
Community Gardens as Health Promoters: Effects on Mental and Physical Stress Levels in Adults with and without Mental Disabilities

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
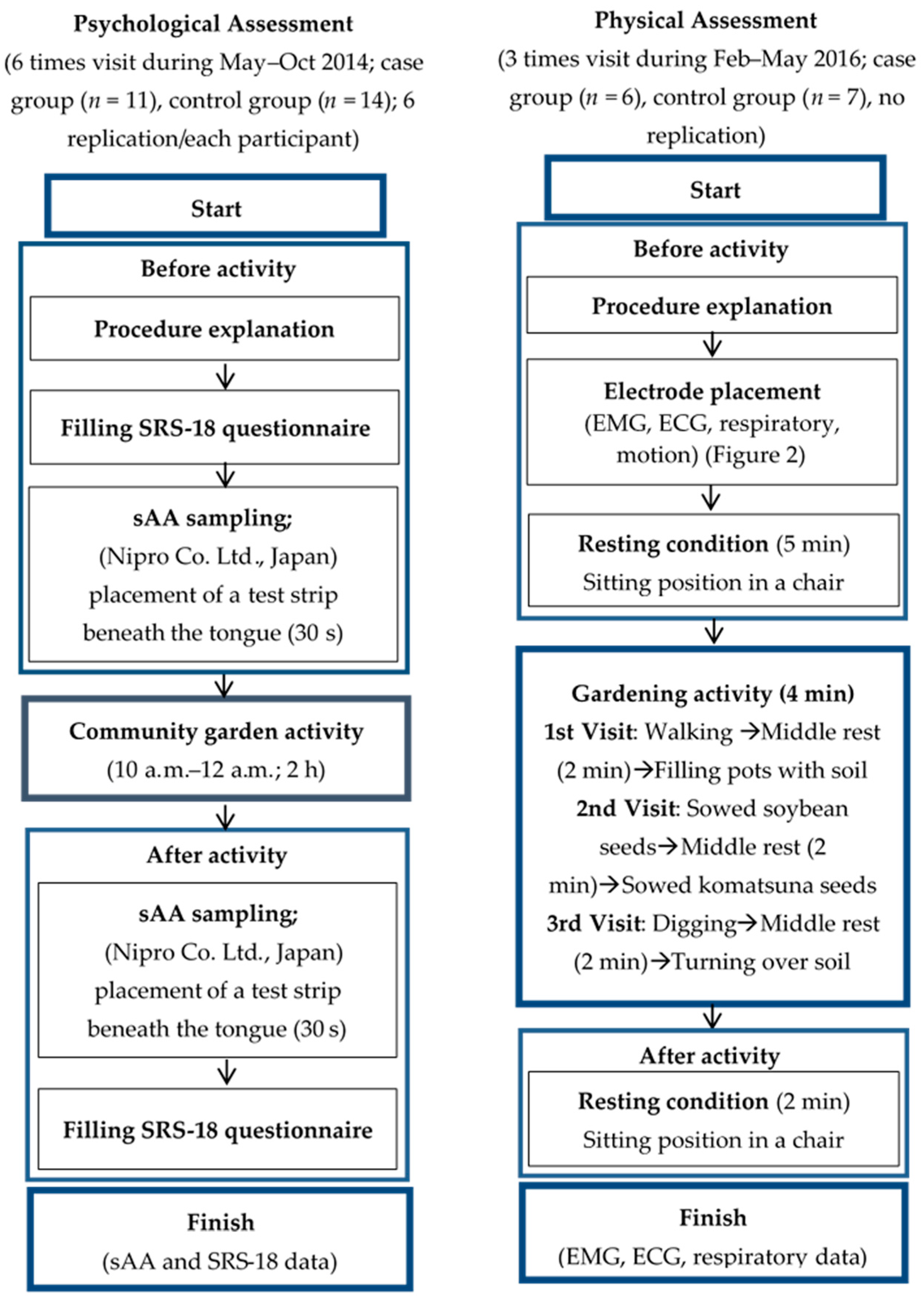
2.1. Research Design
2.2. Participants
2.3. Psychological Assessment
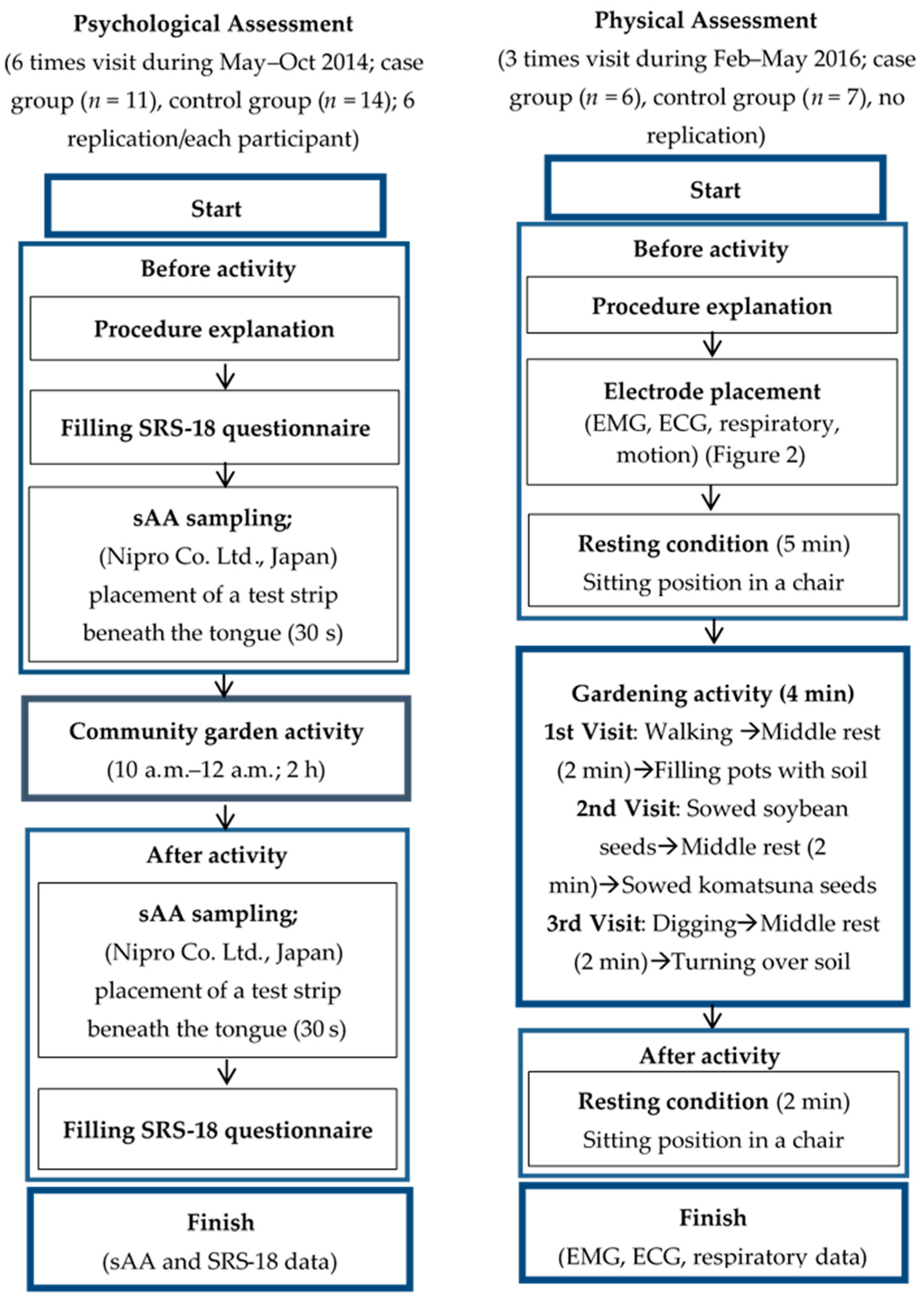
2.3.1. Procedure
2.3.2. Constructs and Measures
2.3.3. Data Analysis
2.4. Physical Assessment
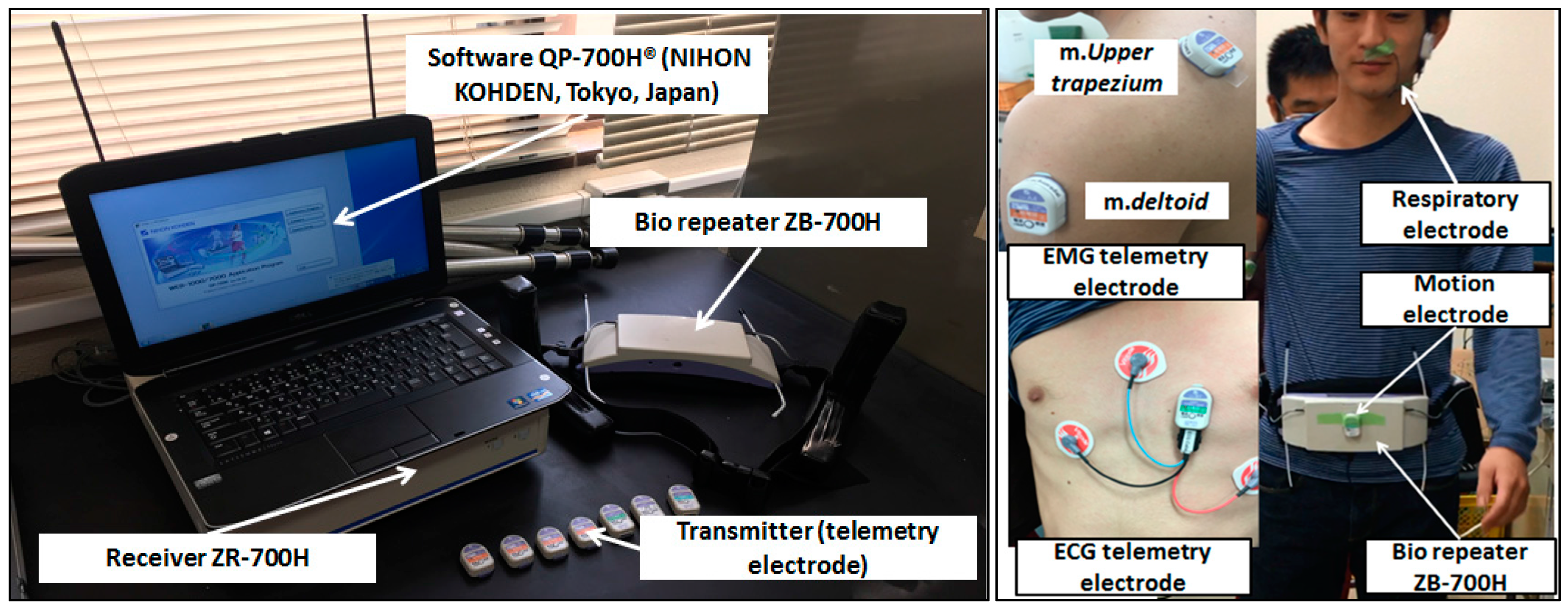
2.4.1. Procedure
2.4.2. Data Analysis
3. Results
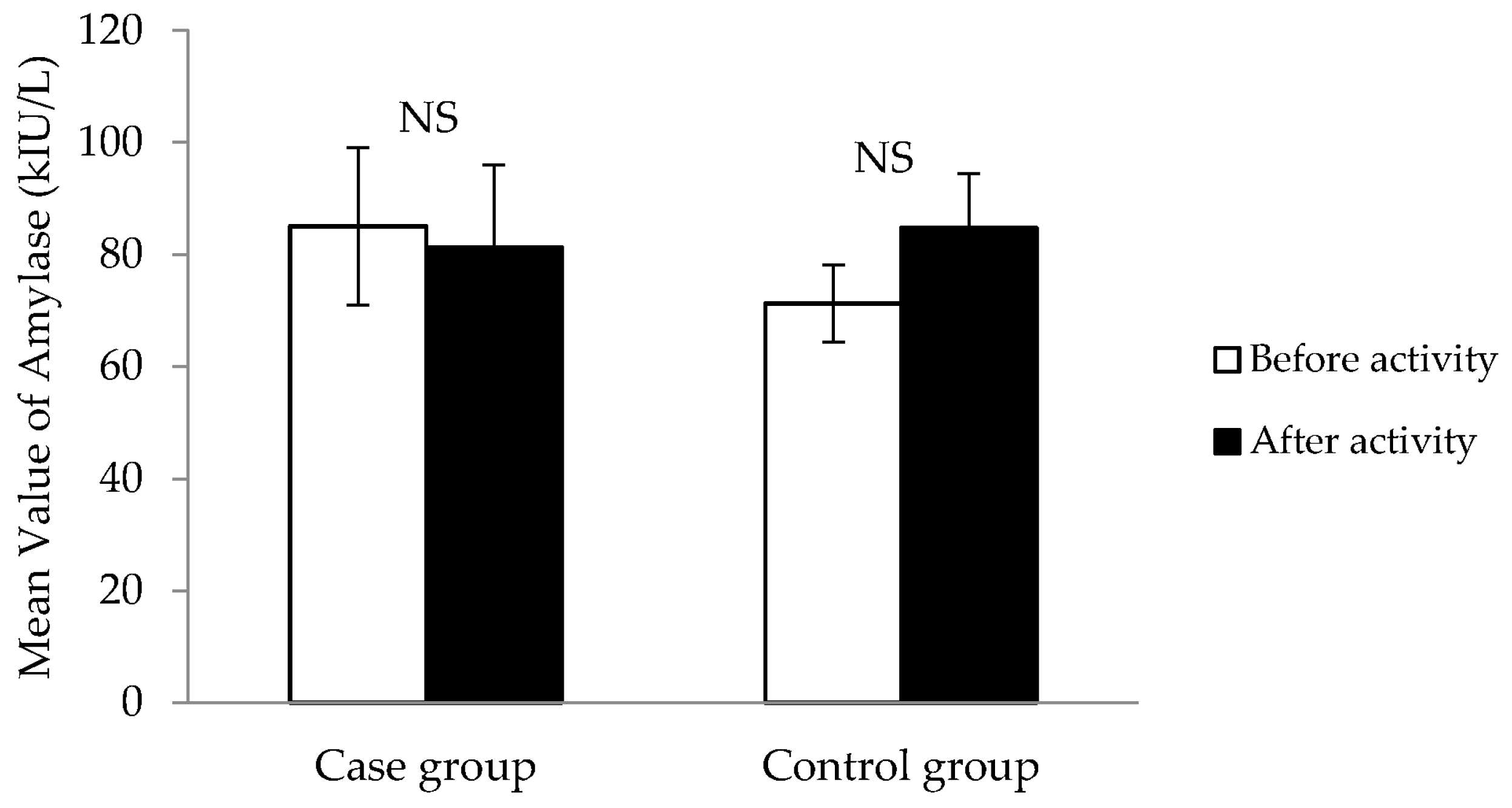
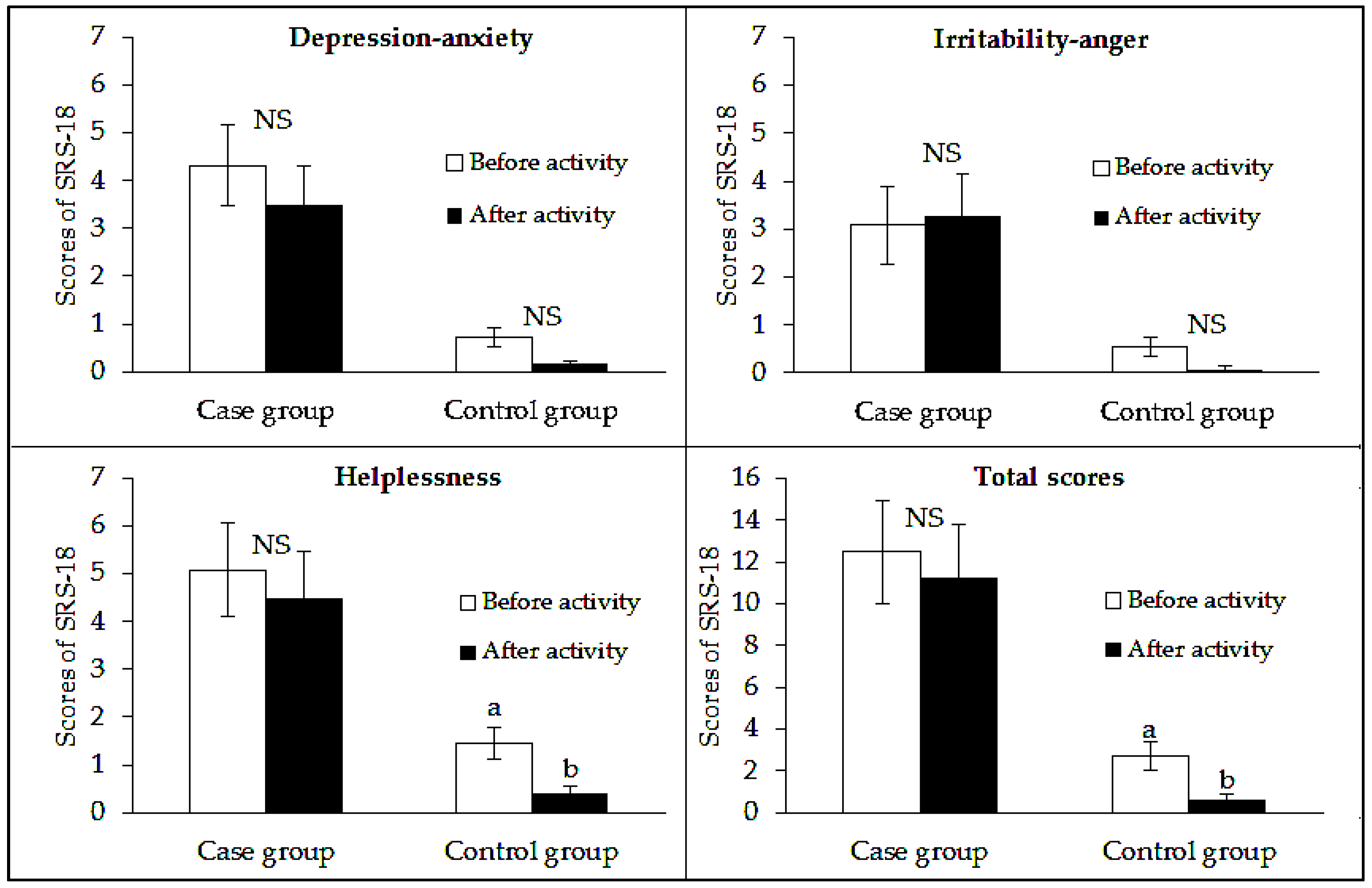
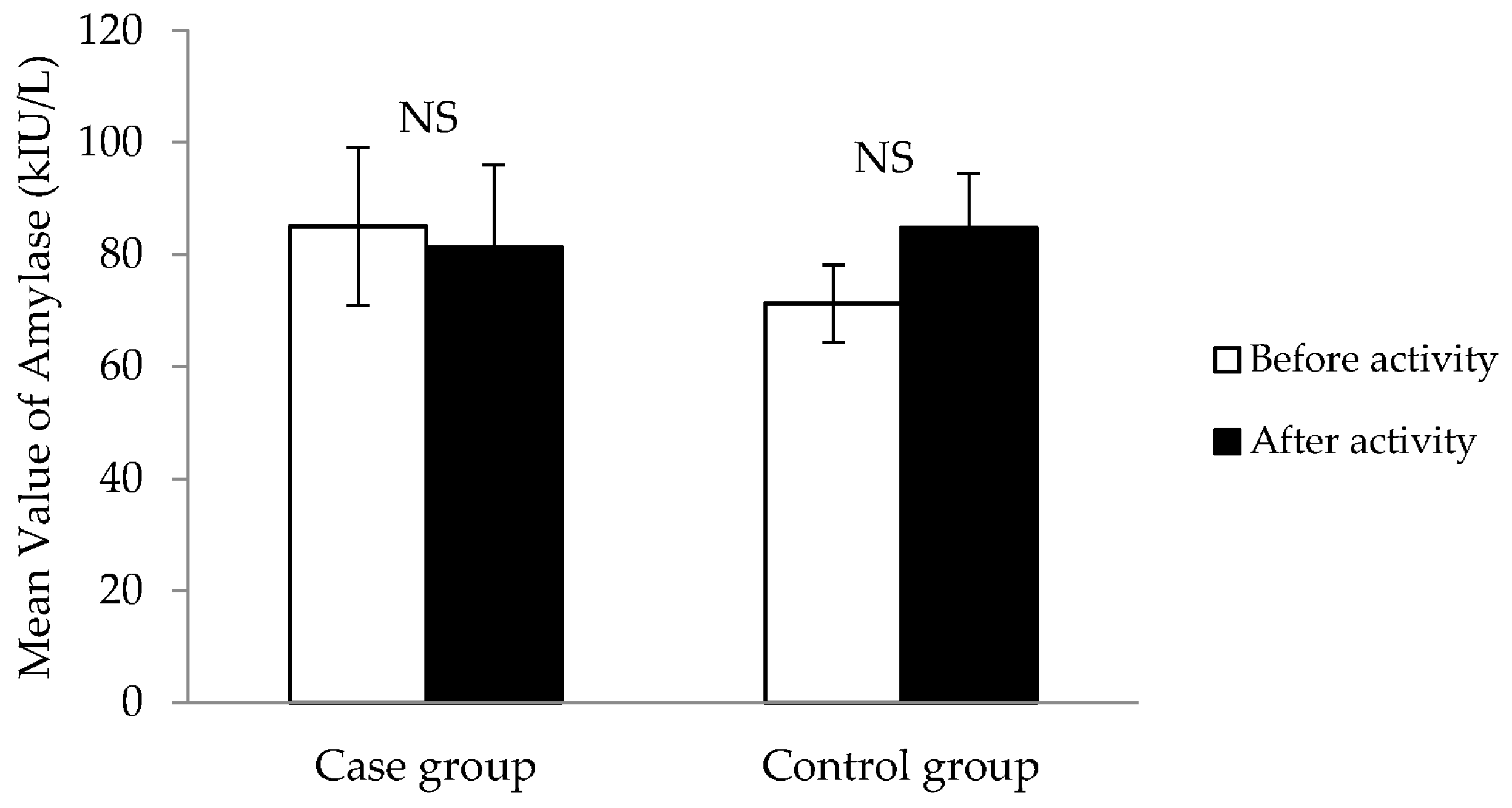
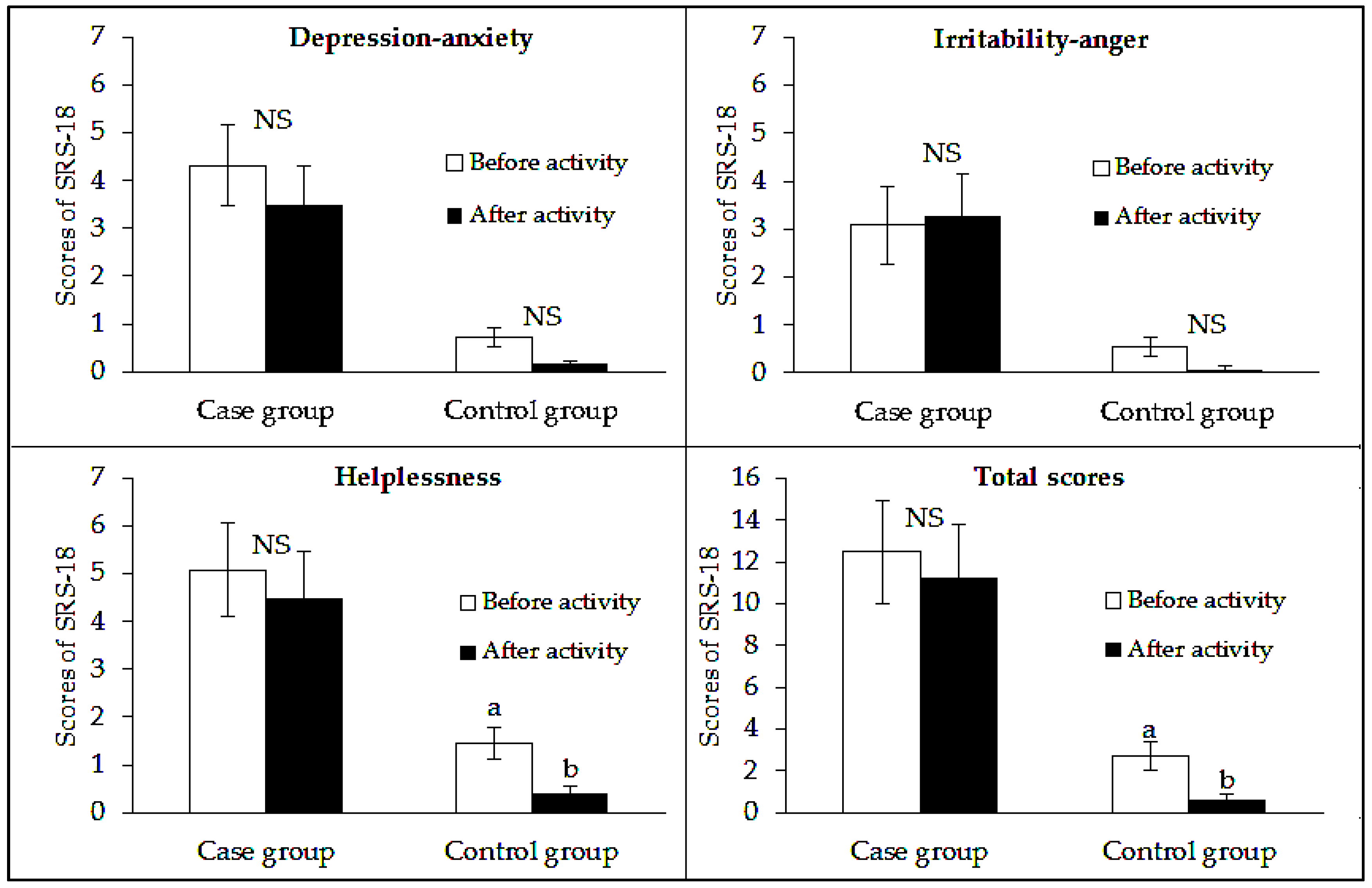
3.1. Psychological Assessment
3.2. Physical Assessment
3.2.1. Increase in the Ratio of the Heart Rate (IRHR)
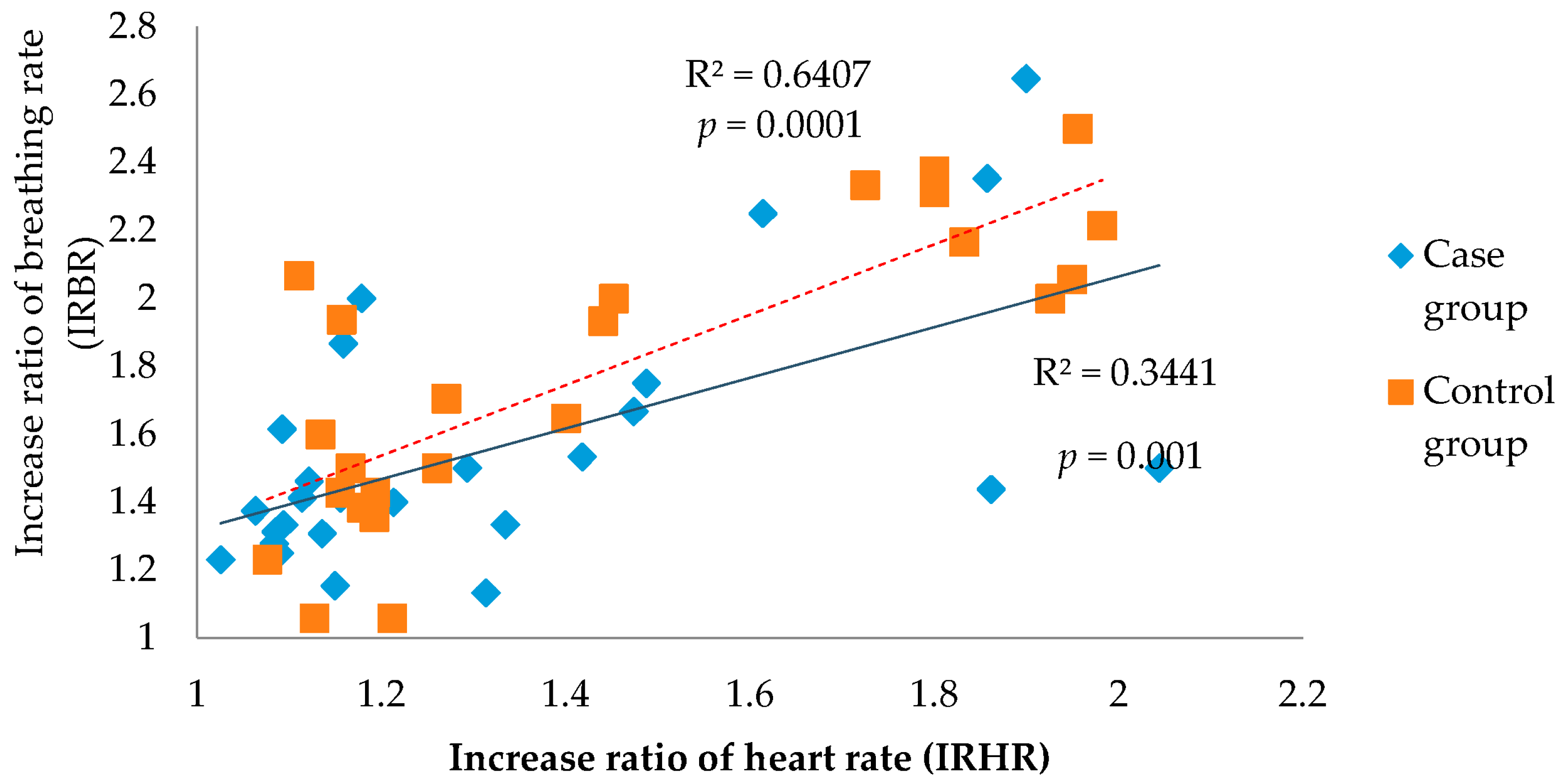
3.2.2. Correlation between the Increase in the Ratio of the Heart Rate (IRHR) and the Increase in the Ratio of the Breathing Rate (IRBR)
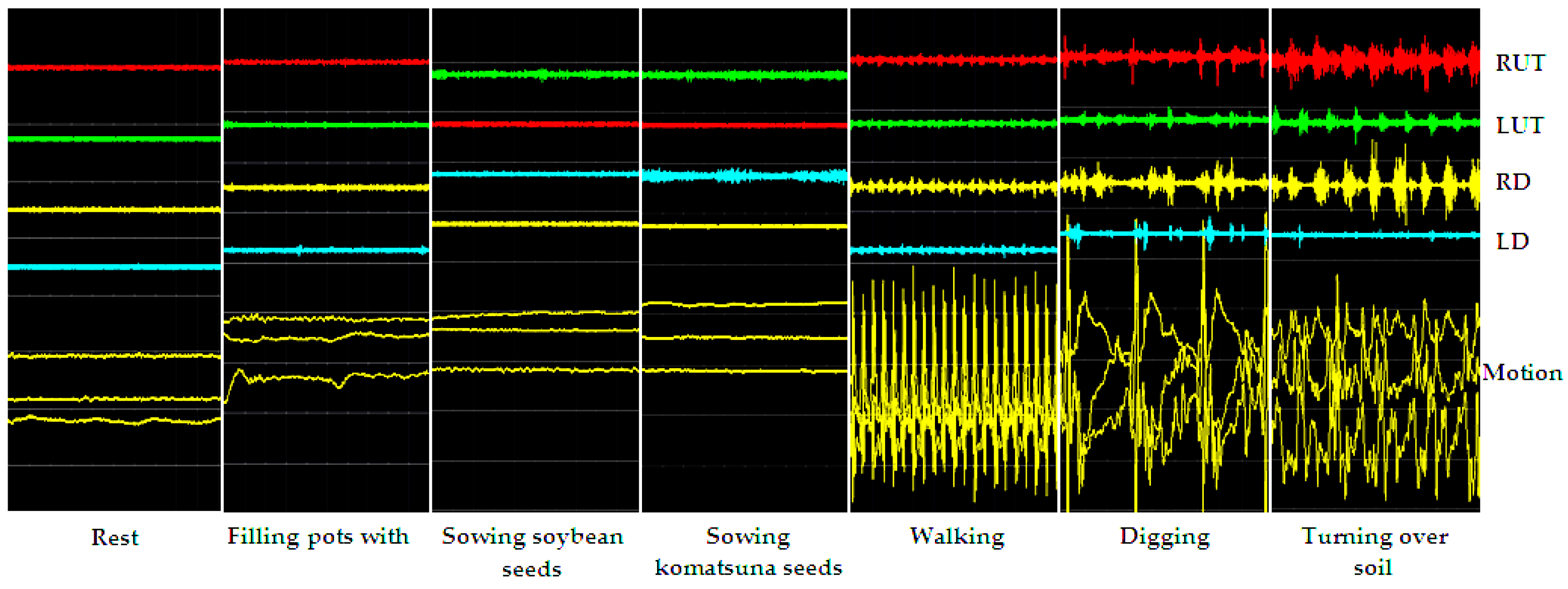
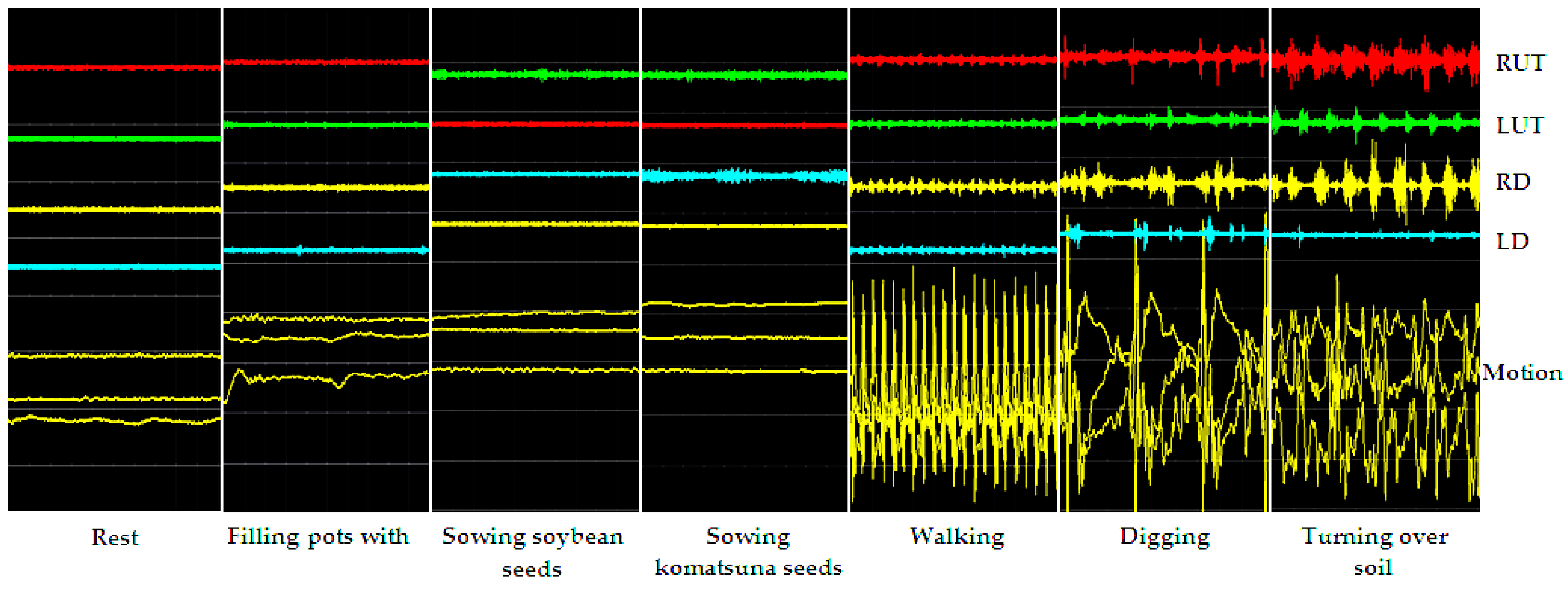
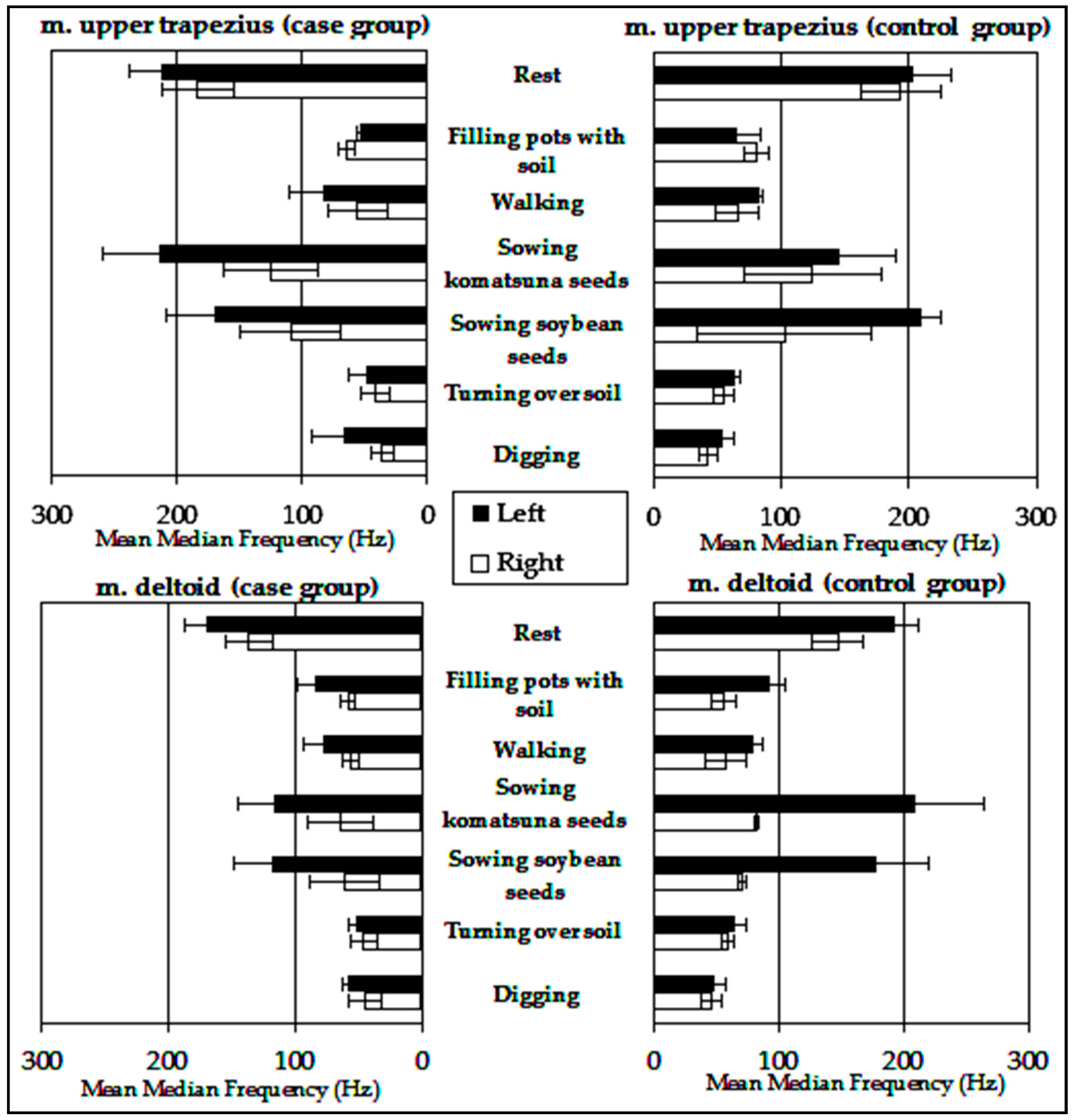
3.2.3. Muscle Activity
4. Discussion
4.1. Psychological Assessment
4.2. Physical Assessment
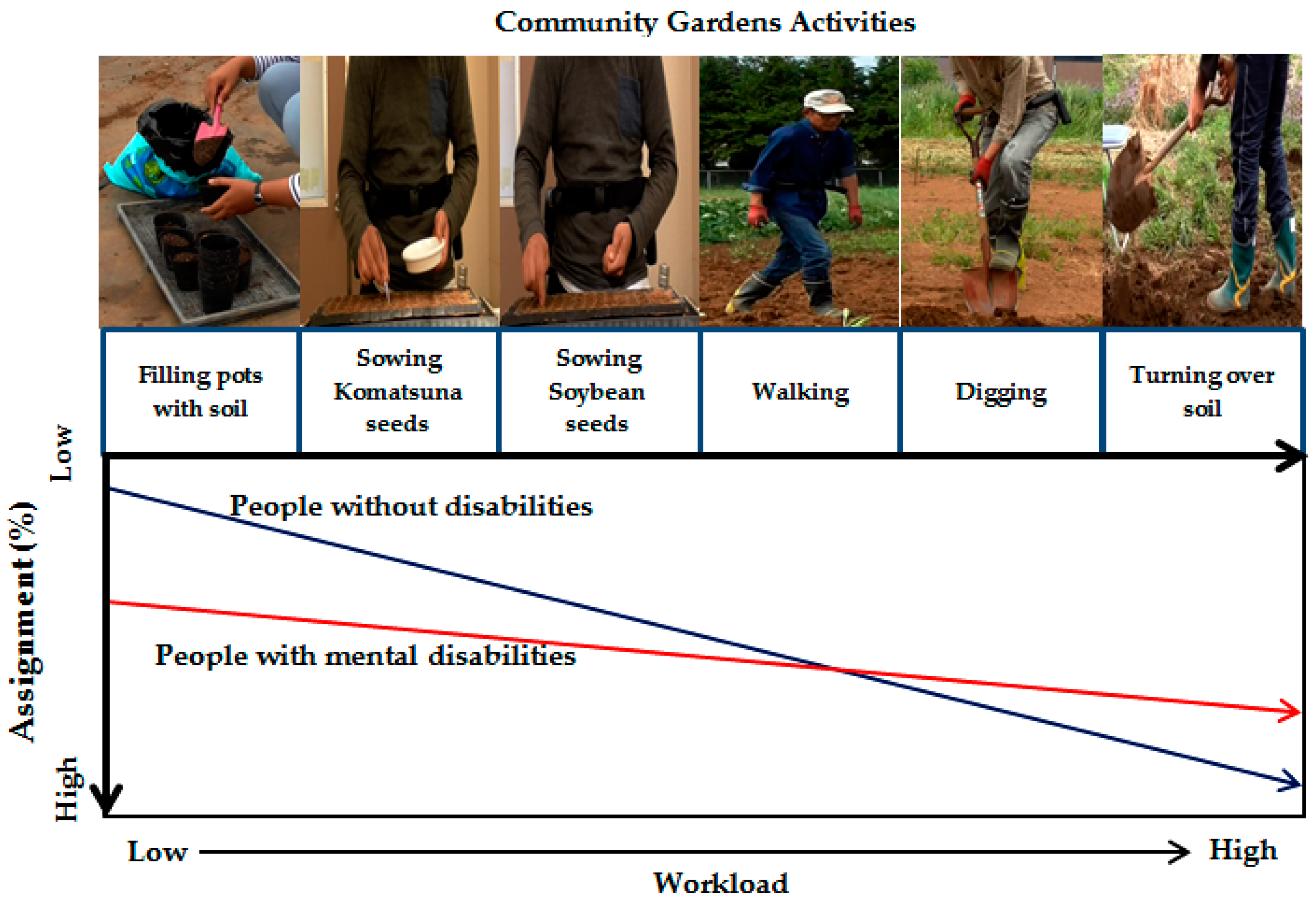
4.3. Comparison among Case and Control Groups through Community Garden Activities
4.4. Implications for Task Allocation in Community Gardens
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- James, P. Urban Sustainability in Theory and Practice. Circles of Sustainability, 2015. Available online: http://www.circlesofsustainability.org/wp-content/uploads/2014/10/Ch-08-Circles-Questionnaire-2015.pdp (accessed on 18 September 2016).
