Antioxidative Efficacy of a Pistacia Lentiscus Supplement and Its Effect on the Plasma Amino Acid Profile in Inflammatory Bowel Disease: A Randomised, Double-Blind, Placebo-Controlled Trial

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
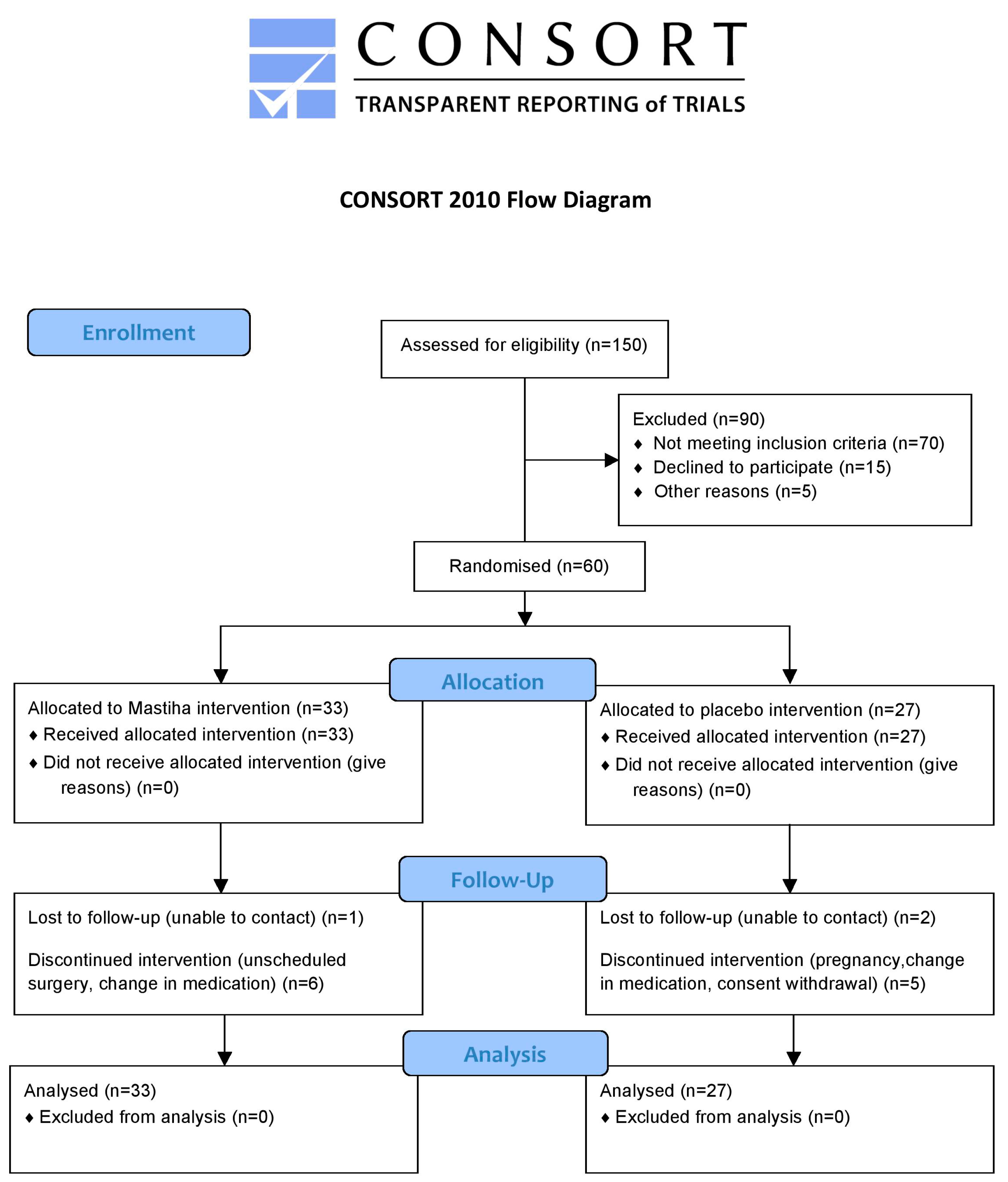
2.1. Study Design
2.2. Laboratory Analyses
2.2.1. Evaluation of Oxidative Stress
The Total Serum Oxidisability Assay
The oxLDL Assay
The Uric Acid Assay
2.2.2. AA Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Kirchgesner, J.; Beaugerie, L.; Carrat, F.; Andersen, N.N.; Jess, T.; Schwarzinger, M. BERENICE study group, Increased risk of acute arterial events in young patients and severely active IBD: A nationwide French cohort study. Gut 2018, 67, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Aniwan, S.; Pardi, D.S.; Tremaine, W.J.; Loftus, E.V., Jr. Increased risk of acute myocardial infarction and heart failure in patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.; Grácio, D.; Teixeira, J.P.; Magro, F. Oxidative stress and DNA damage: Implications in inflammatory bowel disease. Inflamm. Bowel. Dis. 2015, 21, 2403–2417. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Tang, W.; Ching, J.Y.; Wong, M.; Chow, C.M.; Hui, A.J.; Wong, T.C.; Leung, V.K.; Tsang, S.W.; Yu, H.H.; et al. Asia–Pacific Crohn’s and Colitis Epidemiologic Study (ACCESS) Study Group. Incidence and phenotype of inflammatory bowel disease based on results from the Asia-pacific Crohn’s and colitis epidemiology study. Gastroenterology 2013, 145, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Zhu, Z.; Yang, Y.; Ruan, W.; Peng, X.; Su, Y.; Peng, L.; Chen, J.; Yin, Q.; Zhao, C.; et al. Incidence and clinical characteristics of inflammatory bowel disease in a developed region of Guangdong Province, China: A prospective population-based study. J. Gastroenterol. Hepatol. 2013, 28, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Matheson, P.J.; Wilson, M.A.; Garrison, R.N. Regulation of intestinal blood flow. J. Surg. Res. 2000, 93, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Almenier, H.A.; Al Menshawy, H.H.; Maher, M.M.; Al Gamal, S. Oxidative stress and inflammatory bowel disease. Front. Biosci. (Elite Ed.) 2012, 4, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Kullo, I.J.; Pardi, D.S.; Loftus, E.V., Jr. Epidemiology, risk factors and management of cardiovascular diseases in IBD. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Jia, F.; Zhang, B.; Zhang, P. Risk of cardiovascular disease in inflammatory bowel disease. Exp. Ther. Med. 2017, 13, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, X.; Hu, C.A. Therapeutic Potential of Amino Acids in Inflammatory Bowel Disease. Nutrients 2017, 9, 920. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Feng, Z.; Yao, J.; Li, T.; Yin, Y. Roles of Dietary Amino Acids and Their Metabolites in Pathogenesis of Inflammatory Bowel Disease. Mediat. Inflamm. 2017. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, F.; Wu, C.; Li, P.; Li, N.; Zhang, D.; Zhu, Q.; Ren, W.; Peng, Y. Functions and signaling pathways of amino acids in intestinal inflammation. Biomed. Res. Int. 2018. [Google Scholar] [CrossRef] [PubMed]
