Food Parenting Practices among Parents with Overweight and Obesity: A Systematic Review

Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
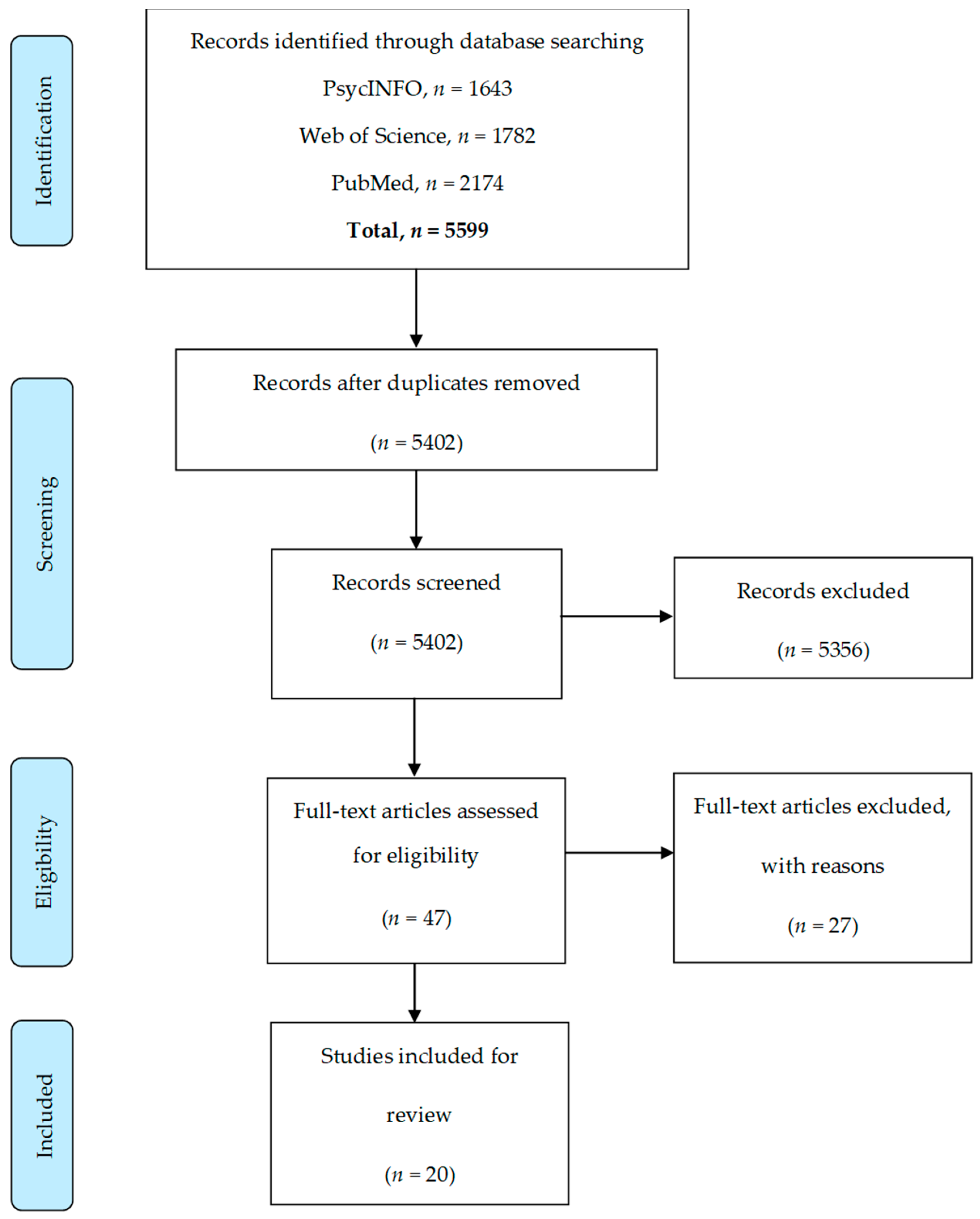
2.3. Article Screening
2.4. Data Extraction and Synthesis
2.5. Quality Assessment
3. Results
3.1. Summary of Included Studies
3.2. Study Quality
3.3. FPP Results
3.3.1. Coercive Control
Parental control
Using food to control negative emotions
Threats and bribes
Discipline
Pressure to eat
Restriction
3.3.2. Structure
Meal and snack routines
Monitoring
Food accessibility
Rules and limits
Food availability
Modelling
Unstructured practices
3.3.3. Autonomy Support/Promotion
Child involvement
Encouragement
Praise
Nutrition education
4. Discussion
Study Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reilly, J.J.; Armstrong, J.; Dorosty, A.R.; Emmett, P.M.; Ness, A.; Rogers, I.; Steer, C.; Sherriff, A. Early life risk factors for obesity in childhood: Cohort study. BMJ 2005, 330, 1357. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, K.L.; Jarvis, M.J.; Beeken, R.J.; Boniface, D.; Wardle, J. Comparing maternal and paternal intergenerational transmission of obesity risk in a large population-based sample. Am. J. Clin. Nutr. 2010, 91, 1560–1567. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.; Li, L.; Kuh, D.; Hardy, R. How has the age-related process of overweight or obesity development changed over time? co-ordinated analyses of individual participant data from five united kingdom birth cohorts. PLoS Med. 2015, 12, e1001828. [Google Scholar] [CrossRef] [PubMed]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.A.; Llewellyn, D.J.; Alexander, K.; Melzer, D. Obesity, physical function, and mortality in older adults. J. Am. Geriatr. Soc. 2008, 56, 1474–1478. [Google Scholar] [CrossRef]
- Hemminki, K.; Li, X.; Sundquist, J.; Sundquist, K. Obesity and familial obesity and risk of cancer. Eur. J. Cancer Prev. 2011, 20, 438–443. [Google Scholar] [CrossRef]
- Resta, O.; Foschino-Barbaro, M.P.; Legari, G.; Talamo, S.; Bonfitto, P.; Palumbo, A.; Minenna, A.; Giorgino, R.; De Pergola, G. Sleep-related breathing disorders, loud snoring and excessive daytime sleepiness in obese subjects. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 669–675. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Welch, S.L.; Doll, H.A.; Davies, B.A.; O’Connor, M.E. Risk factors for bulimia nervosa. A community-based case-control study. Arch. Gen. Psychiatry 1997, 54, 509–517. [Google Scholar] [CrossRef]
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef]
- Moskowitz, L.; Weiselberg, E. Anorexia Nervosa/Atypical Anorexia Nervosa. Curr. Probl. Pediatr. Adolesc. Health Care 2017, 47, 70–84. [Google Scholar] [CrossRef]
- Tozzi, F.; Sullivan, P.F.; Fear, J.L.; McKenzie, J.; Bulik, C.M. Causes and recovery in anorexia nervosa: The patient’s perspective. Int. J. Eat. Disord. 2003, 33, 143–154. [Google Scholar] [CrossRef] [PubMed]
- WHO. Facts and Figures on Childhood Obesity. Available online: http://www.who.int/end-childhood-obesity/facts/en/ (accessed on 30 August 2018).
