Demand and Supply Side Barriers that Limit the Uptake of Nutrition Services among Pregnant Women from Rural Ethiopia: An Exploratory Qualitative Study

 ,
,
Abstract
:1. Introduction
2. Methods and Materials
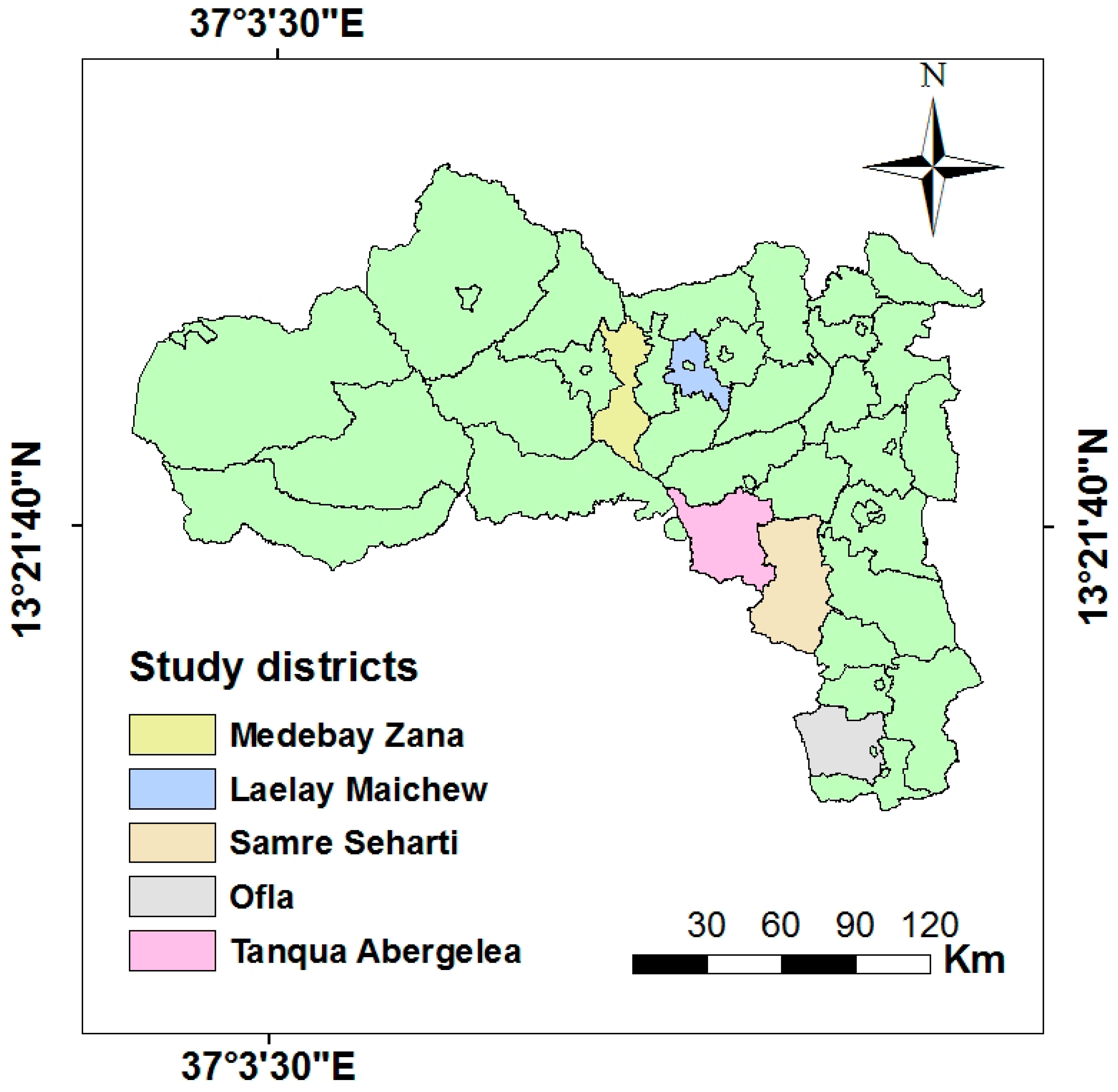
2.1. Study Setting
2.2. Study Design
2.3. Sample
2.4. Data Collection Tools
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
3.1. Characteristics of Study Participants
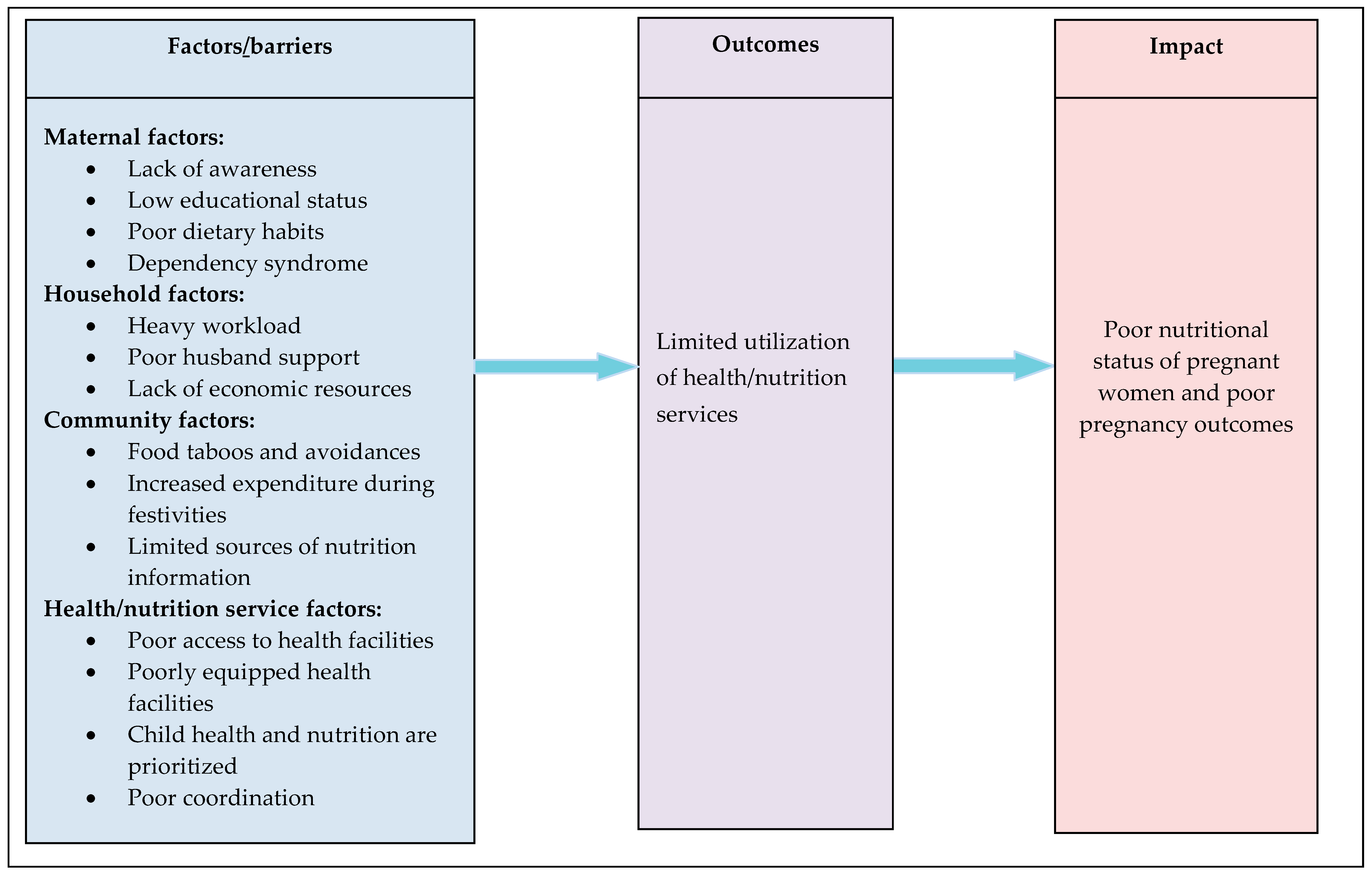
3.2. Emergent Themes
3.3. Maternal Factors
3.3.1. Lack of Awareness
3.3.2. Low Educational Status
3.3.3. Poor Dietary Habits
3.3.4. Dependency Syndrome
3.4. Household Factors
3.4.1. Heavy Workload
3.4.2. Poor Husband Support
3.4.3. Lack of Economic Resources
3.5. Community Factors
3.5.1. Food Taboos and Avoidances
3.5.2. Increased Expenditure on Cultural and Religious Festivities
3.5.3. Limited Sources of Nutrition Information
3.6. Health/Nutrition Service Factors
3.6.1. Poor Access to Health Facilities
3.6.2. Poorly Equipped Health Facilities
3.6.3. Focus on Child Health and Nutrition
3.6.4. Poor Coordination
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ingebretsen, H.; Lundbye, V.; Nutrition during Pregnancy. A Qualitative Study Performed in Pailin Province, Rural Cambodia. 2016. Available online: https://www.duo.uio.no/bitstream/handle/10852/55032/Prosjektoppgave-.pdf?sequence=1&isAllowed=y (accessed on 12 September 2018).