- Shiomi, Y.; Nishiumi, S.; Ooi, M.; Hatano, N.; Shinohara, M.; Yoshie, T.; Kondo, Y.; Furumatsu, K.; Shiomi, H.; Kutsumi, H.; et al. GCMS-based metabolomic study in mice with colitis induced by dextran sulfate sodium. Inflamm. Bowel Dis. 2011, 17, 2261–2274. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, T.; Okamoto, S.; Hashimoto, M.; Muramatsu, T.; Andou, A.; Uo, M.; Kitazume, M.T.; Matsuoka, K.; Yajima, T.; Inoue, N.; et al. Novel, objective, multivariate biomarkers composed of plasma amino acid profiles for the diagnosis and assessment of inflammatory bowel disease. PLoS ONE 2012, 7, e31131. [Google Scholar] [CrossRef] [PubMed]
- Ooi, M.; Nishiumi, S.; Yoshie, T.; Shiomi, Y.; Kohashi, M.; Fukunaga, K.; Nakamura, S.; Matsumoto, T.; Hatano, N.; Shinohara, M.; et al. GC/MS-based profiling of amino acids and TCA cycle-related molecules in ulcerative colitis. Inflamm. Res. 2011, 60, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lin, L.; Xu, Y.; Lin, Y.; Jin, Y.; Zheng, C. 1H NMR-based spectroscopy detects metabolic alterations in serum of patients with early-stage ulcerative colitis. Biochem. Biophys. Res. Commun. 2013, 433, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, Y.; Zhang, Q.W.; Sugimoto, T.; Furuhata, Y.; Sakai, R.; Mori, M.; Takahashi, M.; Kimura, T. Network analysis of plasma and tissue amino acids and the generation of an amino index for potential diagnostic use. Am. J. Clin. Nutr. 2016, 83, 513S–519S. [Google Scholar] [CrossRef] [PubMed]
- Kaliora, A.C.; Mylona, A.; Chiou, A.; Petsios, D.G.; Andrikopoulos, N.K. Detection and identification of simple phenolics in pistacia lentiscus resin. J. Liq. Chromatogr. Relat. Technol. 2004, 27. [Google Scholar] [CrossRef]
- Assimopoulou, A.N.; Papageorgiou, V.P. GC-MS analysis of penta- and tetra-cyclic triterpenes from resins of Pistacia species. Part I. Pistacia lentiscus var. Chia. Biomed. Chromatogr. 2005, 19, 285–311. [Google Scholar] [CrossRef] [PubMed]
- Paraschos, S.; Magiatis, P.; Mitakou, S.; Petraki, K.; Kalliaropoulos, A.; Maragkoudakis, P.; Mentis, A.; Sgouras, D.; Skaltsounis, A.L. In vitro and in vivo activities of Chios mastic gum extracts and constituents against Helicobacter pylori. Antimicrob. Agents Chemother. 2007, 51, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Papada, E.; Gioxari, A.; Brieudes, V.; Amerikanou, C.; Halabalaki, M.; Skaltsounis, A.L.; Smyrnioudis, I.; Kaliora, A.C. Bioavailability of terpenes and postprandial effect on human antioxidant potential. An open–label study in healthy subjects. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef]
- Dedoussis, G.V.; Kaliora, A.C.; Psarras, S.; Chiou, A.; Mylona, A.; Papadopoulos, N.G.; Andrikopoulos, N.K. Antiatherogenic effect of Pistacia lentiscus via GSH restoration and downregulation of CD36 mRNA expression. Atherosclerosis 2004, 174, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Heo, C.; Kim, S.W.; Kim, K.J.; Kim, D.W.; Kim, H.J.; Do, J.H.; Chang, S.K. Protective effects of mastic in non- steroidal anti-inflammatory drug induced gut damage and bacterial translocation in a rat model. Korean J. Med. 2006, 71, 354–361. [Google Scholar]
