1. Introduction
Cancer is the second-leading cause of death worldwide [
1]. Globally, the number of cancer cases and cancer deaths in 2012 was 14 million and eight million, respectively [
2]. The most frequently diagnosed cancer and cause of cancer mortality in women worldwide is breast cancer [
1]. There were an estimated 1.7 million new breast cancer cases (25.2% of the total cancer cases) and 0.5 million breast cancer deaths (14.7% of the total cancer deaths) in 2012 [
1]. In Poland, the number of cancer cases and cancer deaths has increased and was about 156 thousand and 95 thousand, respectively, in 2013 [
3]. Breast cancer is the leading cause of cancer incidence (21.9% of the total cancer cases) and the second cause of cancer deaths (13.9% of the total cancer deaths) in Polish women [
3,
4].
Breast cancer aetiology is composed of many factors, including: age, genetic, reproductive, hormonal, and lifestyle factors, of which diet is of particular interest [
1,
5]. There are many studies examining the association between dietary factors and breast cancer, and, depending on the strength of conclusions, several grades of evidence have been distinguished [
6,
7,
8,
9,
10,
11,
12,
13,
14]. Strong evidence has been obtained only for alcoholic drink consumption as a convincing and probable factor increasing the risk of post- and premenopausal breast cancer, respectively [
14]. There is limited evidence suggesting that non-starchy vegetables (for oestrogen-receptor-negative breast cancer only), foods containing carotenoids, and diets that are high in calcium might decrease the risk of breast cancer, both in pre- and postmenopausal women [
14]. Evidence of the impact of the consumption of other foods or nutrients on the risk of breast cancer is too limited to draw any conclusions [
14]. This evidence may be limited in many aspects, including the number of studies available, especially a lack of good-quality data, methodological heterogeneity between studies (e.g., adjustment for other confounders), or lack of direct association [
14].
An approach that is focused on individual foods or nutrients to assess the association with cancer does not include the complex interactions between the various components of foods [
15]. Another approach is to focus on evaluating the diet as a whole, based on dietary patterns (DPs) [
15]. Many previous studies have used
a posteriori analyses, mainly Principal Components Analysis (PCA) or Factor Analysis (FA), to identify dietary patterns [
6,
7,
8,
11,
12,
13]. Less commonly used is an
a priori approach, like the Mediterranean diet score [
16,
17,
18,
19]. There are many studies regarding the association between dietary patterns, including Mediterranean diet and breast cancer risk, however, the findings are inconsistent [
6,
7,
8,
11,
12,
13,
16,
17]. These discrepancies could result from various study designs, including the race and size of the sample, the composition of the Mediterranean diet, the use of different methods of statistical analysis to identify DPs, or the choice of another set of confounders [
20,
21,
22].
In addition to the dietary factors, breast cancer is linked to metabolic and hormone-related factors, including endogenous sex hormone levels. The contribution of some hormones, especially oestrogens and androgens [
23,
24,
25,
26] in hormone-dependent postmenopausal breast cancer pathogenesis has been well established. As for other hormones, such as progesterone or prolactin [
27,
28], there is not enough evidence for dependence in this regard. Recent data have indicated the possible contribution of cortisol in the pathogenesis of breast cancer [
29,
30]. Many complex mechanisms indicate the association of many hormones and hormones with metabolic syndrome in the pathogenesis of breast cancer, through interactions in signalling pathways involving oestrogen, insulin, growth factors, and cytokines, especially in the postmenopausal case of hormone-dependent cancers [
31,
32]. Metabolic syndrome is characterized by at least three of the following metabolic risks: visceral obesity, high blood triglycerides, low high-density lipoprotein cholesterol, high fasting glucose, and hypertension [
33]. Several studies have examined the association between metabolic syndrome and its individual components with breast cancer risk [
33,
34,
35,
36,
37,
38]. Due to possible preclinical bias and taking into account the cut-off levels of blood lipid fractions, the results have been inconclusive and they should be interpreted with caution. Therefore, there are no evident associations with breast cancer risk and the underlying mechanisms are not fully understood [
35].