- Ezzati, M.; Lopez, D.; Rodgers, A.; Murray, J. Comparative Quantification of Health Risks. The Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; World Health Organization: Geneva, Switzerland, 2004; Available online: http://apps.who.int/iris/handle/10665/42770 (accessed on 10 September 2018).
- Malik, S.; Diot, A.; Morten, K.; DombiE, S.; Vatish, M.; Richard, C.A.; Poulton, J. Acute nutritional stress during pregnancy affects placental efficiency, fetal growth, and adult glucose homeostasis. Oncotarget 2017, 8, 109478–109486. [Google Scholar] [CrossRef] [PubMed]
- Herring, S.J.; Oken, E. Weight Gain during Pregnancy: Importance for Maternal and Child Health. Ann. Nestlé 2010, 68, 17–28. [Google Scholar] [CrossRef]
- The Manoff Group. Guidance for Formative Research on Maternal Nutrition; Prepared for the Infant and Young Child Nutrition Project; The Manoff Group: Washington, DC, USA, 2011. [Google Scholar]
- Black, E.; Victora, G.; Walker, P.; Bhutta, A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Barker, D.J. Developmental origins of chronic disease. Public Health 2012, 126, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM); National Research Council (NRC). Weight Gain during Pregnancy: Reexamining the Guidelines; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Black, E.; Allen, H.; Bhutta, A.; Caulfield, E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Ensenauer, R.; Chmitorz, A.; Riedel, C.; Fenske, N.; Hauner, H.; Nennstiel-Ratzel, U.; von Kries, R. Effects of suboptimal or excessive gestational weight gain on childhood overweight and abdominal adiposity: Results from a retrospective cohort study. Int. J. Obes. 2013, 37, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Stotland, N.E.; Gilbert, P.; Bogetz, A.; Harper, C.C.; Abrams, B.; Gerbert, B. Preventing excessive weight gain in pregnancy: How do prenatal care providers approach counseling. J. Womens Health 2010, 19, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Mamo, N.; Tsegaye, G.; Desta, G. Housheold food inecurity, low dietary diversity, and early marriage were predictors of undernutrition among pregnant women residing in Gambella, Ethiopia. Adv. Public Health 2018. [Google Scholar] [CrossRef]
- Weinshet, G.; Tefera, B.; Amare, D. Prevalence of anemia and associated factors among pregnant women attending antenatal care (ANC) in Butajera General Hospital, Southern Ethiopia. Int. J. Immunol. 2016, 4, 13–19. [Google Scholar]
- Asefa, F.; Nemomsa, D. Gestational weight gain and its associated factors in Harari Regional State: Institution based cross-sectional study, Eastern Ethiopia. Reprod. Health 2016, 13, 101. [Google Scholar] [CrossRef] [PubMed]
- Darnton-Hill, L.; Webb, P.; Harvey, P.W.J.; Hunt, J.M.; Dalmiya, N.; Chopra, M.; Ball, M.J.; Bloem, M.W.; de Benoist, B. Micronutrient deficiencies and gender: Socila and economic costs. Am. J. Clin. Nutr. 2005, 819, 1198S–1205S. [Google Scholar] [CrossRef] [PubMed]
- Meselech, D.; Ejigu, Z.; Shimelash, W.; Ayanaw, B. Folic acid usage and associated factors in the prevention of neural tube defects among pregnant women in Ethiopia: Cross sectional study. BMC Pregnancy Childbirth 2017, 17, 313. [Google Scholar]
- Tesfaye, B.; Mequanent, B.; Fantahun, M. Compliance with iron and folic acid supplementation in pregnancy, Northwest Ethiopia. BMC Res. Notes 2018, 11, 345. [Google Scholar]
- Abel, G.; Sisay, T.; Birkneh, T. Magnitude of Neural Tube Defects and Associated Factors at Three Teaching Hopitals in Addis Ababa, Ethiopia. Hindawi BioMed Res. Int. 2018. [Google Scholar] [CrossRef]
- Tadesse, Z.; Melaku, U.; Kaleab, B. Dietary diversity during pregnancy is associated with reduced risk of maternal anemia, preterm birth delivery and low birth weight in a prospective cohort study in rural Ethiopia. Am. J. Clin. Nutr. 2016, 103, 1482–1488. [Google Scholar]
- Ministry of Health (MOH). Program Implementation Manual of National Nutrition Program; Ministry of Health (MOH): Addis Ababa, Ethiopia, 2016.
