1. Introduction
The problems of medical resource shortages and an aging population have become increasingly prominent in China. The number of elderly people aged over 60 years in China is more than 200 million, accounting for 14.9% of the total population in China [
1]. This figure was significantly higher than the traditional aging society standard (10%) set by the United Nations. In particular, about 80%~90% of old people suffered from various chronic diseases and faced the corresponding pressures from home healthcare problems. According to the forecasting from the National Aging Committee of China, in the next 20 years, China would enter the period of its aging peak, and the old population (According to the China Report of the Development on Aging Cause 2013, the population aged 60 and over is counted as the old population. This statistical principle is based on the regulations on retirement age. In China, men currently can retire at the age of 60 years, while women who work in factories can retire as early as 50 years old. Additionally, women who work in public sectors can retire at the age of 55. Therefore, people aged 60 and over are regarded as the elderly.) is expected to increase at a sustained amount of 10 million per annum. In a word, the problem of “getting old before getting rich” has become more severe in China [
2].
As a new mode of health services, home healthcare service is more efficient, flexible and convenient, which can effectively alleviate the problem of medical resource shortages. Especially, it can reduce the medical cost and improve the service quality at the same time [
3,
4]. “Home healthcare” can be defined as home-visiting medical services provided by general practitioner service teams based on online and/or phone-call reservation systems. The patients include the elderly population (people aged 60 and over), families that have lost their only child, the disabled and other special populations. In developed countries, such as European countries (especially France), Australia and Canada [
5], home healthcare has played an increasingly important role in the healthcare systems. In recent years, some healthcare services in the U.S. have been transferred from hospitals to patient’s homes [
6]. Additionally, the demand for home healthcare services has shown an increasing trend in many developed countries over the years. The market for home healthcare in the U.S. exceeded $7.7 billion in 2012 [
7]. The development of home healthcare in developed countries has proven that it is conducive to alleviating medical resource imbalances, reducing the costs of healthcare systems, increasing the life quality of patients and improving the degree of patient satisfaction [
8].
In order to cope with the medical problems resulting from an aging population, the Chinese government has paid more attention to the promotion of home healthcare services in recent years. Take Shanghai as an example. In order to explore the service mode of “developing community health services provided by healthcare teams dominated by general practitioners” (in the medical profession, a general practitioner (GP) is a medical doctor who treats acute and chronic illnesses and provides preventive care and health education to patients), 11 pilots of community health centers have been set up in Changning, Putuo and other districts in Shanghai since 2003. As of 2014, the system of family doctors or nurse practitioners was established for all community health centers in Shanghai, and about 1/6 of the residents signed home care nursing service contracts with family doctors.
As China’s most populous city, Shanghai is facing a serious challenge of aging population. Therefore, the investigation of Shanghai on the barriers, as well as decisive factors of the development of home healthcare services can be a good reference for other regions in China. Based on this concern, we conducted a face-to-face survey in several districts in Shanghai to explore the influencing factors of the development of home healthcare services. The results indicate that the location of service centers for home healthcare is decisive for the improvement of patient satisfaction, which is of paramount importance for medical service providers. However, although many scholars have conducted research on the determinants of patient satisfaction [
9], there is no agreed definition of the concept of patient satisfaction, because satisfaction is multi-dimensional [
10,
11]. According to the results from the face-to-face survey in China [
12], there are four indexes for measuring patient satisfaction in home healthcare: first, response time; second, patient wait time; third, service quality; fourth, service price. In general, response time is affected by factors, such as the level of convenience in contacting, as well as the number of medical staff. Patient wait time, a quality indicator of home healthcare services, is influenced by location planning of service centers for home healthcare, as well as the scheduling and dispatching of medical staff. Service quality in home healthcare is affected by the levels of healthcare workers and the degree of advancement of medical equipment. Service price is influenced by the pricing scheme or the price specifications regulated by the government. Particularly, the inappropriate location of service centers for home healthcare, which is a decisive factor influencing whether medical staff are able to provide timely and convenient services for patients, is the major determinant of patient satisfaction. Therefore, the location planning problem of service centers for home healthcare becomes particularly important.
The contributions of this study are summarized as follows: (1) we investigate the current situation of home healthcare in Shanghai, so as to explore the influencing factors of the development of home healthcare services, which can provide a valuable reference for the location planning of service centers for home healthcare in other regions in China; (2) we propose a location planning model that considers the actual constraints and then conduct a sensitivity analysis to optimize the current layout of the service centers for home health to a certain extent; (3) based on the empirical analysis of Shanghai, we provide some policy implications for the decision makers to build an effective location plan and promote the sustainable development of China’s home healthcare.
The rest of this paper will be organized as follows. A concise literature review is presented in
Section 2.
Section 3 discusses the data collection and presentation.
Section 4 constructs the location optimization model.
Section 5 provides the empirical analysis and relevant results in this study. Finally, the conclusion will be given in
Section 6.
2. Literature Review
Many scholars have conducted research on the application of home healthcare [
13,
14,
15]. In addition, in recent years, the sustainability of healthcare has also attracted increasing attention from researchers and policy makers [
16,
17,
18].
The location planning problem is a classical problem in the field of operations research. In other words, the solution to the problem aims to maximally meet the resource demand by a given number of facilities. Specifically, the intermediate value problem, the maximal covering location problem and the center problem are the three classical models of the location problem. The solution to the intermediate value problem, which could provide the shortest distances from service requiring places to the destinations, was posed by Hakimi in 1964 [
19]. The covering location problem can be divided into the maximal covering location problem and the set covering location problem. Church and ReVelle [
20] posed the maximal covering location problem by restricting the optimal location sites of the service centers to the network nodes. The set covering location problem was first posed by Roth [
21], who resolved the location problem of fire centers, the optimal ambulance location and other emergency service facilities. Different from the set covering the location problem, the center problem is the minimax problem, which calculates the minimax distance from any service requiring places to the nearest facilities under the constraint of a fixed number of facilities.
