1. Introduction
In previous centuries, sugar was used as a commodity currency and represented wealth [
1,
2]. In this way, it was common to use high amounts of sugar in the food preparations to demonstrate possessions, and this influenced the taste preferences as a result of experiential learning that was passed down the generations [
1,
3]. On the other hand, sugar is traditionally used as preservative of foods, just as salt [
1].
Nowadays, despite some studies having shown that sugar intake is decreasing [
4,
5,
6,
7], globally a high sugar intake is often seen [
4,
8,
9,
10,
11,
12,
13,
14,
15,
16]. In epidemiological studies developed around the world, total sugar was observed ranging from 14.5 to 21.9% of total energy intake (%TE) in adults of both genders assessed in Italy [
9] and individuals of both genders, 18–34 years, assessed in National Health and Nutritional Examination Survey III in the United States of America [
4]. Furthermore, for added sugar ranges from 7.2 to 21.4%TE were observed in men, 18–70 years, assessed in Norkost 3, Norway [
4], and individuals of both genders, 18–34 years, assessed in the National Health and Nutritional Examination Survey in the United States of America [
4].
With the worldwide increase in non-communicable disease (NCD) epidemics, and the known association of sugar intake with health implications [
14,
17,
18], the global health agenda has been drawn to public health policies with the purpose of awareness in the population and the private sector to the emerging need to reduce, mainly, added sugar consumption [
19]. More recently, the World Health Organization (WHO) has highlighted the consumption of free sugar, referred to as the sum of added sugar, sugars naturally present in honey, syrups and fruit juices and fruit juice concentrates, and whose consumption has been associated with poor dietary quality, besides higher risk of developing dental caries, obesity, and NCD [
19]. However, despite some authors having attempted to show the extent of free sugar intake [
10,
16,
20], the assessment is globally limited because of the lack of databases on free sugar in the national tables of nutritional composition, and by the lack of a universal standardized definition [
20,
21,
22].
Despite the difficulty of evaluating added sugar, and particularly free sugar, the reporting of sugar intake can guide adoption of public policies, and it is suggested that this information must be monitored more rigorously, especially in countries whose data from sugar intake are scarce, which includes most Latin American countries, a region of the south American continent characterized by a conglomerate of developing countries that experience a dual scenario referred to as nutritional transition. In addition, it is important to identify factors such as gender, socioeconomic level, and age that may influence dietary habits and contribute to a higher sugar intake [
8,
23,
24,
25]. This will facilitate the planning of action strategies targeting the most vulnerable groups.
Given this background, this study aimed to assess the total and added sugar intake in a representative sample of Latin American countries, and to verify the adherence to the WHO recommendations, considering gender, socioeconomic level (SEL), and age range.
2. Materials and Methods
This survey was approved by the Western Institutional Review Board (#20140605), by the ethics review boards of the participating institutions, and is registered at Clinical Trials (#NCT02226627). Written informed consent/assent was obtained from all individuals before commencement of the study. Participant confidentiality for the pooled data was maintained via the use of numeric identification codes rather than names. All data transfer was done with a secure file sharing system.
2.1. Study Population
This study examined data from the Latin American Study of Nutrition and Health (‘Estudio Latinoamericano de Nutrición y Salud’; ELANS), a household-based multi-national cross-sectional population-based survey, conducted from March 2014 to December 2015 in eight Latin American countries: Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru, and Venezuela.
Sample recruitment was performed using a random complex, multistage sampling. Individuals (
n = 9218; aged 15 to 65 years) were stratified by geographical location (only urban areas), gender, age, and SEL. Only urban areas were included considering that almost all countries included in ELANS have at least 80–90% of the population living in urban areas. The sample size was calculated using a confidence level of 95% and a sample error of 3.49% at a 5% significance level and survey design effect of 1.75. More details can be seen in Fisberg et al. [
26].
Pregnant and lactating women (in the first six months postpartum), individuals with major physical or mental impairments that affect food intake or physical activity, individuals outside of age range 15–65 years, adolescents without assent or consent of a parent or legal guardian, individuals living in institutions, and individuals unable to read were not included in the sample.