- Ministry of Health (MOH). Sector Transformation Plan (2016–2020); Ministry of Health (MOH): Addis Ababa, Ethiopia, 2016.
- Peters, D.H.; Garg, A.; Bloom, G.; Walker, D.G.; Brieger, W.R.; Hafizur Rahman, M. Poverty and access to health care in developing countries. Ann. N. Y. Acad. Sci. 2008, 1136, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (MOH). The Seqota Declaration: A Government of Ethiopia Commitment to End Child Undernutrition in Ethiopia by 2030; Ministry of Health (MOH): Addis Ababa, Ethiopia, 2016.
- Stephen, D. Food Insecurity in Ethiopia: A Discussion Paper for DFID; IDS Sussex: Brighton, UK, 2000. [Google Scholar]
- Amaha, K.; Afework, M.; Omer, S. Nutritional status of children (6–59 months) from food secure and food insecure households in rural communities of SaesieTsaeda-Emba District, Tigray, North Ethiopia: Comparative study. Int. J. Food Sci. Nutr. 2015, 4, 51–65. [Google Scholar]
- Maes, K.; Closser, S.; Yihenew, T.; Yasmine, G.; Roza, A. Volunteers in Ethiopia’s women’s development army are more deprived and distressed than their neighbors: Cross-sectional survey data from rural Ethiopia. BMC Public Health 2018, 18, 258. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (MOH). Ethiopia Federal Ministry of Health. Health Sector Development Programme-IV2011. 2011. Available online: http://www.nationalplanningcycles.org/sites/default/files/country_docs/Ethiopia/ethiopia_hsdp_iv_final_draft_2010_-2015.pdf (accessed on 6 September 2018).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Kululanga, L. Barriers to husbands’ involvement in maternal health care in a rural setting in Malawi: A qualitative study. J. Res. Nurs. Midwifery 2012, 1, 1–10. [Google Scholar]
- Daba, G.; Beyene, F.; Fekadu, H.; Garoma, W. Assessment of Knowledge of Pregnant Mothers on Maternal Nutrition and Associated Factors in Guto Gida Woreda, East Wollega Zone, Ethiopia. J. Nutr. Food Sci. 2013, 3, 130. [Google Scholar]
- Nguyen, P.; Sanghvi, T.; Kim, S.S.; Tran, L.M.; Afsana, K.; Mahmud, Z.; Aktar, B.; Menon, P. Factors influencing maternal nutrition practices in a large scale maternal, newborn and child health program in Bangladesh. PLoS ONE 2017, 12, e0179873. [Google Scholar] [CrossRef] [PubMed]
- Fallah, F.; Pourabbas, A.; Delpisheh, A.; Veisani, Y.; Shadnoush, M. Effects of Nutrition Education on Levels of Nutritional Awareness of Pregnant Women in Western Iran. Int. J. Endocrinol. Metab. 2013, 11, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Daniel, S.; Gnanaraj, G.; Sharmine, E. Effect of nutrition education among pregnant women with low body mass index: A community based intervention. Int. J. Community Med. Public Health 2016, 3, 3135–3139. [Google Scholar] [CrossRef]
- Mohannad, A.; Irfan, G. Impact of Maternal Education, and Socioeconomic Status on Maternal Nutritional Knowledge and Practices Regarding Iron Rich Foods and Iron Supplements. Ann. Pak. Inst. Med. Sci. 2012, 8, 101–105. [Google Scholar]
- Dai, L.; Mao, Y.-Y.; Luo, X.-M.; Shen, Y.-P. Prenatal Care in Combination with Maternal Educational Level Has a Synergetic Effect on the Risk of Neonatal Low Birth Weight: New Findings in a Retrospective Cohort Study in Kunshan City, China. PLoS ONE 2014, 9, e113377. [Google Scholar] [CrossRef] [PubMed]
- Taddese, A.; Melaku, U.; Kaleab, B. Dietary habits, food taboos, and perceptions towards weight gain during pregnancy in Arsi, rural central Ethiopia: A qualitative cross-sectional study. J. Health Popul. Nutr. 2016, 35, 22. [Google Scholar] [CrossRef]