As of now, much research has been done to solve the location problem in the medical field. In order to optimize the location of hospitals, Liu and Li [
22] built a Pareto multi-objective generic algorithm location model. Diao and Jiang [
23] not only introduced factors, such as customer preference and traffic weight, but also simulated the monthly number of hospital visits using the Monte Carlo method. Vahidnia
et al. [
24] utilized a fuzzy analytic hierarchy process to optimize the hospital location by combining a geographic information system (GIS). Soltani and Marandi [
25] studied the potential location for hospitals based on fuzzy multiple criteria decision making (MCDM). Varnakovida and Messina [
26] performed an empirical analysis for the location of community hospitals in Michigan, U.S. Kim
et al. [
27] adopt branch and bound algorithms to determine the location for long-term care facilities. Toregas
et al. [
28] presented the emergency facilities as a set covering problem and solved this problem using linear programming. To optimize the location approaches, the problems of location and capability deployment were also considered by Cong
et al. [
29] in the study of the network location problem of home healthcare centers under a certain demand.
Research on the problem of the location planning of service centers for home healthcare is still relatively scarce [
30,
31,
32]. Compared to the traditional healthcare service, home healthcare is special considering that the medical staff needs to offer visiting services, and patient satisfaction drops with longer waiting time [
33,
34,
35,
36]. However, if the waiting time exceeds the acceptable and tolerable limit, there would be an exponential plummet in patient satisfaction, and patient satisfaction could even drop to zero when patients terminate a service request for home healthcare and choose other kinds of medical services [
12]. Meanwhile, the number of medical staff of different levels also has an impact on the capabilities of each service center. Based on the above analysis, this paper tries to build a location model of service centers for home healthcare to reduce medical cost and improve medical efficiency.
In this paper, two versions of questionnaires (questionnaires for individuals and medical staff) are designed to investigate the current situation and problems of home healthcare in Shanghai. The results indicate that unreasonable location planning is a crucial factor for patient dissatisfaction. Therefore, we build a mixed integer programming model that considers various actual constraints. In order to validate the effectiveness of the proposed model and methodology, we conduct a case study of Putuo district in Shanghai and the sensitivity analysis of the proposed optimization model. Results indicate that the proposed model can provide a reference for decision makers to solve the location planning problem of service centers for home healthcare, so as to improve the efficiency, as well as the levels of home healthcare services in China.
3. Data Collection and Presentation
3.1. Variables and Data Collection
According to the data from the Chinese Health and Family Planning Statistical Yearbook [
37], we can see that the number of patients visiting community health centers increased greatly during 2003–2012, while the number of patients visiting hospitals and other medical institutions decreased correspondingly (See
Figure 1). Specifically, the number of patients visiting hospitals dropped from 143.34 thousand persons in 2003 to 62.89 thousand persons in 2012, and the average annual decrease rate was 7%. Comparatively, the number of patients visiting community health centers increased from 564.84 thousand persons in 2003 to 1155.17 thousand persons in 2012, which was equivalent to a growth of 104.5%.
Figure 1.
Number of patients visiting different types of medical institutions in Shanghai. Data source: Chinese Health and Family Planning Statistical Yearbook [
37].
Figure 1.
Number of patients visiting different types of medical institutions in Shanghai. Data source: Chinese Health and Family Planning Statistical Yearbook [
37].
In order to do further research on home healthcare services, we conducted an in-depth survey on the major challenges, as well as obstacles for the sustainable development of home healthcare in Shanghai, China. Variables and data of the following part used in this paper are based on the face-to-face survey. The survey was launched by the Business School of East China Normal University in the first half of 2015. We designed two kinds of questionnaires: questionnaires for medical staff and questionnaires for individuals. Medical staff include doctors, nurses and administrative staff of hospitals. Individuals are mainly residents in Shanghai. The respondents (individuals) in our survey include patients in the hospitals, patients in the community health centers, home care patients and households in communities in various districts in Shanghai. Therefore, individuals in this paper refer to the broader community. Much effort has been made to improve the design of the questionnaires. For instance, we gathered advice from medical staff in relative departments of hospitals to improve the questionnaire design and to ensure the scientificity and effectiveness of the questionnaires. In addition, in order to guarantee the validity of the survey, we adjusted and amended the questionnaires several times after interviewing administrative staff and staff members of home health centers. Especially, aiming at redesigning and improving the quality of the survey, the pre-test survey were conducted twice to identify problems related to questionnaire design. It is important to test the effectiveness of the survey questionnaire before actually using it to collect data. In other words, pretesting and piloting help identify questions that do not make any sense to participants or problems that might lead to biased answers.
We experienced several problems related to the question and questionnaire design during the pre-test of the questionnaire. For example, some respondents could not completely and accurately fill out the forms because of the unclear classification of hospitals in the previous questionnaire. Generally, hospitals in China are organized according to a three-tier system, and hospitals are designated as primary, secondary or tertiary institutions. Therefore, in the pre-test questionnaire, we only provided the above three options for respondents to choose. However, hospitals in different districts in Shanghai have a more detailed subdivision, and therefore, the related questions and answer options for survey questions should be designed more precisely. Another problem is that the demographics of families, including nuptiality, family structure, living arrangements, and so on, are diversified and complicated, and the answer options for survey questions in the previous questionnaire cannot fully cover the various situations. Other problems include: (1) some respondents are still unfamiliar with the definition, as well as the scope of home healthcare services; (2) some respondents have never used home healthcare services, the answers of whom might influence the effectiveness of the questionnaires; (3) some respondents cannot give accurate answers to questions due to the lack of medical knowledge. Therefore, in order to obtain more accurate answers, on the one hand, we revised and improved the design of specific questions; on the other hand, we trained the investigators to provide more detailed explanations to respondents on several questions during the actual face-to-face survey.
Questionnaires for individuals are designed to investigate the expectations and the degrees of urgency of demand for home healthcare of households at different ages, with different income levels and living situations. The urgency of home healthcare in our survey is measured by the degree of urgency of demand in home healthcare services at different ages. In general, we could expect that there would be more people requiring home healthcare in China, and the degree of urgency of demand for home healthcare services would increase with age. First, there would be more people suffering from chronic illnesses or physical disabilities due to the aging population. Second, the number of frail elderly people would rise due to a higher life expectancy. Third, specific healthcare conditions, such as recovering from surgery or acute illnesses, often need consistent and further medical treatment at home. Based on the above analysis, we set the specific question in the questionnaire as follows:
Would you please describe the degree of urgency of demand for home healthcare services?