2.2. Data Entry and Databases
Trained interviewers visited the selected households twice. At the first visit, the ELANS’ purpose was explained, and the eligible individuals signed the informed consent/assent form. Thereafter, a structured questionnaire was used to collect information about demographics (age, gender, years of education, number of people in the household, race/ethnicity, marital status, and number of years living in the country) and SEL. A 24-h dietary recall (24-HR) was applied, and anthropometric measurements were assessed. At the second visit, a second 24-HR and a beverage intake questionnaire were answered.
Gender was classified as male or female. Age on the date of interview was considered in complete years, and the individuals were stratified into four age groups: 15–19, 20–34, 35–49, and 50–65 years. SEL was classified into high, medium, and low strata, and these were based on the national indexes used in each country, as described in Fisberg et al. [
26].
The 24-HR were collected in nonconsecutive days, including weekend days, by trained interviewers who used a structured script elaborated in paper form to be used in the home interviews. The United States Department of Agriculture’s (USDA) five-step multiple-pass method [
27] was followed during the interviews to guide the individuals and to facilitate in recalling the foods and beverages consumed. This method is composed by the following steps: 1. quick list—the interviewee lists, without interruption, all foods and beverages consumed the previous day; 2. forgotten foods list—the interviewer repeats the list of foods and beverages mentioned by the interviewee to identify foods that may have been forgotten; 3. time and occasion—the interviewee elaborates on the time he/she consumed foods and on what he/she considers to be a meal; 4. detail cycle—the interviewee provides descriptions and amounts of each food reported, and the interviewer reviews each occasion and the interval between occasions; 5. final review probe—the interviewer repeats all information with the intention of collecting data on additional foods not remembered earlier. The data were analyzed using the Nutrition Data System for Research software version 2014 (NDS-R), a dietary assessment tool developed by the Nutrition Coordinating Center of University of Minnesota, Minneapolis, MN, whose steps to 24-HR data insertion follow the five-steps multiple pass method. Further details about the food matching standardized procedures can be seen elsewhere [
28].
2.3. Total and Added Sugar Intakes
Information on total and added sugar intakes were obtained from the 24-HR analysis using the NDS-R, that includes in the 2014 version the USDA’s database, data from scientific literature, food manufactures, and foreign food composition tables, including Latin American Food Composition Table. In this software database, information on total sugar is captured and analyzed as being composed of the individual intrinsic and extrinsic monosaccharides (glucose, fructose and galactose) and disaccharides (sucrose, lactose and maltose); and added sugar (by total sugars) by those sugars and syrups added to foods during food preparation or commercial food processing (white sugar (sucrose), brown sugar, powdered sugar, honey, molasses, pancake syrup, corn syrups, high fructose corn syrups, invert sugar, invert syrup, malt extract, malt syrup, fructose, glucose (dextrose), galactose, and lactose), excluding mono- and disaccharides occurring naturally in foods, such as lactose in milk or fructose in fruit [
29].
When necessary, sugar and added sugar content were corrected to approximate the local reality using a data correction routine made to be used in the Stata software (version 13.0; StataCorp LP, College Station, TX, USA), and a corrected database was generated.
The prevalence of individual excessive added sugar intake was determined using the WHO’s recommendations intake of free sugars—below 10%TE—and the WHO’s conditional recommendations on intake of free sugars—below 5%TE [
19].
2.4. Statistical Analyses
Usual dietary intake of sugars was estimated using the Multiple Source Method, a web-based tool developed by researchers at the European Prospective Investigation into Cancer and Nutrition (EPIC) for estimating usual dietary intakes of nutrients and foods consumed by populations and individuals, available at
https://msm.dife.de/. The method is accomplished in three steps which requires at least two days of dietary measurements on a random subsample of the target population. First, the probability of nutrient/food intake for each individual is estimated using logistic regression with random effects (probability model). Second, the usual amount of nutrient/food intake in days of consumption is estimated using linear regression, also with random effects (quantity model). Finally, the individual’s usual nutrient/food intake is calculated by multiplying the result of the probability of nutrient/food intake obtained in the first step with the usual amount of nutrient/food intake obtained in the second step [
30].