- Kartalis, A.; Didagelos, M.; Georgiadis, I.; Benetos, G.; Smyrnioudis, N.; Marmaras, H.; Voutas, P.; Zotika, C.; Garoufalis, S.; Andrikopoulos, G. Effects of Chios mastic gum on cholesterol and glucose levels of healthy volunteers: A prospective, randomised, placebo-controlled, pilot study (CHIOS-MASTIHA). Eur. J. Prev. Cardiol. 2016, 23, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Kaliora, A.C.; Stathopoulou, M.G.; Triantafillidis, J.K.; Dedoussis, G.V.; Andrikopoulos, N.K. Alterations in the function of circulating mononuclear cells derived from patients with Crohn’s disease treated with mastic. World J. Gastroenterol. 2007, 13, 6031–6036. [Google Scholar] [PubMed]
- Kaliora, A.C.; Stathopoulou, M.G.; Triantafillidis, J.K.; Dedoussis, G.V.; Andrikopoulos, N.K. Chios mastic treatment of patients with active Crohn’s disease. World J. Gastroenterol. 2007, 13, 748–753. [Google Scholar] [CrossRef] [PubMed]
- EMA. Committee on Herbal Medicinal Products European Union Herbal Monograph on Pistacia lentiscus L., Resin (Mastix). London, UK, 2015. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Herbal_-_Herbal_monograph/2015/07/WC500190099.pdf (accessed on 8 January 2018).
- Papada, E.; Gioxari, A.; Amerikanou, C.; Forbes, A.; Tzavara, C.; Smyrnioudis, I.; Kaliora, A.C. Regulation of faecal biomarkers in inflammatory bowel disease patients treated with oral mastiha (Pistacia lentiscus) supplement: A double-blind and placebo-controlled randomised trial. Phytother. Res. 2018. [Google Scholar] [CrossRef]
- Papada, E.; Torović, L.; Amerikanou, C.; Kalogeropoulos, N.; Smyrnioudis, I.; Kaliora, A.C. Μodulation of free amino acid profile in healthy humans administered with mastiha terpenes. Αn open-label trial. Nutrients 2018, 10, 715. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Yin, Y.L.; Li, D.; Kim, S.W.; Wu, G. Amino acids and immune function. Br. J. Nutr. 2007, 98, 237–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakaya, M.; Xiao, Y.; Zhou, X.; Chang, J.H.; Chang, M.; Cheng, X.; Blonska, M.; Lin, X.; Sun, S.C. Inflammatory T cell responses rely on amino acid transporter ASCT2 facilitation of glutamine uptake and mTORC1 kinase activation. Immunity 2014, 40, 692–705. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 8167, 514. [Google Scholar] [CrossRef]
- Lewis, J.D.; Chuai, S.; Nessel, L.; Lichtenstein, G.R.; Aberra, F.N.; Ellenberg, J.H. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm. Bowel Dis. 2008, 14, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Aurrekoetxea, I.; Ruiz-Sanz, J.I.; del Agua, A.R.; Navarro, R.; Hernández, M.L.; Matorras, R.; Prieto, B.; Ruiz-Larrea, M.B. Serum oxidizability and antioxidant status in patients undergoing in vitro fertilization. Fertil. Steril. 2010, 94, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Gioxari, A.; Kaliora, A.C.; Papalois, A.; Agrogiannis, G.; Triantafillidis, J.K.; Andrikopoulos, N.K. Pistacia lentiscus resin regulates intestinal damage and inflammation in trinitrobenzene sulfonic acid-induced colitis. J. Med. Food. 2011, 14, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Guidance on the scientific requirements for health claims related to antioxidants, oxidative damage and cardiovascular health. EFSA J. 2011, 9, 474. [Google Scholar] [CrossRef]
