Association between Sarcopenia and Metabolic Syndrome in Middle-Aged and Older Non-Obese Adults: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
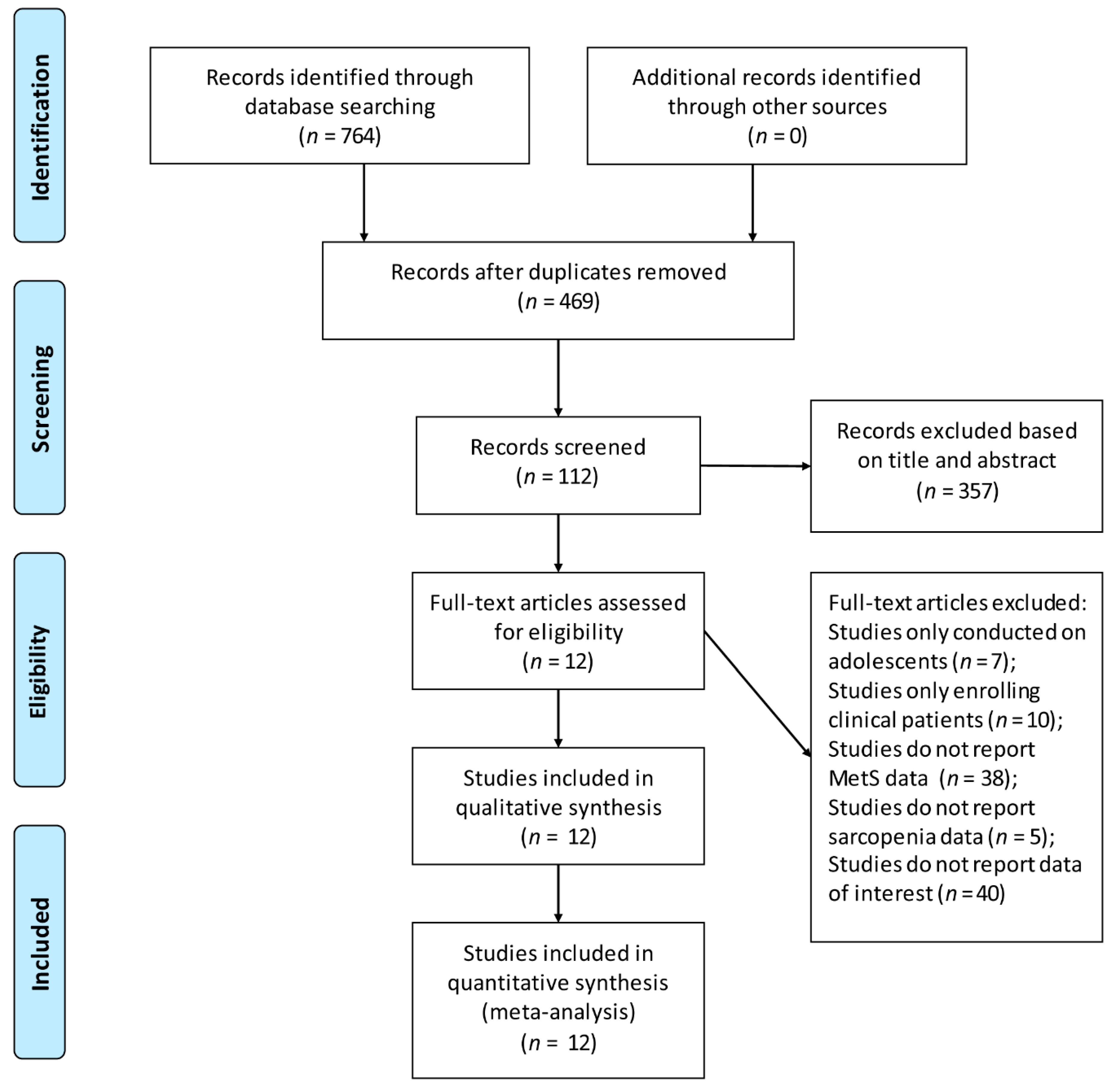
3.1. Literature Search
3.2. Study and Participants’ Characteristics
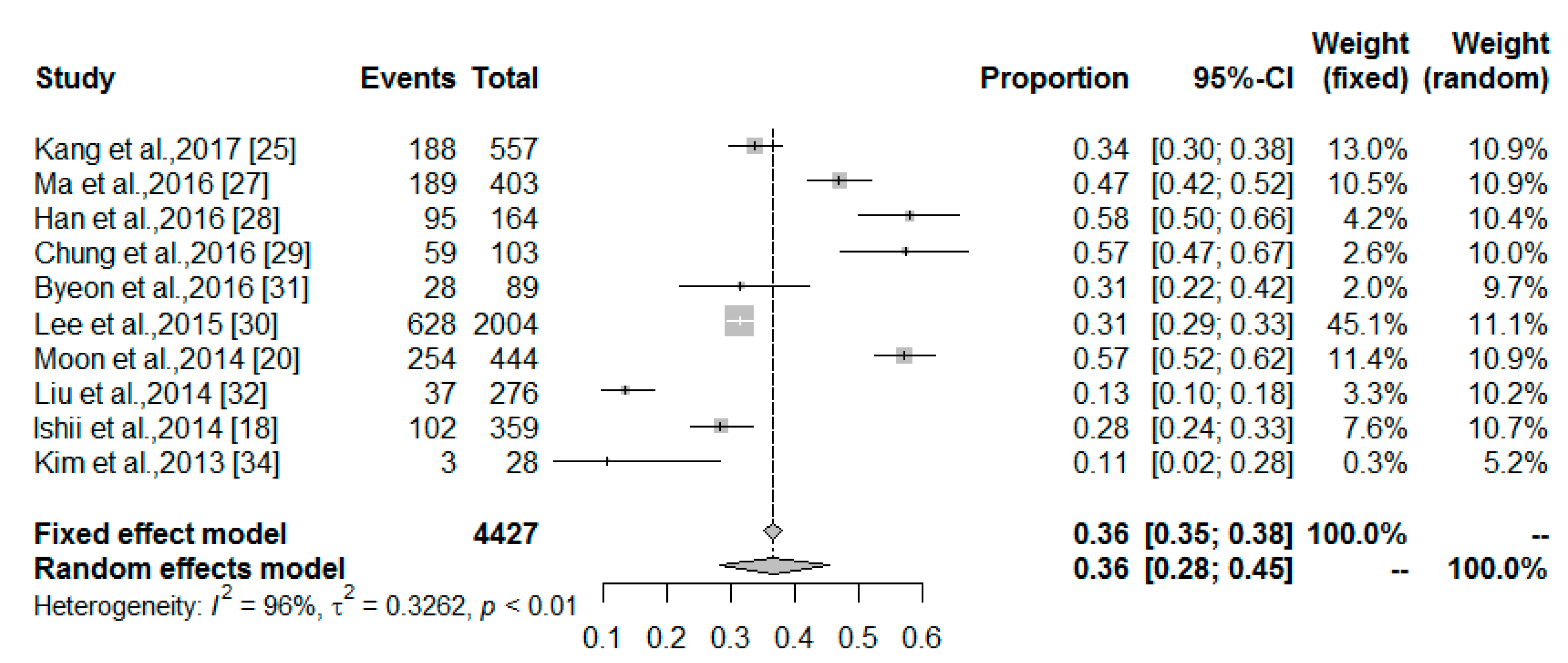
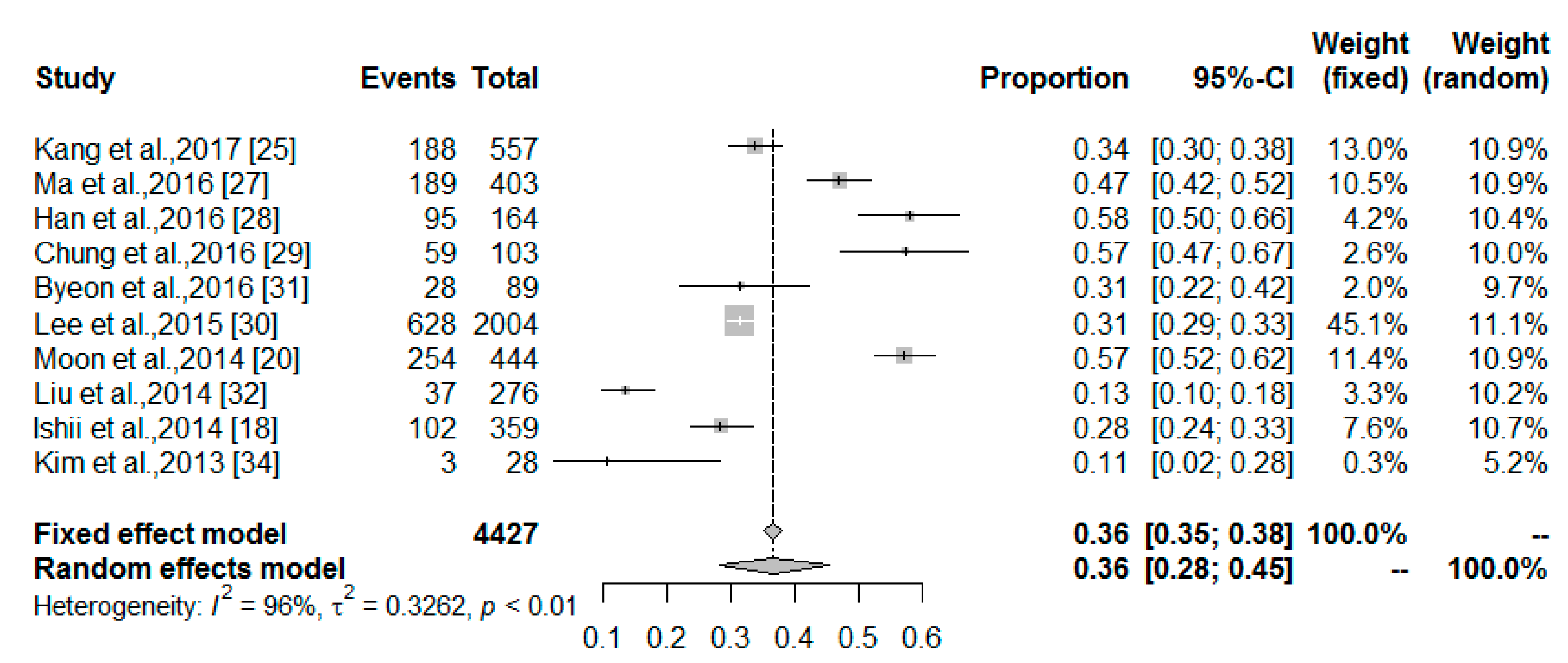
3.3. The MetS Prevalence among Middle-Aged and Older Non-Obese Adults with Sarcopenia
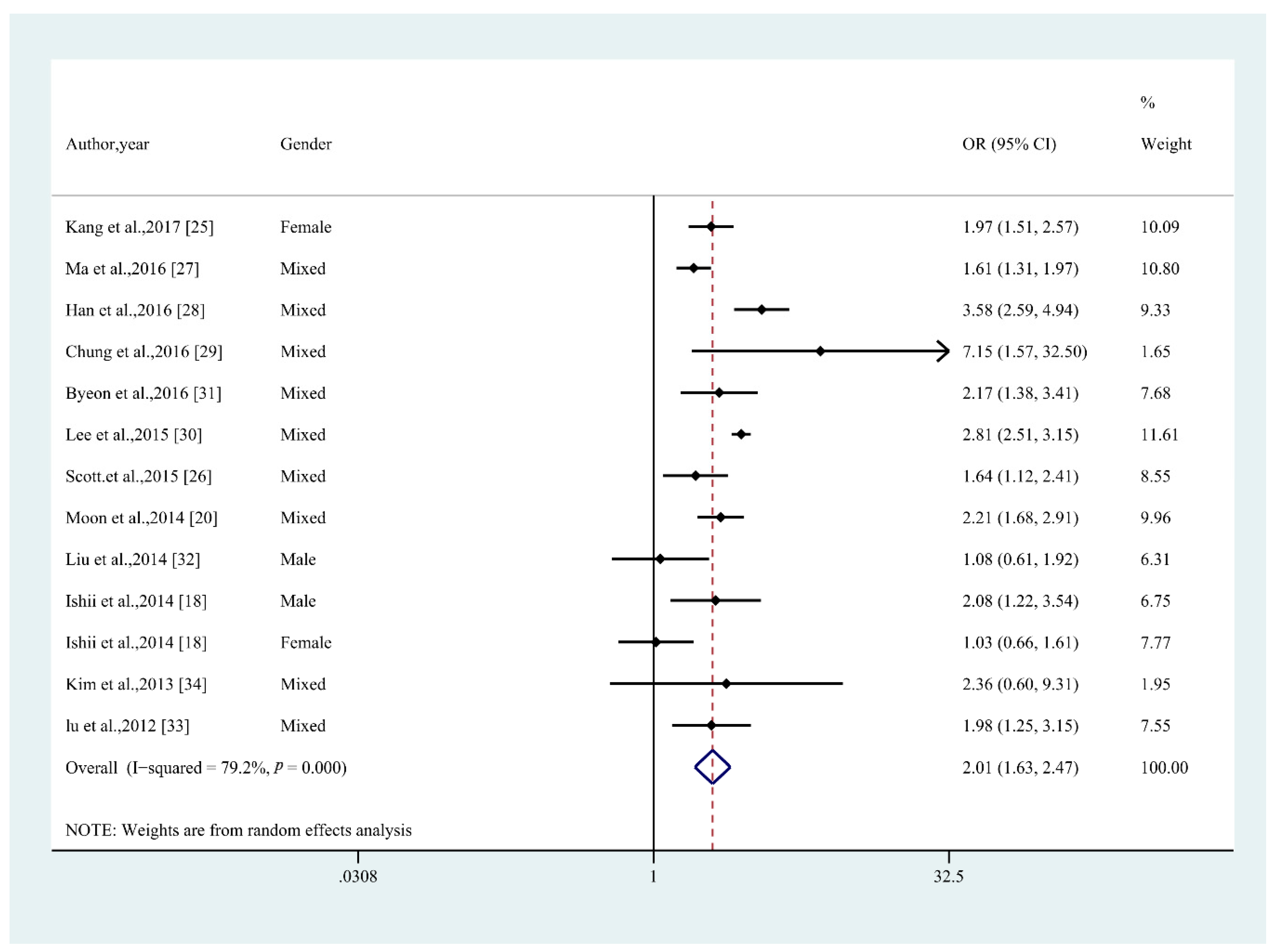
3.4. Odds Ratio of MetS in Middle-Aged and Older Non-Obese Adults with Sarcopenia
4. Discussion
4.1. Potential Biological Mechanisms
4.2. Directions for Further Research
4.3. Strengths and Limitations
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European working group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Kan, G.A.V.; Andrieu, S.; Bauer, J.; Breuille, D. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L. The predictive value of the EWGSOP definition of sarcopenia: Results from the InCHIANTI study. J. Gerontol. 2016, 71, 259–264. [Google Scholar]
- Boutin, R.D.; Yao, L.; Canter, R.J.; Lenchik, L. Sarcopenia: Current concepts and imaging implications. Am. J. Roentgenol. 2015, 205, W255–W266. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.P.; Syddall, H.E.; Jameson, K.; Robinson, S.; Denison, H.; Roberts, H.C.; Edwards, M.; Dennison, E.; Cooper, C.; Sayer, A.A. Prevalence of sarcopenia in community-dwelling older people in the UK using the European working group on sarcopenia in older people (EWGSOP) definition: Findings from the Hertfordshire Cohort Study (HCS). Age Ageing 2013, 42, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Smoliner, C.; Sieber, C.C.; Wirth, R. Prevalence of sarcopenia in geriatric hospitalized patients. Clin. Nutr. 2014, 15, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Haffner, S.M.; Valdez, R.A.; Hazuda, H.P.; Mitchell, B.D.; Morales, P.A.; Stern, M.P. Prospective analysis of the insulin-resistance syndrome (syndrome X). Diabetes 1992, 41, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsén, B.; Lahti, K.; Nissén, M.; Taskinen, M.R.; Groop, L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, M.; Liu, J.; Bahsas, F.B.; Menotti, A. Syndrome X and mortality: A population-based study. Risk factor and life expectancy research group. Am. J. Epidemiol. 