Total and added sugar intake were presented as means, standard deviation, percentiles, %TE, and percentage of carbohydrate contribution (%CHO). The percentage of individuals with excessive added sugar intake was shown as columns in the figures. Stata software was used to perform these statistical analyses, and data were stratified by gender, SEL, and age groups, and considered in the set of the countries assessed in ELANS and individually. The proportions of sugar adequacy were compared using the Mann–Whitney or Kruskal–Wallis test, after the normality had been tested by the Skewness and Kurtosis test. The level of significance was established at 5%.
3. Results
The mean total sugar intake for all countries was 99.4 g/day, which accounted for 20.1% of total energy (%TE) and contributed to 36.7% of the total carbohydrates consumed (
Table 1). Of total sugar intake, 65.9% was coming from added sugar intake, which contributed to 13.2%TE (65.5 g of added sugar/day; 23.9% of the total carbohydrates;
Table 2). Comparing the countries, in absolute terms (g/day), Argentina, Colombia, and Peru had the highest values of total sugar intake. In these three countries, as well as Costa Rica and Venezuela, there was a greater contribution of total sugar intake to the energy intake in relative terms (%TE) compared to the other countries. On the other hand, Brazil and Chile had the lowest values of total sugar intake in absolute terms, and Brazil and Ecuador in relative terms (
Table 1). With respect to added sugar intake, the values in Argentina were considerably higher than the other countries in absolute (g/day) and relative terms (%TE and % of sugar from total carbohydrates; %CHO), whereas the lowest values were observed in Chile in absolute terms, and in Ecuador in relative terms (%TE and %CHO) (
Table 2).
