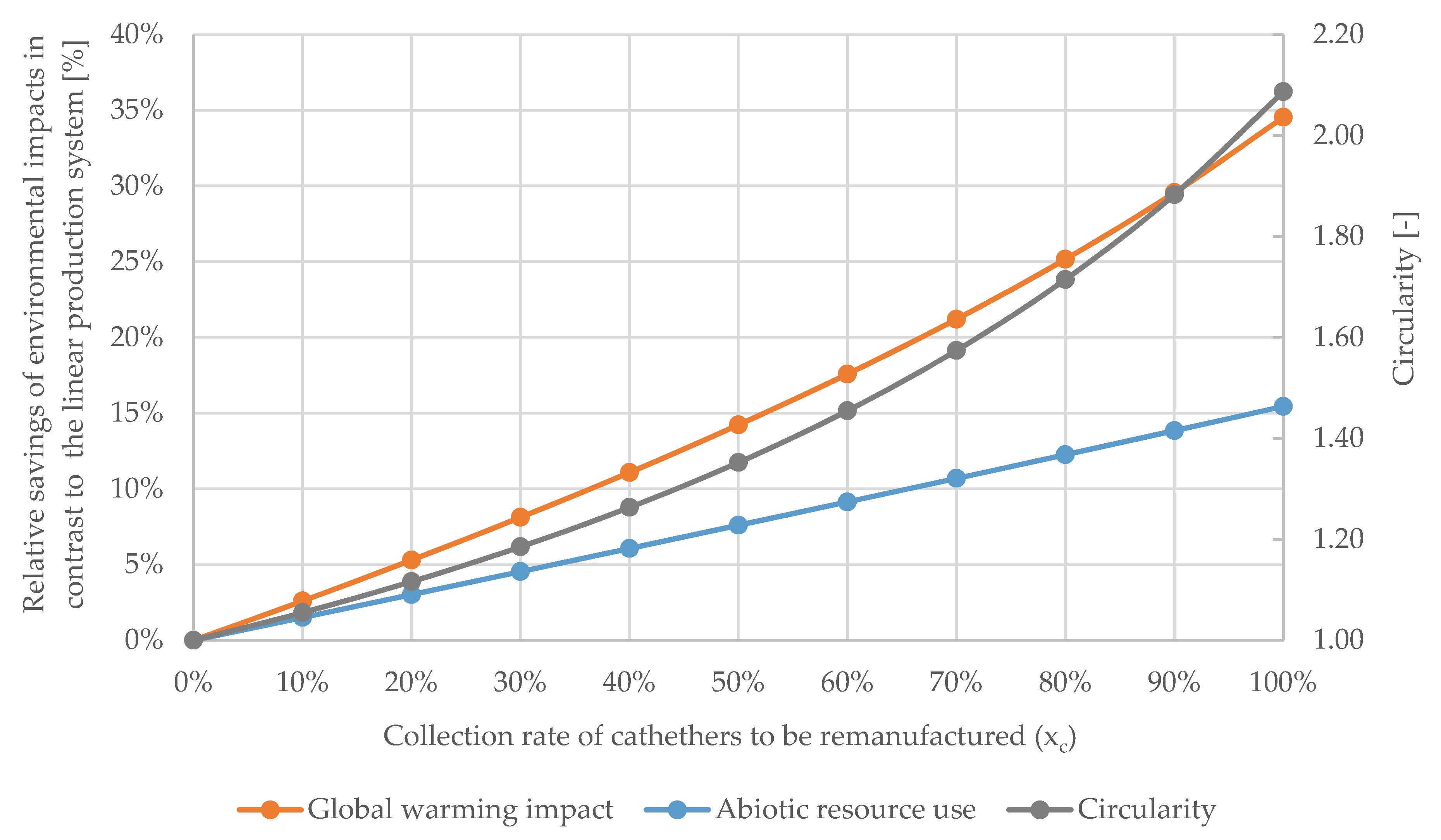
3.2. Results of Linking LCA and Circularity
3.3. Limitations of the Study
4. Conclusions and Outlook
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Behrens, A.; Giljum, S.; Kovanda, J.; Niza, S. The material basis of the global economy. Ecol. Econ. 2007, 64, 444–453. [Google Scholar] [CrossRef]
- Ghisellini, P.; Cialani, C.; Ulgiati, S. A review on circular economy: The expected transition to a balanced interplay of environmental and economic systems. J. Clean. Prod. 2016, 114, 11–32. [Google Scholar] [CrossRef]
- Ellen MacArthur Foundation. Circularity Indicators. An Approach to Measuring Circularity: Methodology; Ellen MacArthur Foundation: Cowes, UK, 2015. [Google Scholar]
- Saidani, M.; Yannou, B.; Leroy, Y.; Cluzel, F.; Kendall, A. A taxonomy of circular economy indicators. J. Clean. Prod. 2019, 207, 542–559. [Google Scholar] [CrossRef] [Green Version]
- European Comission. Circular Economy Action Plan. For a Cleaner and More Competitive Europe; European Comission: Brussels, Belgium, 2020. [Google Scholar]
- Rizos, V.; Tuokko, K.; Behrens, A. The Circular Economy: A Review of Definitions, Processes and Impacts; Centre for European Policy Studies: Brussels, Belgium, 2017. [Google Scholar]
- Lüdeke-Freund, F.; Gold, S.; Bocken, N.M.P. A Review and Typology of Circular Economy Business Model Patterns. J. Ind. Ecol. 2019, 23, 36–61. [Google Scholar] [CrossRef] [Green Version]
- Stewart, R.; Niero, M. Circular economy in corporate sustainability strategies: A review of corporate sustainability reports in the fast-moving consumer goods sector. Bus. Strat. Environ. 2018, 27, 1005–1022. [Google Scholar] [CrossRef] [Green Version]
- Millar, N.; McLaughlin, E.; Börger, T. The Circular Economy: Swings and Roundabouts? Ecol. Econ. 2019, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Djuric Ilic, D.; Eriksson, O.; Ödlund, L.; Åberg, M. No zero burden assumption in a circular economy. J. Clean. Prod. 2018, 182, 352–362. [Google Scholar] [CrossRef]