1998, 148, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Shin, H.; Song, J.H.; Kwak, S.H.; Kang, S.M.; Ji, W.Y.; Choi, S.H.; Cho, S.I.; Park, K.S.; Hong, K.L. Increasing prevalence of metabolic syndrome in Korea: The Korean national health and nutrition examination survey for 1998–2007. Diabetes Care 2011, 34, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Janssen, I.; Heymsfield, S.B. Metabolic syndrome in normal-weight Americans: New definition of the metabolically obese, normal-weight individual. Diabetes Care 2004, 27, 2222–2228. [Google Scholar] [CrossRef] [PubMed]
- Waters, D.L.; Baumgartner, R.N. Sarcopenia and obesity. Clin. Geriatr. Med. 2011, 27, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Abbatecola, A.M.; Paolisso, G.; Fattoretti, P.; Evans, W.; Fiore, V.; Dicioccio, L.; Lattanzio, F. Discovering pathways of sarcopenia in older adults: A role for insulin resistance on mitochondria dysfunction. J. Nutr. Health Aging 2011, 15, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Khamseh, M.E.; Malek, M.; Aghili, R.; Emami, Z. Sarcopenia and diabetes: Pathogenesis and consequences. Br. J. Diabetes Vasc. Dis. 2011, 11, 230–234. [Google Scholar] [CrossRef]
- Baek, S.J.; Nam, G.E.; Han, K.D.; Choi, S.W.; Jung, S.W.; Bok, A.R.; Kim, Y.H.; Lee, K.S.; Han, B.D.; Kim, D.H. Sarcopenia and sarcopenic obesity and their association with dyslipidemia in Korean elderly men: The 2008–2010 Korea national health and nutrition examination survey. J. Endocrinol. Investig. 2014, 37, 247–260. [Google Scholar] [CrossRef] [PubMed]
- Doğan, M.; Karadag, B.; Ozyigit, T.; Kayaoglu, S.; Ozturk, A.; Altuntas, Y. Correlations between sarcopenia and hypertensive target organ damage in a Turkish cohort. Acta Clin. Belg. 2012, 67, 328–332. [Google Scholar] [PubMed]
- Ishii, S.; Tanaka, T.; Akishita, M.; Ouchi, Y.; Tuji, T.; Iijima, K.; Kikutani, T.; Higashiguchi, T.; Ishikawa-Takata, K.; Obuchi, S.P.; et al. Metabolic syndrome, sarcopenia and role of sex and age: Cross-sectional analysis of Kashiwa cohort study. PLoS ONE 2014, 9, e112718. [Google Scholar] [CrossRef] [PubMed]
