Towards Sustainable Public Health Surveillance in India: Using Routinely Collected Electronic Emergency Medical Service Data for Early Warning of Infectious Diseases


Abstract
:1. Introduction—Infectious Disease Surveillance in India
2. Materials and Methods
3. Results
3.1. Needs Assessment
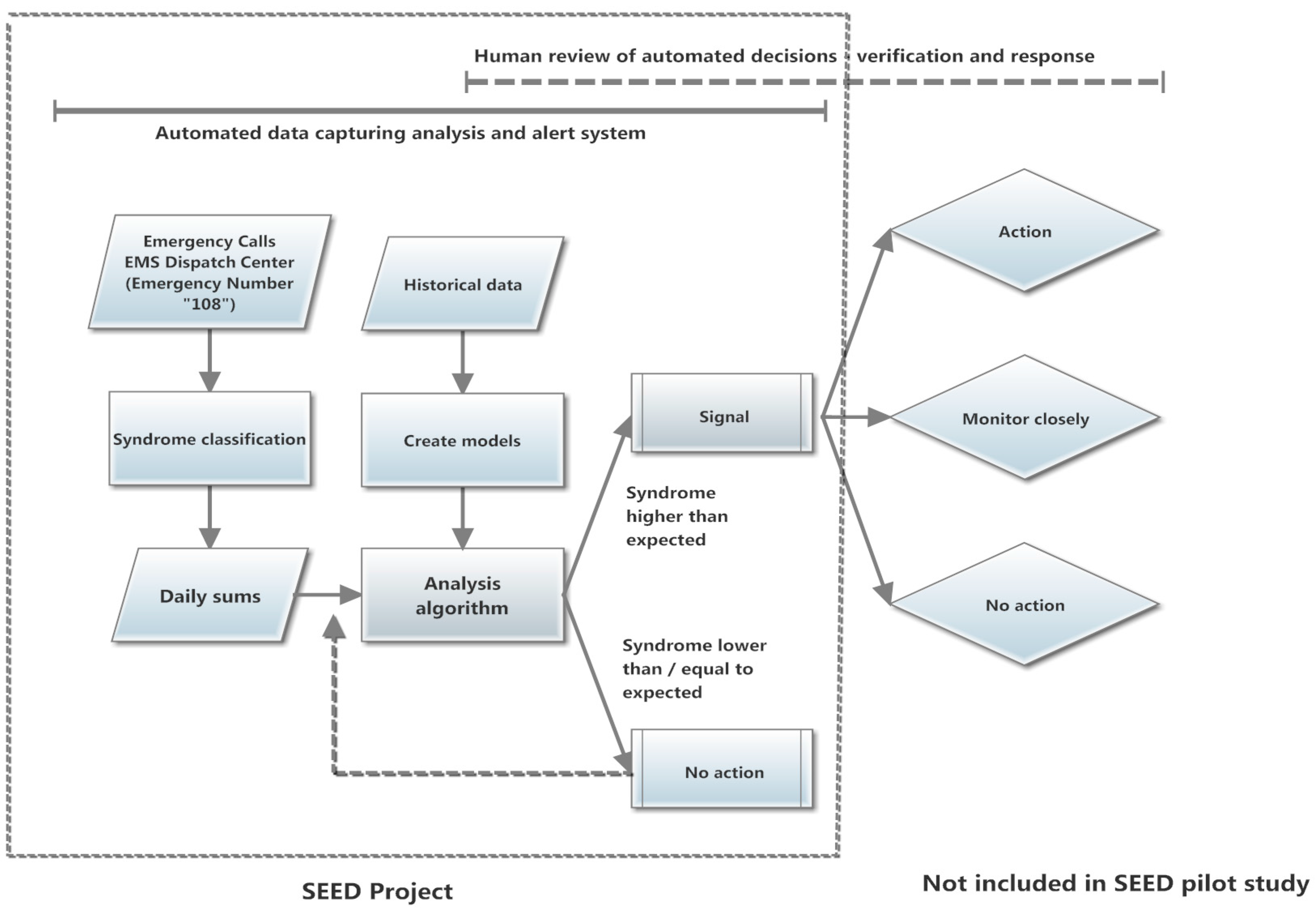
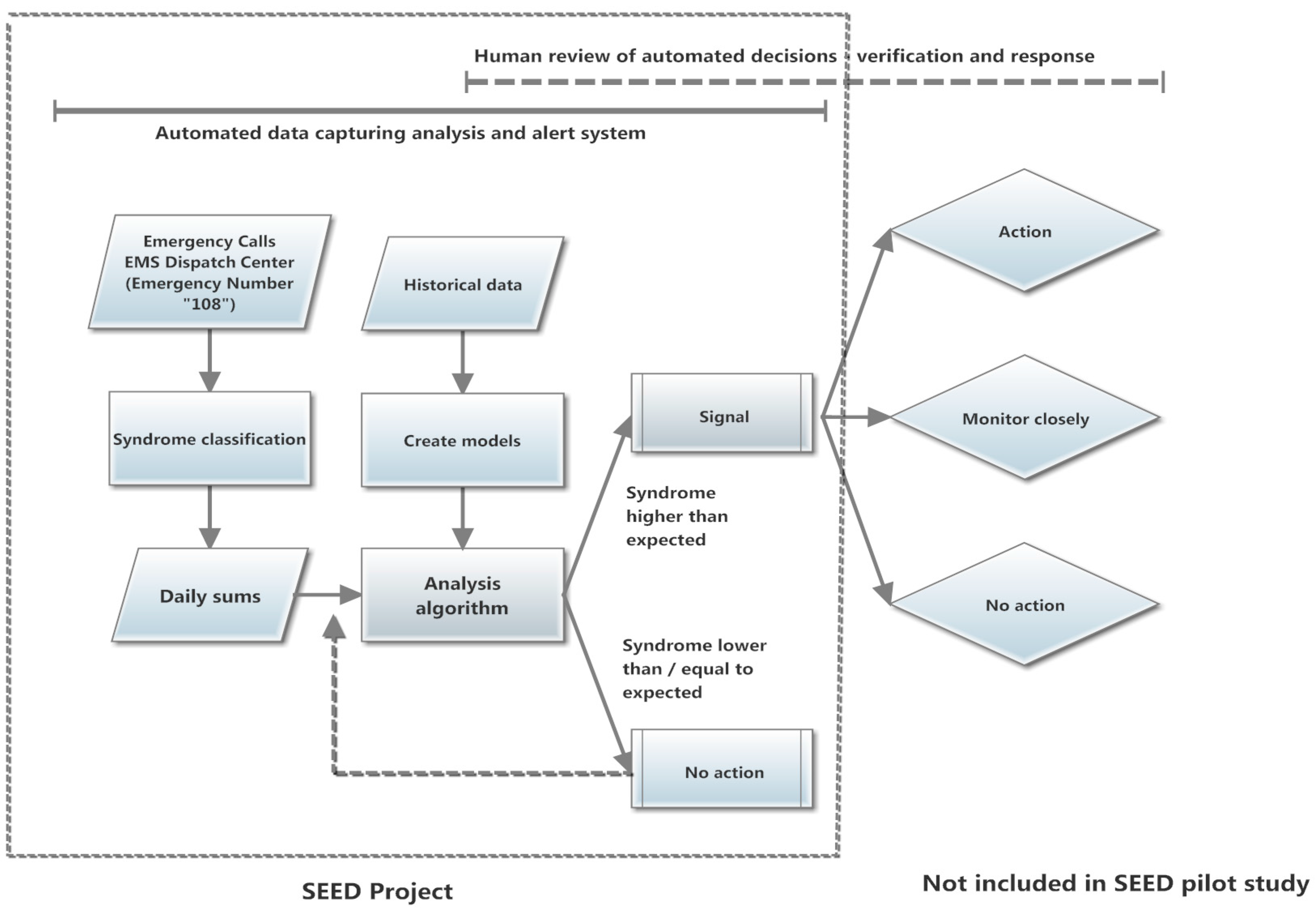
3.2. System for Early Warning Based on Emergency Data (SEED)
3.3. Test Phase of System for Early Warning Using Emergency Data/Case Study for Fever Surveillance in Guntur District, Andhra Pradesh, India
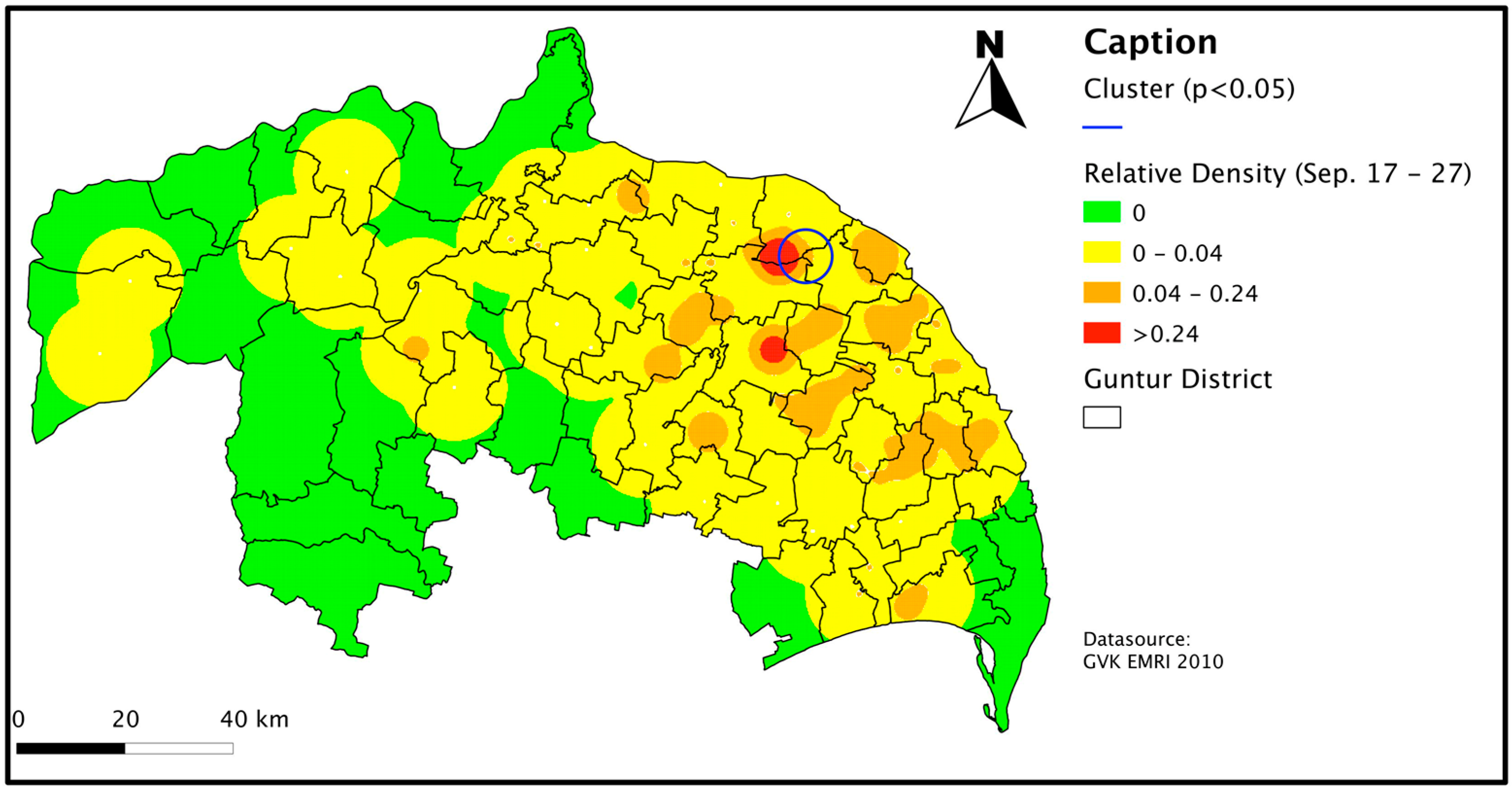
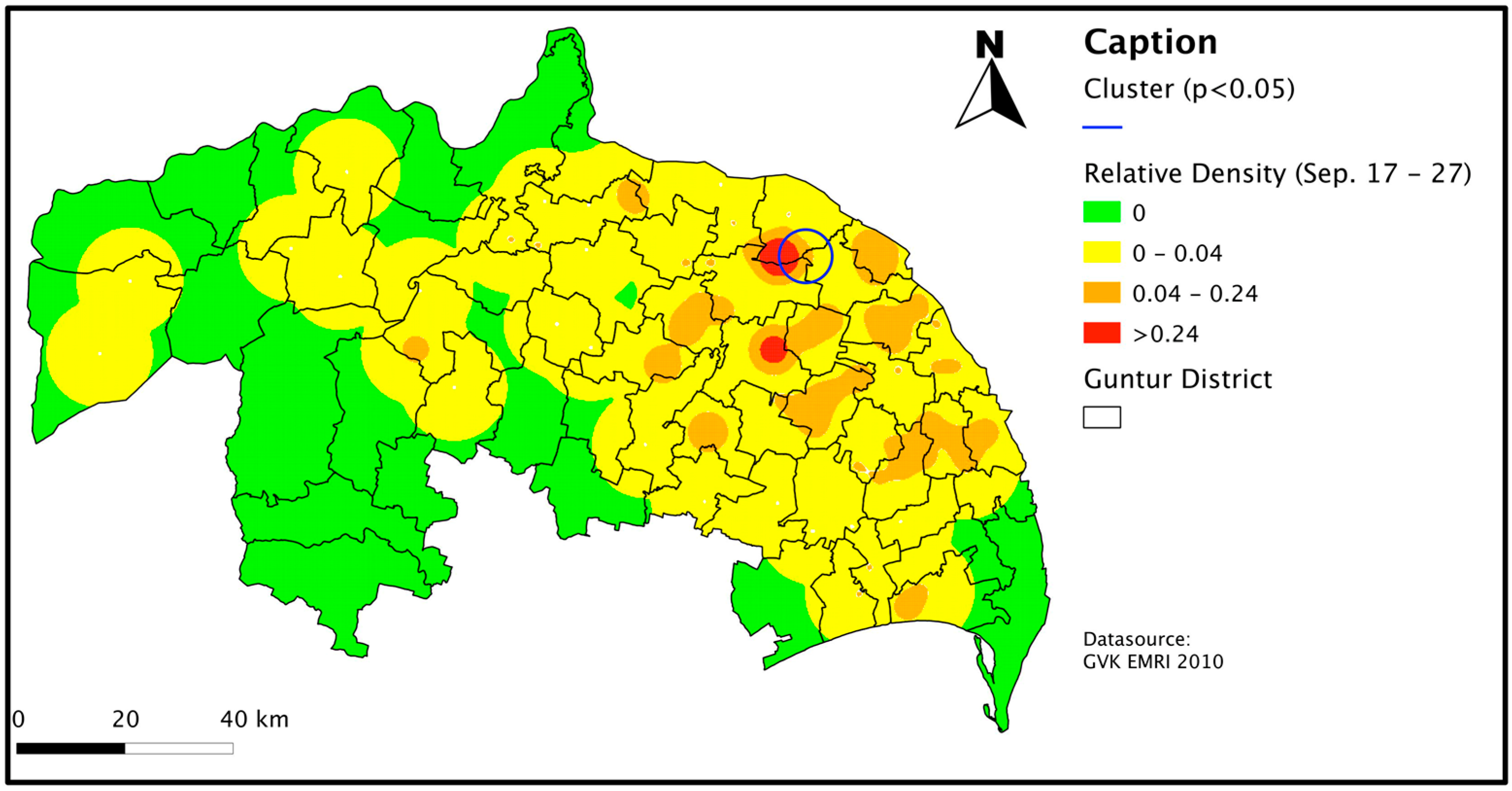
3.3.1. Retrospective Spatio-Temporal Fever Cluster Analysis
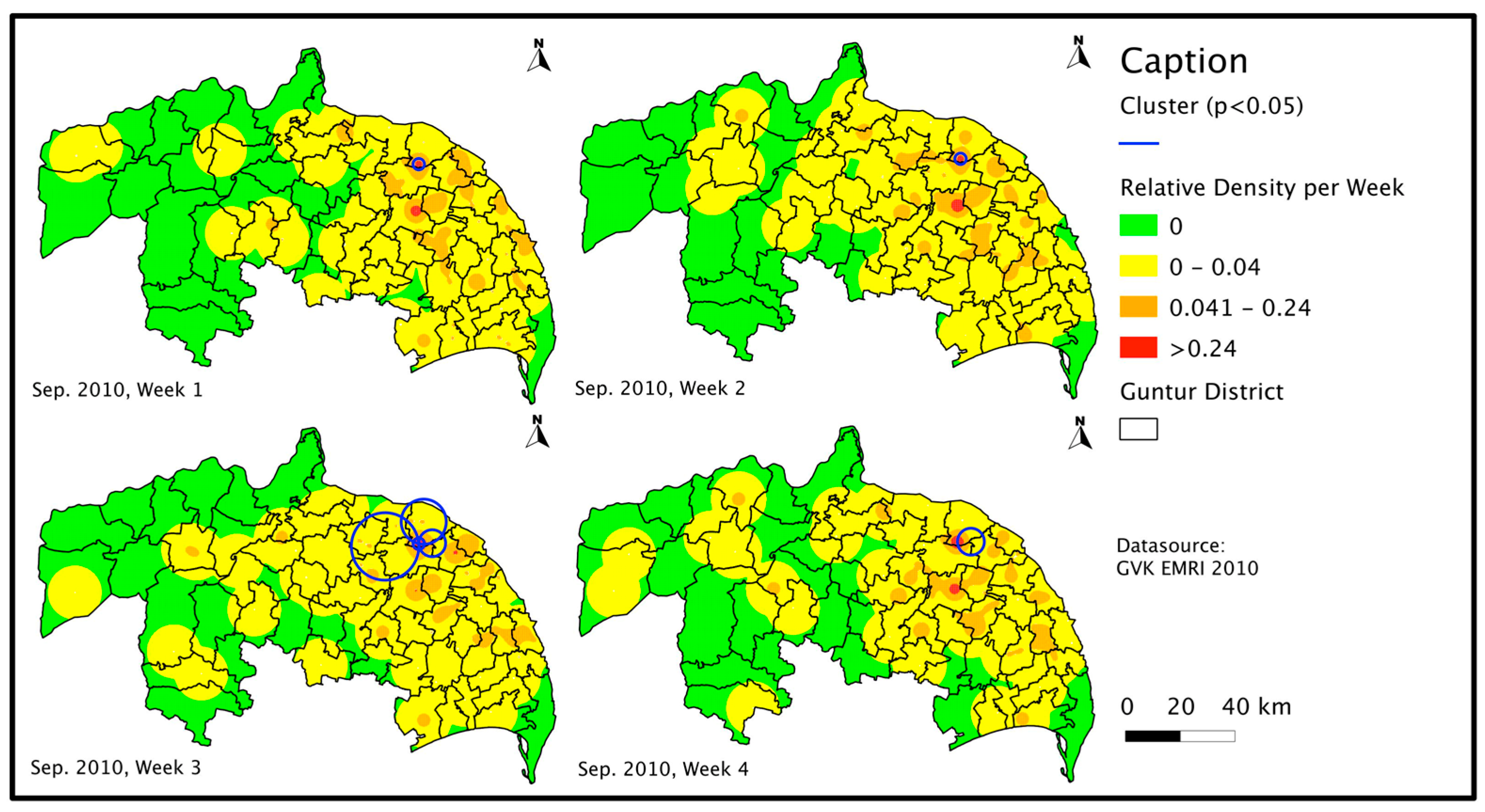
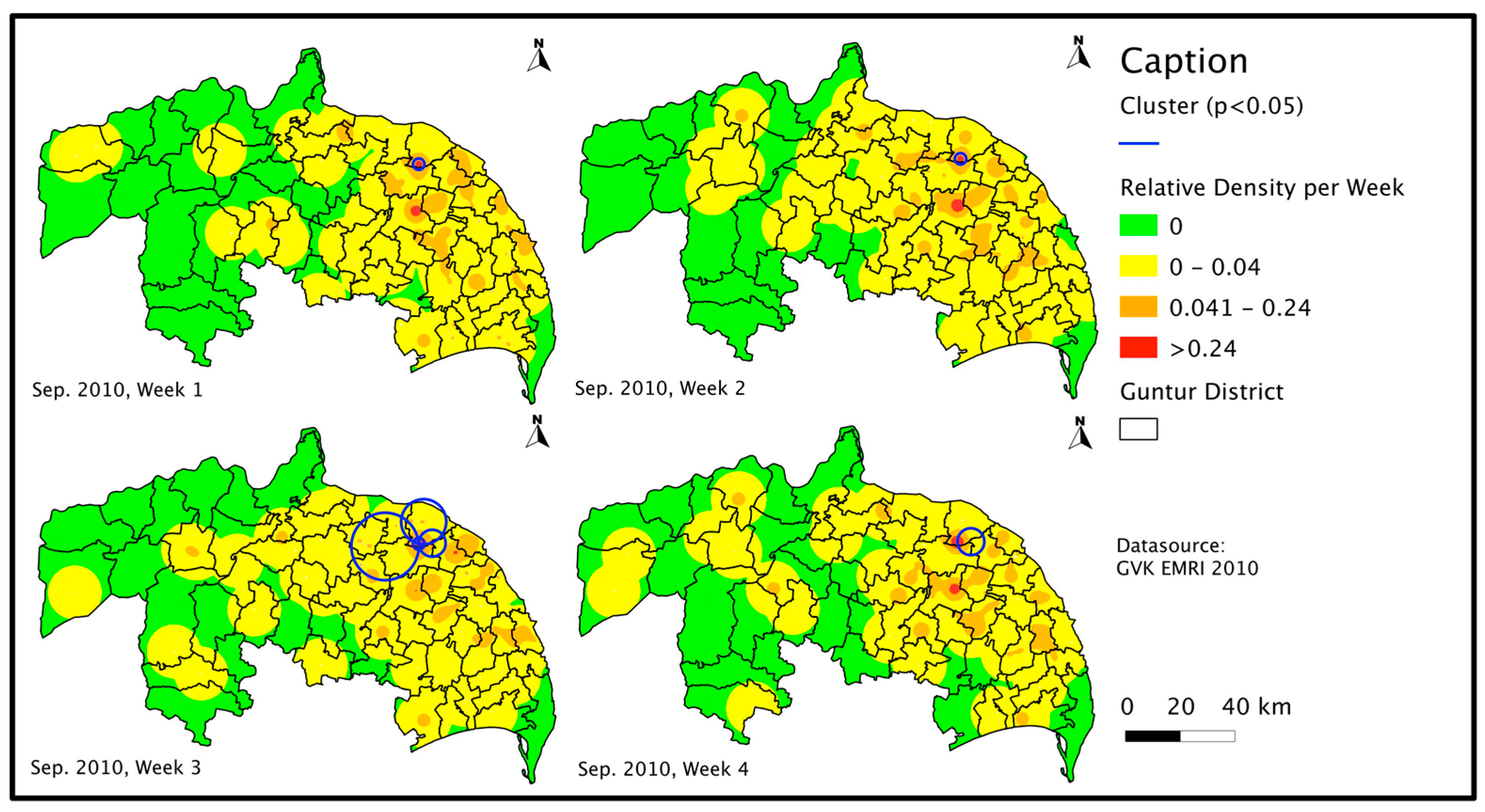
3.3.2. Prospective Spatio-Temporal Cluster Analysis
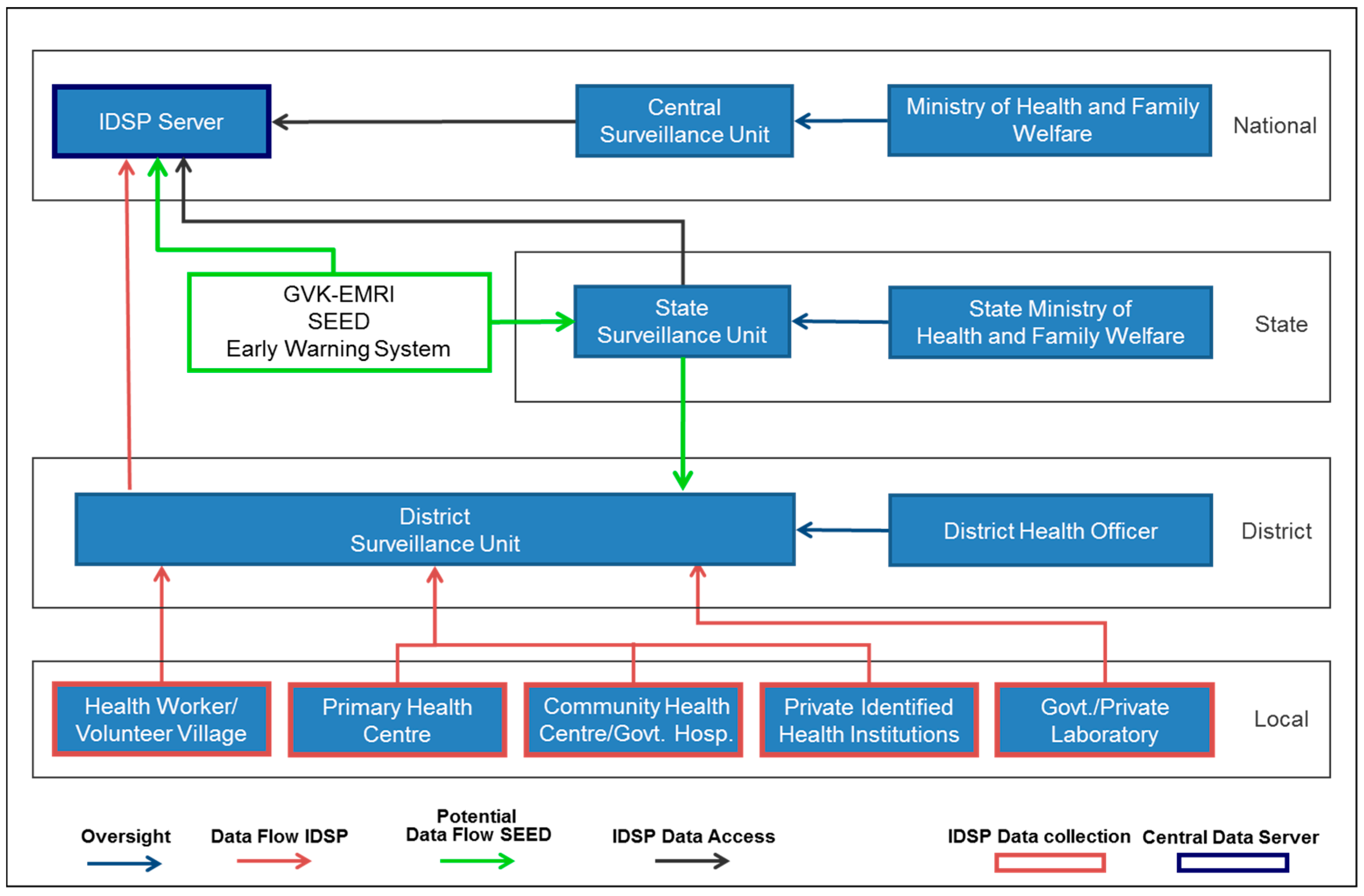
3.4. System of Early Warning Using Emergency Data Potential Integration Analysis into Integrated Disease Surveillance Program
