The Association of Dietary Fiber Intake with Cardiometabolic Risk in Four Countries across the Epidemiologic Transition

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Ethics Approval
2.2. Dietary Intake
2.3. Biochemical Measures
2.4. Physical Activity Measurement
2.5. Clinical Outcomes
- Waist circumference >102 cm in males and >88 cm in females;
- Elevated blood pressure (≥130/85 mm Hg), or receiving treatment;
- Hypertriglyceridemia (≥150 mg/dL), or receiving treatment;
- Low high-density lipoprotein (HDL) cholesterol (<40 mg/dL in males and <50 mg/dL in females), or receiving treatment; and
- Elevated fasting plasma glucose (≥100 mg/dL), or receiving treatment.
2.6. Statistical Analyses
3. Results
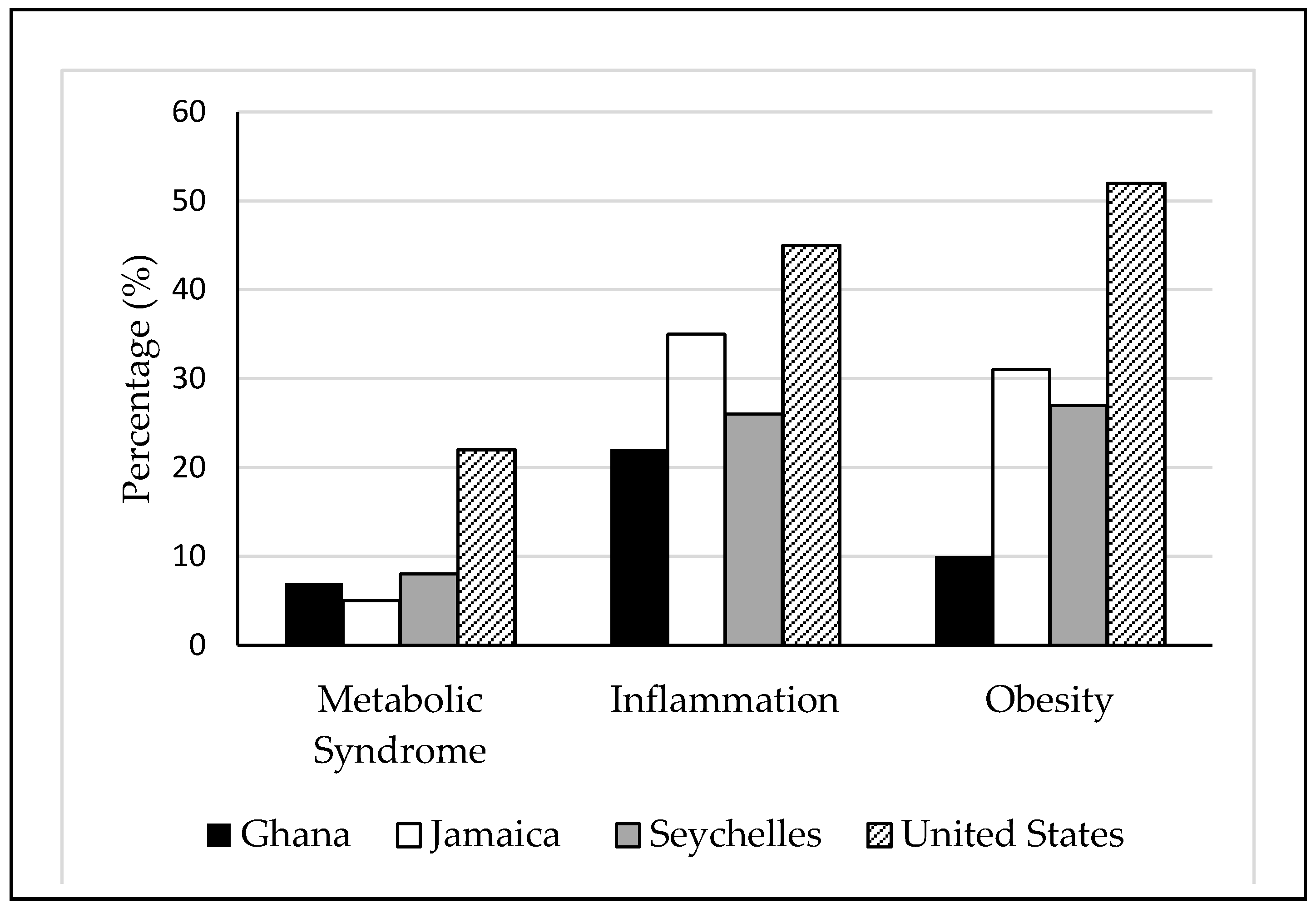
3.1. Cardiometabolic Risk Factors across the Epidemiologic Transition
3.2. The Association of Dietary Fiber Intake on Cardiometabolic Risk Factors across the Epidemiologic Transition
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P.Z.; Magliano, D.J.; Herman, W.H.; Shaw, J.E. Diabetes: A 21st century challenge. Lancet Diabetes Endocrinol. 2014, 2, 56–64. [Google Scholar] [CrossRef]
- Geiss, L.S.; Kirtland, K.; Lin, J.; Shrestha, S.; Thompson, T.; Albright, A.; Gregg, E.W. Changes in diagnosed diabetes, obesity, and physical inactivity prevalence in US counties, 2004–2012. PLoS ONE 2017, 12, e0173428. [Google Scholar] [CrossRef] [PubMed]
- Durazo-Arvizu, R.A.; Luke, A.; Cooper, R.S.; Cao, G.; Dugas, L.; Adeyemo, A.; Adeyemo, A.; Boyne, M.; Forrester, T. Rapid increases in obesity in Jamaica, compared to Nigeria and the United States. BMC Public Health 2008, 8, 133. [Google Scholar] [CrossRef] [PubMed]
- Eckert, S.; Kohler, S. Urbanization and health in developing countries: A systematic review. World Health Popul. 2014, 15, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Ford, N.D.; Patel, S.A.; Narayan, K.M. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Zimmet, P.Z.; Shaw, J.E. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; Grundy, S.M., Ed.; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Albers, R.; Antoine, J.M.; Blum, S.; Bourdet-Sicard, R.; Ferns, G.A.; Folkerts, G.; Friedmann, P.S.; Frost, G.S.; Guarner, F.; et al. Inflammatory disease processes and interactions with nutrition. Br. J. Nutr. 2009, 101 (Suppl. 1), S1–S45. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Cunningham, K.; Esposito, K.; Jönsson, L.S.; Kolb, H.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br. J. Nutr. 2011, 106 (Suppl. 3), S5–S78. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Albers, R.; Bosco, N.; Bourdet-Sicard, R.; Haller, D.; Holgate, S.T.; Jönsson, L.S.; Latulippe, M.E.; Marcos, A.; et al. A consideration of biomarkers to be used for evaluation of inflammation in human nutritional studies. Br. J. Nutr. 2013, 109 (Suppl. 1), S1–S34. [Google Scholar] [CrossRef] [PubMed]
- Suganami, T.; Tanimoto-Koyama, K.; Nishida, J.; Itoh, M.; Yuan, X.; Mizuarai, S.; Kotani, H.; Yamaoka, S.; Miyake, K.; Aoe, S.; et al. Role of the Toll-like receptor 4/NF-kappaB pathway in saturated fatty acid-induced inflammatory changes in the interaction between adipocytes and macrophages. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 84–91. [Google Scholar] [CrossRef] [PubMed]