- Grip, O.; Janciauskiene, S.; Lindgren, S. Circulating monocytes and plasma inflammatory biomarkers in active Crohn’s disease: Elevated oxidised low-density lipoprotein and the anti-inflammatory effect of atorvastatin. Inflamm. Bowel Dis. 2004, 10, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Parker, R.D.; Abdollahi, M. Oxidative stress and pathogenesis of inflammatory bowel disease: An epiphenomenon or the cause? Dig. Dis. Sci. 2007, 52, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Beltran, B.; Nos, P.; Dasi, F.; Iborra, M.; Bastida, G.; Martinez, M.; O’Connor, J.E.; Saez, G.; Moret, I.; Ponce, J. Mitochondrial dysfunction, persistent oxidative damage, and catalase inhibition in immune cells of naive and treated Crohn’s disease. Inflamm. Bowel Dis. 2010, 16, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Iborra, M.; Moret, I.; Rausell, F.; Bastida, G.; Aguas, M.; Cerrillo, E.; Nos, P.; Beltran, B. Role of oxidative stress and antioxidant enzymes in Crohn’s disease. Biochem. Soc. Trans. 2011, 39, 1102–1106. [Google Scholar] [CrossRef] [PubMed]
- Moret-Tatay, I.; Iborra, M.; Cerrillo, E.; Tortosa, L.; Nos, P.; Beltran, B. Possible biomarkers in blood for Crohn’s disease: Oxidative stress and microRNAs-current evidences and further aspects to unravel. Oxid. Med. Cell Longev. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Mai, W.; Liu, D.; Hao, Y.; Tao, J.; Dong, Y. The oxidation ratio of LDL: A predictor for coronary artery disease. Dis. Mark. 2008, 24, 341–349. [Google Scholar] [CrossRef]
- Motamed, M.; Nargesi, A.A.; Heidari, B.; Mirmiranpour, H.; Esteghamati, A.; Nakhjavani, M. Oxidized low-lensity Lipoprotein (ox-LDL) to LDL Ratio (ox-LDL/LDL) and ox-LDL to high-density lipoprotein ratio (ox-LDL/HDL). Clin. Lab. 2016, 62, 1609–1617. [Google Scholar] [CrossRef] [PubMed]
- Gradinaru, D.; Borsa, C.; Ionescu, C.; Margina, D. Advanced oxidative and glycoxidative protein damage markers in the elderly with type 2 diabetes. J. Proteom. 2013, 92, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Harmon, M.E.; Campen, M.J.; Miller, C.; Shuey, C.; Cajero, M.; Lucas, S.; Pacheco, B.; Erdei, E.; Ramone, S.; Nez, T.; et al. Associations of circulating oxidized LDL and conventional biomarkers of cardiovascular disease in a cross-sectional study of the Navajo population. PLoS ONE 2016, 11, e0143102. [Google Scholar] [CrossRef] [PubMed]