- Blomsma, F.; Brennan, G. The Emergence of Circular Economy: A New Framing around Prolonging Resource Productivity. J. Ind. Ecol. 2017, 21, 603–614. [Google Scholar] [CrossRef]
- Ellen MacArthur Foundation. Towards the Circular Economy. Economic and Business Rationale for an Accelerated Transition; Ellen MacArthur Foundation: Cowes, UK, 2013. [Google Scholar]
- Kirchherr, J.; Reike, D.; Hekkert, M. Conceptualizing the circular economy: An analysis of 114 definitions. Resour. Conserv. Recycl. 2017, 127, 221–232. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Medical Devices; Reprocessed Single-Use Devices; Termination of Exemptions from Premarket Notification; Requirement for Submission of Validation Data: List of SUDs Known to Be Reprocessed or Considered for Reprocessing (Attachment 1). Federal Register, 29 September 2005. [Google Scholar]
- Potting, J.; Hekkert, M.; Worrell, E.; Hanemaaijer, A. Circular Economy: Measuring Innovation in the Product Chain; PBL Publishers: Netherlands Environmental Assessment Agency, The Hague, The Netherlands, 2017. [Google Scholar]
- British Standards Institution. Framework for Implementing the Principles of the Circular Economy in Organizations—Guide; BSI: Frankfurt am Main, Germany, 2017; ISBN 9780580926440. [Google Scholar]
- Gopinath, K.P.; Nagarajan, V.M.; Krishnan, A.; Malolan, R. A critical review on the influence of energy, environmental and economic factors on various processes used to handle and recycle plastic wastes: Development of a comprehensive index. J. Clean. Prod. 2020, 274, 123031. [Google Scholar] [CrossRef]
- De Decker, K. How Circular Is the Circular Economy? Available online: https://www.lowtechmagazine.com/2018/11/how-circular-is-the-circular-economy.html (accessed on 5 January 2021).