Given that breast cancer is an etiologically complex disease, comprised of lifestyle, molecular, and metabolic factors, a transdisciplinary approach is the key to understanding the mechanisms linking diet, metabolic syndrome, and hormones with cancer. Previous studies have examined the association of dietary patterns [
6,
7,
8,
9,
10,
11,
12,
13,
16,
17,
18,
19,
20,
21,
22] or the individual endogenous hormone levels [
23,
24,
25,
26,
27,
28,
29,
30] or the individual metabolic syndrome components with breast cancer risk [
33,
34,
35,
36,
37,
38]. However, to our knowledge, no studies investigating all of the factors mentioned above in regard to breast cancer have been published to date.
The aim of the study was to assess the associations of dietary patterns, including ‘Polish-adapted Mediterranean Diet’ (‘Polish-aMED’) score and metabolic-hormone profiles (M-HPs) with breast cancer risk in women from north-eastern Poland. Here, we further investigated these observations by also taking into consideration many potential confounders, including hormone receptor status.
2. Materials and Methods
2.1. Ethical Approval
The study was approved by the Bioethics Committee of the Faculty of Medical Sciences, University of Warmia and Mazury in Olsztyn on 2 October 2013 (resolution no. 29/2013). All of the subjects gave their written informed consent to participate in the study, including to blood sample collection and to use clinical data for research.
2.2. Study Design and Sample Characteristics
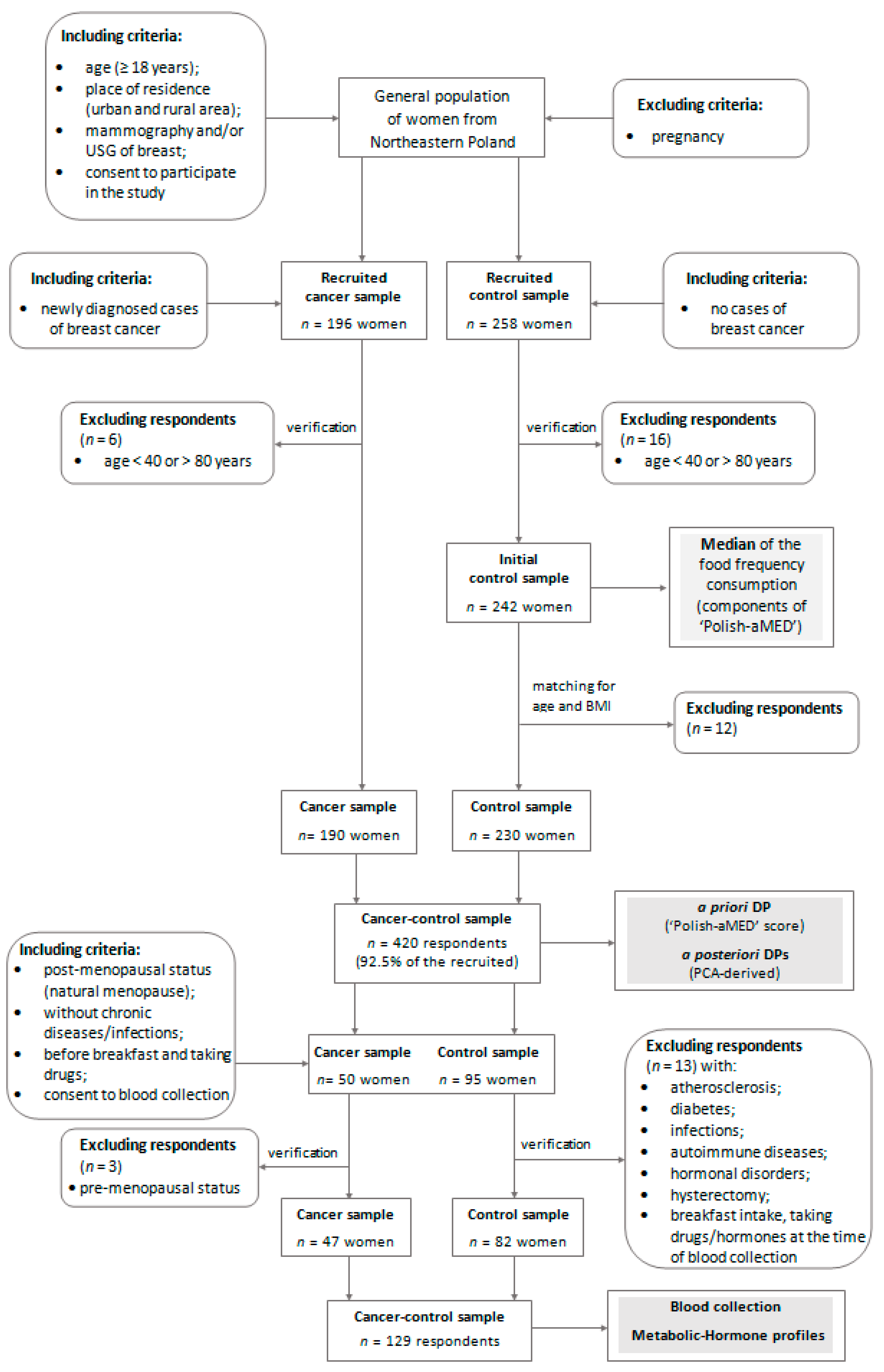
The present study was conducted in 2014–2017 among adult women from north-eastern Poland. The study protocol with a case-control design was developed. In total, the cancer-control sample involved 420 subjects, aged 40.0–79.9 (mean 59.9 SD 8.6) years.