- Atkuri, K.R.; Mantovani, J.J.; Herzenberg, L.A.; Herzenberg, L.A. N-Acetylcysteine—A safe antidote for cysteine/glutathione deficiency. Curr. Opin. Pharmacol. 2007, 7, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Forrest, C.M.; Mackay, G.M.; Stoy, N.; Egerton, M.; Christofides, J.; Stone, T.W.; Darlington, L.G. Tryptophan loading induces oxidative stress. Free Radic. Res. 2004, 38, 1167–1171. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, N.; Dickman, M.B.; Becker, D.F. Proline modulates the intracellular redox environment and protects mammalian cells against oxidative stress. Free Radic. Biol. Med. 2008, 44, 671–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katayama, S.; Mine, Y. Antioxidative activity of amino acids on tissue oxidative stress in human intestinal epithelial cell model. J. Agric. Food Chem. 2007, 55, 8458–8464. [Google Scholar] [CrossRef] [PubMed]
- Son, D.O.; Satsu, H.; Shimizu, M. Histidine inhibits oxidative stress- and TNF-alpha-induced interleukin-8 secretion in intestinal epithelial cells. FEBS Lett. 2005, 579, 4671–4677. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| IBD (N = 60) | CD (N = 40) | UC (N = 20) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Placebo (27) | PL (33) | P | Placebo (18) | PL (22) | P | Placebo (9) | PL (11) | P | |
| Sex | |||||||||
| Females | 9 (33.3) | 18 (54.5) | 0.100 + | 7 (38.9) | 11 (50) | 0.482 + | 2 (22.2) | 7 (63.6) | 0.092 ++ |
| Males | 18 (66.7) | 15 (45.5) | 11 (61.1) | 11 (50) | 7 (77.8) | 4 (36.4) | |||
| Age (years), mean (SD) | 45 (17.4) | 38.2 (11.9) | 0.076 ‡ | 48.1 (17.6) | 36 (10.7) | 0.011 ‡ | 38.9 (16.1) | 42.5 (13.6) | 0.597 ‡ |
| Marital status | |||||||||
| Unmarried/Divorced | 14 (51.9) | 14 (42.4) | 0.466 + | 9 (50) | 11 (50) | 1.000 + | 5 (55.6) | 3 (27.3) | 0.362 ++ |
| Married | 13 (48.1) | 19 (57.6) | 9 (50) | 11 (50) | 4 (44.4) | 8 (72.7) | |||
| Education (years) | |||||||||
| 1–9 | 3 (11.1) | 7 (21.2) | 0.510 + | 2 (11.1) | 2 (9.1) | 0.884 ++ | 1 (11.1) | 5 (45.5) | 0.326 ++ |
| 10–12 | 5 (18.5) | 7 (21.2) | 3 (16.7) | 6 (27.3) | 2 (22.2) | 1 (9.1) | |||
| >12 | 19 (70.4) | 19 (57.6) | 13 (72.2) | 14 (63.6) | 6 (66.7) | 5 (45.5) | |||
| Smoking# | |||||||||
| No | 20 (74.1) | 23 (69.7) | 0.653 + | 11 (61.1) | 15 (68.2) | 0.641 + | 9 (100) | 8 (72.7) | 0.211 ++ |
| Yes | 7 (25.9) | 10 (30.3) | 7 (38.9) | 7 (31.8) | 0 (0) | 3 (27.3) | |||
| IBD (N = 60) | P | CD (N = 40) | P | UC (N = 20) | P | ||||
|---|---|---|---|---|---|---|---|---|---|
| Placebo (27) | Mastiha (33) | Placebo (18) | Mastiha (22) | Placebo (9) | Mastiha (11) | ||||
| BMI (kg/m2) mean (SD) | 24.5 (6.6) | 23.4 (5.3) | 0.481 ‡ | 24.4 (6.1) | 22 (4.2) | 0.149 ‡ | 24.7 (7.8) | 26.2 (6.2) | 0.628 ‡ |
| Normal | 17 (63.0) | 23 (69.7) | 0.863 ++ | 11 (61.1) | 17 (77.3) | 0.292 ++ | 6 (66.7) | 6 (54.5) | 0.830 ++ |
| Overweight | 5 (18.5) | 6 (18.2) | 3 (16.7) | 4 (18.2) | 2 (22.2) | 2 (18.2) | |||
| Obese | 5 (18.5) | 4 (12.1) | 4 (22.2) | 1 (4.5) | 1 (11.1) | 3 (27.3) | |||
| Disease duration (years), mean (SD) | 13.9 (10.7) | 9.4 (7.0) | 0.061 ‡ | 14.8 (12.0) | 10.2 (6.9) | 0.131 ‡ | 12.0 (7.7) | 7.9 (7.4) | 0.240 ‡ |
| Age of first symptoms, mean (SD) | 29.6 (16.1) | 27.0 (11.9) | 0.480 ‡ | 31.2 (16.6) | 25.0 (10.3) | 0.152 ‡ | 26.4 (15.7) | 31.6 (14.2) | 0.463 ‡ |
| Age of diagnosis, mean (SD) | 32.0 (17.4) | 27.9 (11.9) | 0.290 ‡ | 34.5 (18.0) | 25.8 (10.6) | 0.065 ‡ | 26.9 (15.9) | 32.4 (13.9) | 0.431 ‡ |
| Disease extent | |||||||||
| Ileal | 9 (50.0) | 8 (36.4) | |||||||
| Ileocolonic | 7 (39.0) | 9 (40.9) | |||||||
