Milk Other Than Breast Milk and the Development of Asthma in Children 3 Years of Age. A Birth Cohort Study (2006–2011)

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. The Environments for Healthy Living Study
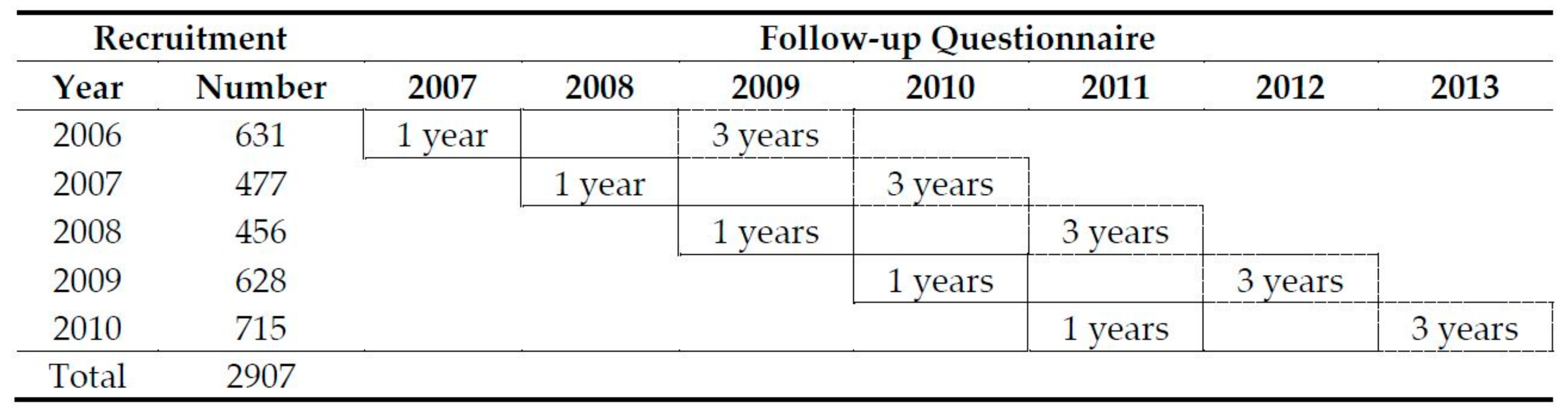
2.2. Study Population
2.3. Study Variables
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Cohort
3.2. Association between Developing Persistent Asthma and MOTBM and Other Covariates
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Asthma Australia, Statistics: People and Asthma. Available online: https://www.asthmaaustralia.org.au/national/about-asthma/ (accessed on 4 May 2018).
- World Health Organization. Media Centre: Asthma. 2018. Available online: http://www.who.int/respiratory/asthma/en/ (accessed on 4 February 2018).
- Australian Centre for Asthma Monitoring. Asthma in Australian Children: Findings from Growing Up in Australia, the Longitudinal Study of Australian Children; Cat. no. ACM 17; AIHW: Canberra, Australia, 2009. [Google Scholar]
- Oddy, W.H. Breastfeeding, Childhood Asthma, and Allergic Disease. Ann. Nutr. Metab. 2017, 70 (Suppl. 2), 26–36. [Google Scholar] [CrossRef] [PubMed]
- Brooks, C.; Pearce, N.; Douwes, J. The hygiene hypothesis in allergy and asthma: An update. Curr. Opin. Allergy Clin. Immunol. 2013, 13, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, E.G. Urbanization and childhood asthma: An African perspective. J. Allergy Clin. Immunol. 2000, 105 (Pt 1), 224–231. [Google Scholar] [CrossRef]
- Miliku, K.; Azad, M. Breastfeeding and the Developmental Origins of Asthma: Current Evidence, Possible Mechanisms, and Future Research Priorities. Nutrients 2018, 10, 995. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, A.; Asero, R. Asthma and autoimmunity: A complex but intriguing relation. Expert Rev. Clin. Immunol. 2008, 4, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Goksör, E.; Gustafsson, P.M.; Alm, B.; Åmark, M.; Wennergren, G. Reduced airway function in early adulthood among subjects with wheezing disorder before two years of age. Pediatr. Pulmonol. 2008, 43, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Piippo-Savolainen, E.; Korppi, M. Wheezy babies—Wheezy adults? Review on long-term outcome until adulthood after early childhood wheezing. Acta Paediatr. 2008, 97, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Azad, M.B.; Vehling, L.; Lu, Z.; Dai, D.; Subbarao, P.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; et al. Breastfeeding, maternal asthma and wheezing in the first year of life: A longitudinal birth cohort study. Eur. Respir. J. 2017, 49, 1602019. [Google Scholar] [CrossRef] [PubMed]
- Xiaoqin, L.; Agerbo, E.; Schlünssen, V.; Wright, R.J.; Li, J.; Trine Munk-Olsen, T.M. Maternal asthma severity and control during pregnancy and risk of offspring asthma. J. Allergy Clin. Immunol. 2018, 141, 886–892.e3. [Google Scholar] [CrossRef]
- Sherriff, A.; Peters, T.J.; Henderson, J.; Strachan, D. Risk factor associations with wheezing patterns in children followed longitudinally from birth to 3 1/2 years. Int. J. Epidemiol. 2001, 30, 1473–1484. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.M.; Ruiz, M.; Goldblatt, P.; Morrison, J.; Porta, D.; Forastiere, F.; Hryhorczuk, D.; Zvinchuk, O.; Saurel-Cubizolles, M.J.; Lioret, S.; et al. Mother’s education and offspring asthma risk in 10 European cohort studies. Eur. J. Epidemiol. 2017, 32, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Brock, C.; McGuane, J. Determinants of asthma in Indigenous Australians: Insights from epidemiology. Aust. Indig. Health 2018, 18, 2. [Google Scholar]