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. The World Health Report 2007: A Safer Furture Global Public Health Security in the 21st Century; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Bayntun, C.; Houlihan, C.; Edmunds, J. Ebola crisis: Beliefs and behaviours warrant urgent attention. Lancet 2014, 384, 1424. [Google Scholar] [CrossRef]
- Nuttall, I. International Health Regulations (2005): Taking stock. Bull. WHO 2014, 92, 310. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Health Regulations (2005), 2nd ed.; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Ijaz, K.; Kasowski, E.; Arthur, R.R.; Angulo, F.J.; Dowell, S.F. International Health Regulations—What Gets Measured Gets Done. Emerg. Infect. Dis. 2012, 18, 1054–1057. [Google Scholar] [CrossRef] [PubMed]
- May, L.; Chretien, J.P.; Pavlin, J. Beyond traditional surveillance: Applying syndromic surveillance to developing settings–opportunities and challenges. BMC Public Health 2009, 9, 242. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Implementation of the International Health Regulations (2005). Responding to Public Health Emergencies; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Suresh, K. Integrated Diseases Surveillance Project (IDSP) Through a Consultant’s Lens. Indian J. Public Health 2008, 52, 136–143. [Google Scholar] [PubMed]
- Davies, S.E. The challenge to know and control: Disease outbreak surveillance and alerts in China and India. Glob. Public Health 2012, 7, 695–716. [Google Scholar] [CrossRef] [PubMed]
- Flahault, A. Emerging infectious diseases: The example of the Indian Ocean chikungunya outbreak (2005–2006). Bulletin de L’Academie Nationale de Medicine 2007, 191, 113–124. [Google Scholar]
- John, T.J.; Dandona, L.; Sharma, V.P.; Kakkar, M. Continuing challenge of infectious diseases in India. Lancet 2011, 377, 252–269. [Google Scholar] [CrossRef]
- Patel, V.; Kumar, A.K.S.; Paul, V.K.; Rao, K.D.; Reddy, K.S. Universal health care in India: The time is right. Lancet 2011, 377, 448–449. [Google Scholar] [CrossRef]