- El Din, H.S.; Shalaby, A.; Farouh, H.E.; Elariane, S.A. Principles of urban quality of life for a neighborhood. HBRC J. 2013, 9, 86–92. [Google Scholar] [CrossRef]
- Chen, D.; Jaenicke, E.C.; Volpe, R.J. Food environments and obesity: Household diet expenditure versus food deserts. Am. J. Public Health 2016, 106, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Amstrong, D. A survey of community gardens in upstate New York: Implications for health promotion and community development. Health Place 2000, 6, 319–327. [Google Scholar] [CrossRef]
- Blair, D.; Giesecke, C.; Sherman, S. A dietary, social and economic evaluation of the Philadelphia Urban Gardening Project. J. Nutr. Educ. 1991, 23, 161–167. [Google Scholar] [CrossRef]
- Pitt, H. Therapeutic experience of community gardens: Putting flow in its place. Health Place 2014, 27, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Twiss, J.; Dickinson, J.; Duma, S.; Kleinman, T.; Paulsen, H.; Rilveria, L. Community gardens: Lessons learned from California Healthy Cities and Communities. Am. J. Public Health 2003, 93, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.C.; Samuels, M.; Harman, A.E. Growing healthy kids: A community garden-based obesity prevention program. Am. J. Prev. Med. 2013, 44, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Qiu, F.; Swallow, B. Can community gardens and farmers’ markets relieve food dessert problems? A study of Edmonton, Canada. Appl. Geogr. 2014, 55, 127–137. [Google Scholar]