- King, D.E.; Egan, B.M.; Woolson, R.F.; Mainous, A.G., 3rd; Al-Solaiman, Y.; Jesri, A. Effect of a high-fiber diet vs a fiber-supplemented diet on C-reactive protein level. Arch. Intern. Med. 2007, 167, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Kruger, H.S. Associations of serum C-reactive protein with physical activity, fitness and fatness in South African adolescents. Cardiovasc. J. Afr. 2010, 21, 309–310. [Google Scholar] [PubMed]
- Ridker, P.M.; Buring, J.E.; Cook, N.R.; Rifai, N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: An 8-year follow-up of 14,719 initially healthy American women. Circulation 2003, 107, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J.; Group IDFETFC. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Dugas, L.R.; Forrester, T.E.; Plange-Rhule, J.; Bovet, P.; Lambert, E.V.; Durazo-Arvizu, R.A.; Cao, G.; Cooper, R.S.; Khatib, R.; Tonino, L.; et al. Cardiovascular risk status of Afro-origin populations across the spectrum of economic development: Findings from the Modeling the Epidemiologic Transition Study. BMC Public Health 2017, 17, 438. [Google Scholar] [CrossRef] [PubMed]
- WHO. The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Reddy, K.S.; Yusuf, S. Emerging epidemic of cardiovascular disease in developing countries. Circulation 1998, 97, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, T.A.; Bitton, A.; Anand, S.; Abrahams-Gessel, S.; Murphy, A. Growing epidemic of coronary heart disease in low- and middle-income countries. Curr. Probl. Cardiol. 2010, 35, 72–115. [Google Scholar] [CrossRef] [PubMed]
- Lang, T. The new globalisation, food and health: Is public health receiving its due emphasis? J. Epidemiol. Commun. Health 1998, 52, 538–539. [Google Scholar] [CrossRef]
- Tucker, L.A.; Thomas, K.S. Increasing total fiber intake reduces risk of weight and fat gains in women. J. Nutr. 2009, 139, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Montonen, J.; Knekt, P.; Jarvinen, R.; Aromaa, A.; Reunanen, A. Whole-grain and fiber intake and the incidence of type 2 diabetes. Am. J. Clin. Nutr. 2003, 77, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S.; Pereira, M.A.; Kroenke, C.H.; Hilner, J.E.; Van Horn, L.; Slattery, M.L. Dietary fiber, weight gain, and cardiovascular disease risk factors in young adults. JAMA 1999, 282, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Galisteo, M.; Duarte, J.; Zarzuelo, A. Effects of dietary fibers on disturbances clustered in the metabolic syndrome. J. Nutr. Biochem. 2008, 19, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Luke, A.; Bovet, P.; Forrester, T.E.; Lambert, E.V.; Plange-Rhule, J.; Schoeller, D.A.; Dugas, L.R.; Durazo-Arvizu, R.A.; Shoham, D.; Cooper, R.S.; et al. Protocol for the modeling the epidemiologic transition study: A longitudinal observational study of energy balance and change in body weight, diabetes and cardiovascular disease risk. BMC Public Health 2012, 11, 927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barro, R.J.; Lee, J.W. A New Data Set of Educational Attainment in the World, 1950–2010; The National Bureau of Economic Research: Cambridge, MA, USA, 2011; Available online: http://www.nber.org/papers/w15902 (accessed on 15 May 2018).