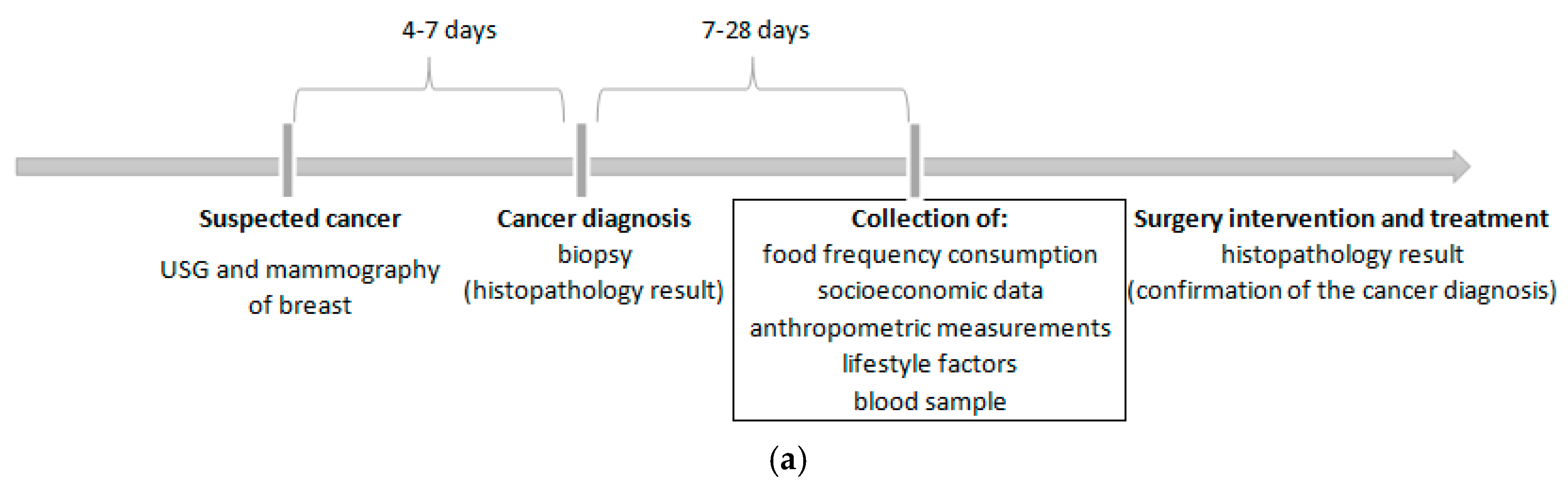
The cancer sample involved 190 women with a newly diagnosed (primary) and histologically confirmed breast cancer (invasive or in situ) identified by codes C50.0–50.9 of the International Classification of Diseases for Oncology [
39]. The time from cancer diagnosis to case recruitment in the study and data collection ranged from seven days to 28 days (
Figure 1a). Breast cancer cases were patients of the surgical oncology ward at the Ministry of Internal Affairs Hospital with the Warmia and Mazury Oncology Centre in Olsztyn. The exclusion criteria of the cancer sample collection were described previously [
40]. Briefly, cases diagnosed of other cancer or secondary breast cancer, or with benign changes, after active treatment (e.g., chemotherapy, hormone therapy, radiotherapy) or surgical intervention were not eligible for participation in the study.
