Active Image-Assisted Food Records in Comparison to Regular Food Records: A Validation Study against Doubly Labeled Water in 12-Month-Old Infants



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Anthropometry
2.3. Doubly Labeled Water
2.4. Water Isotope Analysis
2.5. Food Record and Dietary Assessment
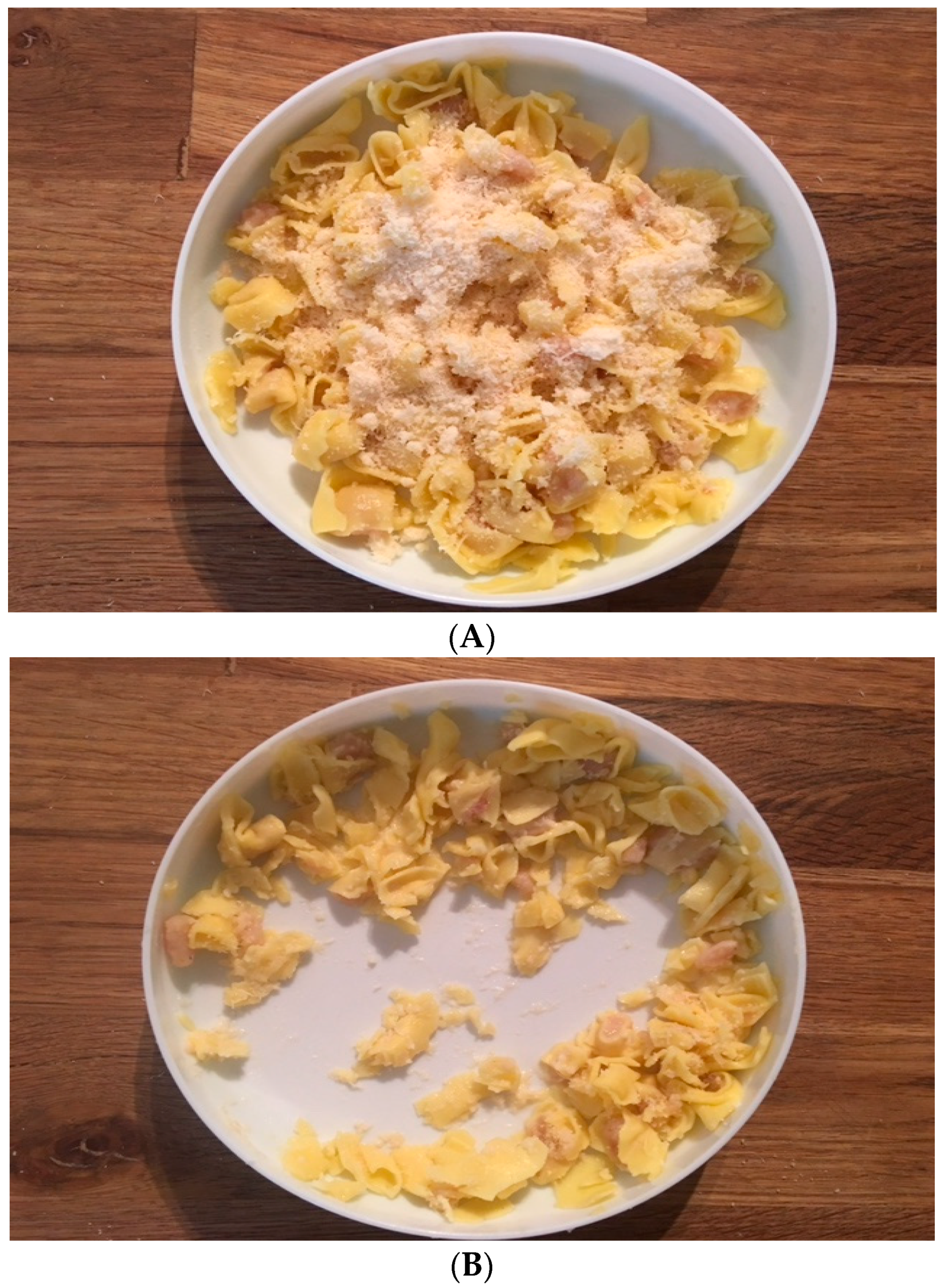
2.6. Food Record with an Active Image-Assisted Method
2.7. Pilot Testing
2.8. Group Size Calculation
2.9. Ethical Considerations
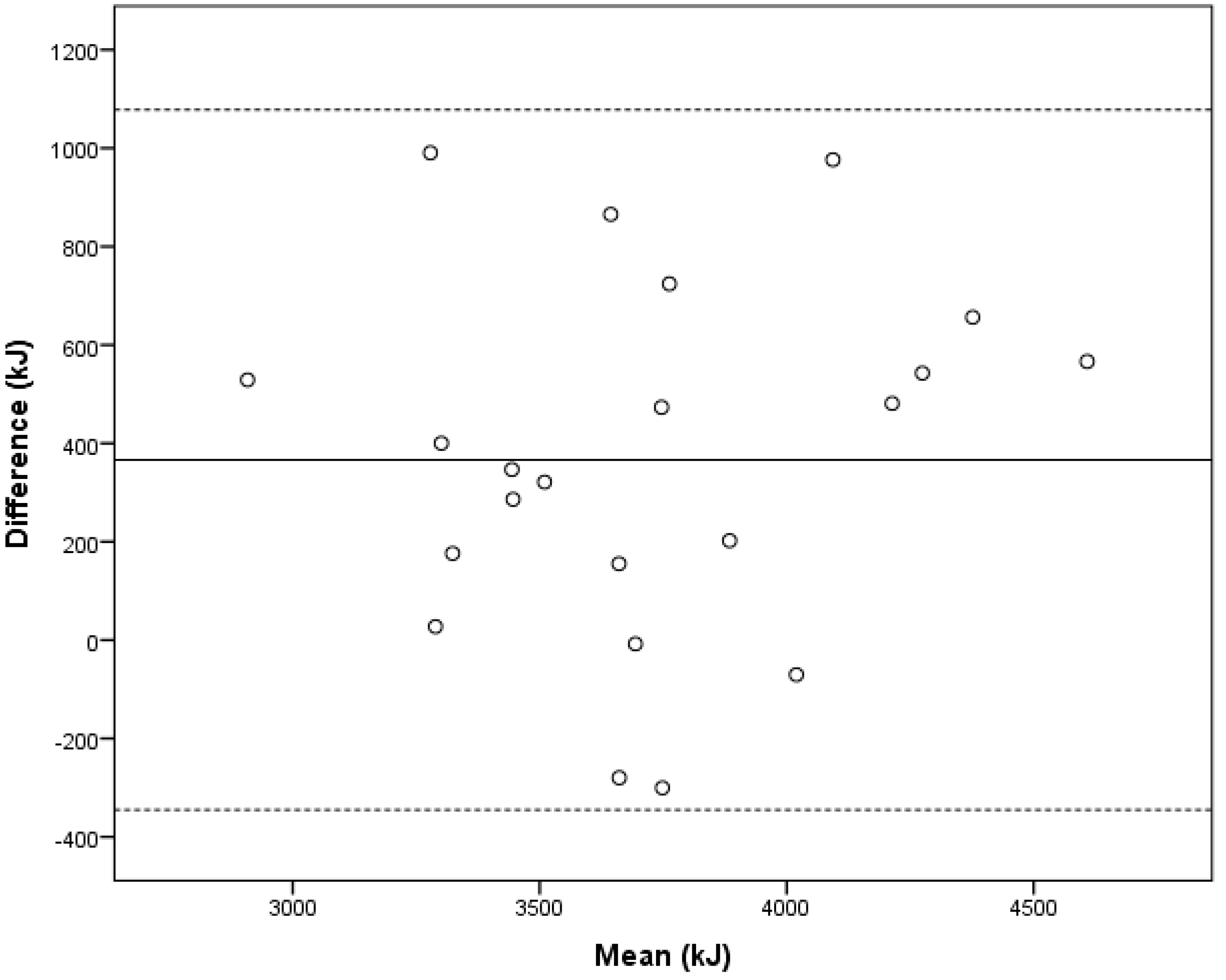
2.10. Statistical Analyses
3. Results
3.1. Energy and Macronutrient Intake
3.2. Main Course Meals with an Active Image-Assisted Method
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
| FR | Food record |
| DLW | Doubly labeled water |
| EI | Energy intake |
| ICC | Intra-class correlation coefficient |
| ME | Metabolizable energy |
| SD | Standard deviation |
| TEE | Total energy expenditure |
| OTIS | Optimized complementary feeding study |
References
- Burrows, T.L.; Martin, R.J.; Collins, C.E. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labeled water. J. Am. Diet. Assoc. 2010, 110, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Lanigan, J.A.; Wells, J.C.K.; Lawson, M.S.; Cole, T.J.; Lucas, A. Number of days needed to assess energy and nutrient intake in infants and young children between 6 months and 2 years of age. Eur. J. Clin. Nutr. 2004, 58, 745–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, L.A.; Kersting, M.; de Henauw, S.; González-Gross, M.; Sichert-Hellert, W.; Matthys, C.; Mesana, M.I.; Ross, N. How to measure dietary intake and food habits in adolescence: The European perspective. Int. J. Obes. 2005, 29, 66–77. [Google Scholar] [CrossRef]
- Lanigan, J.A.; Wells, J.C.K.; Lawson, M.S.; Lucas, A. Validation of food diary method for assessment of dietary energy and macronutrient intake in infants and children aged 6–24 months. Eur. J. Clin. Nutr. 2001, 55, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, K.; Zhang, L.; Huang, L.; Tao, Y. Validity and practicability of smartphone-based photographic food records for estimating energy and nutrient intake. Asia Pac. J. Clin. Nutr. 2017, 26, 396–401. [Google Scholar] [PubMed]