A. I am in urgent need.
B. I am in need of home healthcare, but it is not urgent.
C. I do not need them.
The top three reasons for respondents who are in urgent need of home healthcare are summarized as follows: (1) the respondent is a chronic disease patient or physically-disabled patient; (2) the respondent cannot stand the long waiting times, as well as the high-cost health expenses for receiving treatment at hospitals; (3) the respondent prefers to receive medical treatment at home because he/she is unsatisfied with the treatment environment of hospitals.
Questionnaires for staff in hospitals mainly focus on their attitudes towards home healthcare services and their expectations of possible medical-supporting funds, facilities and payment for medical staff.
The data processing and expected objectives of the questionnaires on home healthcare (overview) are as follows:
1. Questionnaires for individuals:
- (1)
Demands for home healthcare among different groups (indexes of analysis: age, income level, living conditions, etc.).
- (2)
Understanding levels of the system of family doctors or nurse practitioners among different groups (indexes of analysis: age, educational level, etc.).
- (3)
The degrees of familiarity with healthcare institutions around the accommodations or work places among different groups (indexes of analysis: age, income level, etc.).
- (4)
The degrees of familiarity with commercial health insurance or medical insurance among different groups (results from the survey on commercial insurance are used for comparison).
2. Questionnaires for staff working in hospitals:
- (1)
The attitudes of doctors and nurses toward home healthcare services.
- (2)
The current or expected ways of providing home health services by hospitals.
- (3)
The expected facilities and possible medical-supporting funds provided by hospitals for home healthcare services.
The survey is aimed at not only learning about the general situation of home healthcare in Shanghai city, but also analyzing the influencing factors of the sustainable development of home healthcare at the micro-level. Considering that there is a large number of health centers in Shanghai, we only selected a few representative districts (Putuo, Xuhui, Minghang, Changning,
etc.) for our investigation (see
Figure 2). The most prestigious medical centers in Shanghai, including Shanghai Sixth People’s Hospital, Shanghai Putuo District Central Hospital, Shanghai Minhang District Central Hospital and several hospitals in the Caoyang district, are investigated in our survey. In addition, we conducted an in-depth study on home healthcare by doing face-to-face interviews with doctors, nurses and administrative staff in the above-mentioned hospitals. The total number of questionnaires is 511, for which the number of valid questionnaires is 493, and the number of questionnaires for individuals is 319.
Figure 2.
The representative districts of Shanghai for the survey.
Figure 2.
The representative districts of Shanghai for the survey.
3.2. Data Presentation
Some investigation results are presented as follows:
Figure 3 shows that 62% of respondents are in need of home healthcare services, but the need is not urgent; 9% of respondents are in urgent need of home healthcare services; and 29% of respondents do not need home healthcare services.
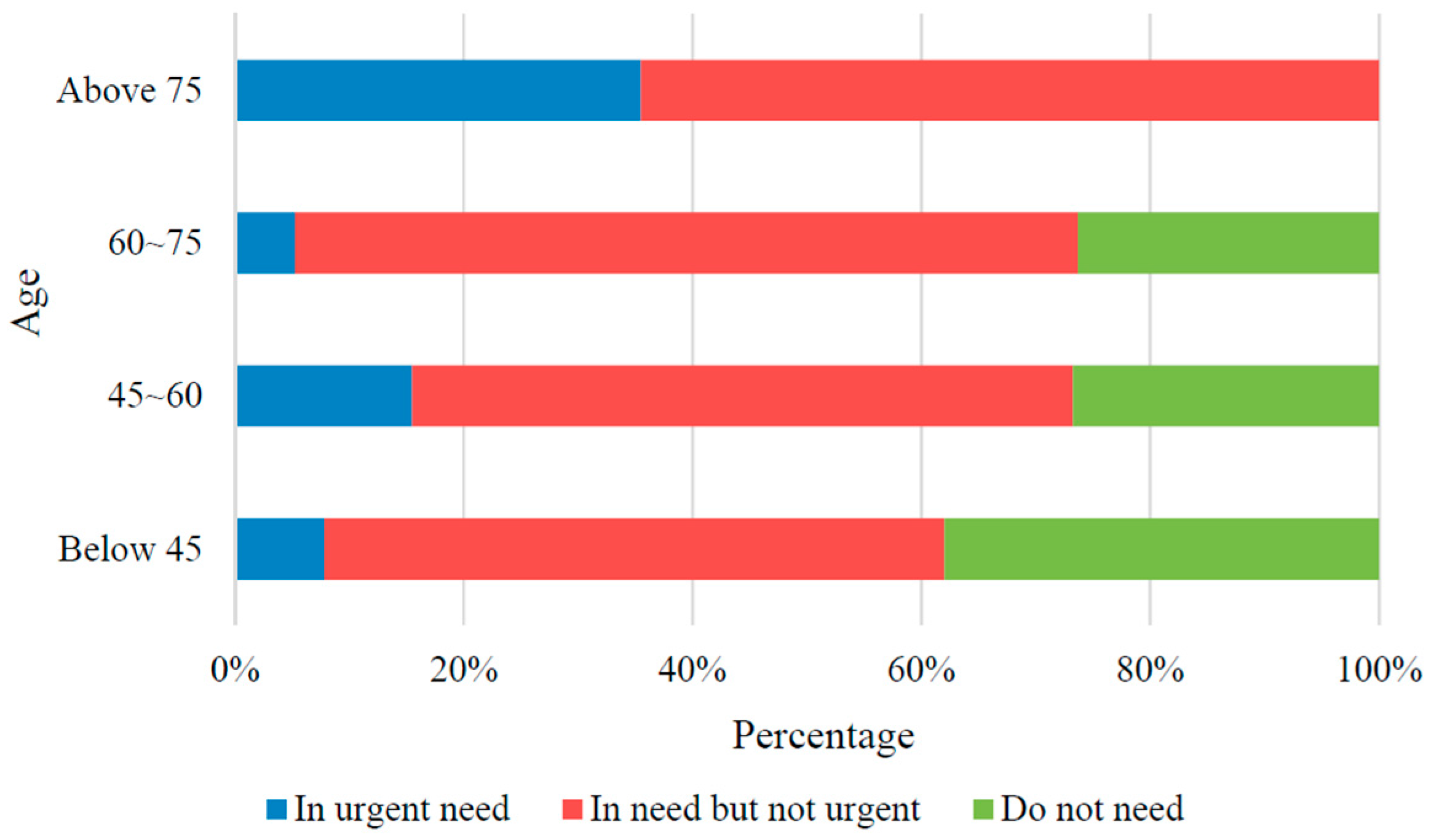
We further investigate the urgency of demand for home healthcare at different ages. As shown in
Figure 4, residents aged below 45 showed the lowest demand for home healthcare, for which about 35 percent of respondents do not need home health services. However, the demand for home healthcare services rises gradually with age, and the share of “in urgent need” is the highest for residents aged over 75 (35.5%).