- D’Adamo, I.; Rosa, P. Remanufacturing in industry: Advices from the field. Int. J. Adv. Manuf. Technol. 2016, 86, 2575–2584. [Google Scholar] [CrossRef]
- Eze, S.; Ijomah, W.; Wong, T.C. Remanufacturing: A potential sustainable solution for increasing medical equipment availability. J. Remanuf. 2020, 10, 141–159. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-M.; Woo, W.-S.; Roh, Y.-H. Remanufacturing: Trends and issues. Int. J. Precis. Eng. Manuf. Green Technol. 2017, 4, 113–125. [Google Scholar] [CrossRef]
- Krystofik, M.; Wagner, J.; Gaustad, G. Leveraging intellectual property rights to encourage green product design and remanufacturing for sustainable waste management. Resour. Conserv. Recycl. 2015, 97, 44–54. [Google Scholar] [CrossRef]
- Shen, W.; Pang, K.; Liu, C.; Ge, M.; Zhang, Y.; Wang, X. The quality control method for remanufacturing assembly based on the Jacobian-torsor model. Int. J. Adv. Manuf. Technol. 2015, 81, 253–261. [Google Scholar] [CrossRef]
- Schau, E.M.; Traverso, M.; Lehmann, A.; Finkbeiner, M. Life Cycle Costing in Sustainability Assessment—A Case Study of Remanufactured Alternators. Sustainability 2011, 3, 2268–2288. [Google Scholar] [CrossRef] [Green Version]
- Krystofik, M.; Luccitti, A.; Parnell, K.; Thurston, M. Adaptive remanufacturing for multiple lifecycles: A case study in office furniture. Resour. Conserv. Recycl. 2018, 135, 14–23. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). Environmental Management—Life Cycle Assessment—Requirements and Guidelines; 13.020.10 (14044); International Organization for Standardization: Geneva, Switzerland, 2006. [Google Scholar]
- Peters, K. Methodological issues in life cycle assessment for remanufactured products: A critical review of existing studies and an illustrative case study. J. Clean. Prod. 2016, 126, 21–37. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, M.; Zhang, H.; Jiang, Z.; Liu, C.; Cai, W. A review on energy, environment and economic assessment in remanufacturing based on life cycle assessment method. J. Clean. Prod. 2020, 255, 120160. [Google Scholar] [CrossRef]
- Schau, E.M.; Traverso, M.; Finkbeiner, M. Life cycle approach to sustainability assessment: A case study of remanufactured alternators. J. Remanuf. 2012. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Li, T.; Jiang, Q.; Zhang, H. Life Cycle Assessment-based Comparative Evaluation of Originally Manufactured and Remanufactured Diesel Engines. J. Ind. Ecol. 2014, 18, 567–576. [Google Scholar] [CrossRef]
- Vanguard AG. Information Provided by the Vanguard AG; Vanguard AG: Berlin, Germany, 2020. [Google Scholar]
- Figge, F.; Thorpe, A.S.; Givry, P.; Canning, L.; Franklin-Johnson, E. Longevity and Circularity as Indicators of Eco-Efficient Resource Use in the Circular Economy. Ecol. Econ. 2018, 150, 297–306. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). Environmental Management—Life Cycle Assessment—Principles and Framework; 13.020.10 (14040); ISO: Geneva, Switzerland, 2009. [Google Scholar]
- Vanguard AG. Picture of Electrophysiological Diagnostic Catheter; Vanguard AG: Berlin, Germany, 2020. [Google Scholar]
- Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege. Abfallentsorgung. Informationen zur Sicheren Entsorgung von Abfällen im Gesundheitsdienst; Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege: Hamburg, Germany, 2019; Available online: https://www.bgw-online.de/SharedDocs/Downloads/DE/Medientypen/BGW%20Broschueren/BGW09-19-000_Abfallentsorgung_Download.pdf?__blob=publicationFile (accessed on 1 July 2020).