- Tennefors, C.; Coward, W.A.; Hernell, O.; Wright, A.; Forsum, E. Total energy expenditure and physical activity level in healthy young Swedish children 9 or 14 months of age. Eur. J. Clin. Nutr. 2003, 57, 647–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buday, R.; Tapia, R.; Maze, G.R. Technology-driven dietary assessment: A software developer’s perspective. J. Hum. Nutr. Diet. 2014, 27, 10–17. [Google Scholar] [CrossRef]
- Boushey, C.; Kerr, D.; Wright, J.; Lutes, K.; Ebert, D.; Delp, E. Use of technology in children’s dietary assessment. Eur. J. Clin. Nutr. 2009, 63, 50–57. [Google Scholar] [CrossRef]
- Boushey, C.J.; Spoden, M.; Zhu, F.M.; Delp, E.J.; Kerr, D.A. New mobile methods for dietary assessment: Review of image-assisted and image-based dietary assessment methods. Proc. Nutr. Soc. 2016, 76, 283–294. [Google Scholar] [CrossRef]
- Svensson, Å.; Waling, M.; Bäcklund, C.; Larsson, C. Overweight and obese children’s ability to report energy intake using digital camera food records during a 2-year study. J. Nutr. Metab. 2012, 2012, 247389. [Google Scholar] [CrossRef]
- Delisle Nyström, C.; Forsum, E.; Henriksson, H.; Trolle-Lagerros, Y.; Larsson, C.; Maddison, R.; Timpka, T.; Löf, M. A mobile phone based method to assess energy and food intake in young children: A validation study against the doubly labelled water method and 24 h dietary recalls. Nutrients 2016, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Rollo, M.E.; Williams, R.L.; Burrows, T.; Kirkpatrick, S.I.; Bucher, T.; Collins, C.E. What are they really eating? A review on new approaches to dietary intake assessment and validation. Curr. Nutr. Rep. 2016, 5, 307–314. [Google Scholar] [CrossRef]
- National Food Administration. Good Foods for Infants Under One Year; Sweden Food Agency: Uppsala, Sweden, 2011. [Google Scholar]
- Lohman, T.G.; Hingle, M.; Going, S.B. Body composition in children. Pediatr. Exerc. Sci. 2013, 25, 573–590. [Google Scholar] [CrossRef]
- Roether, W. Water-CO2 exchange set-up for the routine 18oxygen assay of natural waters. Int. J. Appl. Radiat. Isot. 1970, 21, 379–387. [Google Scholar] [CrossRef]
- Craig, H. Isotopic standards for carbon and oxygen and correction factors for mass-spectrometric analysis of carbon dioxide. Geochim. Cosmochim. Acta 1957, 12, 133–149. [Google Scholar] [CrossRef]