- Carriquiry, A.L. Estimation of usual intake distributions of nutrients and foods. J. Nutr. 2003, 133, 601S–608S. [Google Scholar] [CrossRef] [PubMed]
- Carriquiry, A.L.; Fuller, W.A.; Goyeneche, J.J.; Dodd, K.W. Estimation of the Usual Intake Distributions of Ratios of Dietary Components; Center for Agricultural and Rural Development, Iowa State University: Ames, IA, USA, 1995. [Google Scholar]
- Guenther, P.M.; Kott, P.S.; Carriquiry, A.L. Development of an approach for estimating usual nutrient intake distributions at the population level. J. Nutr. 1997, 127, 1106–1112. [Google Scholar] [CrossRef] [PubMed]
- Steyn, N.P.; Nel, J.H.; Parker, W.A.; Ayah, R.; Mbithe, D. Dietary, social, and environmental determinants of obesity in Kenyan women. Scand. J Public Health 2011, 39, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (U.S.). Panel on Macronutrients. II. Institute of Medicine (U.S.). Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. QP141.D529 2005. Available online: https://www.nal.usda.gov/sites/default/files/fnic_uploads/energy_full_report.pdf (accessed on 15 April 2018).
- Luke, A.; Bovet, P.; Plange-Rhule, J.; Forrester, T.E.; Lambert, E.V.; Schoeller, D.A.; Dugas, L.R.; Durazo-Arvizu, R.A.; Shoham, D.A.; Cao, G.; et al. A mixed ecologic-cohort comparison of physical activity & weight among young adults from five populations of African origin. BMC Public Health 2014, 14, 397. [Google Scholar]
- Dugas, L.R.; Bovet, P.; Forrester, T.E.; Lambert, E.V.; Plange-Rhule, J.; Durazo-Arvizu, R.A.; Shoham, D.; Kroff, J.; Cao, G.; Cooper, R.S.; et al. Comparisons of intensity-duration patterns of physical activity in the US, Jamaica and 3 African countries. BMC Public Health 2014, 14, 882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SAS Programs for Analyzing NHANES 2003–2004 Accelerometer Data. 2014. Available online: http://appliedresearch.cancer.gov/nhanes_pam/ (accessed on 25 July 2014).
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- National Cholesterol Education Program; Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Giles, W.H.; Mokdad, A.H.; Myers, G.L. Distribution and correlates of C-reactive protein concentrations among adult US women. Clin. Chem. 2004, 50, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Rifai, N.; Ridker, P.M. Population distributions of C-reactive protein in apparently healthy men and women in the United States: Implication for clinical interpretation. Clin. Chem. 2003, 49, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: Executive summary. Am. J. Clin. Nutr. 1998, 68, 899–917. [Google Scholar]
- Popkin, B.M. Synthesis and implications: China’s nutrition transition in the context of changes across other low- and middle-income countries. Obes. Rev. 2014, 15 (Suppl. 1), 60–67. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Slining, M.M. New dynamics in global obesity facing low- and middle-income countries. Obes. Rev. 2013, 14 (Suppl. 2), 11–20. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Gordon-Larsen, P. The nutrition transition: Worldwide obesity dynamics and their determinants. Int. J. Obes. Relat. Metab. Disord. 2004, 28 (Suppl. 3), S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Paeratakul, S.; Zhai, F.; Ge, K. A review of dietary and environmental correlates of obesity with emphasis on developing countries. Obes. Res. 1995, 3 (Suppl. 2), 145s–153s. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th Edition. December 2015. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 15 April 2018).