| Colonic | 1 (5.5) | 3 (13.6) | |||||||
| Colonic and duodenum | 1 (5.5) | 0 (0.0) | |||||||
| Colonic and upper GI- | 0 (0.0) | 2 (9.1) | |||||||
| Pancolitis | 6 (66.7) | 8 (72.7) | |||||||
| Left-sided | 3 (33.3) | 2 (18.2) | |||||||
| Rectitis | 0 (0) | 1 (9.1) | |||||||
| Surgical therapy in the past | 12 (44.4) | 12 (36.4) | 0.525 + | 10 (55.5) | 10 (45.5) | 0.525 + | 2 (22.2) | 2 (18.2) | 1.000 ++ |
| Concomitant treatment | |||||||||
| None | 9 (33.3) | 12 (36.4) | 0.966 + | 7 (38.9) | 10 (45.5) | 0.783 + | 2 (22.2) | 2 (18.2) | 0.850 ++ |
| One | 10 (37.0) | 12 (36.4) | 5 (27.8) | 7 (31.8) | 5 (55.6) | 5 (45.5) | |||
| Combined | 8 (29.6) | 9 (27.3) | 6 (33.3) | 5 (22.7) | 2 (22.2) | 4 (36.4) | |||
| Medication | |||||||||
| Mesalamine | 11 (40.7) | 13 (39.4) | 0.916 + | 5 (27.8) | 4 (18.2) | 0.705 ++ | 6 (66.7) | 9 (81.8) | 0.617 ++ |
| Azathioprine | 7 (25.9) | 7 (21.2) | 0.668 + | 5 (27.8) | 4 (18.2) | 0.705 ++ | 2 (22.2) | 3 (27.3) | 1.000 ++ |
| Corticosteroids | 9 (33.3) | 14 (42.4) | 0.807 + | 7 (38.9) | 10 (45.5) | 0.676 + | 2 (22.2) | 4 (36.4) | 1.000 ++ |
| IBD (N = 60) | CD (N = 40) | UC (N = 20) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre- | Post- | Change | P1 | P2 | Pre- | Post- | Change | P1 | P2 | Pre- | Post- | Change | P1 | P2 | |
| oxLDL (U/L) | |||||||||||||||
| Placebo | 135.3 (48.38) | 135.45 (38.92) | 0.15 (52.76) | ns | ns | 122.7 (47.1) | 128.3 (43) | 5.6 (50.4) | ns | ns | 160.4 (42.8) | 149.7 (25.4) | −10.7 (58.8) | ns | ns |
| PL | 160.42 (34.26) | 140.12 (41.91) | −20.3 (51.7) | 0.031 | 159.4 (34.5) | 138.2 (44.1) | −21.2 (55.3) | ns | 162.4 (35.3) | 144 (39) | −18.4 (46) | ns | |||
| P 3 | 0.022 | ns | 0.007 | ns | ns | ns | |||||||||
| oxLDL/HDL | |||||||||||||||
| Placebo | 2.44 (1.22) | 2.63 (1.38) | 0.19 (1.67) | ns | 0.044 | 2.44 (1.2) | 2.51 (1.51) | 0.07 (1.63) | ns | ns | 2.45 (1.33) | 2.88 (1.11) | 0.43 (1.83) | ns | ns |
| PL | 3.06 (0.91) | 2.37 (1.42) | −0.69 (1.63) | 0.020 | 2.98 (0.85) | 2.45 (1.42) | −0.53 (1.46) | ns | 3.23 (1.03) | 2.2 (1.45) | −1.03 (1.96) | ns | |||
| P 3 | 0.028 | ns | ns | ns | ns | ns | |||||||||
| oxLDL/LDL | |||||||||||||||
| Placebo | 1.62 (0.88) | 1.7 (0.88) | 0.07 (0.82) | ns | 0.015 | 1.55 (0.99) | 1.79 (0.96) | 0.24 (0.73) | ns | 0.010 | 1.78 (0.63) | 1.51 (0.73) | −0.27 (0.92) | ns | ns |
| PL | 1.84 (0.73) | 1.3 (0.85) | −0.54 (1.03) | 0.005 | 1.95 (0.84) | 1.34 (0.94) | −0.61 (1.15) | 0.006 | 1.62 (0.38) | 1.23 (0.65) | −0.39 (0.76) | ns | |||
| P 3 | ns | ns | ns | ns | ns | ns | |||||||||
| Lagtime (s) | |||||||||||||||
| Placebo | 4279.8 (2573.79) | 4889.15 (2094.22) | 609.31 (2159.4) | ns | ns | 4014.1 (2335.6) | 4619.9 (1869.8) | 605.8 (2210) | ns | ns | 4811.3 (3075.8) | 5427.6 (2516.9) | 616.3 (2185.5) | ns | ns |
| PL | 4271.12 (2236.36) | 4959.46 (1760.57) | 688.34 (2327.7) | ns | 3823.2 (1763.5) | 4852.6 (1793.3) | 1029.4 (2119) | 0.031 | 5166.9 (2854.6) | 5173.2 (1757.7) | 6.3 (2672.4) | ns | |||
| P 3 | ns | ns | ns | ns | ns | ns | |||||||||
| UA (mg/dL) | |||||||||||||||