- Strong, C.; Chang, L.Y. Family socioeconomic status, household tobacco smoke, and asthma attack among children below 12 years of age: Gender differences. J. Child Health Care 2014, 18, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Marfortt, D.A.; Josviack, D.; Lozano, A.; Cuestas, E.; Agüero, L.; Castro-Rodriguez, J.A. Differences between preschoolers with asthma and allergies in urban and rural environments. J. Asthma 2018, 55, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Metsälä, J.; Kilkkinen, A.; Kaila, M.; Tapanainen, H.; Klaukka, T.; Gissler, M.; Virtanen, S.M. Perinatal factors and the risk of asthma in childhood—A population-based register study in Finland. Am. J. Epidemiol. 2008, 168, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.Y.Y.; Li, A.M.; Leung, G.M.; Schooling, C.M. Mode of delivery and childhood hospitalizations for asthma and other wheezing disorders. Clin. Exp. Allergy 2015, 45, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Been, J.V.; Lugtenberg, M.J.; Smets, E.; van Schayck, C.P.; Kramer, B.W.; Mommers, M.; Sheikh, A. Preterm Birth and Childhood Wheezing Disorders: A Systematic Review and Meta-Analysis. PLoS Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Mu, M.; Ye, S.; Bai, M.J.; Liu, G.L.; Tong, Y.; Wang, S.F.; Sheng, J. Birth weight and subsequent risk of asthma: A systematic review and meta-analysis. Heart Lung Circ. 2014, 23, 511–519. [Google Scholar] [CrossRef] [PubMed]
- von Kobyletzki, L.B.; Bornehag, C.-G.; Hasselgren, M.; Larsson, M.; Lindström, C.B.; Svensson, Å. Eczema in early childhood is strongly associated with the development of asthma and rhinitis in a prospective cohort. BMC Dermatol. 2012, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Caffarelli, C.; Garrubba, M.; Greco, C.; Mastrorilli, C.; Povesi Dascola, C. Asthma and Food Allergy in Children: Is There a Connection or Interaction? Front. Pediatr. 2016, 4, 34. [Google Scholar] [CrossRef] [PubMed]
- Verduci, E.; Martelli, A.; Miniello, V.L.; Landi, M.; Mariani, B.; Brambilla, M.; Diaferio, L.; Peroni, D.G. Nutrition in the first 1000 days and respiratory health: A descriptive review of the last five years’ literature. Allergol. Immunopathol. 2017, 45, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, J.; Tanaka, K.; Nagata, C.; Furukawa, S.; Arakawa, M.; Miyake, Y. Breastfeeding duration is inversely associated with asthma in Japanese children aged 3 years. J. Asthma 2018, 55, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Liu, W.; Cai, J.; Weschler, L.B.; Wang, X.; Hu, Y.; Zou, Z.; Shen, L.; Sundell, J. Breastfeeding and timing of first dietary introduction in relation to childhood asthma, allergies, and airway diseases: A cross-sectional study. J. Asthma 2017, 54, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Abarca, N.E.; Garro, A.C.; Pearlman, D.N. Relationship between breastfeeding and asthma prevalence in young children exposed to adverse childhood experiences. J. Asthma 2018, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nasser, A.; Omer, F.; Al-Lenqawi, F.; Al-Awwa, R.; Khan, T.; El-Heneidy, A.; Kurdi, R.; Al-Jayyousi, G. Predictors of continued breastfeeding at one year among women attending primary healthcare centers in Qatar: A cross-sectional study. Nutrients 2018, 10, 983. [Google Scholar] [CrossRef] [PubMed]
