Celiac Disease Diagnosed through Screening Programs in At-Risk Adults Is Not Associated with Worse Adherence to the Gluten-Free Diet and Might Protect from Osteopenia/Osteoporosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Setting
2.2. Inclusion and Exclusion Criteria
2.3. Clinical Evaluations
2.4. Evaluation of Adherence to the GFD
2.5. Ethics
2.6. Sample Size Considerations
2.7. Statistical Analysis
3. Results
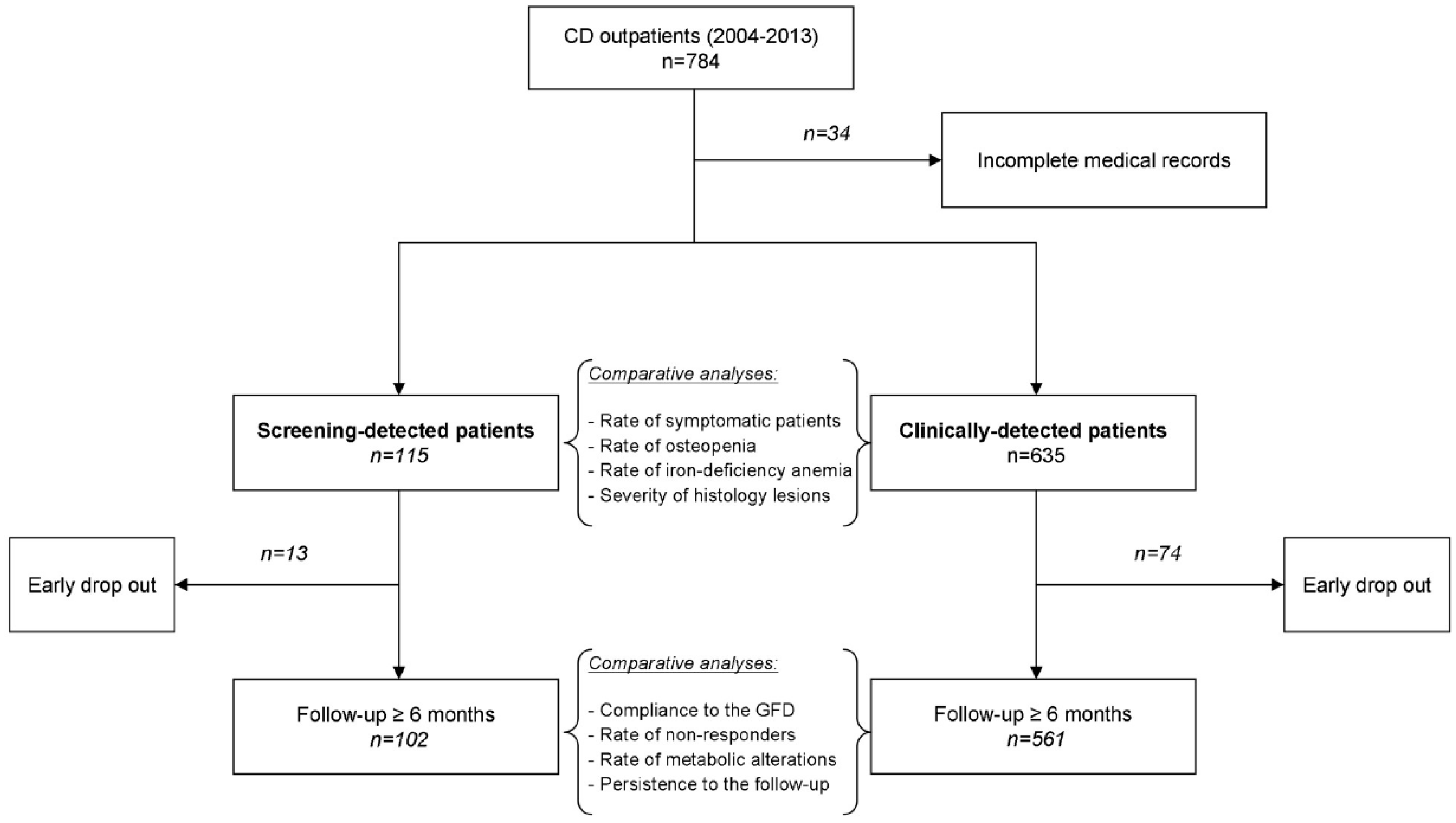
3.1. Study Population
3.2. Characteristics at Diagnosis
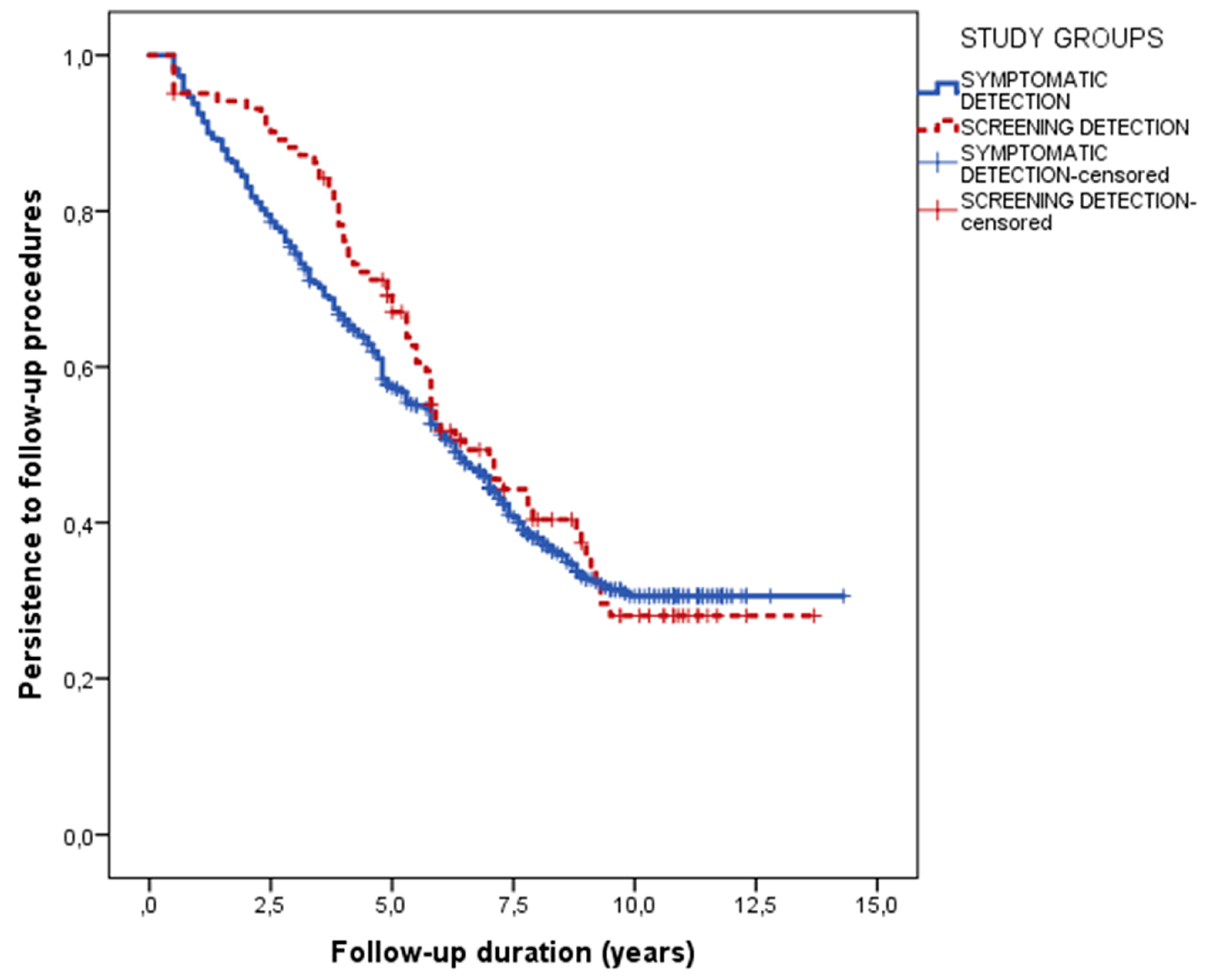
3.3. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ludvigsson, J.L.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Green, P.H. Where are all those patients with Celiac disease? Am. J. Gastroenterol. 2007, 102, 1461–1463. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- Hill, I.D.; Dirks, M.H.; Liptak, G.S.; Colletti, R.B.; Fasano, A.; Guandalini, S.; Hoffenberg, E.J.; Horvath, K.; Murray, J.A.; Mitchell, P.; et al. Guideline for the diagnosis and treatment of celiac disease in children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef] [PubMed]