| Placebo | 4.99 (1.92) | 4.45 (1.22) | −0.54 (1.79) | ns | ns | 5.25 (2.22) | 4.39 (1.29) | −0.9 (2) | 0.037 | ns | 4.46 (1.04) | 4.58 (1.12) | 0.1 (0.9) | ns | ns |
| PL | 5.76 (4.9) | 4.64 (1.11) | −1.12 (4.82) | ns | 5.14 (1.45) | 4.58 (1.15) | −0.6 (1.4) | ns | 7.01 (8.36) | 4.76 (1.08) | −2.3 (8.3) | ns | |||
| P 3 | ns | ns | ns | ns | ns | ns | |||||||||
| Pre- | Post- | Change | P1 | P2 | |
|---|---|---|---|---|---|
| IBD (N = 60) | |||||
| Aspartic acid | |||||
| Placebo | 7 (4.1) | 6.7 (4.2) | −0.3 (6.2) | ns | ns |
| PL | 8.2 (4.5) | 5.3 (3.3) | −2.9 (6) | 0.009 | |
| P 3 | ns | ns | |||
| Cysteine ‡ | |||||
| Placebo | 27.9 (26.5; 28.8) | 27.5 (26.3; 29.6) | 0 (−2; 2.1) | ns | ns |
| PL | 27.1 (25.4; 28.5) | 28.7 (26.2; 29.5) | 1.3 (−0.7; 3.5) | 0.042 | |
| P 3 | ns | ns | |||
| Glutamic acid ‡ | |||||
| Placebo | 12.3 (5.1; 26.5) | 20.2 (9.5; 30) | 3.6 (−7.4; 15.1) | 0.039 | ns |
| PL | 18.6 (10.4; 26.6) | 25.7 (21.7; 28.2) | 4 (−3.6; 16.3) | 0.045 | |
| P 3 | ns | 0.042 | |||
| Glutamine ‡ | |||||
| Placebo | 433.9 (392.9; 461.8) | 385 (375.1; 446.4) | −34.4 (−60.4; −13.8) | ns | ns |
| PL | 368.4 (303.1; 428.4) | 385.4 (311; 413.1) | −7.4 (−53.7; −67.6) | ns | |
| P 3 | 0.011 | ns | |||
| Lysine ‡ | |||||
| Placebo | 185.3 (160.1; 222.3) | 171.3 (153.4; 177.1) | −25.8 (−58.5; −0.9) | ns | ns |
| PL | 188.1 (163.3; 220.8) | 164.3 (150.3; 172.2) | −27 (−55.8; 1.9) | ns | |
| P 3 | ns | ns | |||
| Thioproline | |||||
| Placebo | 16.7 (4.1) | 14.1 (2.3) | −2.7 (5.2) | 0.006 | ns |
| PL | 18.1 (4.2) | 13.7 (2.8) | −4.4 (4.6) | <0.001 | |
| P 3 | ns | ns | |||
| CD (N = 40) | |||||
| Cysteine ‡ | |||||
| Placebo | 28.3 (26.9; 29.3) | 27.2 (26.3; 29.3) | −0.8 (−2.2; 1.7) | ns | ns |
| PL | 27.2 (25.6; 28.5) | 27.7 (25; 29.2) | 0.2 (−1.9; 3.7) | ns | |
| P 3 | 0.050 | ns | |||
| Lysine ‡ | |||||
| Placebo | 165.3 (142.8; 218.4) | 173.4 (155; 178.2) | −9.9 (−50.1; 1.5) | ns | ns |
| PL | 192.6 (175.3; 221.6) | 160.8 (142.7; 171.4) | −30.6 (−62.2; −4) | 0.036 | |
| P 3 | ns | ns | |||
| Thioproline | |||||
| Placebo | 15.6 (3.6) | 14.4 (2.4) | −1.2 (4.9) | ns | ns |
| PL | 17.8 (4.8) | 13.4 (3.1) | −4.4 (5) | <0.001 | |
| P 3 | ns | ns | |||
| UC (N = 20) | |||||
| Alo-isoleucine ‡ | |||||
| Placebo | 58.4 (53; 68.9) | 48.7 (41.4; 55.5) | −14.4 (−15.4; −11.6) | 0.038 | 0.016 |
| PL | 45.5 (32; 52.4) | 51.8 (47.3; 55.6) | 7.9 (−4.2; 17.2) | ns | |
| P 3 | 0.007 | ns | |||
| β-Aminobutyric acid ‡ | |||||
| Placebo | 98.1 (96.8; 99.9) | 98 (97; 98.8) | −1.1 (−2.5; −0.4) | ns | ns |
| PL | 98.7 (97.3; 99.4) | 98.8 (98.1; 101.7) | 1 (−0.9; 3.8) | ns | |
| P 3 | ns | 0.022 | |||
| Aspartic acid | |||||
| Placebo | 6.4 (2.4) | 5.6 (2.5) | −0.8 (4.4) | 0.672 | ns |
| PL | 9.7 (4.6) | 5.6 (3.5) | −4.1 (5.6) | 0.016 | |
| P 3 | ns | ns | |||
| Cysteine ‡ | |||||
| Placebo | 27.7 (26.5; 27.9) | 28.8 (26.5; 29.6) | 1.2 (0.2; 2.3) | ns | ns |
| PL | 26.4 (25.1; 28.6) | 29.2 (28.1; 31.5) | 2.1 (0.8; 3.5) | <0.001 | |
| P 3 | ns | ns | |||
| Glutamic acid ‡ | |||||
| Placebo | 4.1 (2.9; 17.1) | 14.9 (9.1; 19.6) | 2.2 (−2.8; 6.6) | ns | ns |
| PL | 21.1 (10.4; 34.1) | 24.4 (21.7; 30.3) | 2.2 (−3; 19.9) | ns | |
| P 3 | ns | 0.005 | |||