- Amanuel, N.; Tona, Z. Dietary practices, and associated factors during pregnancy in northwestern Ethiopia. BMC Pregnancy Childbirth 2018, 18, 183. [Google Scholar] [CrossRef]
- Eren, N.; Şencan, I.; Aksoy, H. Evaluation of dietary habits during pregnancy. Turk. J. Obstet. Gynecol. 2015, 12, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, P.; Jeremy, L. Dependency and Humanitarian Relief: A Critical Analysis; Humanitarian Policy Group, Overseas Development Institute: London, UK, 2005; ISBN 0-85003-756-5. [Google Scholar]
- Bethelhem, L.; Gerald, S.; Hoden, S. Does Ethiopia’s Productive Safety Net Program Improve Child Nutrition? Center for Land Tenure Studies Working Paper 01/14; Norwegian University of Life Sciences: Akershus, Norway, 2014. [Google Scholar]
- USAID. Maternal Dietary Diversity and the Implications for Children’s Diets in the Context of Food Security. 2012. Available online: http://www.iycn org (accessed on 12 September 2018).
- Lennox, J.; Petrucka, P.; Bassendowski, S. Eating practices during pregnancy: Perceptions of select Maasai women in Northern Tanzania. Glob. Health Res. Policy 2017, 2, 9. [Google Scholar] [CrossRef] [PubMed]
- Holmboe-Ottesen, G.; Mascarenhas, O.; Wandel, M. Women’s role in food production and nutrition: Implications for their quality of life. Food Nutr. Bull. 1988, 10, 13. [Google Scholar]
- Lowe, M.; Chen, D.-R.; Huang, S.-L. Social and Cultural Factors Affecting Maternal Health in Rural Gambia: An Exploratory Qualitative Study. PLoS ONE 2016, 11, e0163653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mkandawire, E.; Hendriks, S. A qualitative analysis of men’s involvement in maternal and child health as a policy intervention in rural Central Malawi. BMC Pregnancy Childbirth 2018, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Matovu, A.; Kirunda, B.G.; Rugamba-Kabagambe, M.; Tumwesigye, N.; Nuwaha, F. Factors influencing adherence to exclusive breast feeding among HIV positive mothers in Kabarole District, Uganda. East Afr. Med. J. 2008, 85, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Kansiime, N.; Atwine, D.; Nuwamanya, S.; Bagenda, F. Effect of Male Involvement on the Nutritional Status of Children Less Than 5 Years: A Cross Sectional Study in a Rural Southwestern District of Uganda. J. Nutr. Metab. 2017, 2017, 3427087. [Google Scholar] [CrossRef] [PubMed]
- Kululanga, L.; Sundby, J.; Malata, M.; Chirwa, E. Striving to promote male involvement in maternal health care in rural and urban settings in Malawi—A qualitative study. BMC Reprod. Health 2011, 8, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levay, V.; Mumtaz, Z.; Rashid, F.; Willows, N. Influence of gender roles and rising food prices on poor, pregnant women’s eating and food provisioning practices in Dhaka, Bangladesh. Reprod. Health 2013, 10, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, A.; Pike, I.L. A biocultural framework for examining maternal cravings and aversions among pastoral women in East Africa. Ecol. Food Nutr. 2012, 51, 444–462. [Google Scholar] [CrossRef] [PubMed]
- Suzan, C.; Yang, W.; Herring, A.; Barbara, A.; Gary, S. The Maternal Food Insecurity Is Associated with Increased Risk of Certain Birth Defects. J. Nutr. Epidemiol. 2007, 137, 2087–2092. [Google Scholar]
- Torheim, L.; Ferguson, EL.; Penrose, K.; Arimond, M. Women in resourcepoor settings are at risk of inadequate intakes of multiple micronutrients. J. Nutr. Food Sci. 2010, 140, 2051S–2058S. [Google Scholar]