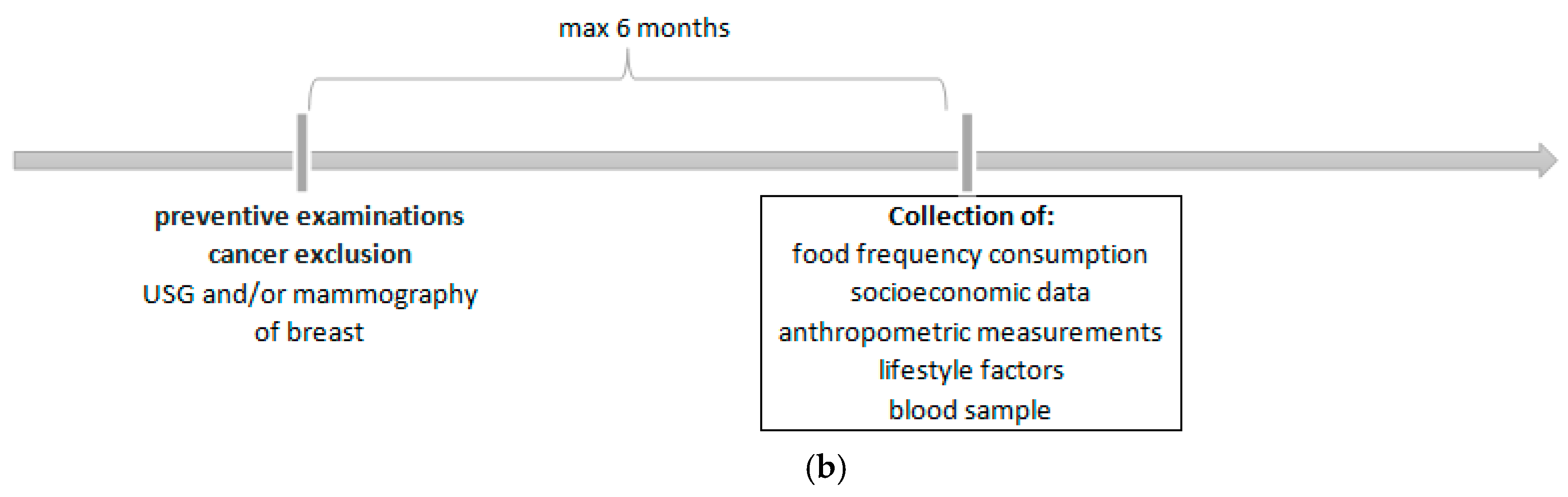
The control sample involved 230 women who were excluded from breast cancer based on mammography (MM) and/or ultrasonography (USG) of the breasts. The time from cancer exclusion to subject recruitment in the study and data collected did not exceed six months (
Figure 1b). Control subjects did not have any cancer or benign changes in their medical history. The control sample were women who visited the Centre for Prevention and Breast Diagnostics in Olsztyn and other clinics in north-eastern Poland and attended in the prophylactic screening of breast cancer. Details of the study design and the collection of cancer and control samples are shown in
Figure 2.
Breast cancer diagnosis and pathologic characteristics of the tumours were confirmed through surgery results and oncology consultant reports. Information that was related to the hormone receptor status was obtained for tumours with available results of the immunohistochemical analyses of the breast cancer tissue in the medical record (
Table 1). These data were available for 140 of the 190 breast cancer cases. In the most cases, the ductal tumours (81.4%), with positive oestrogen (ER+) and progesterone receptor status (PR+) and negative human epidermal growth factor receptor 2 (HER2-) of cancer (70.0%; Luminal A) were diagnosed.
2.3. Food Frequency Consumption and Polish-Adapted Mediterranean Diet Score
Dietary data were collected using a validated and interviewer-administered version of the 62-item Food Frequency Questionnaire (FFQ-6) [
41]. The wide application and validation results of the FFQ-6 were described elsewhere [
40]. In brief, respondents provided information about the frequency consumption of 62 food groups at least 12 months prior to participation in the study. The frequency consumption (six categories) was expressed as times/day after assigning the appropriate values as given below in
Supplementary Table S1. The consumption frequency of some food groups was summed up to form 21 food groups (
Table S1).