- Viljamaa, M.; Collin, P.; Huhtala, H.; Sievänen, H.; Mäki, M.; Kaukinen, K. Is coeliac disease screening in risk groups justified? A fourteen-year follow-up with special focus on compliance and quality of life. Aliment. Pharmacol. Ther. 2005, 22, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ukkola, A.; Mäki, M.; Kurppa, K.; Collin, P.; Huhtala, H.; Kekkonen, L.; Kaukinen, K. Diet improves perception of health and well-being in symptomatic, but not asymptomatic, patients with celiac disease. Clin. Gastroenterol. Hepatol. 2011, 9, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Kivelä, L.; Popp, A.; Arvola, T.; Huhtala, H.; Kaukinen, K.; Kurppa, K. Long-term health and treatment outcomes in adult coeliac disease patients diagnosed by screening in childhood. United Eur. Gastroenterol. J. 2018, 6, 1022–1031. [Google Scholar] [CrossRef]
- van Koppen, E.J.; Schweizer, J.J.; Csizmadia, C.G.; Krom, Y.; Hylkema, H.B.; van Geel, A.M.; Koopman, H.M.; Verloove-Vanhorick, S.P.; Mearin, M.L. Long-term health and quality-of-life consequences of mass screening for childhood celiac disease: A 10-year follow-up study. Pediatrics 2009, 123, e582-8. [Google Scholar] [CrossRef]