- Ram, F.S.F.; Scarlett, J.F. Development of childhood asthma and formula milk. Br. J. Midwifery 2004, 12, 221–229. [Google Scholar] [CrossRef]
- Boyle, R.J.; Ierodiakonou, D.; Khan, T.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Afxentiou, T.; Reeves, T.; Cunha, S.; et al. Hydrolysed formula and risk of allergic or autoimmune disease: Systematic review and meta-analysis. BMJ 2016, 352, i974. [Google Scholar] [CrossRef] [PubMed]
- Klopp, A.; Vehling, L.; Becker, A.B.; Subbarao, P.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; Azad, M.B.; CHILD Study Investigators. Modes of Infant Feeding and the Risk of Childhood Asthma: A Prospective Birth Cohort Study. J. Pediatr. 2017, 190, 192–199.e2. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Horvath, A. Meta-analysis of the evidence for a partially hydrolyzed 100% whey formula for the prevention of allergic diseases. Curr. Med. Res. Opin. 2010, 26, 423–437. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.; Roberts, G.; Kurukulaaratchy, R.J.; Matthews, S.; Nove, A.; Arshad, S.H. Multifaceted allergen avoidance during infancy reduces asthma during childhood with the effect persisting until age 18 years. Thorax 2012, 67, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.M.; Scuffham, P.A.; Spinks, A.; Scott, R.; Sipe, N.; Ng, S.K.; Wilson, A.; Searle, J.; Lyons, R.A.; Kendall, E.; et al. Environments for Healthy Living (EFHL) Griffith birth cohort study: Background and methods. Matern. Child Health J. 2012, 16, 1896–1905. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.M.; Scuffham, P.A.; Shibl, R.; Ng, S.; Scott, R.; Spinks, A.; Mihala, G.; Wilson, A.; Kendall, E.; Sipe, N.; et al. Environments for Healthy Living (EFHL) Griffith birth cohort study: Characteristics of sample and profile of antenatal exposures. BMC Public Health 2012, 12, 1080. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemeshow, S.S.R. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013; ISBN 978-0-470-58247-3. [Google Scholar]
- Lemeshow, S.; Moeschberger, M.L. Review of Regression Methods in Biostatistics: Linear, Logistic, Survival, and Repeated Measures Models; Vittinghoff, E., Glidden, D.V., Shiboski, S.C., McCulloch, C.E., Eds.; Springer: New York, NY, USA, 2005. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S. Goodness of fit tests for the multiple logistic regression model. Commun. Stat. Theory Methods 1980, 9, 1043–1069. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software; StataCorp LP: College Station, TX, USA, 2017. [Google Scholar]
- Martin, C.; Ling, P.-R.; Blackburn, G. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [PubMed]