In general, men had consumed larger amounts of total and added sugar in absolute terms (mean g/day), a finding that was consistent among the countries when assessed separately (
Table 3 and
Table 4). However, in relative terms, the %TE and %CHO showed that women had the highest values in all countries with respect to total sugar intake (
Table 3) and in most countries with respect to added sugar intake (
Table 4).
Considering the SEL, the total sugar intake in absolute and relative terms of all countries was greater among individuals in the high strata compared to the others (
Table 5); however, there were no differences in added sugar intake among the strata of SEL (
Table 6). When the countries were considered independently, the profile observed for all countries was maintained for the majority of the countries (
Table 5 and
Table 6).
According to age groups, total and added sugar intakes showed a decrease with advancing age, markedly in the absolute terms (
Table 7 and
Table 8). However, when the amount of total sugar intake was expressed relative to total energy intake (%TE), the differences among age groups were observed only for Brazil and Chile. For added sugar intake, more countries showed differences, being similar between groups for Colombia, Ecuador, Peru, and Venezuela (
Table 7 and
Table 8).
As shown by means of %TE from added sugar in
Table 1,
Table 2,
Table 3,
Table 4,
Table 5,
Table 6,
Table 7 and
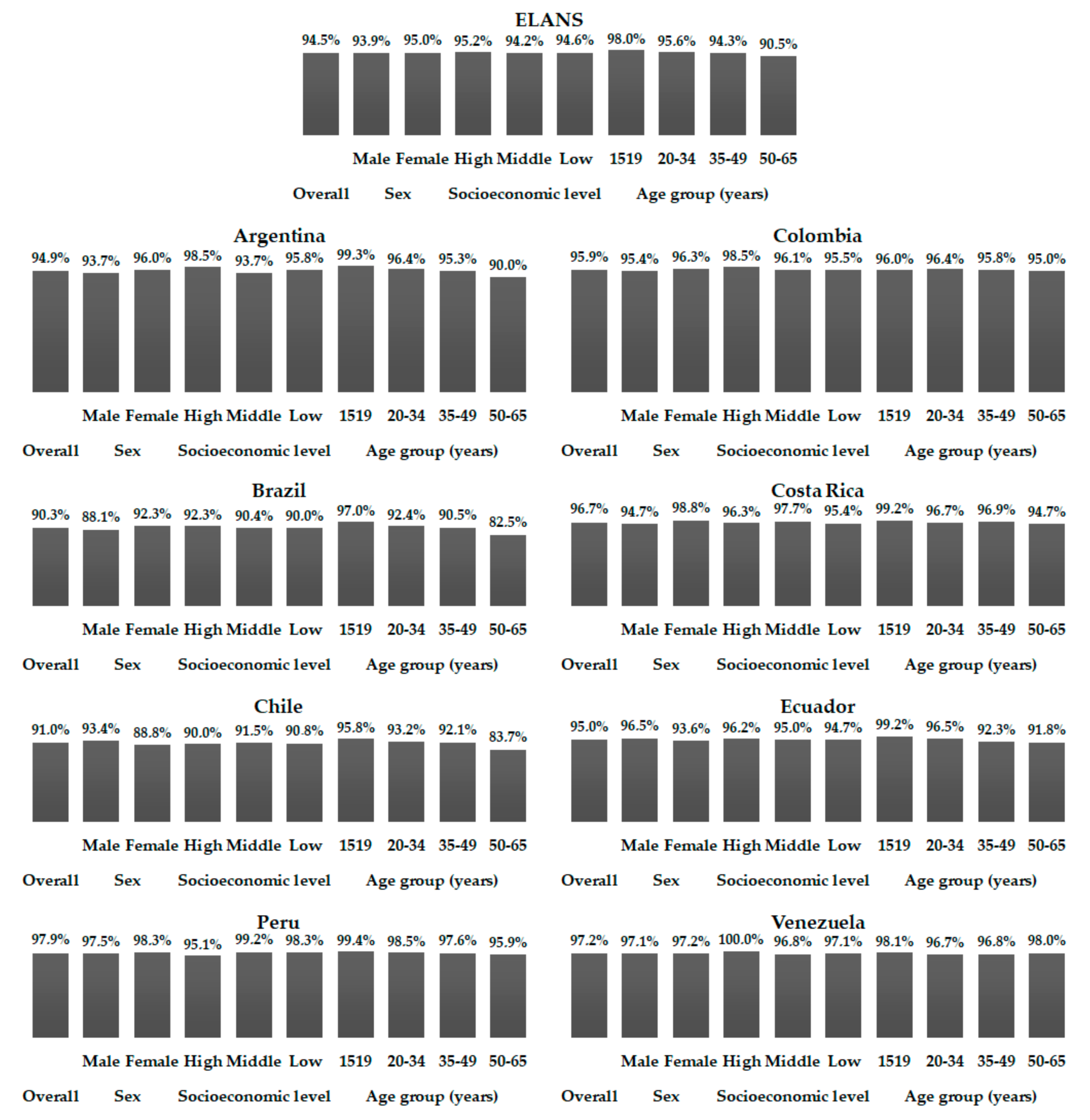
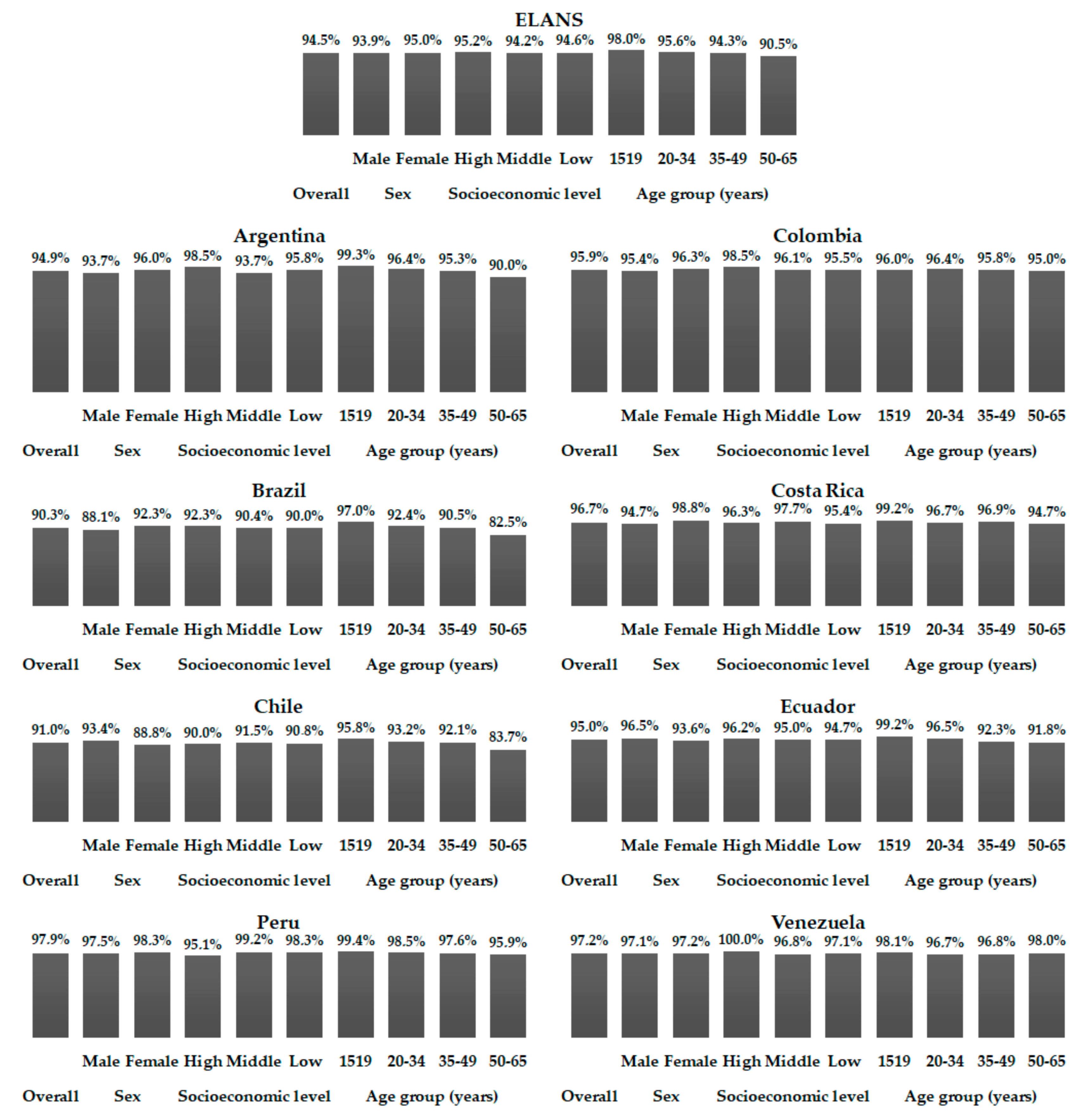
Table 8, a high percentage of individuals had excessive added sugar intake (
Figure 1 and
Figure 2). Considering the 10%TE recommendation, approximately 70% of all individuals showed added sugar intake above 10%TE, ranging from 49.1% in Ecuador to 79.6% in Costa Rica. Considering the stratifications performed (gender, SEL, and age), minimal differences were observed in relation to the data presented in the tables among the countries independently (