- U.S. Food and Drug Administration. Ethylene Oxide Sterilization for Medical Devices. Available online: https://www.fda.gov/medical-devices/general-hospital-devices-and-supplies/ethylene-oxide-sterilization-medical-devices (accessed on 6 January 2021).
- Wernet, G.; Bauer, C.; Steubing, B.; Reinhard, J.; Moreno-Ruiz, E.; Weidema, B. The ecoinvent database version 3 (part I): Overview and methodology. Int. J. Life Cycle Assess. 2016, 21, 1218–1230. [Google Scholar] [CrossRef]
- Thinkstep. GaBi Software-System and Database for Life Cycle Engineering: DB Version 40. Available online: http://www.gabi-software.com/international/databases/ (accessed on 29 April 2016).
- Car, A. Polyether Block Amide (PEBAX). In Encyclopedia of Membranes; Drioli, E., Giorno, L., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 1–2. ISBN 978-3-642-40872-4. [Google Scholar]
- Zampori, L.; Pant, R. Suggestions for Updating the Product Environmental Footprint (PEF) Method; EUR 29682 EN. 2019. Available online: https://ec.europa.eu/jrc (accessed on 30 November 2020).
- Moraga, G.; Huysveld, S.; Mathieux, F.; Blengini, G.A.; Alaerts, L.; van Acker, K.; de Meester, S.; Dewulf, J. Circular economy indicators: What do they measure? Resour. Conserv. Recycl. 2019, 146, 452–461. [Google Scholar] [CrossRef]
- Elia, V.; Gnoni, M.G.; Tornese, F. Measuring circular economy strategies through index methods: A critical analysis. J. Clean. Prod. 2017, 142, 2741–2751. [Google Scholar] [CrossRef]
- Banaitê, D. Towards Circular Economy: Analysis of Indicators in the Context of Sustainable Development. Soc. Transform. Contemp. Soc. 2016, 4, 142–150. [Google Scholar]
- Camacho-Otero, J.; Boks, C.; Pettersen, I. Consumption in the Circular Economy: A Literature Review. Sustainability 2018, 10, 2758. [Google Scholar] [CrossRef] [Green Version]
- Corona, B.; Shen, L.; Reike, D.; Carreón, J.R.; Worrell, E. Towards sustainable development through the circular economy—A review and critical assessment on current circularity metrics. Resour. Conserv. Recycl. 2019, 151, 104498. [Google Scholar] [CrossRef]
- EASAC. Indicators for a Circular Economy; EASAC Secretariat Deutsche Akademie der Naturforscher Leopoldina: Halle (Saale), Germany, 2016; ISBN 9783804736801. [Google Scholar]
- Helander, H.; Petit-Boix, A.; Leipold, S.; Bringezu, S. How to monitor environmental pressures of a circular economy: An assessment of indicators. J. Ind. Ecol. 2019, 139, 1011. [Google Scholar] [CrossRef]
- Howard, M.; Hopkinson, P.; Miemczyk, J. The regenerative supply chain: A framework for developing circular economy indicators. Int. J. Prod. Res. 2019, 57, 7300–7318. [Google Scholar] [CrossRef] [Green Version]
- Iacovidou, E.; Velis, C.A.; Purnell, P.; Zwirner, O.; Brown, A.; Hahladakis, J.; Millward-Hopkins, J.; Williams, P.T. Metrics for optimising the multi-dimensional value of resources recovered from waste in a circular economy: A critical review. J. Clean. Prod. 2017, 166, 910–938. [Google Scholar] [CrossRef]
- Ioannidou, D.; Heeren, N.; Sonnemann, G.; Habert, G. The future in and of criticality assessments. J. Ind. Ecol. 2019, 23, 751–766. [Google Scholar] [CrossRef]
- Jain, S.; Jain, N.K.; Metri, B. Strategic framework towards measuring a circular supply chain management. Benchmarking 2018, 25, 3238–3252. [Google Scholar] [CrossRef]