- England, P.H. Childhood Obesity: Applying All Our Health. Available online: https://www.gov.uk/government/publications/childhood-obesity-applying-all-our-health/childhood-obesity-applying-all-our-health (accessed on 24 August 2017).
- Health and Social Care Information Centre. Health Survey for England-2014. Available online: https://www.gov.uk/government/statistics/health-survey-for-england-2014 (accessed on 14 December 2017).
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Lydecker, J.A.; Grilo, C.M. Children of parents with BED have more eating behavior disturbance than children of parents with obesity or healthy weight. Int. J. Eat. Disord. 2017, 50, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, D.L.; Warschburger, P.A. Familial transmission of eating behaviors in preschool-aged children. Obesity (Silver Spring) 2008, 16, 1821–1825. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental influence on eating behavior: Conception to adolescence. J. Law Med. Ethics. 2007, 35, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Keukelier, E.; Maes, L. Influence of mother’s educational level on food parenting practices and food habits of young children. Appetite 2004, 43, 93–103. [Google Scholar] [CrossRef] [PubMed]
- McCaffree, J. Childhood eating patterns: The roles parents play. J. Am. Diet. Assoc. 2003, 103, 1587. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Carnell, S.; Cooke, L. Parental control over feeding and children’s fruit and vegetable intake: How are they related? J. Am. Diet. Assoc. 2005, 105, 227–232. [Google Scholar] [CrossRef]
- Skouteris, H.; McCabe, M.; Ricciardelli, L.A.; Milgrom, J.; Baur, L.A.; Aksan, N.; Dell’Aquila, D. Parent–child interactions and obesity prevention: A systematic review of the literature. Early Child. Dev. Care 2012, 182, 153–174. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental constructs in food parenting practices: A content map to guide future research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef]
- Blissett, J. Relationships between parenting style, feeding style and feeding practices and fruit and vegetable consumption in early childhood. Appetite 2011, 57, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.K.; Hermans, R.C.; Sleddens, E.F.; Engels, R.C.; Fisher, J.O.; Kremers, S.P. How parental dietary behavior and food parenting practices affect children’s dietary behavior. Interacting sources of influence? Appetite 2015, 89, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting styles, feeding styles, feeding practices, and weight status in 4–12 year-old children: A systematic review of the literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef] [PubMed]
- Jansen, P.W.; Tharner, A.; van der Ende, J.; Wake, M.; Raat, H.; Hofman, A.; Verhulst, F.C.; van Ijzendoorn, M.H.; Jaddoe, V.W.; Tiemeier, H. Feeding practices and child weight: Is the association bidirectional in preschool children? Am. J. Clin. Nutr. 2014, 100, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Strauss, R.S.; Knight, J. Influence of the home environment on the development of obesity in children. Pediatrics 1999, 103, e85. [Google Scholar] [CrossRef] [PubMed]
- Danielzik, S.; Langnäse, K.; Mast, M.; Spethmann, C.; Müller, M.J. Impact of parental BMI on the manifestation of overweight 5–7 year old children. Eur. J. Nutr. 2002, 41, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, C.; Talamini, G.; Tatò, L. Influence of diet, physical activity and parents’ obesity on children’s adiposity: A four-year longitudinal study. Int. J. Obes. 1998, 22, 758. [Google Scholar] [CrossRef]
- Birbilis, M.; Moschonis, G.; Mougios, V.; Manios, Y. Obesity in adolescence is associated with perinatal risk factors, parental BMI and sociodemographic characteristics. Eur. J. Clin. Nutr. 2013, 67, 115–121. [Google Scholar] [CrossRef]
- Laitinen, J.; Power, C.; Jarvelin, M.R. Family social class, maternal body mass index, childhood body mass index, and age at menarche as predictors of adult obesity. Am. J. Clin. Nutr. 2001, 74, 287–294. [Google Scholar] [CrossRef]
- Anzman, S.L.; Rollins, B.Y.; Birch, L.L. Parental influence on children’s early eating environments and obesity risk: Implications for prevention. Int. J. Obes. 2010, 34, 1116–1124. [Google Scholar] [CrossRef]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94, S2006–S2011. [Google Scholar] [CrossRef] [PubMed]