- Von Berg, A.; Filipiak-Pittroff, B.; Krämer, U.; Link, E.; Bollrath, C.; Brockow, I.; Koletzko, S.; Grübl, A.; Heinrich, J.; Wichmann, H.E.; et al. Preventive effect of hydrolyzed infant formulas persists until age 6 years: Long-term results from the German Infant Nutritional Intervention Study (GINI). J. Allergy Clin. Immunol. 2008, 121, 1442–1447. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.A.; Sinn, J.K.H.; Jones, L.J. Infant formulas containing hydrolysed protein for prevention of allergic disease and food allergy. Cochrane Database Syst. Rev. 2017, 15, CD003664. [Google Scholar] [CrossRef]
- Cabana, M.D. The Role of Hydrolyzed Formula in Allergy Prevention. Ann. Nutr. Metab. 2017, 70 (Suppl. 2), 38–45. [Google Scholar] [CrossRef] [PubMed]
- Verduci, E.; Banderali, G.; Peroni, D.; Lassandro, C.; Radaelli, G. Duration of exclusive breastfeeding and wheezing in the first year of life: A longitudinal study. Allergol. Immunopathol. 2017, 45, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Arif, A.A.; Racine, E.F. Does longer duration of breastfeeding prevent childhood asthma in low-income families? J. Asthma 2017, 54, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Jelding-Dannemand, E.; Malby Schoos, A.M.; Bisgaard, H. Breast-feeding does not protect against allergic sensitization in early childhood and allergy-associated disease at age 7 years. J. Allergy Clin. Immunol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Ek, W.E.; Karlsson, T.; Hernándes, C.A.; Rask-Andersen, M.; Johansson, Å. Breast-feeding and risk of asthma, hay fever, and eczema. J. Allergy Clin. Immunol. 2018, 141, 1157–1159.e9. [Google Scholar] [CrossRef] [PubMed]
- Subbarao, P.; Mandhane, P.J.; Sears, M.R. Asthma: Epidemiology, etiology and risk factors. CMAJ 2009, 181, E181–E190. [Google Scholar] [CrossRef] [PubMed]
- Le Souef, P.N.; Sears, M.R.; Sherrill, D. The Effect of Size and Age of Subject on Airway Responsiveness in Children. Am. J. Respir. Crit. Care Med. 1995, 152, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Mandhane, P.J.; Greene, J.M.; Cowan, J.O.; Taylor, D.R.; Sears, M.R. Sex differences in factors associated with childhood- and adolescent-onset wheeze. Am. J. Respir. Crit. Care Med. 2005, 172, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Terry, D.; Robins, S.; Gardiner, S.; Wyett, R.; Islam, M.R. Asthma hospitalisation trends from 2010 to 2015: Variation among rural and metropolitan Australians. BMC Public Health 2017, 17, 723. [Google Scholar] [CrossRef] [PubMed]
- Demehri, S.; Morimoto, M.; Holtzman, M.J.; Kopan, R. Skin-derived TSLP triggers progression from epidermal-barrier defects to asthma. PLoS Biol. 2009. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.A.; Lowe, A.J.; Matheson, M.C.; Varigos, G.; Abramson, M.J.; Dharmage, S.C. Does eczema lead to asthma? J. Asthma 2009, 46, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.A.; Dharmage, S.C.; Byrnes, G.B.; Matheson, M.C.; Gurrin, L.C.; Wharton, C.L.; Johns, D.P.; Abramson, M.J.; Hopper, J.L.; Walters, E.H. Childhood eczema and asthma incidence and persistence: A cohort study from childhood to middle age. J. Allergy Clin. Immunol. 2008, 122, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Dezateux, C.; Stocks, J.; Dundas, I.; Fletcher, M.E. Impaired airway function and wheezing in infancy: The influence of maternal smoking and a genetic predisposition to asthma. Am. J. Respir. Crit. Care Med. 1999, 159, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Tariq, S.M.; Hakim, E.A.; Matthews, S.M.; Arshad, S.H. Influence of smoking on asthmatic symptoms and allergen sensitisation in early childhood. Postgrad. Med. J. 2000, 76, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Lodrup, C.K. The Environment and Childhood Asthma (ECA) Study in Oslo: ECA-1 and ECA-2. Pediatr. Allergy Immunol. 2002, 13 (Suppl. 15), 29–31. [Google Scholar] [CrossRef]