- Fabiani, E.; Taccari, L.M.; Rätsch, I.M.; Di Giuseppe, S.; Coppa, G.V.; Catassi, C. Compliance with gluten-free diet in adolescents with screening-detected celiac disease: A 5-year follow-up study. J. Pediatr. 2000, 136, 841–843. [Google Scholar] [CrossRef]
- Jadresin, O.; Misak, Z.; Sanja, K.; Sonicki, Z.; Zizić, V. Compliance with gluten-free diet in children with coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 344–348. [Google Scholar] [CrossRef]
- Laurikka, P.; Nurminen, S.; Kivelä, L.; Kurppa, K. Extraintestinal Manifestations of Celiac Disease: Early Detection for Better Long-Term Outcomes. Nutrients 2018, 10, 1015. [Google Scholar] [CrossRef]
- Bathrellou, E.; Kontogianni, M.D.; Panagiotakos, D.B. Celiac disease and non-celiac gluten or wheat sensitivity and health in later life: A review. Maturitas 2018, 112, 29–33. [Google Scholar] [CrossRef]
- Italian Guidelines for the Diagnosis and the Follow-up of Celiac Disease. 2015. Available online: http://www.celiachia.it/public/bo/upload/eventi_progetti/A.07.Booklet%20Celiachia%20-%20Impaginato.pdf (accessed on 7 November 2018).