- Schoeller, D.A.; Ravussin, E.; Schutz, Y.; Acheson, K.J.; Baertschi, P.; Jequier, E. Energy expenditure by doubly labeled water: Validation in humans and proposed calculation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1986, 250, 823–830. [Google Scholar] [CrossRef]
- Elia, M.; Livesey, G. Theory and validity of indirect calorimetry during net lipid synthesis. Am. J. Clin. Nutr. 1988, 47, 591–607. [Google Scholar] [CrossRef] [Green Version]
- Jéquier, E.; Acheson, K.J.; Schutz, Y. Assessment of energy expenditure and fuel utilization in man. Annu. Rev. Nutr. 1987, 7, 187–208. [Google Scholar] [CrossRef]
- Wells, J.C.; Davies, P.S. Estimation of the energy cost of physical activity in infancy. Arch. Dis. Child. 1998, 78, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Paul, A.A.; Black, A.E.; Evans, J.; Cole, T.J.; Whitehead, R.G. Breastmilk intake and growth in infants from two to ten months. J. Hum. Nutr. Diet. 1988, 1, 437–450. [Google Scholar] [CrossRef]
- Michaelsen, K.M.; Skafte, L.; Badsberg, J.H.; Jorgensen, M. Variation in Macronutrients in Human Bank Milk: Influencing Factors and Implications for Human Milk Banking. J. Pediatr. Gastroenterol. Nutr. 1990, 11, 229–239. [Google Scholar] [CrossRef] [PubMed]
- National Food Administration. Available online: https://slv.se (accessed on 1 January 2017).
- Gemming, L.; Utter, J.; Ni Mhurchu, C. Image-assisted dietary assessment: A systematic review of the evidence. J. Acad. Nutr. Diet. 2015, 115, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.K.; Kaya, S.; Gunturk, B.K. Quantification of food intake using food image analysis. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2009, 2009, 6869–6872. [Google Scholar] [PubMed]
- Stumbo, P.J. New technology in dietary assessment: A review of digital methods in improving food record accuracy. Proc. Nutr. Soc. 2013, 72, 70–76. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Söderberg, L.; Lind, T.; Karlsland Åkeson, P.; Sandström, A.-K.; Hernell, O.; Öhlund, I. A validation study of an interviewer-administered short food frequency questionnaire in assessing dietary vitamin D and calcium intake in Swedish children. Nutrients 2017, 9, 682. [Google Scholar] [CrossRef] [PubMed]