Further, we investigated the satisfaction degree of respondents who received healthcare services at home. Results show that the overall satisfaction rate is 79.8%. Specifically, the share of high ratings for home healthcare services is 2.5%; the share of middle-high ratings for home healthcare services is 25.8%; and the share of moderate ratings is 51.5% (see
Figure 5).
Figure 3.
The demand for home healthcare.
Figure 3.
The demand for home healthcare.
Figure 4.
Demands for home healthcare of respondents at different ages.
Figure 4.
Demands for home healthcare of respondents at different ages.
Figure 5.
The degrees of satisfaction of respondents on home healthcare services.
Figure 5.
The degrees of satisfaction of respondents on home healthcare services.
We further investigate the reasons behind patient dissatisfaction, and the results are shown in
Figure 6:
Figure 6.
Reasons for not choosing home healthcare services.
Figure 6.
Reasons for not choosing home healthcare services.
As shown in
Figure 6, one of the major reasons for patient dissatisfaction is that the requirements of patients cannot be met by medical staff in a timely manner. Additionally, the limited capability of home healthcare services that could not meet patients’ expectations is another reason for patient dissatisfaction.
According to the results of the questionnaires, the inappropriate location of service centers for home healthcare was an important obstacle for the further promotion and development of home healthcare in China. In summary, the major reasons for residents who are unwilling to choose home healthcare services are: (1) the inadequacy of the local healthcare infrastructure and medical devices, (2) inefficient healthcare services; (3) the inadequacy of the capabilities of medical staff; (4) inconvenient contact methods. We should note that some of the above problems, such as inefficient healthcare services and inconvenient contact methods, could be addressed through process improvement initiatives, known as Kaizen events (Kaizen means “improvement” in Japanese, and Kaizen events focus on implementing improvements to the process of meeting customer demands) [
38]. Therefore, we undertake a root cause analysis to alleviate or even eliminate the above problems.
- (1)
“The inadequacy in the local healthcare infrastructure and medical devices” is mainly caused by the lack of funding to support home care services. The solutions could be: first, seeking to optimize investments in home healthcare; second, looking for financial assistance to increase medical devices; third, seeking government financial support to the home healthcare industry.
- (2)
Reasons for “inefficient healthcare services” are as follows: first, there is not enough staff to pick up telephone calls; second, the imperfect customer service response mechanism; third, ineffective communication; fourth, long wait times for health services. Possible solutions could be: first, increasing medical staff; second, optimizing the dispatch and scheduling of healthcare staff; third, creating a reasonable location plan of service centers for home healthcare; fourth, under the constraint of limited medical resources, further optimizing the allocation of medical staff in the aspects of workload assignment and minimizing the traveling time of nurse practitioners.
- (3)
The main reason for “the inadequacy in the capabilities of medical staff” is that there is not enough medical staff, especially senior doctors and skilled medical staff. Possible solutions could be: first, conducting medical staff training; second, attracting more skilled medical staff to join the home healthcare industry.
- (4)
The main reason for “inconvenient contact method” is the inadequacy of modern communication services. The problem can be solved by providing better online customer support and online reservation services, developing customized telephone booking services, providing reservation services based on mobile application system, etc.
In conclusion, home healthcare services in China still have shortcomings in terms of management and operational efficiency. The delayed or late responses of medical staff to the patients’ demands are the major reasons for patient dissatisfaction. Due to this reason, the inefficient services have resulted in the distrust of patients for home healthcare. Therefore, in order to improve the operational efficiency and to achieve the effective allocation of medical resources, it is necessary to build an optimized model to solve the location planning problem of service centers for home healthcare [
39].
4. Construction of the Optimization Model
This paper focuses on how to resolve the location planning problem of home health centers with the unknown candidate service centers for home healthcare and service-requiring places (considering the constraints of the capabilities of service facilities and differentiated service competencies). The model is based on the following basic assumptions:
- (1)
The service demands in each phase are certain;
- (2)
The existing health centers shall not be closed, and the size of the health centers can be expanded in the next phase;
- (3)
Healthcare services of the existing centers shall not be stopped, and we do not consider the situation of firing employees;
- (4)
Wages and unit travel cost of medical staff would not change with time.
The model in this paper uses the following subscripts, parameters and variables:
Subscripts:
i represents the i-th service center (i = 1, …, I);
j represents the j-th destination (j = 1,…, J);
k represents the k-th type of service (k = 1,…, K);
l represents the services provided by the l-th grade medical staff (l = 1,…, L);
t represents the t-th time phase (t = 1,…, T).
Parameters:
ci represents the investment cost of building the i-th service center, which is related to the geographic location;
ck represents the investment cost to open the k-th type of service (namely the professional equipment cost), which is related to the service type;
ck’ represents the hourly wage of the medical staff providing the k-th type of service;
cij represents the transportation cost of providing one service from the i-th service center to the j-th service-requiring place;
djkt represents the demand of the k-th type of service for the j-th service-requiring place in the t-th time phase;
τk represents the execution time of the k-th type of service;
tij represents the transportation time from the i-th service center to the j-th service-requiring place (namely response time of demand); therefore, the total time for the i-th service center to provide the k-th type of service for the j-th service-requiring place is τk + 2tij;
α represents the time value of money;
αt−1 represents the time value coefficient of capital in the t-th time phase; the time value of money means a certain amount of currency held at present will have a higher value in the future;
Fi represents the maximum size of the i-th service center, and it is related to the floor area and other factors of the service center;
Hlt represents the maximum number of the l-th grade of medical staff in the t-th time phase;
P represents the minimum satisfactory rate of the service-requiring place;
Uk represents the maximum response time of the k-th type of service (maximum transportation time from service centers to service-requiring places);
Ek represents the customer expected response time of the k-th type of service.