- Agustina, I.; Beilin, R. Community gardens: Space for interactions and adaptations. Procedia Soc. Behav. Sci. 2012, 36, 439–448. [Google Scholar] [CrossRef]
- Teig, E.; Amulya, J.; Bardwell, L.; Buchenau, M.; Marshall, J.A.; Litt, J.S. Collective efficacy in Denver, Colorado: Strengthening neighborhoods and health through community gardens. Health. Plc. 2009, 15, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Hale, J.; Knapp, C.; Bardwell, L.; Buchenau, M.; Marshall, J.; Sancar, F.; Litt, J.S. Connecting food environments and health through the relational nature of aesthetics: Gaining insight through the community gardening experience. J. Soc. Sci. Med. 2011, 72, 1853–1863. [Google Scholar] [CrossRef] [PubMed]
- Rodiek, S. Influence of an outdoor garden on mood and stress in older adults. J. Ther. Hortic. 2002, 18, 13–21. [Google Scholar]
- Igarashi, M.; Miwa, M.; Ikei, H.; Song, C.; Takagaki, M.; Miyazaki, Y. Physiological and Psychological Effects of Viewing a Kiwifruit (Actinidia deliciosa ‘Hayward’) Orchard Landscape in Summer in Japan. Int. J. Environ. Res. Public Health 2015, 12, 6657–6668. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare of Japan. Exercise and Physical Activity Guide for Health Promotion. 2006. Available online: http://www0.nih.go.jp/eiken/programs/pdf/exercise_guide.pdf (accessed on 3 June 2016). [Google Scholar]
- Park, S.A.; Lee, K.S.; Son, K.C. Determining Exercise intensities of gardening task as a physical activity using metabolic equivalents in older adults. HortScience 2011, 46, 1706–1710. [Google Scholar]