- Öhlund, I.; Lind, T.; Hörnell, A.; Hernell, O. Predictors of iron status in well-nourished 4-y-old children. Am. J. Clin. Nutr. 2008, 87, 839–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öhlund, I.; Hernell, O.; Hörnell, A.; Stenlund, H.; Lind, T. BMI at 4 years of age is associated with previous and current protein intake and with paternal BMI. Eur. J. Clin. Nutr. 2010, 64, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Huysentruyt, K.; Laire, D.; Avondt, T.V.; Schepper, J.D.; Vandenplas, Y. Energy and macronutrient intakes and adherence to dietary guidelines of infants and toddlers in Belgium. Eur. J. Nutr. 2016, 55, 1595–1604. [Google Scholar] [CrossRef] [PubMed]
- Grote, V.; Verduci, E.; Scaglioni, S.; Vecchi, F.; Contarini, G.; Giovannini, M.; Koletzko, B.; Agostoni, C. Breast milk composition and infant nutrient intakes during the first 12 months of life. Eur. J. Clin. Nutr. 2015, 70, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymlek-Gay, E.A.; Domellöf, M.; Hernell, O.; Hurrell, R.F.; Lind, T.; Lönnerdal, B.; Zeder, C.; Egli, I.M. Mode of oral iron administration and the amount of iron habitually consumed do not affect iron absorption, systemic iron utilisation or zinc absorption in iron-sufficient infants: A randomised trial. Br. J. Nutr. 2016, 116, 1046–1060. [Google Scholar] [CrossRef] [PubMed]
- Sharp, D.B.; Allman-Farinelli, M. Feasibility and validity of mobile phones to assess dietary intake. Nutrition 2014, 30, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, A.S.; Hörnell, A.; Hedelin, M.; Waling, M.; Gunnarsdottir, I.; Olsson, C. Development and validation of a photographic method to use for dietary assessment in school settings. PLoS ONE 2016, 11, e0163970. [Google Scholar] [CrossRef] [PubMed]
- Fatehah, A.A.; Poh, B.K.; Shanita, S.N.; Wong, J.E. Feasibility of reviewing digital food images for dietary assessment among nutrition professionals. Nutrients 2018, 10, 984. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean ± SD | |
| Age infants (months) | 11.9 ± 0.34 |
| Body weight (kg) | 10.5 ± 1.2 |
| Body length (cm) | 76.9 ± 3.1 |
| Head circumference (cm) | 47.1 ± 0.9 |
| Mothers age (year) | 31 ± 5.1 |
| Fathers age (year) | 32 ± 5.3 |
| n (%) | |