- Kivelä, L.; Kaukinen, K.; Huhtala, H.; Lähdeaho, M.L.; Mäki, M.; Kurppa, K. At-Risk Screened Children with Celiac Disease are Comparable in Disease Severity and Dietary Adherence to Those Found because of Clinical Suspicion: A Large Cohort Study. J. Pediatr. 2017, 183, 115–121. [Google Scholar] [CrossRef]
- Kinos, S.; Kurppa, K.; Ukkola, A.; Collin, P.; Lähdeaho, M.L.; Huhtala, H.; Kekkonen, L.; Mäki, M.; Kaukinen, K. Burden of illness in screen-detected children with celiac disease and their families. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 412–416. [Google Scholar] [CrossRef]
- Kurppa, K.; Lauronen, O.; Collin, P.; Ukkola, A.; Laurila, K.; Huhtala, H.; Mäki, M.; Kaukinen, K. Factors associated with dietary adherence in celiac disease: A nationwide study. Digestion 2012, 86, 309–314. [Google Scholar] [CrossRef]
- Vilppula, A.; Kaukinen, K.; Luostarinen, L.; Krekelä, I.; Patrikainen, H.; Valve, R.; Luostarinen, M.; Laurila, K.; Mäki, M.; Collin, P. Clinical benefit of gluten-free diet in screen-detected older celiac disease patients. BMC Gastroenterol. 2011, 11, 136. [Google Scholar] [CrossRef]
- Mustalahti, K.; Collin, P.; Sievänen, H.; Salmi, J.; Mäki, M. Osteopenia in patients with clinically silent coeliac disease warrants screening. Lancet 1999, 354, 744–745. [Google Scholar] [CrossRef]
- Sundar, N.; Crimmins, R.; Swift, G. Clinical presentation and incidence of complications in patients with coeliac disease diagnosed by relative screening. Postgrad. Med. J. 2007, 83, 273–276. [Google Scholar]
- Heikkila, K.; Pearce, J.; Maki, M.; Kaukinen, K. Celiac disease and bone fractures: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2015, 100, 25–34. [Google Scholar] [CrossRef]
- Davie, M.W.; Gaywood, I.; George, E.; Jones, P.W.; Masud, T.; Price, T.; Summers, G.D. Excess non-spine fractures in women over 50 years with celiac disease: A cross-sectional, questionnaire-based study. Osteoporos. Int. 2015, 16, 1150–1155. [Google Scholar] [CrossRef]
- Meyer, D.; Stavropolous, S.; Diamond, B.; Shane, E.; Green, P.H. Osteoporosis in a north american adult population with celiac disease. Am. J. Gastroenterol. 2001, 96, 112–119. [Google Scholar] [CrossRef]
- Pantaleoni, S.; Luchino, M.; Adriani, A.; Pellicano, R.; Stradella, D.; Ribaldone, D.G.; Sapone, N.; Isaia, G.C.; Stefano, M.D.; Astegiano, M. Bone mineral density at diagnosis of celiac disease and after 1 year of gluten-free diet. Sci. World J. 2014, 173082. [Google Scholar] [CrossRef]
- Tolone, C.; Bellini, G.; Punzo, F.; Papparella, A.; Miele, E.; Vitale, A.; Nobili, B.; Strisciuglio, C.; Rossi, F. The DMT1 IVS4+44C>A polymorphism and the risk of iron deficiency anemia in children with celiac disease. PLoS ONE. 2017, 12, e0185822. [Google Scholar] [CrossRef]
- Moreno, M.L.; Crusius, J.B.; Cherñavsky, A.; Sugai, E.; Sambuelli, A.; Vazquez, H.; Mauriño, E.; Peña, A.S.; Bai, J.C. The IL-1 gene family and bone involvement in celiac disease. Immunogenetics 2005, 57, 618–620. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Familiar Screening (Total) | 78 (67.8) |