- Park, S.A.; Shoemaker, C.; Haub, M. Can older gardeners meet the physical activity recommendation through gardening? HortTechnology 2008, 18, 639–643. [Google Scholar]
- Park, S.A.; Shoemaker, C.; Haub, M. Physical and psychological health conditions of older adults classified as gardeners or nongardeners. HortScience 2009, 44, 206–210. [Google Scholar]
- Ministry of Health, Labor and Welfare of Japan. Handbook of Health and Welfare Statistic 2015: Total Number of Patients by Sex and Classification of Diseases. 2015. Available online: http://www.mhlw.go.jp/english/database/db-hh/xls/2-66.xls (accessed on 1 October 2016). [Google Scholar]
- McGrath, J.; Saha, S.; Welham, J.; El Saadi, O.; MacCauley, C.; Chant, D. A systematic review of the incidence of schizophrenia. BMC Med. 2004, 2, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, W.T.; Leung, S.F.; Yeung, F.K.K.; Wong, W.K. Current approaches to treatments for schizophrenia spectrum disorders, part II: Psychosocial interventions and patient-focused perspectives in psychiatric care. Neuropsychiatr. Dis. Treat. 2013, 9, 1463–1481. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bo, L.; Sampson, S.; Roberts, S.; Zhang, G.; Wu, W. Horticultural therapy for schizophrenia (review). Cochrane Database Syst. Rev. 2014, 5, 1–31. [Google Scholar]
- Kam, M.C.Y.; Siu, A.M.H. Evaluation of a horticultural activity program for persons with psychiatric illness. J. Occup. Ther. 2010, 20, 80–86. [Google Scholar]