- Musher-Eizenman, D.; Holub, S. Comprehensive feeding practices questionnaire: Validation of a new measure of parental feeding practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Paxton, S.J.; Massey, R.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Schwartz, M.B. If you are good you can have a cookie: How memories of childhood food rules link to adult eating behaviors. Eat. Behav. 2003, 4, 283–293. [Google Scholar] [CrossRef]
- Birch, L.L.; Zimmerman, S.I.; Hind, H. The Influence of social-affective context on the formation of children’s food preferences. Child Dev. 1980, 51, 856–861. [Google Scholar] [CrossRef]
- Ventura, A.K.; Worobey, J. Early influences on the development of food preferences. Curr. Biol. 2013, 23, R401–R408. [Google Scholar] [CrossRef]
- Baughcum, A.E.; Burklow, K.A.; Deeks, C.M.; Powers, S.W.; Whitaker, R.C. Maternal feeding practices and childhood obesity: A focus group study of low-income mothers. Arch. Pediatr. Adolesc. Med. 1998, 152, 1010–1014. [Google Scholar] [CrossRef]
- Tan, C.C.; Ruhl, H.; Chow, C.M.; Ellis, L. Retrospective reports of parental feeding practices and emotional eating in adulthood: The role of food preoccupation. Appetite 2016, 105, 410–415. [Google Scholar] [CrossRef]
- Allen, K.L.; Byrne, S.M.; La Puma, M.; McLean, N.; Davis, E.A. The onset and course of binge eating in 8- to 13-year-old healthy weight, overweight and obese children. Eat. Behave. 2008, 9, 438–446. [Google Scholar] [CrossRef]
- Waller, G.; Osman, S. Emotional eating and eating psychopathology among non-eating-disordered women. Int. J. Eat. Disord. 1998, 23, 419–424. [Google Scholar] [CrossRef]
- Stifter, C.A.; Anzman-Frasca, S.; Birch, L.L.; Voegtline, K. Parent use of food to soothe infant/toddler distress and child weight status. An exploratory study. Appetite 2011, 57, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Haycraft, E.; Farrow, C. Inducing preschool children’s emotional eating: Relations with parental feeding practices. Am. J. Clin. Nutr. 2010, 92, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Carper, J.L.; Orlet Fisher, J.; Birch, L.L. Young girls’ emerging dietary restraint and disinhibition are related to parental control in child feeding. Appetite 2000, 35, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.A.; MacLehose, R.F.; Fulkerson, J.A.; Crow, S.; Neumark-Sztainer, D. Are food restriction and pressure-to-eat parenting practices associated with adolescent disordered eating behaviors? Int. J. Eat. Disord. 2014, 47, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Haycraft, E. Parental eating disorder symptoms and observations of mealtime interactions with children. J. Psychosom. Res. 2011, 70, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Meyer, C.; Haycraft, E. Maternal and paternal controlling feeding practices with male and female children. Appetite 2006, 47, 212–219. [Google Scholar] [CrossRef]
- Galloway, A.T.; Fiorito, L.M.; Francis, L.A.; Birch, L.L. ‘Finish your soup’: Counterproductive effects of pressuring children to eat on intake and affect. Appetite 2006, 46, 318–323. [Google Scholar] [CrossRef]
- Kröller, K.; Jahnke, D.; Warschburger, P. Are maternal weight, eating and feeding practices associated with emotional eating in childhood? Appetite 2013, 65, 25–30. [Google Scholar] [CrossRef]
- Clark, H.R.; Goyder, E.; Bissell, P.; Blank, L.; Peters, J. How do parents’ child-feeding behaviours influence child weight? Implications for childhood obesity policy. J. Public Health 2007, 29, 132–141. [Google Scholar] [CrossRef]
- Birch, L.; Davison, K. Family environmental factors influencing the developing behavioral controls of food intake and childhood overweight. Pediatr. Clin. North Am. 2001, 48, 893–907. [Google Scholar] [CrossRef]
- WHO. 10 Facts on Obesity. Available online: http://www.who.int/features/factfiles/obesity/en/ (accessed on 16 December 2016).
- Horsley, T.; Dingwall, O.; Sampson, M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, V.; Foley, M.; Quirk, A.; McCambridge, J. Shedding light on research participation effects in behaviour change trials: A qualitative study examining research participant experiences. BMC Public Health 2016, 16, 91. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E. Systematic reviews: CRD’s guidance for undertaking reviews in health care. Lancet Infect. Dis. 2010, 10, 226. [Google Scholar] [CrossRef]
- NICE. Guidelines Manual. Appendix G: Quality Appraisal Checklist-Quantitative Studies Reporting Correlations and Associations. Available online: https://www.nice.org.uk/process/pmg4/chapter/appendix-g-quality-appraisal-checklist-quantitative-studies-reporting-correlations-and (accessed on 10 January 2017).