| Index case: brother/sister | 26 (22.6) |
| Index case: father/mother | 18 (15.7) |
| Index case: son/daughter | 18 (15.7) |
| Index case: nephew/grandchild | 11 (9.6) |
| Index case: cousin | 5 (4.3) |
| At-Risk Associated Conditions (Total) | 37 (32.2) |
| Autoimmune thyroid disease | 10 (8.7) |
| Type-1 diabetes mellitus | 6 (5.2) |
| Primary biliary cholangitis | 3 (2.6) |
| IgA deficiency | 3 (2.6) |
| Down syndrome | 3 (2.6) |
| Vitiligo | 3 (2.6) |
| Sjogren syndrome | 1 (0.9) |
| Turner syndrome | 1 (0.9) |
| Other | 7 (6.1) |
| Parameter | Screening (n = 115) | Clinical Suspicion (n = 635) | p |
|---|---|---|---|
| Age (Years) | 34 (22–46) | 33 (22–44) | 0.690 |
| Sex (Female) | 80 (69.6) | 502 (79.1) | 0.021 |
| Time since Diagnosis (Years) | 1.5 (0.0–5.0) | 2.0 (0.0–6.50) | 0.145 |
| Symptoms | 29 (25.2) | 594 (93.5) | <0.001 |
| Iron-Deficiency Anemia | 25 (21.7) | 324 (51.0) | <0.001 |
| Osteopenia/Osteoporosis | 36 (31.3) | 292 (46.0) | 0.003 |
| Histology | |||
| -Marsh 3a | 33 (28.7) | 182 (28.7) | |
| -Marsh 3b | 43 (37.4) | 180 (28.3) | 0.100 |
| -Marsh 3c | 39 (33.9) | 273 (42.3) |
| Parameter | Screening (n = 102) | Clinical suspicion (n = 561) | p |
|---|---|---|---|
| Correct Compliance | 93 (91.2) | 504 (89.8) | 0.857 |
| Accidental Contaminations | 2 (2.0) | 25 (4.5) | 0.410 |
| Voluntary Gluten Ingestion | 7 (6.9) | 32 (5.7) | 0.647 |
| Gerd-like Symptoms | 2 (2.0) | 17 (3.0) | 0.753 |
| Ibs-like Symptoms (Total) | 8 (7.8) | 79 (14.1) | 0.110 |
| (a) classical ibs | 4 (3.9) | 43 (7.7) | 0.212 |
| (b) Diarrhea-predominant IBS | 1 (1.0) | 6 (1.1) | 1.000 |
| (c) Constipation-predominant IBS | 3 (2.9) | 30 (5.3) | 0.457 |
| Metabolic Alterations (tOtal) | 15 (14.7) | 96 (17.1) | 0.666 |
| (a) weight increase >10% | 7 (6.9) | 34 (6.1) | 0.823 |
| (b) cholesterol increase >50 mg/dL | 7 (6.9) | 36(6.4) | 0.864 |
| (c) metabolic syndrome | 1 (1.0) | 26 (4.6) | 0.103 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tovoli, F.; Negrini, G.; Sansone, V.; Faggiano, C.; Catenaro, T.; Bolondi, L.; Granito, A. Celiac Disease Diagnosed through Screening Programs in At-Risk Adults Is Not Associated with Worse Adherence to the Gluten-Free Diet and Might Protect from Osteopenia/Osteoporosis. Nutrients 2018, 10, 1940. https://doi.org/10.3390/nu10121940
Tovoli F, Negrini G, Sansone V, Faggiano C, Catenaro T, Bolondi L, Granito A. Celiac Disease Diagnosed through Screening Programs in At-Risk Adults Is Not Associated with Worse Adherence to the Gluten-Free Diet and Might Protect from Osteopenia/Osteoporosis. Nutrients. 2018; 10(12):1940. https://doi.org/10.3390/nu10121940
Chicago/Turabian StyleTovoli, Francesco, Giulia Negrini, Vito Sansone, Chiara Faggiano, Teresa Catenaro, Luigi Bolondi, and Alessandro Granito. 2018. "Celiac Disease Diagnosed through Screening Programs in At-Risk Adults Is Not Associated with Worse Adherence to the Gluten-Free Diet and Might Protect from Osteopenia/Osteoporosis" Nutrients 10, no. 12: 1940. https://doi.org/10.3390/nu10121940