| Glutamine ‡ | |||||
| Placebo | 427.2 (401.8; 456.3) | 385 (375.1; 394.7) | −37.5 (−47.9; −22.7) | ns | 0.038 |
| PL | 330.6 (255.4; 428.4) | 387.1 (311; 413.1) | 50.3 (−50.2; 129.8) | ns | |
| P 3 | 0.048 | ns | |||
| Isoleucine ‡ | |||||
| Placebo | 68.3 (61.8; 80.2) | 51.5 (49.1; 63.6) | −16.9 (−17.6; −10.4) | 0.019 | 0.009 |
| PL | 55.4 (38.1; 61.5) | 60.4 (55.2; 67.8) | 0.8 (−3.3; −24.4) | ns | |
| P 3 | 0.008 | ns | |||
| Leucine ‡ | |||||
| Placebo | 132.3 (115.2; 146.6) | 117.7 (92.3; 139.3) | −23.8 (−29.9; −7.9) | ns | 0.043 |
| PL | 102.1 (85; 123.7) | 127.8 (120.1; 137.3) | 16.1 (0.7; 42.8) | ns | |
| P 3 | ns | ns | |||
| Lysine ‡ | |||||
| Placebo | 207.2 (190.5; 222.3) | 164.1 (153.4; 174.3) | −47.5 (−69.1; −41.6) | 0.002 | 0.009 |
| PL | 163.3 (129.9; 209.9) | 166.7 (159.5; 182.8) | −0.6 (−33.4; 26.5) | ns | |
| P 3 | ns | ns | |||
| Ornithine ‡ | |||||
| Placebo | 103.5 (77.8; 125.5) | 75.2 (69.1; 82.9) | −20.8 (−50.3; −3.8) | ns | 0.036 |
| PL | 77.1 (47.1; 96.1) | 85 (68.5; 92.9) | 15.2 (−27.6; 22.4) | ns | |
| P 3 | ns | ns | |||
| Proline | |||||
| Placebo | 257.9 (55.7) | 223.6 (56.1) | −34.3 (92.2) | ns | ns |
| PL | 240.6 (90.9) | 275.7 (49.6) | 35.1 (114.8) | ns | |
| P 3 | ns | 0.041 | |||
| Serine | |||||
| Placebo | 130.4 (36.2) | 114.1 (19.8) | −16.3 (32.8) | ns | 0.028 |
| PL | 94.8 (28.1) | 108.3 (15.3) | 13.5 (23) | ns | |
| P 3 | 0.023 | ns | |||
| Thioproline | |||||
| Placebo | 19.1 (4.4) | 13.3 (1.8) | −5.8 (4.8) | 0.001 | 0.047 |
| PL | 18.7 (2.7) | 14.1 (2.1) | −4.6 (4) | 0.003 | |
| P 3 | ns | ns | |||
| Tryptophane | |||||
| Placebo | 65.3 (12.3) | 57 (12.8) | −8.3 (12) | 0.050 | 0.037 |
| PL | 55.1 (13.9) | 58.8 (9) | 3.7 (11.7) | ns | |
| P 3 | ns | ns | |||
| Tyrosine | |||||
| Placebo | 71 (18.4) | 58.1 (17.2) | −12.9 (17.3) | 0.045 | 0.005 |
| PL | 50.4 (18.6) | 63.3 (11.9) | 12.9 (18.6) | 0.029 | |
| P 3 | 0.023 | ns | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papada, E.; Forbes, A.; Amerikanou, C.; Torović, L.; Kalogeropoulos, N.; Tzavara, C.; Triantafillidis, J.K.; Kaliora, A.C. Antioxidative Efficacy of a Pistacia Lentiscus Supplement and Its Effect on the Plasma Amino Acid Profile in Inflammatory Bowel Disease: A Randomised, Double-Blind, Placebo-Controlled Trial. Nutrients 2018, 10, 1779. https://doi.org/10.3390/nu10111779
Papada E, Forbes A, Amerikanou C, Torović L, Kalogeropoulos N, Tzavara C, Triantafillidis JK, Kaliora AC. Antioxidative Efficacy of a Pistacia Lentiscus Supplement and Its Effect on the Plasma Amino Acid Profile in Inflammatory Bowel Disease: A Randomised, Double-Blind, Placebo-Controlled Trial. Nutrients. 2018; 10(11):1779. https://doi.org/10.3390/nu10111779
Chicago/Turabian StylePapada, Efstathia, Alastair Forbes, Charalampia Amerikanou, Ljilja Torović, Nick Kalogeropoulos, Chara Tzavara, John K. Triantafillidis, and Andriana C. Kaliora. 2018. "Antioxidative Efficacy of a Pistacia Lentiscus Supplement and Its Effect on the Plasma Amino Acid Profile in Inflammatory Bowel Disease: A Randomised, Double-Blind, Placebo-Controlled Trial" Nutrients 10, no. 11: 1779. https://doi.org/10.3390/nu10111779