The ‘Polish-adapted Mediterranean Diet’ (‘Polish-aMED’) score is a Polish version of the Mediterranean diet (MED) score described by Fung et al. [
42]. In developing the ‘Polish-aMED’ score, updated evidence of breast cancer risk factors was considered [
14]. The ‘Polish-aMED’ score was calculated based on the qualitative data of the frequency of consumption (times/day) of eight selected dietary items. The set of food items included in the ‘Polish-aMED’ score, and details of its calculation are shown in the
Supplementary Table S2 and were described previously [
40]. The adherence to the ‘Polish-aMED’ score was expressed in a range from 0 to 8 points and it was considered at three levels established
a priori: low (0–2 points), average (3–5 points), and high (6–8 points).
2.4. Blood Sample Collection and Serum Biomarkers Concentration
We limited the blood sample collection to the selected 129 postmenopausal women aged 45.0–79.9 (mean 62.1 SD 8.2) years, including 47 breast cancer cases and 82 controls. Cancer and control sub-samples were chosen through a convenient and non-random selection, without a significant difference in age or BMI. Blood samples from cases were collected after breast cancer diagnosis and prior to surgery or therapy initiation (
Figure 1a). All women were free from acute medical conditions, including diabetes, and had not taken any form of hormonal supplement, including hormone replacement therapy (HRT), for the past year prior to blood sampling and at the time of blood collection. Details of including or excluding blood collection criteria are shown in
Figure 2.
At baseline, a 12 mL fasting blood sample was obtained from participants via venipuncture (antecubital venous blood) and was collected in two 6 mL pre-labelled and red top tubes (Clot Activator Tube; BD Vacutainer®, Franklin Lakes, NJ, USA) between 8:00 a.m. and 10:00 a.m., all according to standardized procedures. Blood samples were allowed to stand for 30 min at 22 °C, and were then centrifuged at 3000 rpm for 10 min at 22 °C, and the separated serum was then obtained. For all analyses, laboratory staff were blind to the case-control status of samples. All methods were fully automated with automatic calibration and performed at the Laboratory of Biochemical Studies of Nutritional Status in the Department of Human Nutrition at the University of Warmia and Mazury in Olsztyn.
Glucose, triglycerides (TG), total-cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C) concentrations were measured in serum samples using a Cobas Integra 400plus auto-analyser (Roche Diagnostics®, Basel, Switzerland), according to the manufacturer’s instructions. Glucose was measured enzymatically with the hexokinase method. Enzymatic-colorimetric tests were used to determine TG, TC, and HDL-C. The low-density lipoprotein cholesterol (LDL-C) concentrations were calculated using the Friedwald’s formula. Serum endogenous hormones: oestradiol, progesterone, prolactin, and testosterone and cortisol and insulin concentrations were measured in serum samples with electrochemiluminescence immunoassays (ECLIA) using an automated immune-analyser Cobas e411 (Roche Diagnostics®). The minimum detectable concentrations (MDC) were as follows: glucose 4.32 mg/dL, TG 8.85 mg/dL, TC 3.87 mg/dL, HDL-C 3.0 mg/dL, oestradiol 5.0 pg/mL, progesterone 0.03 ng/mL, prolactin 0.047 ng/mL, testosterone 0.025 ng/mL, insulin 0.2 µU/mL, and cortisol 0.054 µg/dL. Women with hormone concentrations below the MDC (oestradiol, n = 66; progesterone, n = 39; testosterone, n = 10) were assigned the value of the minimum level of detection.
2.5. Metabolic Syndrome Components
The definition of metabolic syndrome according to the Expert panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults [
43], with a slight modification was used. This definition requires the presence of at least three or more of the following components: waist circumference ≥ 88 cm (measured), glucose ≥ 100 mg/dL, HDL-C < 50 mg/dL, TG ≥ 150 mg/dL, and hypertension (self-declared in our study). Metabolic syndrome components were categorized according to the cut-offs that are mentioned above. For LDL/HDL, log TG/HDL, and non-HDL, the cut-offs were based on the values used in the European Guidelines on cardiovascular disease prevention (3.50, 0.50, and 145 mg/dL, respectively) [
44]. Women were categorized as: with and without metabolic syndrome and with 0 metabolic syndrome components, 1–2 components, and 3–5 components. The sum of an individual’s number of metabolic syndrome components was used to create a metabolic syndrome score (MetS; range: 0–5).