Figure 1). When the 5%TE recommendation was considered, the percentage of excessive added sugar intake leapt to more than 90%, varying among countries from 90.3% in Brazil to 97.9% in Peru, and again showed only slight differences to the general standard when countries were analyzed individually (
Figure 2).
4. Discussion
This is the first multinational nutrition survey of a representative sample of Latin American countries. It showed a considerable percentage of individuals with a high intake of total and, mainly, added sugar in the countries assessed in ELANS. In addition, in most countries assessed, total sugar intake, in particular, has been influenced by gender, SEL and age.
Sugars occur naturally in foods and is one source of calories which provide energy for the bodily functions [
6]. Mainly added sugars overconsumption is frequently associated with reduced diet quality [
31,
32,
33], and it has an important pathophysiological role, predisposing to critical cardiometabolic effects, including weight gain, diabetes, and cardiovascular disease outcomes [
17,
34,
35,
36,
37] which negatively impact on the prevalence of disease and mortality, disability-adjusted life years and costs averted [
38]. Although some countries have shown that sugar intake is decreasing [
4,
5,
6,
7], the total amounts consumed are still high considering the current recommendations, as demonstrated in the present study. There is a discussion about which type of sugar is unhealthier, intrinsic or added sugars [
39,
40,
41], and for this reason its consumption should be used as a sentinel, or if the concern should not be sugar itself but the set of unbalanced factors associated with high sugar intake [
39,
40,
42] is an important reason why sugar intake should be monitored.