- Narain, J.P. Public Health Challenges in India: Seizing the Opportunities. Indian J. Community Med. 2016, 41, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.K.M.; Awasthi, S.; deSilva, H.J. Burden of infectious diseases in South Asia. BMJ (Clin. Res. Ed.) 2004, 328, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis; SAGE Publications: London, UK, 2006. [Google Scholar]
- Riesgo, L.G.; Ziemann, A.; Rosenkoetter, N.; Krafft, T.; Fischer, M.; Lippert, F.; Vergeiner, G.; Gillet, J.B.; Meulemans, A.; Kraemer, A.; et al. Use of routinely collected emergency medical data for earlier detection of health threats in Europe: First evaluation results of the SIDARTHa syndromic surveillance system. Resuscitation 2010, 81, S7. [Google Scholar] [CrossRef]
- Ziemann, A.; Riesgo, L.G.; Boris, K.; Schrell, S.; Rosenkötter, N.; Fischer, M.; Vergeiner, G.; Gillet, J.; Meulemans, A.; Krafft, T. Added value of routine emergency medical data for detecting clusters of acute gastrointestinal illness in Europe. Resuscitation 2012, 83, e30. [Google Scholar] [CrossRef]
- Jena, B.; Murthy, M.P.; Ramanarao, G. Demand pattern of Medical Emergency Services for Infectious Diseases in Andhra Pradesh-A Geo spatial Temporal Analysis of Fever cases. Indian Emerg. J. 2010, V, 5–9. [Google Scholar]
- Costa, M.A.; Kulldorff, M. Maximum linkage space–time permutation scan statistics for disease outbreak detection. Int. J. Health Geogr. 2014, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- SaTScan. SaTScan Software for the Spatial, Temporal, and Space–Time Scan Statistics. Available online: http://www.satscan.org/ (accessed on 26 September 2016).
- QGIS. QGIS A Free and Open Source Geographic Information System. 2016. Available online: http://www.qgis.org/en/site/ (accessed on 26 September 2016).
- National Commission on Macroeconomics and Health. Burden of Disease in India; National Commission on Macroeconomics and Health: New Delhi, India, 2005. [Google Scholar]