Decision variables:
xit is a binary variable and represents whether the i-th service center is built in the t-th time phase (one: yes; zero: no);
yikt is a binary variable and represents whether the k-th type of service is launched by the i-th service center in the t-th time phase (one: yes; zero: no);
nilkt represents the capability to provide the k-th type of service by the l-th grade of medical staff from the i-th service center in the t-th time phase;
zijkt is a binary variable and represents the percentage for the i-th service center to meet the demands from the j-th service-requiring place while providing the k-th type of service in the t-th time phase.
The mathematic model is as follows:
The constraints are as follows:
Objective Equation (1) represents the model with the lowest total cost and includes four items. The first item represents the total investment cost of building the service center, while the second item represents the total investment cost of starting the business. Both of the items have considered the time value of money. The third item represents the total labor cost of the service center, and the fourth item represents the total transportation cost of providing the service.
Constraint Equation (2) denotes that services can be provided for customers only if the service center has already been built;
Constraints Equations (3) and (4) represent that a particular service can be provided only if the service has been launched by the service center;
Constraint Equation (5) represents that the capacity of the service center cannot exceed its limits;
Constraint Equation (6) represents that the total services provided by each service center shall meet the restrictions of the service capacity of each service center;
Constraint Equation (7) represents that there is a maximum number of medical staff of each grade;
Constraint Equation (8) represents that the demands of each service-requiring place shall be met proportionally;
Constraint Equation (9) represents that the degree of satisfaction will decrease with the increasing waiting times; once the response time of the medical staff has exceeded the expectations of the customers, especially, the healthcare services will become invalid after exceeding the maximum response time;
Constraints Equations (10) and (11) represent that the existing service centers or services cannot be closed or terminated;
Constraints Equations (12)–(14) represent the value range of the variables.
5. Empirical Analysis
We take service centers for home healthcare in Putuo district in Shanghai as an example for the empirical analysis in this paper. There are eight sub-districts and two towns in Putuo district, namely the sub-districts of Changshou Road, Yichuan Road, Ganquan Road, Shiquan Road, Changfeng Xincun, Caoyang Xincun, Wanli, Zhenru, as well as the towns of Taopu and Changzhen. The population of this district is about 1.3 million. Calculated from the research data, there are about 0.85 million people in the potential target market of home healthcare. In this paper, we try to verify the effectiveness of the model through the research on the location problem of the home health centers in Putuo district at Shanghai, China. The following numerical calculation is achieved by running IBM ILOGCPLEX Program 12.6 under the Windows 7 operating system.
5.1. Existing Condition of Service Point Location
Firstly, we can check whether the existing service centers for home healthcare can meet the requirements of the residents using the location model in this paper. Home healthcare services of Putuo district are mainly provided by the community health centers of Changshou Sub-district, Yichuan Sub-district, Ganquan Sub-district, Shiquan Sub-district, Changfeng, Baiyu, Caoyang, Zhenru Town, Taopu Town and Changzheng Town. Relevant data of these ten main service centers are shown in
Table 1.
The opportunity cost for building a community health center can be calculated by the area of a service center multiplied by the rent level in the community. The number of maximum members determines the maximum annual capability of each service center (the number of maximum members × the annual workload). Taking the current data as the data in the first year, the maximum capacity of the second year will increase proportionally with the increase in the planned area (shown in
Table 2).
At present, healthcare services provided by each service center can be classified into “hospital bed at home” and “health record establishment”. The former means that patients can receive medical treatment and care in a familiar environment by transferring the treatment places from hospitals to homes, and the latter means that family doctors or nurse practitioners will create and maintain the authoritative records of physical and psychological health for community residents by providing visiting services. Relevant data of these two services and other relevant data are shown in
Table 3.
Table 1.
Relevant data of community health centers.
Table 1.
Relevant data of community health centers.
| Community Health Centers | Total Area (m2) | Planned Increased Area (m2) | Nearby Rent (RMB/m2) | Max Members of the Service Center (Persons) | Total Number of Medical Staff at Different Levels (Persons) |
|---|
| Primary | Intermediate | Advanced |
|---|
| Changshou Sub-district (i1) | 1978 | 514 | 3100 | 20 | 8 | 10 | 2 |
| Yichuan Sub-district (i2) | 6024 | 489 | 2200 | 40 | 15 | 18 | 7 |
| Ganquan Sub-district (i3) | 2236 | 218 | 2200 | 25 | 10 | 12 | 3 |
| Shiquan Sub-district (i4) | 2647 | 345 | 2000 | 20 | 6 | 12 | 2 |
| Changfeng Community (i5) | 4987 | 678 | 3200 | 35 | 15 | 15 | 5 |
| Baiyu Community (i6) | 1616 | 1000 | 3000 | 15 | 8 | 4 | 3 |
| Caoyang Community (i7) | 6074 | 845 | 2100 | 50 | 21 | 20 | 9 |
| Zhenru Town (i8) | 3961 | 987 | 2200 | 30 | 10 | 15 | 5 |
| Taopu Town (i9) | 6280 | 879 | 1000 | 50 | 18 | 24 | 8 |
| Changzheng Town (i10) | 4600 | 678 | 2000 | 35 | 15 | 15 | 5 |
Table 2.
Input data of community health centers.
Table 2.
Input data of community health centers.
| Community Health Centers | Annual Investment Cost (Million RMB) | Service Capacity of the 1st Year (Thousand Hours) | Service Capacity of the 2nd Year (Thousand Hours) |
|---|
| Changshou Sub-district | 6.13 | 40 | 50.39 |
| Yichuan Sub-district | 13.25 | 80 | 86.49 |
| Ganquan Sub-district | 4.91 | 50 | 54.88 |
| Shiquan Sub-district | 5.29 | 40 | 45.21 |
| Changfeng Community | 15.95 | 70 | 79.52 |
| Baiyu Community | 4.84 | 30 | 48.56 |
| Caoyang Community | 12.75 | 100 | 113.91 |
| Zhenru Town | 8.71 | 60 | 74.95 |
| Taopu Town | 6.28 | 100 | 114.00 |
| Changzheng Town | 9.20 | 70 | 80.32 |
The settlements of residents are randomly distributed; therefore, the service-requiring places input into this model are also randomly generated (shown in
Table 4). In addition, the demand data are randomly generated after determining the threshold in accordance with the research results. Additionally, the demand of the second year is calculated by the 10% increase compared to that of the first year.