- Janik, A.; Ryszko, A. [Duplikat] Circular economy in companies: An analysis of selected indicators from a managerial perspective. Multidiscip. Asp. Prod. Eng. 2019, 2, 523–535. [Google Scholar] [CrossRef] [Green Version]
- Mayer, A.; Haas, W.; Wiedenhofer, D.; Krausmann, F.; Nuss, P.; Blengini, G.A. Measuring Progress towards a Circular Economy: A Monitoring Framework for Economy-wide Material Loop Closing in the EU28. J. Ind. Ecol. 2019, 23, 62–76. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.; Singh, S.P.; Johansen, J.; Cheng, Y.; Farooq, S. Evaluating indicators for international manufacturing network under circular economy. Manag. Decis. 2019, 57, 811–839. [Google Scholar] [CrossRef]
- Moriguchi, Y. Material flow indicators to measure progress toward a sound material-cycle society. J. Mater. Cycles Waste Manag. 2007, 9, 112–120. [Google Scholar] [CrossRef]
- Parchomenko, A.; Nelen, D.; Gillabel, J.; Rechberger, H. Measuring the circular economy—A Multiple Correspondence Analysis of 63 metrics. J. Clean. Prod. 2019, 210, 200–216. [Google Scholar] [CrossRef]
- Pauliuk, S. [Duplikat] Critical appraisal of the circular economy standard BS 8001:2017 and a dashboard of quantitative system indicators for its implementation in organizations. Resour. Conserv. Recycl. 2018, 129, 81–92. [Google Scholar] [CrossRef]
- Sheldon, R.A. Metrics of Green Chemistry and Sustainability: Past, Present and Future. ACS Publ. 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Saidani, M. How to Assess Product Performance in the Circular Economy? Proposed Requirements for the Design of a Circularity Measurement Framework. Recycling 2017, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Walker, S.; Coleman, N.; Hodgson, P.; Collins, N.; Brimacombe, L. Evaluating the Environmental Dimension of Material Efficiency Strategies Relating to the Circular Economy. Sustainability 2018, 10, 666. [Google Scholar] [CrossRef] [Green Version]
- World Business Council for Sustainable Development (WBCSD). Circular Metrics Landscape Analysis. A Joint Report on the Current Landscape of Circular Metrics Use and Recommendations for a Common Measurement Framework; WBCSD: Geneva, Switzerland, 2018. [Google Scholar]
- Niero, M.; Kalbar, P.P. Coupling material circularity indicators and life cycle based indicators: A proposal to advance the assessment of circular economy strategies at the product level. Resour. Conserv. Recycl. 2019, 140, 305–312. [Google Scholar] [CrossRef]
- Spierling, S.; Venkatachalam, V.; Behnsen, H.; Herrmann, C.; Endres, H.-J. Bioplastics and Circular Economy—Performance Indicators to Identify Optimal Pathways. In Progress in Life Cycle Assessment; Schebek, L., Herrmann, C., Cerdas, F., Eds.; Springer International Publishing: Cham, Switerland, 2019; pp. 147–154. ISBN 978-3-319-92236-2. [Google Scholar]
- Huysman, S.; de Schaepmeester, J.; Ragaert, K.; Dewulf, J.; de Meester, S. Performance indicators for a circular economy: A case study on post-industrial plastic waste. Resour. Conserv. Recycl. 2017, 120, 46–54. [Google Scholar] [CrossRef]
- Kuznecova, I.; Babica, V.; Melecis, V.; Baranenko, D.; Ozarskis, M.; Gusca, J. Initial indicator analysis of bioethylen production pathways. Energy Procedia 2018, 147, 544–548. [Google Scholar] [CrossRef]
- Evans, J.; Bocken, N. Circular Economy Toolkit. Available online: http://circulareconomytoolkit.org (accessed on 6 November 2020).