- Hwang, S.-H.; Hwang, J.H.; Moon, J.S.; Lee, D.-H. Environmental tobacco smoke and children’s health. Korean J. Pediatr. 2012, 55, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Kim, K.W.; Choi, B.S.; Jee, H.M.; Sohn, M.H.; Kim, K.E. Relationship between mode of delivery in childbirth and prevalence of allergic diseases in Korean children. Allergy Asthma Immunol. Res. 2010, 2, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Sevelsted, A.; Stokholm, J.; Bisgaard, H. Risk of Asthma from Cesarean Delivery Depends on Membrane Rupture. J. Pediatr. 2016, 171, 38–42.e4. [Google Scholar] [CrossRef] [PubMed]
- Prickett, K.C.; Augustine, J.M. Maternal Education and Investments in Children’s Health. J. Marriage Fam. 2016, 78, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Berti, P.R.; Mildon, A.; Siekmans, K.; Main, B.; MacDonald, C. An adequacy evaluation of a 10-year, four-country nutrition and health programme. Int. J. Epidemiol. 2010, 39, 613–629. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Persistent Asthma | Total | ||
|---|---|---|---|---|
| % | No. | % | ||
| Total | 100.0 | 76 | 6.8 | 1121 |
| MOTBM introduced at <6 months | ||||
| No | 49.0 | 26 | 4.7 | 549 |
| Yes | 51.0 | 50 | 8.7 | 572 |
| Stopped breastfeeding at <6 months | ||||
| No | 39.5 | 28 | 6.3 | 443 |
| Yes | 60.5 | 48 | 7.1 | 678 |
| Gender | ||||
| Male | 47.8 | 56 | 10.4 | 536 |
| Female | 51.7 | 20 | 3.4 | 580 |
| Delivered by caesarean section 1 | ||||
| No | 68.4 | 49 | 7.7 | 767 |
| Yes | 31.2 | 27 | 6.4 | 350 |
| Low birth weight (Weight < 2500 g) | ||||
| No | 97.9 | 75 | 6.8 | 1098 |
| Yes | 2.1 | 1 | 4.3 | 23 |
| Preterm delivery (Gestational age < 37 weeks) | ||||
| No | 97.7 | 73 | 6.7 | 1095 |
| Yes | 2.3 | 3 | 11.5 | 26 |
| Frequency exposed to cigarettes smoke 1 | ||||
| Sometimes | 6.3 | 8 | 11.3 | 71 |
| Not at all | 93.6 | 68 | 6.5 | 1049 |
| Ever been diagnosed with eczema | ||||
| No | 89.9 | 61 | 6.1 | 1008 |
| Yes | 10.1 | 15 | 13.3 | 113 |
| Even been diagnosed with food allergy | ||||
| No | 95.7 | 71 | 6.6 | 1073 |
| Yes | 4.3 | 5 | 10.4 | 48 |
| Total | Persistent Asthma | Total | ||
|---|---|---|---|---|
| % | No. | % | No. | |
| Age in years | ||||
| 16–25 | 17.9 | 22 | 10.9 | 201 |
| 26–30 | 30.9 | 19 | 5.5 | 346 |
| 31–35 | 31.1 | 26 | 7.4 | 349 |
| 36–45 | 20.1 | 9 | 4.0 | 225 |
| Highest level of education 1 | ||||
| Did not complete high school | 14.4 | 12 | 7.5 | 161 |
| Completed high school | 29.6 | 28 | 8.4 | 332 |
| TAFE/trade or apprenticeship | 30.8 | 27 | 7.8 | 345 |
| University degree | 24.8 | 8 | 2.9 | 278 |
| Place of birth | ||||
| Elsewhere | 27.8 | 18 | 5.8 | 312 |
| Australia | 72.2 | 58 | 7.2 | 809 |
| Indigenous status 2 | ||||
| Aboriginal/TSI | 1.4 | 0 | 0.0 | 16 |
| Otherwise | 96.5 | 75 | 6.9 | 1082 |
| Average number of cigarettes smoked each day during pregnancy 1 | ||||
| 0 | 89.2 | 62 | 6.2 | 1000 |
| ≤10 | 5.4 | 4 | 6.6 | 61 |
| >10 | 4.7 | 10 | 18.9 | 53 |