- Sanada, K.; Iemitsu, M.; Murakami, H.; Gando, Y.; Kawano, H.; Kawakami, R.; Tabata, I.; Miyachi, M. Adverse effects of coexistence of sarcopenia and metabolic syndrome in Japanese women. Eur. J. Clin. Nutr. 2012, 66, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.S. Low skeletal muscle mass is associated with insulin resistance, diabetes, and metabolic syndrome in the Korean population: The Korea National Health and Nutrition Examination Survey (KNHANES) 2009–2010. Endocr. J. 2014, 61, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K. Adipokines, myokines and cardiovascular disease. Circ. J. 2009, 73, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- Stang, A. Critical evaluation of the newcastle-ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Herzog, R.; Álvarezpasquin, M.J.; Díaz, C.; Barrio, J.L.D.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.Y.; Lim, G.E.; Kim, Y.K.; Kim, H.W.; Lee, K.; Park, T.J.; Kim, J. Association between sarcopenic obesity and metabolic syndrome in postmenopausal women: A cross-sectional study based on the Korean national health and nutritional examination surveys from 2008 to 2011. J. Bone Metab. 2017, 24, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Park, M.S.; Kim, T.N.; Ryu, J.Y.; Hong, H.C.; Yoo, H.J.; Baik, S.H.; Jones, G.; Choi, K.M. Associations of low muscle mass and the metabolic syndrome in Caucasian and Asian middle-aged and older adults. J. Nutr. Health Aging 2016, 20, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Hwang, S.-J.; McMahon, G.M.; Curhan, G.C.; McLean, R.R.; Murabito, J.M.; Fox, C.S. Mid-adulthood cardiometabolic risk factor profiles of sarcopenic obesity. Obesity 2016, 24, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Lee, Y.-H.; Kim, G.; Kim, S.R.; Lee, B.-W.; Kang, E.S.; Ahn, C.W.; Cha, B.-S. Sarcopenia is associated with albuminuria independently of hypertension and diabetes: KNHANES 2008–2011. Metabolism 2016, 65, 1531–1540. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.M.; Hyun, M.H.; Lee, E.; Seo, H.S. Novel effects of sarcopenic osteoarthritis on metabolic syndrome, insulin resistance, osteoporosis, and bone fracture: The national survey. Osteoporos. Int. 2016, 27, 2447–2457. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-H.; Jung, K.S.; Kim, S.U.; Yoon, H.-J.; Yun, Y.J.; Lee, B.-W.; Kang, E.S.; Han, K.-H.; Lee, H.C.; Cha, B.