- Ando, S.; Yamaguchi, S.; Aoki, Y.; Thornicroft, G. Review of mental-health-related stigma in Japan. Psychiatry Clin. Neurosci. 2013, 67, 471–482. [Google Scholar] [CrossRef] [PubMed]
- McNamee, L.; mead, G.; MacGilivray, S.; lawrie, S.M. Schizoprenia, poor physical health and physical activity: Evidence-based interventions are required to reduce major health inequalities. Br. J. Psychiatry 2013, 203, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.R.; Faulkner, G.; McDevitt, J.; Skrinar, G.S.; Hutchinson, D.S.; Piette, J.D. Integrating physical activity into mental health services for persons with serious mental illness. Psychiatr. Serv. 2005, 56, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Janney, C.A.; Ganguli, R.; Tang, G.; Cauley, J.A.; Holleman, R.G.; Richardson, C.R.; Kriska, A.M. Physical activity and sedentary behavior measured objectively and subjectively in overweight and obese adults with schizophrenia or schizoaffective disorders. J. Clin. Psychiatry 2015, 76, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.D.; McGregor, J.C.; Perencevich, E.N.; Furuno, J.P.; Zhu, J.; Peterson, D.E.; Finkelstein, J. The use and interpretation of quasi experimental studies in medical informatics. J. Am. Med. Inform. Assoc. 2006, 13, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Szeto, G.P.Y.; Straker, L.M.; O’Sullivan, P.B. EMG median frequency changes in the neck-shoulder stabilizers of symptomatic office workers when challenged by different physical stressors. J. Electromyogr. Kinesiol. 2005, 15, 544–555. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.B.; Park, J.K.; Cho, S. Development of the somatic stress response scale and its application in clinical practice. Yonsei Med. J. 2005, 46, 614–624. [Google Scholar] [CrossRef] [PubMed]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral and biological determinats. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organ: Genewa, Switzerland, 1992; Available online: http://apps.who.int/iris/bitstream/10665/37958/8/9241544228_eng.pdf (accessed on 1 October 2016).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publish: Arlington, VA, USA, 2013. [Google Scholar]
- Yamaguchi, M. Salivary sensors in point-of-care testing. J. Sens. Mater. 2010, 22, 143–153. [Google Scholar]
- Minowa, C.; Koitabashi, K. Salivary alpha-amylase activity—An indicator of relaxation response in perioperative patients. J. Nurs. 2012, 2, 208–214. [Google Scholar] [CrossRef]
- Fukusaki, M.; Miura, K.; Okada, M.; Araki, H.; Terao, Y.; Sumikawa, K. Objective assessment with salivary α-amylase activity of the effect of stellate ganglion block in the patients with cervical radiculopathy: 14AP7-1. Eur. J. Anaesthesiol. 2012, 29, 207–208. [Google Scholar] [CrossRef]
- Suzuki, S.; Shimada, H.; Miura, M.; Katayanagi, K.; Umamo, R.; Sakano, Y. Development of a new psychological stress response scale (SRS-18) and investigation of the reliability and validity. Jpn. J. Behav. Med. 1997, 4, 22–29. [Google Scholar]
- Nakamura, N. The relationships among stages of change for stress management, stress responses, self-efficacy, and frequency of stress-management behavior in Japanese university student. J. Sch. Health 2009, 5, 24–30. [Google Scholar]