- Kelly, S.; Martin, S.; Kuhn, I.; Cowan, A.; Brayne, C.; Lafortune, L. Barriers and facilitators to the uptake and maintenance of healthy behaviours by people at mid-life: A rapid systematic review. PLoS ONE 2016, 11, e0145074. [Google Scholar] [CrossRef]
- Windle, G.; Hughes, D.; Linck, P.; Russell, I.; Woods, B. Is exercise effective in promoting mental well-being in older age? A systematic review. Aging Ment. Health 2010, 14, 652–669. [Google Scholar] [CrossRef]
- McPhie, S.; Skouteris, H.; Daniels, L.; Jansen, E. Maternal correlates of maternal child feeding practices: A systematic review. Matern. Child Nutr. 2014, 10, 18–43. [Google Scholar] [CrossRef]
- Baughcum, A.E.; Powers, S.W.; Johnson, S.B.; Chamberlin, L.A.; Deeks, C.M.; Jain, A.; Whitaker, R.C. Maternal feeding practices and beliefs and their relationships to overweight in early childhood. JDBP 2001, 22, 391–408. [Google Scholar] [CrossRef]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disords. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Cebeci, A.N.; Guven, A. Does maternal obesity have an influence on feeding behavior of obese children? Minerva Pediatr. 2015, 67, 481–487. [Google Scholar] [PubMed]
- Corsini, N.; Wilson, C.; Kettler, L.; Danthiir, V. Development and preliminary validation of the Toddler Snack Food Feeding Questionnaire. Appetite 2010, 54, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.S.; Pino, D.L.; Friedman, R. Caregivers’ attitudes and practices: Influence on childhood body weight. J. Biosoc. Sci. 2011, 43, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Hofer, S.M.; Birch, L.L. Predictors of maternal child-feeding style: Maternal and child characteristics. Appetite 2001, 37, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Birch, L.L. Maternal weight status modulates the effects of restriction on daughters’ eating and weight. Int. J. Obes. 2005, 29, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Haycraft, E.; Karasouli, E.; Meyer, C. Maternal feeding practices and children’s eating behaviours: A comparison of mothers with healthy weight versus overweight/obesity. Appetite 2017, 116, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Jingxiong, J.; Rosenqvist, U.; Huishan, W.; Koletzko, B.; Guangli, L.; Jing, H.; Greiner, T. Relationship of parental characteristics and feeding practices to overweight in infants and young children in Beijing, China. Public Health Nutr. 2009, 12, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Kröller, K.; Warschburger, P. Associations between maternal feeding style and food intake of children with a higher risk for overweight. Appetite 2008, 51, 166–172. [Google Scholar] [CrossRef]
- Lewis, M.; Worobey, J. Mothers and toddlers lunch together. The relation between observed and reported behavior. Appetite 2011, 56, 732–736. [Google Scholar] [CrossRef]
- Lipowska, M.; Lipowski, M.; Jurek, P.; Jankowska, A.M.; Pawlicka, P. Gender and body-fat status as predictors of parental feeding styles and children’s nutritional knowledge, eating habits and behaviours. Int. J. Environ. Res. Public Health 2018. [Google Scholar] [CrossRef]
- Lumeng, J.C.; Burke, L.M. Maternal prompts to eat, child compliance, and mother and child weight status. J. Pediatr. 2006, 149, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.W.; Chamberlin, L.A.; van Schaick, K.B.; Sherman, S.N.; Whitaker, R.C. Maternal feeding strategies, child eating behaviors, and child BMI in low-income African-American preschoolers. Obesity 2006, 14, 2026–2033. [Google Scholar] [CrossRef] [PubMed]
- Raaijmakers, L.G.; Gevers, D.W.; Teuscher, D.; Kremers, S.P.; van Assema, P. Emotional and instrumental feeding practices of Dutch mothers regarding foods eaten between main meals. BMC Public Health 2014, 14, 171. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.T.; Goodman, L.C.; Musher-Eizenman, D.R. Parental correlates of food parenting practices: Socioeconomic status, weight, and dieting status. Ecol. Food Nutr. 2018, 57, 330–345. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.G.; Haszard, J.J.; Taylor, R.W.; Heath, A.M.; Taylor, B.; Campbell, K.J. Parental feeding practices associated with children’s eating and weight: What are parents of toddlers and preschool children doing? Appetite 2018, 128, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Sanderson, S.; Guthrie, C.A.; Rapoport, L.; Plomin, R. Parental feeding style and the inter-generational transmission of obesity risk. Obesity 2002, 10, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Wendt, V.; Bergmann, S.; Herfurth-Majstorovic, K.; Keitel-Korndorfer, A.; von Klitzing, K.; Klein, A.M. Parent-child interaction during feeding or joint eating in parents of different weights. Eat. Behave. 2015, 18, 131–136. [Google Scholar] [CrossRef]
- Williams, J.E.; Helsel, B.; Griffin, S.F.; Liang, J. Associations between parental bmi and the family nutrition and physical activity environment in a community sample. J. Community Health 2017, 42, 1233–1239. [Google Scholar] [CrossRef]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Berge, J.M.; Meyer, C.S.; Loth, K.; MacLehose, R.; Neumark-Sztainer, D. Parent/adolescent weight status concordance and parent feeding practices. Pediatrics 2015, 136, e591–e598. [Google Scholar] [CrossRef]
- Chatoor, I.; Getson, P.; Menvielle, E.; Brasseaux, C.; O’Donnell, R.; Rivera, Y.; Mrazek, D.A. A feeding scale for research and clinical practice to assess mother—infant interactions in the first three years of life. Infant Ment. Health J. 1997, 18, 76–91. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; Orlet Fisher, J.; Mueller, S.; Nicklas, T.A. Revisiting a neglected construct: Parenting styles in a child-feeding context. Appetite 2005, 44, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Grolnick, W.S.; Pomerantz, E.M. Issues and challenges in studying parental control: Toward a new conceptualization. Child Dev. Perspect. 2009, 3, 165–170. [Google Scholar] [CrossRef]