2.6. Confounders
The potential confounders were selected
a priori according to current knowledge regarding convincing and probable breast cancer risk factors [
14]. The list of confounders included the following and is described in
Table S3:
age;
BMI;
socioeconomic status;
overall physical activity;
age at menarche;
menopausal status;
oral contraceptive use;
hormone-replacement therapy use;
number of children;
smoking status;
abuse of alcohol;
vitamin/mineral supplement use;
family history of breast cancer in first- or second-degree relative; and
molecular of breast cancer subtypes.
2.7. Identification of Dietary Patterns and Metabolic-Hormone Profiles
The Principal Component Analysis (PCA) with varimax rotation was applied to identify dietary patterns (DPs) and metabolic-hormone profiles (M-HPs) [
45]. Two separate analyses were executed to identify the PCA-derived DPs or PCA-derived M-HPs. All of the input variables were standardized (to achieve mean equal 0 and standard deviation equal 1) before including them into the PCA. The input variables were: (i) the frequency of consumption of 21 food groups (expressed as times/day) to identify the DPs, and (ii) 11 metabolic syndrome components and serum hormone concentration to identify the M-HPs. In identifying the number of PCA-derived DPs or M-HPs, three criterions were considered: (i) the eigenvalues from the correlation matrix of the standardized variables > 1.0, (ii) the break point identified in the plot of eigenvalues, and (iii) the total variance explained [
45]. Rotated factor loadings > |0.30| were considered as significantly contributing to each DP or M-HP, and higher factor loading indicated a stronger association between a food group and the dietary pattern or biomarker and metabolic-hormone profile [
17,
46]. DPs and M-HPs were labelled according to the highest factor loadings for each of their components. Tertile intervals were calculated for each of the PCA-derived DP M-HPs. For each DP or M-HP, the scores were calculated as a sum of the product of the input variables (frequency of food consumption or the biomarkers values, respectively) and its factor loadings.
2.8. Statistical Analysis
Differences in baseline characteristics between cases and controls were verified with a Pearson Chi
2 test (categorical data) or a Kruskal-Wallis test (continuous data). The association between the frequency consumption of 21 food groups and the ‘Polish-aMED’ score was evaluated using Pearson’s correlation coefficients. The percentage distribution of breast cancer cases was compared by tertiles or levels of DPs and M-HPs using the Pearson Chi
2 test with Yates’ correction as necessary. All serum biomarker concentrations were log-transformed to normalize their variable distributions and Student’s
t-test was then used to compare them between cases and controls. Logistic regression analysis was used to assess the associations of DPs or M-HPs with breast cancer risk. The odds ratio (OR) and 95% confidence interval (95% CI) were calculated. The references (OR = 1.00) were the control sample and the bottom tertile or lowest level of each DP or M-HP. Four models were created: unadjusted model, model 1—adjusted for the potential confounders mentioned above, model 2 and model 3—fully-adjusted models for the same confounders included in model 1 and for M-HPs Score or DPs Score, respectively (excluding the modelled variable from confounders set). The level of significance of the odds ratio was verified with the Wald’s test [
45]. The statistical analysis was performed using STATISTICA software (version 10.0 PL; StatSoft Inc., Tulsa, OK, USA; StatSoft, Krakow, Poland). A
p-value < 0.05 was considered to be statistically significant.
5. Conclusions
The study revealed that pro-healthy diet is insufficient to reduce the risk of breast cancer in peri- and postmenopausal women. These findings provide interesting insights into the strong harmful effect of the high adherence to the ‘High-Hormone’ profile and the ‘Non-Healthy’ dietary pattern on breast cancer risk, independently of many potential confounders, among women from north-eastern Poland.
The results may improve the understanding of the complex aetiology of breast cancer, related to diet, hormone, and metabolic association and may prove useful in establishing primary preventive strategies. In the prevention of breast cancer, special attention should be paid to decreasing adherence to the ‘Non-Healthy’ pattern by reducing the consumption of highly processed food, foods with a high content of sugar and animal fat. There is also a need to monitor the concentration of multiple sex hormones in the context of breast cancer. Further, large prospective studies are needed to confirm the results on the role of diet, hormones, and metabolic syndrome in the aetiology of breast cancer, stratified by menopausal and hormone receptor status.

 ,
, 




{kind=link}
{kind=link}
{kind=link}