-S. Sarcopaenia is associated with NAFLD independently of obesity and insulin resistance: Nationwide surveys (KNHANES 2008–2011). J. Hepatol. 2015, 63, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Byeon, C.-H.; Kang, K.-Y.; Kang, S.-H.; Bae, E.-J. Sarcopenia is associated with Framingham risk score in the Korean population: Korean National Health and Nutrition Examination Survey (KNHANES) 2010–2011. J. Geriatr. Cardiol. 2015, 12, 366–372. [Google Scholar] [PubMed]
- Liu, L.K.; Chen, L.Y.; Yeh, K.P.; Lin, M.H.; Hwang, A.C.; Peng, L.N.; Chen, L.K. Sarcopenia, but not sarcopenic obesity, predicts mortality for older old men: A 3-year prospective cohort study. J. Clin. Gerontol. Geriatr. 2014, 5, 42–46. [Google Scholar] [CrossRef]
- Lu, C.-W.; Yang, K.-C.; Chang, H.-H.; Lee, L.-T.; Chen, C.-Y.; Huang, K.-C. Sarcopenic obesity is closely associated with metabolic syndrome. Obes. Res. Clin. Pract. 2013, 7, E301–E307. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.N.; Park, M.S.; Lim, K.I.; Choi, H.Y.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Choi, H.; Baik, S.H.; et al. Relationships between sarcopenic obesity and insulin resistance, inflammation, and vitamin d status: The Korean sarcopenic obesity study. Clin. Endocrinol. 2013, 78, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Suliga, E.; Kozieł, D.; Głuszek, S. Prevalence of metabolic syndrome in normal weight individuals. Ann. Agric. Environ. Med. 2016, 23, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, X.; Han, X.; Yang, K.; Liu, B.; Li, Y.; Wu, P.; Liu, X.; Yu, K.; Dai, X. Serum creatinine levels and risk of metabolic syndrome in a middle-aged and older Chinese population. Clin. Chim. Acta 2015, 440, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R.; Moulin, P.; Sérusclat, A.; Nony, P.; Bonnet, F. A comparison of the NCEP-ATPIII, IDF and AHA/NHLBI metabolic syndrome definitions with relation to early carotid atherosclerosis in subjects with hypercholesterolemia or at risk of CVD: Evidence for sex-specific differences. Atherosclerosis 2007, 190, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; Mclean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M. The fnih sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Krause, M. Exercise, Sarcopenia and Immunosenescence. Diyhpl Us 2003. Available online: http://back-in-business-physiotherapy.com/images/files/exercise_sracopenia_and_immunsenescence.pdf (accessed on 15 March 2018).