- Snoek, H.M.; Engels, R.C.M.E.; Janssens, J.M.A.M.; van Strien, T. Parental behaviour and adolescents’ emotional eating. Appetite 2007, 49, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.L. The psychobiology of comfort eating: Implications for neuropharmacological interventions. Behav. Pharmacol. 2012, 23, 442–460. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.E.; Paxton, S.J.; Brozovic, A.M. Maternal feeding practices, child eating behaviour and body mass index in preschool-aged children: A prospective analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 55. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Tabak, R.G.; Bryant, M.J.; Ward, D.S. Measuring parent food practices: A systematic review of existing measures and examination of instruments. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Palavras, M.A.; Kaio, G.H.; Mari Jde, J.; Claudino, A.M. A review of Latin American studies on binge eating disorder. Braz. J. Psychiatr. 2011, 33, S81–S108. [Google Scholar] [CrossRef]
- Udo, T.; Grilo, C.M. Prevalence and correlates of DSM-5–Defined eating disorders in a nationally representative sample of U.S. adults. Biol. Psychiatry 2018, 84, 345–354. [Google Scholar] [CrossRef]
- Villarejo, C.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Peñas-Lledó, E.; Granero, R.; Penelo, E.; Tinahones, F.J.; Sancho, C.; Vilarrasa, N.; Montserrat-Gil de Bernabé, M.; et al. Lifetime obesity in patients with eating disorders: Increasing prevalence, clinical and personality correlates. Eur. Eat. Disord. Rev. 2012, 20, 250–254. [Google Scholar] [CrossRef]
- Tiggemann, M.; Lowes, J. Predictors of maternal control over children’s eating behaviour. Appetite 2002, 39, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Haines, J.; Downing, K.L.; Tang, L.; Campbell, K.J.; Hesketh, K.D. Associations between maternal concern about child’s weight and related behaviours and maternal weight-related parenting practices: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 104. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, R.R.; Dzewaltowski, D.A. Model of the home food environment pertaining to childhood obesity. Nutr. Res. 2008, 66, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Biddle, S.J.H.; Gorely, T. Family correlates of fruit and vegetable consumption in children and adolescents: A systematic review. Public Health Nutr. 2009, 12, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Watts, A.W.; Barr, S.I.; Hanning, R.M.; Lovato, C.Y.; Mâsse, L.C. The home food environment and associations with dietary intake among adolescents presenting for a lifestyle modification intervention. BMC Nutrition 2018, 4, 3. [Google Scholar] [CrossRef]
- Emmett, P.M.; Jones, L.R.; Northstone, K. Dietary patterns in the avon longitudinal study of parents and children. Nutr. Res. 2015, 73, 207–230. [Google Scholar] [CrossRef] [PubMed]
- Di Pasquale, R.; Rivolta, A. A conceptual analysis of food parenting practices in the light of self-determination theory: Relatedness-enhancing, competence-enhancing and autonomy-enhancing food parenting practices. Front. Psychol. 2018. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef]
- Gu, C.; Warkentin, S.; Mais, L.A.; Carnell, S. Ethnic differences in parental feeding behaviors in UK parents of preschoolers. Appetite 2017, 113, 398–404. [Google Scholar] [CrossRef]
- Blissett, J.; Bennett, C. Cultural differences in parental feeding practices and children’s eating behaviours and their relationships with child BMI: A comparison of Black Afro-Caribbean, White British and White German samples. Eur. J. Clin. Nutr. 2013, 67, 180–184. [Google Scholar] [CrossRef]
- Cardel, M.; Willig, A.L.; Dulin-Keita, A.; Casazza, K.; Mark Beasley, T.; Fernández, J.R. Parental feeding practices and socioeconomic status are associated with child adiposity in a multi-ethnic sample of children. Appetite 2012, 58, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.A.; MacLehose, R.F.; Fulkerson, J.A.; Crow, S.; Neumark-Sztainer, D. Eat this, not that! Parental demographic correlates of food-related parenting practices. Appetite 2013, 60, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Wehrly, S.E.; Bonilla, C.; Perez, M.; Liew, J. Controlling parental feeding practices and child body composition in ethnically and economically diverse preschool children. Appetite 2014, 73, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J. Applied Multivariate Statistics for the Social Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1996. [Google Scholar]
- Sedgwick, P. Cross sectional studies: Advantages and disadvantages. BMJ 2014. [Google Scholar] [CrossRef]
- Ventura, A.K.; Birch, L.L. Does parenting affect children’s eating and weight status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Scanlon, K.S.; May, A.; Rose, C.; Birch, L. Bottle-feeding practices during early infancy and eating behaviors at 6 years of age. Pediatrics 2014, 134, S70–S77. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Quality Rating |
|---|---|
| Baughcum et al., 2001 [64] | + |
| Cebeci and Guven, 2015 [66] | + |
| Corsini et al., 2010 [67] | - |
| Costa et al., 2011 [68] | - |
| Francis et al., 2001 [69] | + |
| Francis and Birch, 2005 [70] | + |
| Haycraft, Karasouli, and Meyer, 2017 [71] | + |
| Jingxiong et al., 2008 [72] | + |
| Kröller and Warschburger, 2008 [73] | + |
| Lewis and Worobey, 2011 [74] | - |
| Lipowska et al., 2018 [75] | + |
| Lumeng and Burke, 2006 [76] | - |
| Powers et al., 2006 [77] | + |
| Raaijmakers et al., 2014 [78] | + |