| Girls/boys | 6 (27)/16(73) |
| Breastfeeding at 12 mo | 5 (23) |
| ≥1 sibling | 10 (45) |
| Education level Mother | |
| Elementary school | 1 (4.5) |
| High school | 5 (22.7) |
| University | 16 (72.7) |
| Education level Father | |
| Elementary school | 1 (4.5) |
| High school | 7 (31.8) |
| University | 14 (63.6) |
| Born in Sweden | |
| Infant | 22 (100) |
| Mother | 21 (95.5) |
| Father | 17 (77.3) |
| Food Record 1 | Food Record with Image-Assistance 1 | Difference 1 | p for Difference 2 | |
|---|---|---|---|---|
| Total intake | ||||
| Energy (kJ) | 3901 ± 476 | 3905 ± 476 | 3.9 ± 48.0 | 0.71 |
| Protein (g) | 29.8 ± 5.7 | 30.1 ± 6.0 | 0.2 ± 1.1 | 0.30 |
| Fat (g) | 35.4 ± 6.7 | 35.4 ± 6.5 | 0.0 ± 0.6 | 0.89 |
| Carbohydrate (g) | 118.3 ± 17.7 | 118.4 ± 17.2 | 0.1 ± 1.5 | 0.80 |
| Main course meals | ||||
| Energy (kJ) | 1348 ± 388 | 1350 ± 377 | 1.7 ± 55 | 0.89 |
| Protein (g) | 13.0 ± 3.9 | 13.4 ± 4.1 | 0.4 ± 1.5 | 0.19 |
| Fat (g) | 12.5 ± 4.2 | 12.7 ± 3.9 | 0.2 ± 1.3 | 0.37 |
| Carbohydrate (g) | 38.0 ± 13.3 | 38.5 ± 12.9 | 0.5 ± 4.2 | 0.63 |
| Meals (n = 210) | Leftovers n (%) | No Leftovers n (%) | Total n (%) |
|---|---|---|---|
| Non-adjusted meals | 67 (53) | 74 (89) | 141 (67) |
| Adjusted meals | 60 (47) | 9 (11) | 69 (33) |
| Underestimated 1 | 34 (27) | 2 (3) | 36 (52) |
| Overestimated 2 | 26 (20) | 7 (8) | 33 (48) |
| Total | 127 (60) | 83 (40) | 210 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johansson, U.; Venables, M.; Öhlund, I.; Lind, T. Active Image-Assisted Food Records in Comparison to Regular Food Records: A Validation Study against Doubly Labeled Water in 12-Month-Old Infants. Nutrients 2018, 10, 1904. https://doi.org/10.3390/nu10121904
Johansson U, Venables M, Öhlund I, Lind T. Active Image-Assisted Food Records in Comparison to Regular Food Records: A Validation Study against Doubly Labeled Water in 12-Month-Old Infants. Nutrients. 2018; 10(12):1904. https://doi.org/10.3390/nu10121904
Chicago/Turabian StyleJohansson, Ulrica, Michelle Venables, Inger Öhlund, and Torbjörn Lind. 2018. "Active Image-Assisted Food Records in Comparison to Regular Food Records: A Validation Study against Doubly Labeled Water in 12-Month-Old Infants" Nutrients 10, no. 12: 1904. https://doi.org/10.3390/nu10121904