| Treatment for asthma during pregnancy (n = 864) 3 | ||||
| No | 75.4 | 66 | 7.9 | 839 |
| Yes | 2.2 | 4 | 16 | 25 |
| Univariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| RR [95% CI] | p-Value 1 | ARR [95% CI] | p-Value 2 | |
| MOTBM introduced at <6 months | 0.009 | |||
| No | 1.00 | 1.00 | ||
| Yes | 1.93 [1.18, 3.14] | 1.71 [1.03, 2.83] | 0.038 | |
| Stopped breastfeeding at <6 months | 0.621 | |||
| No | 1.00 | |||
| Yes | 1.13 [0.70, 1.83] | |||
| Gender | <0.001 | |||
| Male | 1.00 | 1.00 | ||
| Female | 0.31 [0.18, 0.52] | 0.31 [0.18, 0.53] | 0.000 | |
| Delivered by caesarean section | 0.415 | |||
| No | 1.00 | |||
| Yes | 1.22 [0.75, 1.99] | |||
| Low birth weight (Weight < 2500 g) | 0.642 | |||
| No | 1.00 | |||
| Yes | 0.62 [0.08, 4.66] | |||
| Preterm delivery (Gestational age < 37 weeks) | 0.336 | |||
| No | 1.00 | |||
| Yes | 1.83 [0.54, 6.22] | |||
| Frequency exposed to cigarettes smoke | 0.126 | |||
| Sometimes | 1.00 | |||
| Not at all | 0.55 [0.25, 1.19] | |||
| Ever been diagnosed with eczema | 0.005 | |||
| No | 1.00 | 1.00 | ||
| Yes | 2.38 [1.30, 4.34] | 2.15 [1.15, 4.04] | 0.017 | |
| Even been diagnosed with food allergy | 0.310 | |||
| No | 1.00 | |||
| Yes | 1.64 [0.63, 4.27] | |||
| Age in years | 0.028 | |||
| 16–25 | 1.00 | 1.00 | ||
| 26–30 | 0.47 [0.25, 0.90] | 0.47 [0.24, 0.92] | 0.028 | |
| 31–35 | 0.65 [0.36, 1.19] | 0.67 [0.36, 1.25] | 0.206 | |
| 36–45 | 0.34 [0.15, 0.75] | 0.33 [0.15, 0.75] | 0.009 | |
| Highest level of education | 0.015 | |||
| Did not complete high school | 1.00 | |||
| Completed high school | 1.14 [0.57, 2.31] | |||
| TAFE/trade or apprenticeship | 1.05 [0.52, 2.14] | |||
| University degree | 0.37 [0.15, 0.92] | |||
| Place of birth | 0.404 | |||
| Elsewhere | 1.00 | |||
| Australia | 1.26 [0.73, 2.18] | |||
| Average number of cigarettes smoked each day during pregnancy | 0.001 3 | <0.001 3 | ||
| 0 | 1.00 | 1.00 | ||
| ≤10 | 1.06 [0.37, 3.02] | 0.89 [0.30, 2.61] | 0.831 | |
| >10 | 3.52 [1.69, 7.33] | 4.23 [1.91, 9.37] | <0.001 | |
| Treatment for asthma during pregnancy (n = 864) 4 | 0.004 | - | - | |
| No | 1.00 | - | - | |
| Yes | 2.23 [0.74, 6.69] | - | - | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Heneidy, A.; Abdel-Rahman, M.E.; Mihala, G.; Ross, L.J.; Comans, T.A. Milk Other Than Breast Milk and the Development of Asthma in Children 3 Years of Age. A Birth Cohort Study (2006–2011). Nutrients 2018, 10, 1798. https://doi.org/10.3390/nu10111798
El-Heneidy A, Abdel-Rahman ME, Mihala G, Ross LJ, Comans TA. Milk Other Than Breast Milk and the Development of Asthma in Children 3 Years of Age. A Birth Cohort Study (2006–2011). Nutrients. 2018; 10(11):1798. https://doi.org/10.3390/nu10111798
Chicago/Turabian StyleEl-Heneidy, Asmaa, Manar E. Abdel-Rahman, Gabor Mihala, Lynda J. Ross, and Tracy A. Comans. 2018. "Milk Other Than Breast Milk and the Development of Asthma in Children 3 Years of Age. A Birth Cohort Study (2006–2011)" Nutrients 10, no. 11: 1798. https://doi.org/10.3390/nu10111798
APA StyleEl-Heneidy, A., Abdel-Rahman, M. E., Mihala, G., Ross, L. J., & Comans, T. A. (2018). Milk Other Than Breast Milk and the Development of Asthma in Children 3 Years of Age. A Birth Cohort Study (2006–2011). Nutrients, 10(11), 1798. https://doi.org/10.3390/nu10111798