| Roberts, Goodman, and Musher-Eizenmann, 2018 [79] | ++ |
| Russell et al., 2018 [80] | + |
| Wardle et al., 2002 [81] | + |
| Wendt et al., 2015 [82] | + |
| Williams et al., 2017 [83] | + |
| Berge et al., 2015 [85] | ++ |
| Author(s), Study Country | Design | Aim(s) | Sample | BMI | n | Age of Children | FPP Measures | Relevant FPP Findings | Relevant Conclusions |
|---|---|---|---|---|---|---|---|---|---|
| Baughcum et al. (2001), USA [64] | Cross-sectional | To develop the Pre-schooler Feeding Questionnaire (PFQ). | 634 mothers | 18.5–29.9 | 488 | 23 months–5 year olds | PFQ | Significantly higher degree of age-inappropriate feeding (p = 0.004) (no longer true after adjusting for family income), concern about child overeating or being overweight (p = 0.001) regardless of child overweight and family income. Significantly lower degree of structure during feeding interactions (p = 0.001) (no longer true after adjusting for family income) among mothers with obesity vs. mothers without obesity. No significant differences on child control of feeding interactions (p = 0.070), using food to calm the child, concern about the child being underweight, difficulty in child feeding, and pushing the child to eat more (p values not reported) among mothers with obesity vs. mothers without obesity. | There is no specific feeding style associated with overweight young children. |
| ≥30 | 146 | ||||||||
| Cebeci and Guven (2014), Turkey [66] | Cross-sectional | To examine the influence of maternal obesity on FPPs with their children with obesity. | 491 mothers | 18–24.9 | 41 | 6–18.5 year olds | Turkish CFQ | Other than perceived parent weight (p < 0.001), there were no significant differences in any CFQ subscales (concern over perceived responsibility (p = 0.494), perceived child weight (p = 0.093), concern over child’s weight (p = 0.152), restriction (p = 0.234), pressure to eat (p = 0.072), and monitoring (p = 0.782)) among mothers with obesity vs. mothers without obesity. | Maternal BMI does not appear to have a significant influence on FPPs. |
| 25–29.9 | 134 | ||||||||
| ≥30 | 316 | ||||||||
| Corsini et al. (2010), Australia [67] | Cross-sectional | To develop and validate the Toddler Snack Food Feeding Questionnaire (TSFFQ). | Sample 2: 216 mothers | ≤18.5 | 2 | 4–5 year olds | TFSSQ and CFQ subscales: Restriction, Pressure to Eat and Monitoring | Sample 2 (pre-schoolers, past practices) Mothers without obesity allowed access to snack foods significantly less (p = 0.001), and implemented rules around snacking more (approaching statistical significance, p = 0.022) compared to mothers with obesity. No significant differences were found on any other constructs (p values not reported). | The TSFFQ is a useful measure that could be used in addition to other measures of parental feeding control. |
| 18.5–24.9 | 120 | ||||||||
| 25–29.9 | 45 | ||||||||
| ≥30 | 37 | ||||||||
| NR | 12 | ||||||||
| Costa et al. (2011), Brazil [68] | Cross-sectional | To examine parents feeding attitudes, parent BMI, and children’s weight status. | 105 Parents/Care-givers | <25 | 68 | 6–10 year olds | Portuguese CFQ | Significant differences in perceived parent weight (p = 0.001), concern about child weight (p = 0.006), and restriction (p = 0.023) between parents with healthy-weight vs. parents with overweight/obesity. No significant differences in perceived responsibility (p = 0.861), perceived child weight (p = 0.844), pressure to eat (p = 0.233), and monitoring (p = 0.21) between parents with healthy-weight and parents with overweight/obesity. | Perceptions and attitudes of parents may independently be associated with overweight in children aged 6–10. |
| >25 | 37 | ||||||||
| Francis et al. (2001), USA [69] | Cross-sectional | To explore the predictors of the use of maternal restriction and pressure FPPs. | 196 mothers | <25 | 92 | 5 year olds | CFQ subscales: Perceived child overweight, Child overweight, Restriction, and Pressure to Eat | There were no significant differences in the level of CFQ restriction and CFQ pressure to eat between mothers with healthy-weight and mothers with overweight. Among mothers with overweight, the use of restriction was significantly predicted by concern for daughters’ weight (p ≤ 0.05); pressure to eat was significantly predicted by daughters’ adiposity (p ≤ 0.05) and mothers’ concern for daughters’ weight (p ≤ 0.05). | Maternal weight status does not influence FPPs. |
| ≥25 | 104 | ||||||||
| Francis and Birch (2005), USA [70] | Longitudinal | To explore restriction on food intake, the influence of eating in the absence of hunger on BMI, and maternal weight status as a mediator on these relationships. | 171 mothers | ≤24.9 | 80 | 5–9 year olds | CFQ subscale: Restriction | Overall, there was no significant difference in the amount of restriction used by mothers with overweight vs. mothers with healthy weight. Among mothers with overweight, use of restrictive FPPs significantly predicted daughters’ eating in the absence of hunger (p < 0.05). | There is no specific feeding style associated with mothers with overweight and obesity. |
| ≥25 | 91 | ||||||||
| Haycraft, Karasouli and Meyer (2017), UK [71] | Cross-sectional | To compare maternal FPPs by maternal weight status. | 437 mothers | 19–24.9 | 249 | 2–6 year olds | CFPQ | Significantly higher reports of child control (p < 0.001) and lower reports of encouraging balance and variety (p = 0.029), environment (p = 0.021) and modelling (p < 0.001) among mothers with overweight/obesity vs. mothers with healthy-weight. There were no significant differences between mothers with healthy-weight/overweight and obesity on any other CFPQ subscales (involvement, monitoring, pressure to eat, restriction for health, restrictions for weight control, food as a reward, emotion regulation). | Mothers with overweight and obesity engage in fewer healthy FPPs when compared to a healthy weight sample of mothers. |