However, after inputting these data into the proposed model, an infeasible solution results. After debugging, we find that a feasible solution can be obtained only by decreasing the minimum satisfactory rate of demand to 74%, which means that those 10 candidate service centers need to be opened in the first year. This also indicates that even if all service centers are operated completely at present, only about 74% of the demands can be met. In this case, the optimal configuration is shown in
Table 5.
Table 3.
Relevant data in this paper.
Table 3.
Relevant data in this paper.
| Relevant Data of Service |
|---|
| Services | Annual Investment Cost (RMB) | Service Payment (RMB/Hour) | Execution Time (Hour) | Maximum Response Time (Hour) |
|---|
| Hospital bed at home (k1) | 20,000 | 30 | 1 | 0.5 |
| Health records establishment (k2) | 10,000 | 15 | 0.5 | 0.5 |
| Other Relevant Data |
| Parameters | Minimum percentage of demand satisfied for each service-requiring place | Annual workload of medical staff providing home healthcare services (hours) | Unit transportation speed (km/hour) | Unit transportation cost (RMB/km) |
| Values | 90% | 2000 | 10 | 2 |
Table 4.
Results of randomly-generated demands.
Table 4.
Results of randomly-generated demands.
| Service | Hospital Bed at Home (Hours) | Health Records Establishment (Hours) |
|---|
| Demand | | The 1st year | The 2nd year | The 1st year | The 2nd year |
|---|
| j1 | 5543 | 6098 | 1679 | 1847 |
| j2 | 5020 | 5522 | 1427 | 1569 |
| j3 | 4054 | 4459 | 1188 | 1306 |
| j4 | 4451 | 4896 | 1959 | 2155 |
| j5 | 4224 | 4647 | 1221 | 1344 |
| j6 | 5572 | 6129 | 1343 | 1477 |
| j100 | 6404 | 7045 | 1057 | 1163 |
It can be seen from
Table 5 that the service of the hospital bed at home cannot be met. Therefore, the results need to be further optimized.
Table 5.
The optimal configuration of service capacity under the present situation.
Table 5.
The optimal configuration of service capacity under the present situation.
| Community Health Centers | Number of Persons in the 1st Year | Number of Persons in the 2nd Year |
|---|
| | Hospital bed at Home | Health Records Establishment | Hospital Bed at Home | Health Records Establishment |
|---|
| Changshou Sub-district (i1) | 17 | 3 | 22 | 4 |
| Yichuan Sub-district (i2) | 34 | 6 | 37 | 6 |
| Ganquan Sub-district (i3) | 21 | 4 | 23 | 4 |
| Shiquan Sub-district (i4) | 20 | | 23 | |
| Changfeng Community (i5) | 29 | 6 | 32 | 8 |
| Baiyu Community (i6) | 12 | 3 | 19 | 5 |
| Caoyang Community (i7) | 41 | 9 | 51 | 6 |
| Zhenru Town (i8) | 30 | | 30 | 7 |
| Taopu Town (i9) | 39 | 10 | 26 | 4 |
| Changzheng Town (i10) | 30 | 5 | 35 | 5 |
5.2. Service Point Location Optimization
In order to resolve the problem of unmet demands, it is possible to better meet the needs of the residents by building some new home health centers in the populated areas or improving the service efficiency. The service efficiency could be improved by the following methods: first, minimize the idle time by scheduling and dispatching medical staff; second, minimize the routes, as well as transportation time from service centers to targeted locations by optimizing the route arrangement; third, conduct customer training for medical staff. This paper mainly adopts the location model to optimize the re-layout of the home health centers. According to the above results, three candidate service centers should be built respectively in Wanli Sub-district, Changzheng Town and Taopu Town. Based on the above analysis, there would be 13 candidate service centers. The distribution of the service centers can be referred to in
Figure 7 and
Table 6.
Figure 7.
Candidate community health centers of Putuo district in Shanghai.
Figure 7.
Candidate community health centers of Putuo district in Shanghai.
Table 6.
Relevant data of the new service centers of three candidate points.
Table 6.
Relevant data of the new service centers of three candidate points.
| Community Health Centers | Required Area (m2) | Increased Area in the 2nd Year (m2) | Max Members (Persons) | Investment Cost (Million RMB) |
|---|
| Candidate 1 | 4000 | 700 | 35 | 8 |
| Candidate 2 | 4000 | 700 | 35 | 7.2 |
| Candidate 3 | 4000 | 700 | 35 | 4 |
If the minimum satisfactory rate of demand is 90%, inputting the relevant data of these 13 service centers and the original service-requiring places into this model would obtain the following results (shown in
Table 7).
Compared to the previous results, home healthcare services will be launched in the three new candidate service centers based on the new location results by cancelling the Changshou Road and Changfeng Xincun community health centers (Shown in
Figure 8). A comparison of the results (shown in
Table 8) indicates that the new layout of the service centers can not only improve the demand satisfaction rate from 70% to 90%, but also can decrease the total cost by 0.44 million RMB in two years. Therefore, this optimization scheme is effective and feasible.
Table 7.
Computational results of service centers that should be opened.
Table 7.
Computational results of service centers that should be opened.
| Service Centers | The 1st Year | The 2nd Year |
|---|
| Hospital Bed at Home | Health Records Establishment | Hospital Bed at Home | Health Records Establishment |
|---|
| Changshou Sub-district (i1) | × | × | × | × |
| Yichuan Sub-district (i2) | √ | √ | √ | √ |
| Ganquan Sub-district (i3) | √ | √ | √ | √ |
| Shiquan Sub-district (i4) | √ | √ | √ | √ |
| Changfeng Community (i5) | × | × | × | × |
| Baiyu Community (i6) | √ | √ | √ | √ |
| Caoyang Community (i7) | √ | √ | √ | √ |
| Zhenru Town (i8) | √ | √ | √ | √ |
| Taopu Town (i9) | √ | √ | √ | √ |
| Changzheng Town (i10) | √ | √ | √ | √ |
| Candidate 1 (i11) | √ | √ | √ | √ |
| Candidate 2 (i12) | √ | √ | √ | √ |
| Candidate 3 (i13) | √ | √ | √ | √ |
Figure 8.