- Guarner, V.; Rubioruiz, M.E. Low-grade systemic inflammation connects aging, metabolic syndrome and cardiovascular disease. Interdiscip. Top. Gerontol. 2015, 40, 99–106. [Google Scholar] [PubMed]
- Buford, T.W.; Anton, S.D.; Judge, A.R.; Marzetti, E.; Wohlgemuth, S.E.; Carter, C.S.; Leeuwenburgh, C.; Pahor, M.; Manini, T.M. Models of accelerated sarcopenia: Critical pieces for solving the puzzle of age-related muscle atrophy. Ageing Res. Rev. 2010, 9, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.J. Skeletal muscle loss: Cachexia, sarcopenia, and inactivity. Am. J. Clin. Nutr. 2010, 91, 1123S–1127S. [Google Scholar] [CrossRef] [PubMed]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Xi, B.; Xue, J.; Huai, P.; Zhang, M.; Li, J. Association between leisure time physical activity and metabolic syndrome: A meta-analysis of prospective cohort studies. Endocrine 2014, 46, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Kapilevich, L.; Orlov, S.; Kabachkova, A. Myokines as a promising marker of metabolic disorders and physical activity. In Proceedings of the 5th International Scientific Conference “New Operational Technologies”, Tomsk, Russia, 29–30 September 2015; pp. 2195–2201. [Google Scholar]
- Cleasby, M.E.; Jamieson, P.M.; Atherton, P.J. Insulin resistance and sarcopenia: Mechanistic links between common co-morbidities. J. Endocrinol. 2016, 229, R67–R81. [Google Scholar] [CrossRef] [PubMed]
- Bosello, O.; Zamboni, M. Visceral obesity and metabolic syndrome. Obes. Rev. 2000, 1, 47–56. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country, Setting | Study Design | Cohort Size (Female %) | Average Age, Year | Definition of Sarcopenia | Definition of MetS | Adjustments | Quality Assessment |
|---|---|---|---|---|---|---|---|---|
| Kang et al., 2017 [25] | Korea, community-dwelling | Cross-sectional | 2574 (100%) | Sarcopenia: 61.9 ± 0.5 Control: 61.6 ± 0.3 | Skeletal muscle mass measured by DXA; ASM/Wt was less than 1 standard deviation below the mean of the young reference group | AHA/NHLBI IDF/ | Menopausal age, any female sex hormonal treatment, drinking status, smoking status, physical activity, chronic disease, and economic status | |