| ≥25 | 188 | ||||||||
| Jingxiong et al. (2008), China [72] | Cross-sectional | To examine the relationship between FPPs and parental characteristics. | 430 mothers | ≤24 | 323 | 1–3 year olds | An interview to obtain information on: parent education level, family income, and FPPs (including a 24-h dietary recall) | In comparison to mothers with healthy-weight, mothers with overweight/obesity worry significantly more about their child overeating (p = 0.004) and that their child would develop obesity (p = 0.003). Significantly more mothers with overweight/obesity controlled feeding with a regular schedule in comparison to healthy-weight mothers (p = 0.017) and used food to soothe the child significantly less than healthy-weight mothers (p = 0.008). | Mothers with overweight report controlling child feeding with a regular feeding schedule and soothed children using food less often than mothers with healthy-weight. |
| ≥24 | 107 | ||||||||
| Kröller and Warschburger (2008), Germany [73] | Cross-sectional | To explore the impact of various FPPs on child’s food intake and the influence of socio-economic status and weight on the use of different types of FPPs. | 219 mothers | ≤24.9 | 104 | 3–6 year olds | Items from the CFQ, CFSQ and newly developed questions from interviews with mothers and experts | No significant differences in FPPs between mothers with healthy weight and overweight/obesity. Maternal weight (underweight/healthy weight/overweight/obesity) had no significant effect on the use of FPPs (p = 0.60). | Maternal weight does not influence the use of FPPs. |
| ≥25 | 111 | ||||||||
| Lewis and Worobey (2011), USA [74] | Laboratory observation | To explore maternal control and whether feeding style is different between healthy and overweight mothers. | 20 mothers | <25 | 10 | 2 year olds | CFQ, food record, observed behaviours and video recordings. | No significant differences in pressure (p = 0.56) and restriction (p = 0.28), observed feeding style pressure (p = 0.49), and observed feeding style restriction (p = 0.28) between mothers with healthy weight and mothers with overweight/obesity. Mothers with overweight/obesity demonstrated significantly more concern about their own weight (p = 0.05) than mothers with healthy weight. Maternal BMI was not correlated with reported or observed feeding styles. | Lack of association between reported and observed feeding styles. |
| ≥25 | 10 | ||||||||
| Lipowska et al. (2018), Poland [75] | Cross-sectional | To explore nutritional knowledge, eating habits, and appetite traits among children with and without excess body fat in the context of FPPs and body-fat status. | 315 mothers; 276 fathers | Healthy * Mothers Fathers | 190 109 | 5 year olds | PFSQ | Mothers with healthy body fat use encouragement to eat significantly less than mothers with an overfat body status (p < 0.05). Fathers with healthy body fat use control over eating significantly more than fathers with an overfat body status (p < 0.05). There were no significant findings on food as a reward and emotional feeding and parental body fat status (p values not reported). | Mothers with an overfat body status do not necessarily transmit unhealthy eating behaviours to their children. |
| Overfat * Mothers Fathers | 125 167 | ||||||||
| Lumeng and Burke (2006), USA [76] | Laboratory observation | To explore if there is an association between maternal prompting to eat, child compliance and mother and child weight status. | 71 mothers | <30 | 45 | 3–6 year olds | Parental prompting and child compliance | There was no significant difference found in prompting child to eat (p = 0.55) between mothers with and without obesity. | Greater maternal prompting was predicted by a younger child age, a novel food, more bites of food taken by the mother and low maternal education. |
| ≥30 | 26 | ||||||||
| Powers et al. (2006), USA [77] | Cross-sectional | To explore the association of maternal feeding practices with maternal BMI and child eating behaviours. | 290 mothers | <24.9 | 77 | 2–4.9 year olds | CFQ subscales: Restriction and Pressure to eat, PFSQ subscale: Control | There were no significant differences found with between maternal BMI and maternal FPPs: restriction (p = 0.63), pressure to eat (p = 0.33), and control (p = 0.62). | There is no particular feeding style shared among mothers with overweight or obesity. |
| 25–29.9 | 86 | ||||||||
| 30–39.9 | 97 | ||||||||
| ≥40.0 | 30 | ||||||||
| Raaijmakers et al. (2014), The Netherlands [78] | Cross-sectional | To explore the use of instrumental and emotional feeding practices between main meals. | 359 mothers | ≤18.49 | 11 | 4–12 year olds | Self-constructed instrument developed from interviews with mothers and health promotion experts | Using food as a reward (26.8% of mothers with obesity) was reported more than use of food as a punishment (18.3% of mothers with obesity) and as a comfort (16.9% of mothers with obesity) with their child. No significant association between emotional and instrumental child feeding practices and maternal BMI. | Mothers offered energy dense and nutrient poor food items in emotional and instrumental child feeding practices. |
| 18.5–24.9 | 175 | ||||||||
| 25–29.9 | 101 | ||||||||
| ≥30 | 71 | ||||||||
| Over-weight (≥25) | 5 | ||||||||
| Obese | 10 | ||||||||