- Hashimoto, T.; Mojaverian, T.; Kim, H.S. Culture, interpersonal stress and psychological distress. J. Cross-Cult. Psychol. 2012, 43, 527–532. [Google Scholar] [CrossRef]
- Soderberg, G.L.; Knutson, L.M. A guide for use and interpretation of kinesiologic electromyographic data. J. Am. Phys. Ther. Assoc. 2000, 80, 485–498. [Google Scholar]
- Park, S.A.; Oh, S.R.; Lee, K.S.; Son, K.C. Electromyographic analysis of upper limb and hand muscles during horticultural activity motions. HortTechnology 2013, 23, 51–56. [Google Scholar]
- Balasubramanian, V.; Adalarasu, K. EMG-based analysis of change in muscle activity during simulated driving. J. Bodyw. Mov. Ther. 2007, 11, 151–158. [Google Scholar] [CrossRef]
- Syuaib, M.F.; Moriizumi, S.; Shimizu, H. Ergonomic study on the process of mastering reversible plow operation using ride-on tractor. Jpn. J. Farm Work Res. 2007, 42, 91–103. [Google Scholar] [CrossRef]
- Syuaib, M.F.; Moriizumi, S.; Shimizu, H. Ergonomic study on the process of mastering tractor operation-rotary tillage operation using walking type tractor. Jpn. J. Farm Work Res. 2002, 64, 61–67. [Google Scholar]
- Hermens, H.J.; Bruggen, T.A.M.V.; Baten, C.T.M.; Rutten, W.I.C.; Boom, H.B.K. The median frequency of the surface EMG power spectrum in relation to motor unit firing and action potential properties. J. Electromyogr. Kinesiol. 1992, 2, 15–25. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. 2016. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 27 November 2016).