- Gehin, A.; Zwolinski, P.; Brissaud, D. A tool to implement sustainable end-of-life strategies in the product development phase. J. Clean. Prod. 2008, 16, 566–576. [Google Scholar] [CrossRef]
- Linder, M.; Sarasini, S.; van Loon, P. A Metric for Quantifying Product-Level Circularity. J. Ind. Ecol. 2017, 21, 545–558. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.; Bras, B.; Allen, J.K. Applying Ecological Input-Output Flow Analysis to Material Flows in Industrial Systems: Part II: Flow Metrics. J. Ind. Ecol. 2004, 8. [Google Scholar] [CrossRef]
- Plevin, R.J.; Delucchi, M.A.; Creutzig, F. Using Attributional Life Cycle Assessment to Estimate Climate-Change Mitigation Benefits Misleads Policy Makers. J. Ind. Ecol. 2014, 18, 73–83. [Google Scholar] [CrossRef]
- Lotfy, W.A.; Ghanem, K.M.; El-Helow, E.R. Citric acid production by a novel Aspergillus niger isolate: II. Optimization of process parameters through statistical experimental designs. Bioresour. Technol. 2007, 98, 3470–3477. [Google Scholar] [CrossRef]
- Ärtzeblatt. Knapp 750.000 Herz-katheter-Eingriffe pro Jahr in Deutschland. Available online: https://www.aerzteblatt.de/nachrichten/60394/Knapp-750-000-Herzkatheter-Eingriffe-pro-Jahr-in-Deutschland (accessed on 16 January 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Value | Unit | Description |
|---|---|---|---|
| Input flows | |||
| Carbon dioxide | 2.82 × 10−3 | kg | Ingredient of sterilization gas |
| Corrugated board | 0.14 | kg | Secondary packaging |
| Ethylene oxide | 1.80 × 10−4 | kg | Ingredient of sterilization gas |
| Polyamide 6 fibres (PA 6) | 3.20 × 10−3 | kg | Pre-product for PEBAX® (shaft) |
| Polyetherimide granulate (PEI) | 0.11 | kg | Plug and handle |
| Polyethylene glycol (PEG) | 1.25 × 10−3 | kg | Pre-product for PEBAX® (shaft) |
| Polyethylene high density granulate | 0.02 | kg | Primary packaging |
| Polyethylene low density granulate | 3.00 × 10−4 | kg | Shaft stiffener |
| Polyurethane flexible foam (PU) | 8.00 × 10−4 | kg | Curvature and loop |
| Transporting capacity | 18.34 | kgkm | Small truck for final distribution in Germany |
| Transporting capacity | 2725.16 | kgkm | Sea route from California to Germany |
| Water (desalinated; deionized) | 2.00 × 10−3 | kg | Process water of manufacturing |
| Electricity; consumption mix | 0.36 | kWh | Electricity needed except for plastic production and processing |
| Output flows | |||
| Produced catheter | 1.00 | Item | Reference flow |
| Incineration good | 0.12 | kg | Waste treatment |
| Name | Value | Unit | Description |
|---|---|---|---|
| Input flows | |||
| Aromatics (steam cracking products) | 3.96 × 10−3 | kg | Pre-product of gluteral (ingredient of disinfectant Neodisher endo Sept GA) |
| Carbon dioxide | 2.82 × 10−3 | kg | Ingredient of sterilization gas |
| Citric acid | 8.80 × 10−3 | kg | Ingredient of detergent Sekusept aktiv |
| Corrugated board | 0.14 | kg | Secondary packaging |
| Electricity; consumption mix | 0.52 | kWh | Electricity needed expect plastic production and processing |
| Ethylene oxide | 1.80 × 10−4 | kg | Ingredient of sterilization gas |
| Hydrogen peroxide (100%) | 0.02 | kg | Ingredient of detergent Sekusept aktiv |
| Polyethylene high density granulate | 0.02 | kg | Primary packaging |