The comparative diagram of opening community health centers with two schemes.
Figure 8.
The comparative diagram of opening community health centers with two schemes.
Table 8.
Comparison between the current condition and the optimized scheme.
Table 8.
Comparison between the current condition and the optimized scheme.
| | Current Condition | Optimized Scheme |
|---|
| Service centers | Changshou Sub-district, Yichuan Sub-district, Ganquan Sub-district, Shiquan Sub-district, Changfeng, Baiyu, Caoyang, Zhenru Town, Taopu Town, Changzheng Town community health centers | Yichuan Sub-district, Ganquan Sub-district, Shiquan Sub-district, Baiyu, Caoyang, Zhenru Town, Taopu Town, Changzheng Town community health centers as well as candidates 1, 2 and 3 |
| Quantity of service centers | 10 | 11 |
| Total cost | 207.15 million RMB | 206.71 million RMB |
| Satisfactory rate of demand | More than 74% | More than 90% |
5.3. Sensitivity Analysis of the Optimization Model
We conducted a sensitivity analysis of the demands based on the decision making model. In this process, we assume the number of demand points to be unchanged, while the demand at each demand point changes over time. In this paper, a demand point stands for a household that needs home healthcare. The demand change at each demand point represents the increase or decrease of different types of home healthcare services.
As shown in
Figure 9, the total system cost increases linearly with an upsurge in demand, while the average time of responses showed a stepwise reduction with the growth of demand. When the demand expanded, decision makers would increase service centers for home healthcare and adjust the arrangement of workers, so that the average time of response would be reduced.
Figure 9.
The impact of demand changes on the total cost and the average response time.
Figure 9.
The impact of demand changes on the total cost and the average response time.
When the demand changes (x times of demand) reached over 1.4, the average time of response would reach a minimum value and remain constant. Meanwhile, when all of the service centers are opened, the increase of the overall cost would only be affected by labor cost and transportation cost.
For the case of 26 demand points, it takes about 2 min for the CPLEX program to identify an optimal solution to the location-allocation problem. However, with the increased quantity of demand points, there would be a rapid rise in computing time.
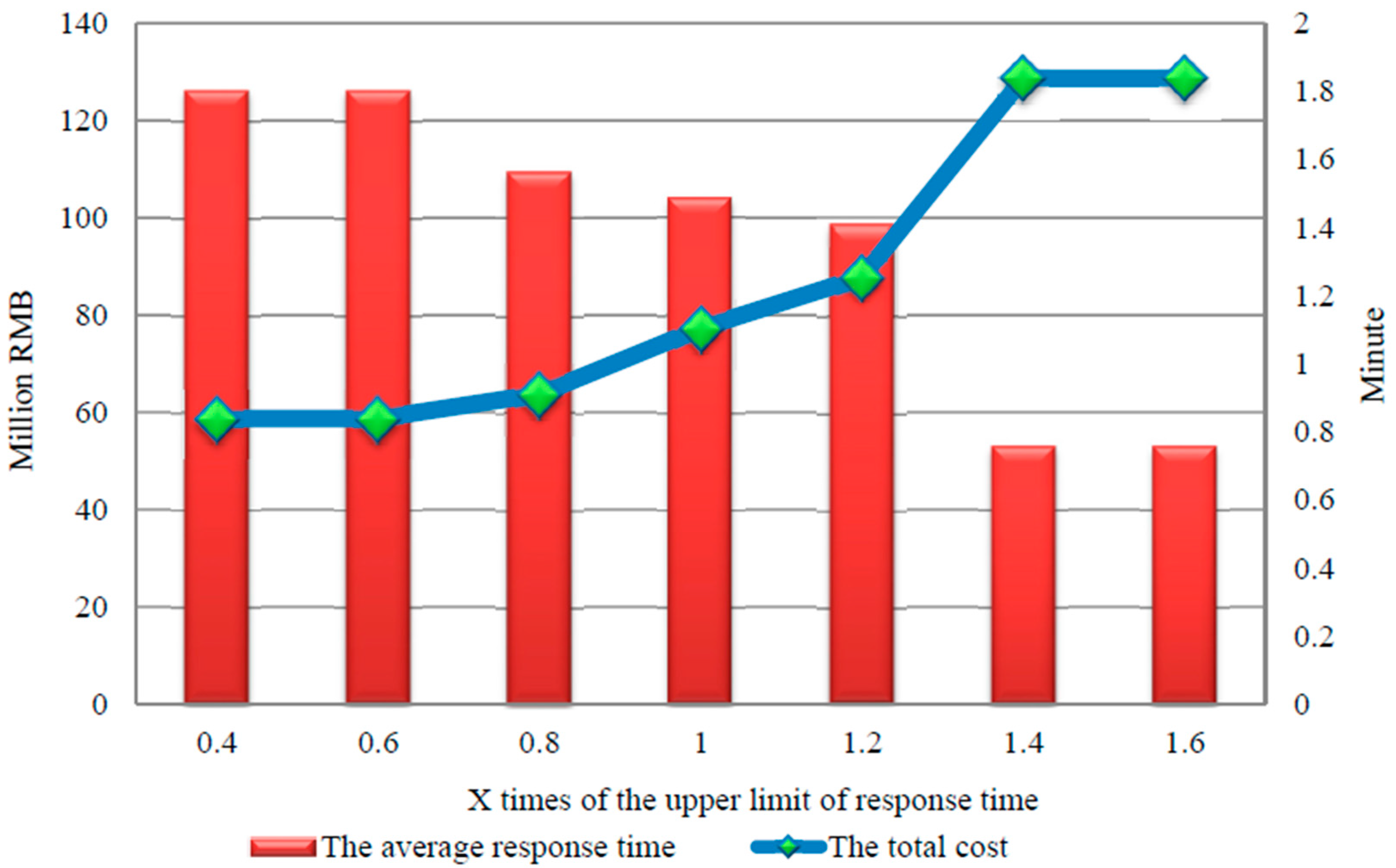
The sensitivity analysis evaluates the impacts of the change in the upper limit of response time (U
k) on the average response time and the total cost. In this paper, we consider the upper bounds of different response times: the minimum U
k is set as 0.4-times the original value of U
k, and the maximum U
k is set as 1.6-times the original value of U
k. In the numerical experiment, the interval of times of U
k is set as 0.2. With the change of U
k, we could obtain its impact on the average response time and the total cost (see
Figure 10).