- Na, M.; Mehra, S.; Christian, P.; Ali, H.; Shaikh, S.; Shamim, A.A.; Labrique, A.B.; Klemm, R.D.; Wu, L.S.; West, K.P., Jr. Maternal Dietary Diversity Decreases with Household Food Insecurity in Rural Bangladesh: A Longitudinal Analysis. J. Nutr. Community Int. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Catherin, N.; Rock, B.; Roger, V.; Ankita, C.; Ashish, G.; Delwin, P.; Deeepthi, S.; Goud, B.R. Beliefs and practices regarding nutrition during pregnancy and lactation in a rural area in Karnataka, India: A qualitative study. Int. J. Community Med. Public Health 2015, 2, 116–120. [Google Scholar] [CrossRef]
- Rakesh, B.; Yifru, T. A study of the impact of Orthodox Christians’ fasting on demand for biscuits in Ethiopia. Afr. J. Mark. Manag. 2010, 2, 10–17. [Google Scholar]
- Murphy, S.; Allen, L.H. The Nutritional importance of animal source foods. J. Nutr. Food Sci. 2003, 133, 3932S–3935S. [Google Scholar] [CrossRef] [PubMed]
- Soltan, H.; Duxbury, A.; Rundle, R.; Marvin-Dowle, K. Dietary habits and supplementation practices of young women during pregnancy: An online cross-sectional survey of young mothers and health care professionals. BMC Nutr. 2017, 3, 19. [Google Scholar] [CrossRef]
- Rao, V. Poverty and Public Celebrations in Rural India; Development Research Group, The World Bank, 1999. Available online: https://pdfs.semanticscholar.org/ea3d/3b45057c6c6f2820862ad4821abeae6a6f90.pdf (accessed on 2 September 2018).
- Gemeda, F.; Wondu, G.; Habtamu, F. Assessment of Nutritional Practices of Pregnant Mothers on Maternal Nutrition and Associated Factors in Guto Gida Woreda, East Wollega Zone, Ethiopia. Sci. Technol. Arts Res. J. 2013, 2, 105–113. [Google Scholar]
- Garnweidner, L.; Pettersen, K.; Mosdøl, A. Experiences with nutrition-related information during antenatal care of pregnant women of different ethnic backgrounds residing in the area of Oslo, Norway. Midwifery 2013, 29, e130–e137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucas, C.; Charlton, K.E.; Yeatman, H. Nutrition advice during pregnancy: Do women receive it and can health professionals provide it? Matern. Child Health J. 2014, 18, 2465–2478. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.; Tetui, M.; Kananura, R.; Ekirapa-Kiracho, E.; George, A.S. Gender dynamics affecting maternal health and health care access and use in Uganda. Health Policy Plan. 2017, 32, v13–v21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, B. Utilisation of Antenatal Care Services in Nepal. Nepal Popul. J. 2004, 11, 79–97. [Google Scholar]
- Matsumura, M.; Gubhaju, B. Women’s Status Household Structure and the Utilisation of Maternal Health Services in Nepal. Asia-Pac. Popul. J. 2001, 16, 23–44. [Google Scholar] [CrossRef]
- Simkhada, B.; Teijlingen, E.R.; Porte, M.; Simkhada, P. Major problems and key issues in Maternal Health in Nepal. Kathmandu Univ. Med. J. 2006, 4, 258–263. [Google Scholar]
- Kiwanuka, S.N.; Ekirapa, E.K.; Peterson, S.; Okui, O.; Rahman, M.H.; Peters, D.; Pariyo, G.W. Access to and utilization of health services for the poor in Uganda: A systematic review of available evidence. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Gelow, J.; Thornburg, K.; Osmond, C.; Kajantie, E.; Eriksson, J.G. The early origins of chronic heart failure: Impaired placental growth and initiation of insulin resistance in childhood. Eur. J. Heart Fail. 2010, 12, 819–825. [Google Scholar] [CrossRef] [PubMed]
- The National Food and Nutrition Commission (NFNC); Infant & Young Child Nutrition Project (IYCN). Qualitative Assessment of Maternal Nutrition Practices in Zambia. 2010. Available online: http://iycn.wpengine.netdna-cdn.com/files/IYCN_Zambia-Maternal-Nutrition-Report_040710.pdf (accessed on 2 September 2018).