| Ma et al., 2016 [27] | Korea, community-dwelling | Cross-sectional | 709 (53.9%) | Sarcopenia: 71.6 ± 8.0 Control: 67.7±7.0 | Skeletal muscle mass evaluated by 24-h UC method; 24-h UC ≥ 12.33 mmol/day for men and ≥10.43 mmol/day for women | NCEP-ATPIII | N/A | |
| Han et al., 2016 [28] | United states, community-dwelling | Cross-sectional | 2326 (54.4%) | Sarcopenia: 66.0 ± 12.6 Control: 51.0 ± 15.8 | Skeletal muscle mass measured by DXA; ASM/BMI < 0.789 for men and <0.512 for women | NCEP-ATPIII | N/A | |
| Chung et al., 2016 [29] | Korea, community-dwelling | Cross-sectional | 1377 (42.6%) | Sarcopenia: 62.7 ± 1.1 Control: 59.6 ± 0.3 | Skeletal muscle mass measured by DXA; (ASM/Ht2)/Wt % < 28.9% for men and <22.4% for women | NCEP-ATPIII | Age, sex, household income, current smoking, alcohol consumption, vitamin D, hypertension and dyslipidemia | |
| Byeon et al., 2015 [31] | Korea, community-dwelling | Cross-sectional | 5001 (N/A) | Sarcopenia: 56.4 ± 2.0 Control: 43.6 ± 0.4 | Skeletal muscle mass measured by DXA; ASM/Wt % < 26.88% for men and 21.02% for women | NCEP-ATPIII | N/A | |
| Lee et al., 2015 [30] | Korea, community-dwelling | Cross-sectional | 10,479 (65%) | Sarcopenia: 56.7 ± 16.3 Control: 47.9 ± 16.8 | Skeletal muscle mass measured by DXA; ASM/Wt % < 32.2% for men and <25.5% for women | NCEP-ATPIII | N/A | |
| Scott et al., 2015 [26] | Korea & Australian community-dwelling | Cross-sectional | 1381 (54.7%) | N/A | Skeletal muscle mass measured by DXA; ASM/BMI < 0.789 for men and <0.512 for women | NCEP-ATPIII | Age and gender | |
| Moon et al., 2014 [20] | Korea, community-dwelling | Cross-sectional | 10,432 (56.3%) | Sarcopenia: 59.8 ± 14.3 Control: 48.3 ± 15.5 | Skeletal muscle mass measured by DXA; ASM/Wt % < 26.98% for men and 21.14% for women | NCEP-ATPIII | Age, sex, region, smoking, alcohol consumption, exercise, and family income level | |
| Ishii et al., 2014 [18] | Japan, community-dwelling | Cross-sectional | 1971 (50.4%) | Sarcopenia: 77.1 ± 5.8 Control: 72.0 ± 5.0 | Skeletal muscle mass measured by BIA; SMI < 7.0 kg/m2 for men and <5.8 kg/m2 for women; muscle strength < 30 kg for men and <20 kg for women; gait speed < 1.26 m/s for each sex | NCEP-ATPIII | Age, height, weight, physical activity and food intake. | |