Figure 10.
The impact of changes in the upper limit of response time on the total cost and the average response time.
Figure 10.
The impact of changes in the upper limit of response time on the total cost and the average response time.
As shown in
Figure 10, the total cost of home health centers demonstrates a decreasing trend with the increase of the upper limit of response time (U
k). This indicates that when patients do not require being served within a short time, the constraint of response time could be relaxed. Accordingly, the number of healthcare centers could be reduced during the location planning process, and the total cost of healthcare centers could also be reduced. In summary, with the increase of the upper limit of response time (U
k), the average response time could be increased, the number of service points could be decreased and the total cost of health service centers could be reduced accordingly.
When the upper limit of response time is increased large enough, the corresponding constraint would no longer have any effects. In other words, the increase of Uk would not affect any decisions in location planning. When the Uk is increased by 1.4 times, the total cost, as well as the average response time would not change any more. When the Uk is increased by less than 0.6 times, the system would achieve the fastest response speed.
Figure 10 shows that there exists an inverse relationship between the total cost and the average response time. Therefore, the decision makers in the home healthcare industry are recommended to comprehensively consider the investment cost and patient satisfaction and to set a reasonable upper limit of response time to achieve the long-term benefit based on their strategic positioning.
Our particular investigation extends the field’s body of knowledge in the following aspects:
- (1)
The proposed model in this paper verifies whether the location of current home health centers is reasonable. There are four evaluation indexes: the minimum total cost for building health centers, the minimum investment cost for starting the business, the minimum labor cost and the minimum transportation cost. This paper investigates the following important issues: where to locate service centers for home healthcare, how to arrange the route to minimize the total cost and how to achieve the highest degree of fulfillment for demand with the fastest response time.
- (2)
Based on the on-site survey, we find that location planning has an important impact on patient satisfaction. The problem identified by the face-to-face survey provides a realistic basis for the research on location planning, and therefore, the results in this paper have higher reference values for policy makers.
- (3)
The model used in this paper considers more realistic constraints, such as the classification of medical staff, multiple types of services provided by health centers and the time window during the service delivery process (or the response time of demand) in the model. The above factors have not been comprehensively considered in the previous studies. Therefore, the results in this paper are more reliable and useful.
- (4)
Results in this paper are based on the two-stage continuous optimization. In the first stage, based on the on-site survey and the verification of the model, we find that the existing ten service centers for home healthcare cannot fully meet the demand. In the second stage, we first set the corresponding candidates for the location planning of service centers based on the on-site survey and then identify the suitable three candidates that have the minimum cost, and the fastest response time should be opened. Meanwhile, two of the existing service centers should be closed.
The theoretical contributions of this paper lie in two aspects. First, from the perspective of the generalization of the model, the model used in this paper can be extended and applied to solve the location planning problems of other industries (e.g., the location planning of Shanghai Disneyland Park, the location planning of distribution centers of logistics systems, etc.). However, we should note that the objective function and constraints need to be revised according to the different characteristics of industries. In summary, the research ideas and the framework construction of the model can provide a reference for the location planning problems of other industries. Second, this paper constructed a mathematical model to solve the location problem of health service centers and obtained the optimal solutions to site selection by computer programming. In other words, different from the traditional qualitative analysis of the location planning problem, this paper provides a theoretical reference for the quantitative analysis of location planning. Based on the mathematical modelling, the estimated results are more scientific and, thus, have higher reference values.
6. Conclusions and Implications
Population ageing is increasingly becoming an issue of concern throughout China. Currently, China’s public healthcare system, as well as pension system are fiscally unsustainable. As a new mode of service, home healthcare service, which contributes to health promotion and disease prevention by establishing a personal health record (PHR) system, providing health information, promoting healthier lifestyles, etc., is crucial for sustainable development in public health. In addition, home healthcare services can effectively alleviate the problem of medical resource shortages especially in large cities in China with a critical shortage of medical resources. In particular, home healthcare services can provide convenient healthcare services to the elderly and other special populations with lower investment cost. Therefore, investigating the systemic challenges of home healthcare, challenges related to the institutional and professional competencies of home healthcare centers, the demands, expectations and degrees of patient satisfaction are of great significance. According to the analysis of survey data, location planning is the key element for reducing the investment cost, as well as avoiding the unnecessary construction of service centers for home healthcare. Therefore, the empirical study of this paper can contribute to the literature in terms of promoting sustainable healthcare in China.
The proper layout of the service centers for home healthcare not only can decrease the investment cost and avoid redundant construction, but also can improve the degree of patient satisfaction, so as to realize sustainable development of home healthcare. The face-to-face survey data show that the location planning is highly important for optimizing the distribution of medical resources, which is therefore conducive for improving the utilization of resources and enhancing the patient satisfaction. To validate the proposed methodology, a location planning model is built and the sensitivity analysis is conducted in this paper, which can optimize the current layout of the home healthcare centers to a certain extent.
Although the proposed optimization model is a common method for the location planning problem, it has distinguished advantages in obtaining reasonable results by considering various actual constraints with limited time. It can be used to solve most of the location planning problems. At present, the Chinese government promotes establishing the home healthcare system, while reasonable location methods, as well as empirical studies based on face-to-face surveys on home healthcare are still scarce. Although only a case study of Shanghai is conducted based on this model, the method can be extended to other regions and, thus, can be a reference for promoting the sustainable development of home healthcare in China.
Considering that medical demands are uncertain, how to establish a stochastic programming model that takes actual constraints into account for a solution will be an important topic for future research. Especially, the integration of the location planning and the personal scheduling is also an interesting research topic.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