- World Health Organization. Country Cooperation Strategy India; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Dikid, T.; Jain, S.K.; Sharma, A.; Kumar, A.; Narain, J.P. Emerging & re-emerging infections in India: An overview. Indian J. Med. Res. 2013, 138, 19–31. [Google Scholar] [PubMed]
- Bachani, D. Integration of disease surveillance in India: Current scenario and future perspective. Indian J. Public Health 2006, 50, 7–10. [Google Scholar] [PubMed]
- High Level Expert Group for Universal Health Coveage. Executive Summary: High Level Expert Group Report on Universal Health Coverage for India; Planning Commission of India: New Delhi, India, 2011. [Google Scholar]
- Instituted by the Planning Commission of India. High Level Expert Group Report on Universal Health Coverage for India; Planning Commission of India: New Delhi, India, 2011. [Google Scholar]
- Pilot, E.; Rao, R.; Jena, B.; Krafft, T. Emergency Medical Service (EMS) Data for Syndromic Surveillance in Andhra Pradesh, India. In Environment and Health in Urban Areas; Wang, W., Krafft, T., Rosenberg, M., Pilot, E., Eds.; China Environmental Press: Beijing, China, 2014. [Google Scholar]
- Foreit, K.; Moreland, S.; LaFond, A. Data Demand and Information Use in the Health Sector Conceptual Framework; MEASURE Evaluation: Chapel Hill, NC, USA, 2006. [Google Scholar]
- Moreland, S.; Misra, S.N.; Agarwal, S.; Gupta, R.B.; Harrison, T.; Agrawal, S.; Gupta, R.B.; Harrison, T. Data Use in the Indian Health Sector; MEASURE Evaluation: Chapel Hill, NC, USA, 2009. [Google Scholar]
- Ministry of Health and Family Welfare. National Health Policy 2015 Draft; Ministry of Health and Family Welfare: New Delhi, India, 2014.
- Balarajan, Y.; Selvaraj, S.; Subramanian, S.V. Health care and equity in India. Lancet 2011, 377, 505–515. [Google Scholar] [CrossRef]
- NCDC; MoHFW; GoI. Integrated Disease Surveillance Programme (IDSP). Available online: http://www.idsp.nic.in/ (accessed on 10 March 2015).