| Soda (sodium carbonate) | 5.77 × 10−3 | kg | Ingredient of detergent Sekusept aktiv |
| Sodium cumene sulphonate (40%) | 3.50 × 10−3 | kg | Ingredient of Neodisher endo CLEAN |
| Transporting capacity | 18.34 | kgkm | Small truck for distribution |
| Water (desalinated; deionized) | 5.00 | kg | Process water |
| Tap water | 7.00 | kg | Process water |
| Output flows | |||
| Produced catheter | 1.00 | Item | Reference flow |
| Incineration good | 0.11 | kg | Waste treatment |
| LCA Method Described in Section 2.1 | LCA Method Combined with the Circularity Metric Described in Section 2.2 | |
|---|---|---|
| Perspective of modeled comparison indicating environmental benefits of | Using a remanufactured or virgin catheter | Applying a linear or circular production system including remanufacturing |
| Functional unit | Identical (provision of a catheter) | |
| Method for setting system boundaries is based on | Cut-off | System expansion to consider several life cycles |
| Time horizon | Short-term | Long-term |
| Observed product cycles | Single | Multiple |
| Impact Category | Virgin Production Route | Medical Remanufacturing Route | Savings from Medical Remanufacturing Compared to Virgin Production per Catheter |
|---|---|---|---|
| Acidification terrestrial and freshwater [Mole of H+ eq.] | 4.73 × 10−3 | 1.18 × 10−3 | 75.1% |
| Cancer human health effects [CTUh] | 3.30 × 10−10 | 1.29 × 10−10 | 60.9% |
| Climate Change [kg CO2-eq.] | 1.75 | 0.87 | 50.4% |
| Ecotoxicity freshwater [CTUe] | 11.9 | 4.69 | 60.6% |
| Eutrophication freshwater [kg P eq.] | 6.29 × 10−6 | 7.87 × 10−6 | −25.1% |
| Eutrophication marine [kg N eq.] | 1.36 × 10−3 | 4.12 × 10−3 | 69.7% |
| Eutrophication terrestrial [Mole of N eq.] | 1.44 × 10−2 | 4.41 × 10−3 | 69.4% |
| Ionising radiation—human health [kBq U235 eq.] | 5.37 × 10−2 | 4.20 × 10−2 | 21.8% |
| Land Use [Pt] | 9.03 | 10.4 | −15.2% |
| Non-cancer human health effects [CTUh] | 1.56 × 10−8 | 7.39 × 10−9 | 52.6% |
| Ozone depletion [kg CFC-11-eq.] | 1.96 × 10−11 | 2.01 × 10−12 | 89.7% |
| Photochemical ozone formation—human health [kg NMVOC eq.] | 3.89 × 10−3 | 1.06 × 10−3 | 72.8% |
| Resource use, energy carriers [MJ] | 29.3 | 9.02 | 69.2% |
| Resource use, mineral and metals [kg Sb eq.] | 2.78 × 10−7 | 1.98 × 10−7 | 28.8% |
| Respiratory inorganics [Disease incidences] | 4.22 × 10−8 | 1.40 × 10−8 | 66.8% |
| Water scarcity [m³ world equiv.] | 1.09 × 10−1 | 1.13 × 10−1 | −3.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulte, A.; Maga, D.; Thonemann, N. Combining Life Cycle Assessment and Circularity Assessment to Analyze Environmental Impacts of the Medical Remanufacturing of Electrophysiology Catheters. Sustainability 2021, 13, 898. https://doi.org/10.3390/su13020898
Schulte A, Maga D, Thonemann N. Combining Life Cycle Assessment and Circularity Assessment to Analyze Environmental Impacts of the Medical Remanufacturing of Electrophysiology Catheters. Sustainability. 2021; 13(2):898. https://doi.org/10.3390/su13020898
Chicago/Turabian StyleSchulte, Anna, Daniel Maga, and Nils Thonemann. 2021. "Combining Life Cycle Assessment and Circularity Assessment to Analyze Environmental Impacts of the Medical Remanufacturing of Electrophysiology Catheters" Sustainability 13, no. 2: 898. https://doi.org/10.3390/su13020898