| Liu et al., 2014 [32] | Taiwan (China), community-dwelling | Cohort study, baseline data | 444 (0%) | Sarcopenia: 83.1 ± 4.8 Control: 82.0 ± 4.5 | Handgrip strength < 22.5 kg | NCEP-ATPIII | N/A | |
| Kim et al., 2013 [34] | Korea, community-dwelling | Cross-sectional | 214 (80.4%) | Sarcopenia: 51.0 ± 10.6 Control: 44.2 ± 14.9 | Skeletal muscle mass measured by DXA; ASM/Wt % was less than 1 standard deviation below the mean of the young reference group | NCEP-ATPIII | N/A | |
| Lu et al., 2012 [33] | Taiwan (China), community-dwelling | Cross-sectional | 420 (72.9%) | Sarcopenia: 61.1 ± 9.6 Control: 64.4 ± 10.3 | Skeletal muscle mass measured by BIA; ASM/Wt % < 37% for man and <27.6% for women | NCEP-ATPIII | Age, gender, current smoking, current drinking, vegetarian diet and physical activity |
| Analysis | Number of Studies | Number of Participants | Meta-Analysis | Between Group p Value | I2 |
|---|---|---|---|---|---|
| Prevalence of MetS in non-obese middle-aged and older people with sarcopenia | |||||
| Prevalence (95% CI) | |||||
| All studies (D + L) | 10 | 4427 | 0.36 (0.28–0.45) | 96% | |
| Continent | 0.0364 | ||||
| Asian | 9 | 4024 | 0.35 (0.26–0.45) | 96% | |
| North America | 1 | 403 | 0.47 (0.42–0.52) | - | |
| Definition of MetS | 0.6102 | ||||
| NCEP-ATPIII | 9 | 3870 | 0.37 (0.27–0.47) | 97% | |
| AHA/NHLBI/IDF | 1 | 557 | 0.34 (0.30–0.38) | - | |
| Sarcopenia measure | <0.0001 | ||||
| DXA | 7 | 3389 | 0.41(0.30–0.52) | 96% | |
| 24 h urinary creatinine | 1 | 403 | 0.47 (0.42–0.52) | - | |
| BIA/HGS/GS | 1 | 359 | 0.28 (0.24–0.33) | - | |
| HGS | 1 | 276 | 0.13 (0.10–0.18) | - | |
| Cohort size (n) | 0.5333 | ||||
| n ≥ 200 | 6 | 4043 | 0.34 (0.25–0.44) | 90% | |
| n < 200 | 4 | 384 | 0.40 (0.24–0.59) | 97% | |
| Prevalence of MetS in non-obese middle-aged and older people without sarcopenia | |||||
| Prevalence (95% CI) | |||||
| All studies (D + L) | 10 | 31,154 | 0.23 (0.18–0.29) | 99% | |
| Continent | <0.0001 | ||||
| Asian | 9 | 30,848 | 0.21 (0.16–0.26) | 99% | |
| North America | 1 | 306 | 0.48 (0.42–0.53) | - | |
| Definition of MetS | 0.7922 | ||||
| NCEP-ATPIII | 9 | 31,154 | 0.23 (0.18–0.29) | 99% | |
| AHA/NHLBI/IDF | 1 | 2071 | 0.23 (0.22–0.25) | - | |
| Sarcopenia measure | <0.0001 | ||||