- TripleS Project. Assessment of syndromic surveillance in Europe. Lancet 2011, 378, 1833–1834. [Google Scholar]
- Seyler, T.; Hutin, Y.; Ramanchandran, V.; Ramakrishnan, R.; Manickam, P.; Murhekar, M. Estimating the burden of disease and the economic cost attributable to chikungunya, Andhra Pradesh, India, 2005–2006. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Gore, M.M. Need for constant monitoring of dengue infections. Indian J. Med. Res. 2005, 121, 9–12. [Google Scholar] [PubMed]
- Garg, P.; Nagpal, J.; Khairnar, P.; Seneviratne, S.L. Economic burden of dengue infections in India. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Rosenkötter, N.; Ziemann, A.; Krafft, T.; Riesgo, L.G.; Vergeiner, G.; Brand, H. Non-infectious events under the International Health Regulations (2005) in Europe—A case for syndromic surveillance. J. Public Health Policy 2014, 35, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Ziemann, A.; Rosenkötter, N.; Riesgo, L.; Fischer, M.; Krämer, A.; Lippert, F.K.; Vergeiner, G.; Brand, H.; Krafft, T. Meeting the International Health Regulations (2005) surveillance core capacity requirements at the subnational level in Europe: The added value of syndromic surveillance. BMC Public Health 2015, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Buehler, J.; Hopkins, R.S.; Overhage, J.M.; Sosin, D.M.; Van Tong, M.P.H. Framework for Evaluating Public Health Surveillance Systems for Early Detection of Outbreaks Recommendations from the CDC Working Group. MMWR. 2014, 53, 1–11. [Google Scholar]
- Umar, N.S.; MNV, P.; Jena, B. Use of ARIMA models for forecasting needs in Emergency data based Syndromic Surveillance. Indian Emerg. J. 2010, V, 17–20. [Google Scholar]
- Kauhl, B.; Pilot, E.; Rao, R.; Gruebner, O.; Schweikart, J.; Krafft, T. Estimating the spatial distribution of acute undifferentiated fever (AUF) and associated risk factors using emergency call data in India. A symptom-based approach for public health surveillance. Health Place 2015, 31, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Kumutha, J.; Rao, G.V.R.; Sridhar, B.N.; Vidyasagar, D. The GVK EMRI maternal and neonatal transport system in India : A mega plan for a mammoth problem. Semi. Fetal Neonatal Med. 2015, 20, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Express News Service. Health Emergency in Guntur District; Indian Express, 2010. Available online: http://www.newindianexpress.com/states/andhra_pradesh/article297732.ece (accessed on 20 May 2007).
- Ramagopal, S. Not an Emergency, But a Calamity in Guntur—The New Indian Express; Indian Express, 2010; Available online: http://www.newindianexpress.com/states/andhra_pradesh/article300929.ece (accessed on 1 October 2014).
- Morse, S.S. Public health surveillance and infectious disease detection. Biosecur. bioterror. 2012, 10, 6–16. [Google Scholar] [CrossRef] [PubMed]
- May, L.; Katz, R.L.; Test, E.; Baker, J. Applications of Syndromic Surveillance in Resource Poor Settings. World Med. Health Policy 2011, 3, 1–29. [Google Scholar] [CrossRef]
- Garg, R.H. Who killed Rambhor?: The state of emergency medical services in India. J. Emerg. Trauma Shock. 2012, 5, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Brand, H.; Krafft, T. The icelandic ash cloud and other erupting health threats:what role for syndormic surveillance? Eur. J. Public Health 2010, 20, 367–368. [Google Scholar] [CrossRef] [PubMed]
- Kant, L.; Krishnan, S.K. Information and communication technology in disease surveillance, India: A case study. BMC Public Health 2010, 10, S11. [Google Scholar] [CrossRef] [PubMed]
- Planning Commission Government of India. Twelfth Five Year Plan (2012–2017) Economic Sector Volume II; Planning Commission Government of India: New Delhi, India, 2013.
- UNECE HLG-MOS. High-Level Group for the Modernisation of Official Statistics. 2016. Available online: http://www1.unece.org/stat/platform/display/hlgbas/High-Level+Group+for+the+Modernisation+of+Official+Statistics (accessed on 1 January 2016).
- Krafft, T.; Pilot, E.; Sarkar, B.K.; Ryland, P.; Reeves, L.; Singh, V. Research and Innovations Guiding Public Health Surveillance in the Twenty-first Century. In Transforming Public Health Surveillance; McNabb, S., Code, J., Ferland, L., Macwright, W., Okutani, S., Park, M., Ryland, P., Shakh, A., Singh, V., Conde, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2015; pp. 388–397. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interview Questions |
|---|
|
| Interview Questions |
|---|
|
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilot, E.; Roa, R.; Jena, B.; Kauhl, B.; Krafft, T.; Murthy, G. Towards Sustainable Public Health Surveillance in India: Using Routinely Collected Electronic Emergency Medical Service Data for Early Warning of Infectious Diseases. Sustainability 2017, 9, 604. https://doi.org/10.3390/su9040604
Pilot E, Roa R, Jena B, Kauhl B, Krafft T, Murthy G. Towards Sustainable Public Health Surveillance in India: Using Routinely Collected Electronic Emergency Medical Service Data for Early Warning of Infectious Diseases. Sustainability. 2017; 9(4):604. https://doi.org/10.3390/su9040604
Chicago/Turabian StylePilot, Eva, Ramana Roa, Biranchi Jena, Boris Kauhl, Thomas Krafft, and GVS Murthy. 2017. "Towards Sustainable Public Health Surveillance in India: Using Routinely Collected Electronic Emergency Medical Service Data for Early Warning of Infectious Diseases" Sustainability 9, no. 4: 604. https://doi.org/10.3390/su9040604