- Rowe, D.A.; Welk, G.J.; Heil, D.P.; Mahar, M.T.; Kemble, C.D.; Calabro, M.A. Stride rate recommendations for moderate intensity walking. Med. Sci. Sports Exerc. 2011, 43, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Nater, U.M.; Rohleder, N. Salivary alpha-amylase as a non-invasive biomarker for the sympathetic nervous system: Current state of research. Psychoneuroendocrinology 2009, 34, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Pruessner, J.C. The salivary alpha amylase over cortisol ratio as a marker to assess dysregulations of the stress systems. Physiol. Behav. 2012, 106, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Chrousos, G.P. Stress and disorders of the stress system. Nat. Rev. Endocrinol. 2009, 5, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Skoluda, N.; Strahler, J.; Schlotz, W.; Niederberger, L.; Marques, S.; Fischer, S.; Thoma, M.V.; Spoerri, C.; Ehlert, U.; Nater, U.M. Intra-individual psychological and physiological responses to acute laboratory stressors of different intensity. Psychoneuroendocrinology 2015, 51, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Deguchi, M.; Wakasugi, J.; Ono, S.; Takai, N.; Higashi, T.; Mizuno, Y. Hand-held monitor of sympathetic nervous system using salivary amylase activity and its validation by driver fatigue assessment. Biosens. Bioelectron. 2006, 21, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.; Koh, D.; Mok, B.Y.Y.; Chia, S.E.; Lim, L.P. Salivary biomarkers associated with academic assessment stress among dental undergraduateds. J. Dent. Educ. 2003, 67, 1091–1094. [Google Scholar] [PubMed]
- Kotozaki, Y.; Takeuchi, H.; Sekiguchi, H.; Araki, T.; Takahashi, K.; Yamamoto, Y.; Nozawa, T.; Taki, Y.; Kawashima, R. Positive effects of the victim by the growing of plants after great east Japan earthquake. Int. J. Recent Sci. Res. 2015, 6, 2850–2858. [Google Scholar]
- Yamaguchi, M.; Kanemori, T.; Kanemaru, M.; Takai, N.; Mizuno, Y.; Yoshida, H. Performance evaluation of salivary amylase activity monitor. Biosens. Bioelectron. 2004, 20, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Tokushige, A. Using salivary amylase to measure stress caused by urinating in diapres. Aino J. 2010, 9, 11–13. [Google Scholar]
- Vineetha, R.; Pai, K.M.; Vengal, M.; Gopalakrishna, K.; Narayanakurup, D. Usefulness of salivary alpha amylase as a biomarker of chronic stress and strees related oral mucosal changes-a pilot study. J. Clin. Exp. Dent. 2014, 6, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Kanemori, T.; Kanemaru, M.; Mizuno, Y.; Yoshida, H. Correlation of stress and salivary amylase activity. J. Med. Electron. Biol. Eng. 2001, 39, 234–239. [Google Scholar]
- Yamaguchi, M.; Kanemaru, M.; Kanemori, T.; Mizuno, Y. Flow-injection-type biosensor system for salivary amylase activity. Biosen. Bioelectron. 2003, 18, 835–840. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Kanemori, T.; Kanemaru, M.; Mizuno, Y.; Takai, N. The Influence of Physical Stress on Amylase Activity in Human Saliva. Life Support 2003, 15, 4–11. [Google Scholar] [CrossRef]
- Koibuchi, E.; Suzuki, Y. Exercise upregulates salivary amylase in humans (Review). Exp. Ther. Med. 2014, 7, 773–777. [Google Scholar] [PubMed]
- Appenzeller, O. The autonomic nervous system and fatigue. Funct. Neurol. 1987, 2, 473–485. [Google Scholar] [PubMed]
- Chrousos, G.P.; Gold, P.W. The concepts of stress and stress system disorders. JAMA 1992, 267, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Elenkov, I.J.; Wilder, R.L.; Chrousos, G.P.; Vizi, E.S. The sympathetic nerve—An integrative interface between two supersystems: The brain and the immune system. Pharmacol. Rev. 2000, 52, 595–638. [Google Scholar] [PubMed]
- Park, S.A.; Lee, H.S.; Lee, K.S.; Son, K.C.; Shoemaker, C.A. The metabolic cost of gardening tasks in children. HortTechnology 2013, 23, 589–594. [Google Scholar]
- Watanabe, N.; Reece, J.; Polus, B.I. Effect of body position on autonomic regulation of cardiovascular function in young, healthy adults. Chiropr. Osteopat. 2007, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.Y.M.; Kam, C.; Lai, K.W.; Lee, H.Y.; Chow, H.T.; Lau, S.F.; Wong, L.M.; He, J. Changes in heart rate and r-wave amplitude with posture. Chin. J. Physiol. 2003, 46, 63–69. [Google Scholar] [PubMed]
- Pitzalis, M.V.; Mastropasqua, F.; Massari, F.; Passantino, A.; Colombo, R.; Mannarini, A.; Forleo, C.; Rizzon, P. Effect of respiratory rate on the relationships between RR interval and systolic blood pressure fluctuations: A frequency-dependent phenomenon. Cardiovasc. Res. 1998, 38, 332–339. [Google Scholar] [CrossRef]
- Jones, D.A. High and low frequency fatigue revisited. Acta Physiol. Scand. 1996, 156, 265–270. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J.; Sabbahi, M.A.; Roy, S.H. Median frequency of the myoelectric signal: Effects of hand dominance. Eur. J. Appl. Physiol. 1986, 55, 457–464. [Google Scholar] [CrossRef]
- Simpson, M.E.; Serdula, M.; Galuska, D.A.; Gillespie, C.; Donehoo, R.; Macera, C.; Mack, K. Walking trends among U.S. adults: The behavioral risk factor surveillance system, 1987–2000. Am. J. Prev. Med. 2003, 25, 95–100. [Google Scholar] [CrossRef]
- Vancampfort, D.; Knapen, J.; Probst, M.; Scheewe, T.; Remans, S.; De Hert, M. A systematic review of correlates of physical activity in patients with schizophrenia. Acta Psychiatr. Scand. 2012, 125, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Zschucke, E.; Gaudlitz, K.; Strohle, A. Exercise and physical activity in mental disorders: Clinical and experimental evidence. J. Prev. Med. Public Health 2013, 46, 12–21. [Google Scholar] [CrossRef] [PubMed]
- U.S. Departement of Health and Human Services. 2008 Physical Activity Guidelines for America. 2008. Available online: www.health.gov/paguidelines (accessed on 1 December 2016). [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Gardening Activity | Description |
|---|---|---|
| 1 | Walking | Walking while carrying a load (1 kg) in the right hand. |
| 2 | Filling pots with soil | Placing soil into pots (upper diameter: 10 cm; bottom diameter: 7 cm; height: 15 cm) using a trowel (squatting position). |
| 3 | Sowing big seed | Sowing soybean (glycine max) seeds in a 128-hole tray (3 cm × 3 cm) filled with soil by hand (standing position). |
| 4 | Sowing small seed | Sowing komatsuna (Brassica rapa var. perviridis) seeds in a 128-hole tray (3 cm × 3 cm) filled with soil by tweezers (standing position). |
| 5 | Digging soil | Digging soil using a shovel with both hands. |
| 6 | Turning over soil | Turning over soil with a shovel after digging with both hands. |
| Variable * | Case Group (n = 6) | Control Group (n = 7) | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age (years) | 37 | 14.2 | 29 | 10.3 |
| Height (cm) | 165.7 | 5.3 | 169.0 | 6.3 |
| Body weight (kg) | 67.3 | 10.2 | 71.3 | 9.9 |
| Body mass index (kg·m−2) | 24.6 | 4.2 | 25.0 | 3.3 |
| Resting heart rate (beats/min) | 75 | 9.7 | 72 | 14.7 |
| Resting breathing rate (breaths/min) | 16 | 1.7 | 16 | 1.6 |
| Age-adjusted HR max (beats/min) | 183 | 14.2 | 190 | 10.3 |
| Activity Achievement | Case Group (n = 6) | Control Group (n = 7) | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Walking (steps/min) | 94 | 16.4 | 122 | 30.4 |
| Filling pots with soil (pots/min) ** | 3 | 0.6 | 5 | 0.5 |
| Sowing soybean seeds (seeds/min) ** | 20 | 2.9 | 29 | 1.2 |
| Sowing komatsuna seeds (seeds/min) | 13 | 2.4 | 16 | 0.6 |
| Shoveling (m/min) * | 3.9 | 1 | 6.1 | 1.2 |
| Turning soil (m/min) * | 2.3 | 0.5 | 3.9 | 1.3 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dewi, N.S.; Komatsuzaki, M.; Yamakawa, Y.; Takahashi, H.; Shibanuma, S.; Yasue, T.; Okayama, T.; Toyoda, A.; Shimonishi, H.; Sasaki, S. Community Gardens as Health Promoters: Effects on Mental and Physical Stress Levels in Adults with and without Mental Disabilities. Sustainability 2017, 9, 63. https://doi.org/10.3390/su9010063
Dewi NS, Komatsuzaki M, Yamakawa Y, Takahashi H, Shibanuma S, Yasue T, Okayama T, Toyoda A, Shimonishi H, Sasaki S. Community Gardens as Health Promoters: Effects on Mental and Physical Stress Levels in Adults with and without Mental Disabilities. Sustainability. 2017; 9(1):63. https://doi.org/10.3390/su9010063
Chicago/Turabian StyleDewi, Nugrahaning Sani, Masakazu Komatsuzaki, Yuriko Yamakawa, Hiromi Takahashi, Saori Shibanuma, Takeshi Yasue, Tsuyoshi Okayama, Atsushi Toyoda, Hikari Shimonishi, and Seiichi Sasaki. 2017. "Community Gardens as Health Promoters: Effects on Mental and Physical Stress Levels in Adults with and without Mental Disabilities" Sustainability 9, no. 1: 63. https://doi.org/10.3390/su9010063