| DXA | 7 | 29,068 | 0.20 (0.16–0.25) | 99% | |
| 24-h urine | 1 | 306 | 0.48 (0.42–0.53) | - | |
| BIA/HGS/GS | 1 | 1612 | 0.38 (0.36–0.40) | - | |
| HGS | 1 | 168 | 0.12 (0.08–0.18) | - | |
| Cohort size (n) | 0.0081 | ||||
| n ≥ 200 | 8 | 30,800 | 0.27 (0.21–0.34) | 99% | |
| n < 200 | 2 | 354 | 0.08 (0.03–0.19) | 84% | |
| Heterogeneity | ||||
|---|---|---|---|---|
| Subgroups | Number of Studies | OR (95% CI) | I2 (%) | Pheterogeneit |
| All studies | 13 | 2.01 (1.63–2.47) | 79.2 | <0.001 |
| Adjustment | ||||
| Adjusted | 7 | 1.85 (1.48–2.32) | 50.4 | 0.060 |
| Unadjusted | 6 | 2.16 (1.54–3.03) | 86.0 | <0.001 |
| Continent | ||||
| Asian | 11 | 2.12 (1.69–2.65) | 74.8 | <0.001 |
| North America | 1 | 1.61 (1.31–1.97) | - | - |
| Asian & Oceania | 1 | 1.64 (1.12–2.41) | - | - |
| Definition of MetS | ||||
| NCEP-ATPIII | 12 | 2.01 (1.59–2.53) | 80.4 | <0.001 |
| AHA/NHLBI/IDF | 1 | 1.97 (1.51–2.57) | - | - |
| Sarcopenia measurement | ||||
| DXA | 8 | 2.41 (1.98–2.94) | 63.1 | 0.008 |
| BIA/HGS/GS | 2 | 1.44 (0.72–2.87) | 74.6 | 0.047 |
| 24 h urinary creatinine | 1 | 1.61 (1.31–1.97) | - | - |
| BIA | 1 | 1.98 (1.25–3.15) | - | - |
| HGS | 1 | 1.08 (0.61–1.92) | - | - |
| Cohort size | ||||
| n ≥ 1000 | 7 | 2.41 (1.96–2.97) | 68.4 | 0.004 |
| n < 1000 | 6 | 1.53 (1.22–1.93) | 32.8 | 0.190 |
| Non-obese evaluation | ||||
| Divided by BMI | 11 | 1.92 (1.53–.41) | 78.9 | <0.001 |
| Adjustment for BMI | 2 | 2.01 (1.63–2.47) | 89.1 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Lin, S.; Gao, T.; Zhong, F.; Cai, J.; Sun, Y.; Ma, A. Association between Sarcopenia and Metabolic Syndrome in Middle-Aged and Older Non-Obese Adults: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 364. https://doi.org/10.3390/nu10030364
Zhang H, Lin S, Gao T, Zhong F, Cai J, Sun Y, Ma A. Association between Sarcopenia and Metabolic Syndrome in Middle-Aged and Older Non-Obese Adults: A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(3):364. https://doi.org/10.3390/nu10030364
Chicago/Turabian StyleZhang, Huaqi, Song Lin, Tianlin Gao, Feng Zhong, Jing Cai, Yongye Sun, and Aiguo Ma. 2018. "Association between Sarcopenia and Metabolic Syndrome in Middle-Aged and Older Non-Obese Adults: A Systematic Review and Meta-Analysis" Nutrients 10, no. 3: 364. https://doi.org/10.3390/nu10030364