| Roberts, Goodman and Musher-Eizenmann (2018), USA [79] | Cross-sectional | To investigate socioeconomic status, parental BMI and dieting status on the use of FPPs. | 376 mothers; 118 fathers | 18.5–24.9 | 223 | 2.5–7.5 year olds | CFPQ, FSQ, MioH, and newly developed questions | Post-hoc analysis revealed that in comparison to parents with healthy-weight and overweight, parents with obesity use significantly less structure FPPs. There was no significant difference between parents with healthy-weight and overweight. There was no significant post-hoc differences between parents with healthy-weight, overweight, and obesity and autonomy promotion (irrespective of a significant main effect) and coercive control. | When compared to other parental characteristics such as parental BMI, socioeconomic status has a small influence on the use of FPPs. |
| 25–29.9 | 149 | ||||||||
| ≥ 30 | 120 | ||||||||
| Russell et al. (2018), Australia and New Zealand [80] | Cross-sectional (secondary data analysis) | To explore FPPs among parents of toddlers and pre-schoolers and to examine the how FPPs differ by parent and child demographic data. | 751 mothers | ≤25 | 383 | 4–6 year olds | CFPQ | Among pre-schoolers (and adjusted for receiving a nutrition intervention before the measurement of FPPs), the odds of mothers with obesity using CFPQ food as a reward and CFPQ child control were higher compared to mothers with healthy-weight (OR = 1.13, 95% CI 0.94, 1.36; OR = 1.22, 95% CI 0.71, 2.09). The odds of mothers with obesity using CFPQ restriction for health and pressure to eat were lower compared to mothers with healthy-weight (OR = 0.86, 95% CI 0.72, 1.02; OR = 0.82, 95% CI 0.73, 0.91). | Nutrition interventions are unlikely to detect change in targeted FPPs since parents already report best practices, such as modelling and a healthy food environment. |
| 25 ≤ 30 | 186 | ||||||||
| ≥30 | 152 | ||||||||
| NR | 30 | ||||||||
| Wardle et al. (2001), UK [81] | Cross-sectional | To identify any differences in feeding styles among mothers with obesity and normal weight. | Families with healthy-weight, over-weight and obesity | ≤25 | 114 | 4–5 year olds | PFSQ | Mothers with obesity reported significantly less control over their children’s eating (p = 0.01) than mothers with healthy-weight. There were no significant differences in reports of emotional feeding, instrumental feeding, and prompting/encouragement to eat. | No difference in use of emotional, instrumental, and prompting/encouragement to eat parental feeding styles among mothers with healthy-weight, and obesity. |
| Mothers ≥28.5 Fathers ≥25 | 100 | ||||||||
| Wendt et al. (2015), Germany [82] | Laboratory observation | To explore parent-child interactions during feeding or joint eating and investigate the differences between mothers and fathers and parental weight. | 148 mothers; 148 fathers | ≤18.5 Mothers Fathers | 4 2 | 7 months–3.9 year olds | Observation rated using the CFS | No significant differences found in CFS subscales: dyadic reciprocity, dyadic conflict, talk/distraction, struggle for control, and non-contingency among mothers with healthy-weight, overweight, and obesity. There were also no significant differences found among fathers with healthy-weight, overweight, and obesity apart from struggle for control. Fathers with overweight demonstrated a significantly higher amount of struggle for control than fathers with healthy-weight and obesity (p = 0.003). | Parents with healthy-weight, overweight, and obesity parents show the same ability to show relatedness, interpret child cues, and affective engagement during feeding and joint eating. |
| 18.5–24.9 Mothers Fathers | 83 77 | ||||||||
| 25–29.9 Mothers Fathers | 17 32 | ||||||||
| ≥30 Mothers Fathers | 44 37 | ||||||||
| Williams et al. (2017), USA [83] | Cross-sectional | To explore parental BMI and family behaviours associated with childhood obesity in a community sample. | 143 parents | ≤25 | 70 | 9–10 year olds | PSEAS | Underweight and healthy-weight parents monitor their child’s diet significantly more than parents with overweight and obesity (p < 0.000). There were no significant differences among parental BMI and discipline (children are disciplined for unhealthy eating), control, limit setting (boundaries with unhealthy eating), and reinforcement (praise for eating healthy foods). | Lower parental BMI is associated with a healthier home food environment. |
| ≥25 | 73 | ||||||||
| Berge et al. (2015), USA [85] | Cross-sectional | To explore food restriction and pressure to eat by parent and adolescent weight concordance and discordance. | 3252 parents | ≤25 | 1444 | Adoles-cents (mean age 14.4 years old) | CFQ subscales: Pressure to eat and Restriction | Parents with healthy-weight reported significantly higher levels of pressure to eat, compared to parents with overweight and obesity (p < 0.05). Parents with overweight/obesity reported significantly more food restriction compared to parent with healthy-weight (p < 0.05). | Use of FPPs are as a result of parental weight status and their adolescent’s weight status. |
| ≥25 | 2108 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, C.; Karasouli, E.; Shuttlewood, E.; Meyer, C. Food Parenting Practices among Parents with Overweight and Obesity: A Systematic Review. Nutrients 2018, 10, 1966. https://doi.org/10.3390/nu10121966
Patel C, Karasouli E, Shuttlewood E, Meyer C. Food Parenting Practices among Parents with Overweight and Obesity: A Systematic Review. Nutrients. 2018; 10(12):1966. https://doi.org/10.3390/nu10121966
Chicago/Turabian StylePatel, Chloe, Eleni Karasouli, Emma Shuttlewood, and Caroline Meyer. 2018. "Food Parenting Practices among Parents with Overweight and Obesity: A Systematic Review" Nutrients 10, no. 12: 1966. https://doi.org/10.3390/nu10121966
APA StylePatel, C., Karasouli, E., Shuttlewood, E., & Meyer, C. (2018). Food Parenting Practices among Parents with Overweight and Obesity: A Systematic Review. Nutrients, 10(12), 1966. https://doi.org/10.3390/nu10121966