On the other hand, an absence of a standardized global definition for added and free sugars ends up failing on recommendations for sugar intake and makes it difficult to compare the intake of sugars among the studies. Some countries and societies have suggested several recommendations based on their own definition for added/free sugar; however, the WHO’s recommendations are the most widely used, and for this reason we opted to use it. Furthermore, Latin American countries do not have a quantitative recommendation for total or added sugar intakes. WHO’s recommendation for free sugar is relied upon in terms of the effects triggered in adults and children from reduced and increased free sugar intake [
36].
Despite the problem of non-standardization, among the countries assessed in ELANS, Argentina was shown to be most vulnerable to high sugar intakes, obtaining the highest values (absolute and relative) compared to the other countries assessed in ELANS [
6,
7,
9] as well as the US adult population [
12,
43] that is known to have markedly high sugars diets. The other countries assessed in ELANS presented absolute and relative values of sugars intake that, on average, are similar to those observed in the other countries.
These observations highlight the importance of understanding what is different in Argentina. Perhaps the food that contributes to sugar intake may be the answer. Analysis of sugars contributors is already being done and will be presented in another manuscript in a close future. On the other hand, particular characteristics of the population, such as an affinity for sweet taste, and food environment can have an influence in this [
3]. It is known that the culture of sugar consumption in Latin American countries is not a novel tendency but a historical fact having been passed on over the generations, and possibly more strongly in Argentina. In addition, factors such as the composition of gut microbiota should be considered, as it has been demonstrated that bacterial composition may exert an influence on the host’s eating behavior by mechanisms independent of taste and flavor which can predispose to craving for sugar foods, for example [
44].
When the prevalence high sugar intake by individuals was assessed, Brazil and Chile showed the lowest and Argentina the highest for added sugar only. The high prevalence was maintained only for total sugar. For other perspectives, Argentina basically presented the same behavior when the sample of the countries assessed in ELANS was stratified by some factors.
In present study, as demonstrated elsewhere [
7,
9,
23,
24], in absolute terms men showed higher sugar intakes than women; however, in relative terms this observation was the opposite, which reflects the greater energy intake by men inherent in their constitution that demands greater energy needs. In contrast, higher relative values in women demonstrate that they are consuming a more nutritionally unbalanced diet, at least as far as sugar intake is concerned, and it is still shown in studies investigating sugar-intake trends that the decline in sugar intake is lower in women compared to men [
7,
9].
Further, in present study when it is observed the total of the countries the difference in SEL were observed only for total sugar intake, being the higher intake observed among those with the highest socioeconomic strata. This finding was the opposite seen in US adults studied by Park et al. [
23]. This can reflect different tax incentives to decrease added sugar consumption, which permits the acquisition of items that have more sugar by individuals of distinct SEL. Nevertheless, this hypothesis cannot be automatically generalized to Latin American countries. Sugar sources of added sugar in Latin America could be part of regional foods; however, this should be investigated in future studies.
With respect to the influence of age, following the trend observed in other studies [
8,
23,
24,
43], younger individuals were seen to be more vulnerable to higher total and added sugars intake, whose consumption decreased over their lifespan. This can be explained by their immaturity in the choice of their foods, and largely by influence of advertisements. The study of food sources might lend greater insights about these findings and provide clear answers to propose a prudent strategy to promote health benefits for the groups that should be monitored more closely.
It is important to emphasize that the WHO’s recommendation was established for free sugar intake [
19]; however, due to the difficulty in quantifying it, this recommendation is used as a reference for added sugar, as used in the present study, and recognized as a limitation. Additionally, it is necessary to recognize that the evaluation of dietary intake is subject to random and systematic errors, despite the care taken to minimize them, as presented elsewhere [
26,
28], and of the adjustment for intra-individual variation. Nevertheless, despite these limitations, the present study provides useful information to be used to develop public policies that may help in healthier food intake and improved quality of life.

 ,
, 


{kind=link}
{kind=link}