- Justine, K.; Megan, L. Addressing barriers to maternal nutrition in low-and middle-income countries: A review of the evidence and programme implications. Matern. Child Nutr. 2018, 14, e12508. [Google Scholar]



{kind=link}
{kind=link}
| Participant Characteristics | KIIs, n (%) N = 90 | FGD Participants, n (%) N = 95 |
|---|---|---|
| Education | ||
| Formal education | - | 63 (66.3) |
| Elementary and secondary education | 18 (20) | 32 (33.7) |
| College and above | 72 (80) | - |
| Occupation | ||
| Farmer | 14 (15.6) | 92 (96.8) |
| Government employee | 76 (84.4) | 3 (3.2) |
| Distribution | ||
| Agriculture experts | 10 (11.1) | - |
| District education heads and school teachers | 13 (14.4) | - |
| Health extension workers | 8 (8.9) | - |
| Health workers | 10 (11.1) | |
| Husbands | -- | 3 (21.4) |
| Nutrition focal persons from the district and regional health offices | 9 (10.0) | - |
| Pregnant mothers | 6 (6.7) | 8 (57.2) |
| Religious leaders | 2 (2.2) | - |
| Tabia/kebelle leaders | 7 (7.8) | - |
| Water resource experts | 4 (4.4) | - |
| Women development groups | 6 (6.7) | 3 (21.4) |
| Women sector experts | 9 (10.0) | - |
| Youth association heads | 6 (6.7) | - |
| The average length of discussion in minutes * | 57.5 | 80 |
| Serial Number | Food Taboos During Pregnancy | Reasons for Avoidance |
|---|---|---|
| 1 | Qollo (roasted) of chickpea and wheat | Causes abdominal cramp in newborns |
| 2 | Green pepper | Green pepper affects eye of the infant |
| 3 | Hot coffee | Causes balding in children |
| 4 | Senaficho (dressing made from brassica) | Could cause miscarriage |
| 5 | Alcohol | Affects the health of the baby. |
| 6 | Shiro (stew/sauce) made from legumes | Provides no calorie/energy and do not protect from anemia |
| 7 | Roasted beans (Qollo of roasted bean) | Causes pain during delivery |
| 8 | Millet | Consumption causes constipation in pregnant women |
| 9 | Niger oil | Consumption of Niger oil causes skin darkness (black color) |
| 10 | Pea, bean, and maize | Causes nausea during pregnancy |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bezabih, A.M.; Wereta, M.H.; Kahsay, Z.H.; Getahun, Z.; Bazzano, A.N. Demand and Supply Side Barriers that Limit the Uptake of Nutrition Services among Pregnant Women from Rural Ethiopia: An Exploratory Qualitative Study. Nutrients 2018, 10, 1687. https://doi.org/10.3390/nu10111687
Bezabih AM, Wereta MH, Kahsay ZH, Getahun Z, Bazzano AN. Demand and Supply Side Barriers that Limit the Uptake of Nutrition Services among Pregnant Women from Rural Ethiopia: An Exploratory Qualitative Study. Nutrients. 2018; 10(11):1687. https://doi.org/10.3390/nu10111687
Chicago/Turabian StyleBezabih, Afework Mulugeta, Mekonnen Haileselassie Wereta, Znabu Hadush Kahsay, Zewditu Getahun, and Alessandra N. Bazzano. 2018. "Demand and Supply Side Barriers that Limit the Uptake of Nutrition Services among Pregnant Women from Rural Ethiopia: An Exploratory Qualitative Study" Nutrients 10, no. 11: 1687. https://doi.org/10.3390/nu10111687