- Grooms, K.N.; Ommerborn, M.J.; Pham, D.Q.; Djousse, L.; Clark, C.R. Dietary fiber intake and cardiometabolic risks among US adults, NHANES 1999–2010. Am. J. Med. 2013, 126, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Steyn, N.P.; McHiza, Z.J. Obesity and the nutrition transition in Sub-Saharan Africa. Ann. N. Y. Acad. Sci. 2014, 311, 88–101. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Ghana | Jamaica | Seychelles | United States | |
|---|---|---|---|---|
| N = 489 | N = 402 | N = 484 | N = 444 | |
| Demographics | ||||
| Female (n, %) | 287 (58.7) | 244 (60.7) | 261 (53.9) | 228 (51.4) |
| Age (year) | 34.2 ± 6.8 | 34.4 ± 6.1 | 36.2 ± 5.6 | 35.2 ± 6.3 |
| Anthropometrics | ||||
| Weight (kg) | 63.5 ± 11.5 | 75.9 ± 17.1 | 75.8 ± 17.0 | 91.9 ± 24.2 |
| Height (cm) | 162.6 ± 8.2 | 169.6 ± 9.2 | 167.1 ± 8.8 | 169.9 ± 9.0 |
| Body Mass Index (kg/m2) | 24.1 ± 4.5 | 26.6 ± 6.4 | 27.1 ± 5.6 | 31.9 ± 8.4 |
| Waist Circumference (cm) | 81.2 ± 12.1 | 86.1 ± 14.2 | 88.7 ± 12.0 | 99.6 ± 20.4 |
| Systolic Blood Pressure (mmHg) | 113.9 ± 14.8 | 118.4 ± 14.2 | 116.2 ± 14.7 | 122.6 ± 16.3 |
| Diastolic Blood Pressure (mmHg) | 67.1 ± 11.3 | 71.7 ± 11.3 | 73.0 ± 10.7 | 80.5 ± 12.8 |
| Biochemical Measures | ||||
| Cholesterol (mg/dL) | 161.4 ± 35.3 | 162.8 ± 33.9 | 170.9 ± 35.4 | 181.1 ± 38.4 |
| HDL-C (mg/dL) Ratio total cholesterol to HDL | 46.0 ± 14.4 3.8 ± 1.7 | 46.5 ± 12.1 3.7 ± 1.0 | 47.7 ± 12.8 3.9 ± 1.2 | 50.8 ± 14.6 3.8 ± 1.1 |
| Triglycerides (mg/dL) | 82.0 ± 40.3 | 73.2 ± 36.3 | 79.8 ± 60.6 | 97.3 ± 57.4 |
| Blood glucose (mg/dL) | 100.3 ± 12.2 | 93.1 ± 9.4 | 100.9 ± 29.5 | 103.5 ± 35.5 |
| CRP (mg/dL) | 4.7 ± 13.3 | 4.2 ± 6.3 | 3.1 ± 4.5 | 6.0 ± 11.0 |
| Lifestyle Habits | ||||
| Smoker or ex-smoker (n, %) Moderate-to-vigorous PA (min/day) | 13 (2.8) 34.3 ± 22.6 | 101 (25.1) 23.3 ± 19.3 | 95 (19.6) 28.9 ± 20.9 | 205 (46.3) 23.3 ± 28.9 |
| Ghana | Jamaica | Seychelles | United States | |
|---|---|---|---|---|
| N = 489 | N = 402 | N = 484 | N = 444 | |
| Energy (kcal) % Energy from fat % Energy from saturated fat % Energy from monounsaturated fat % Energy from polyunsaturated fat | 1849 ± 495.7 21.6 ± 9.2 7.1 ± 4.1 8.2 ± 3.7 4.6 ± 2.5 | 1930 ± 590.5 25.7 ± 6.6 9.4 ± 4.1 8.6 ± 2.6 5.5 ± 2.1 | 1844 ± 590.9 28.4 ± 7.7 8.4 ± 2.9 8.9 ± 3.0 8.6 ± 3.4 | 2294 ± 889.3 36.6 ± 7.0 11.8 ± 2.9 13.6 ± 3.1 7.9 ± 2.8 |
| % Energy from carbohydrates % Energy from protein | 65.9 ± 10.4 11.9 ± 4.0 | 58.6 ± 8.4 14.7 ± 3.9 | 51.3 ± 9.4 18.4 ± 4.7 | 45.8 ± 9.4 15.6 ± 4.1 |
| Meeting 14 g/1000 kcal (n, %) | 208 (42.5) | 35 (8.7) | 28 (5.8) | 14 (3.2) |
| Dietary fiber (g) Soluble fiber (g) Insoluble dietary fiber (g) | 24.9 ± 9.7 6.1 ± 2.8 18.8 ± 7.5 | 16.0 ± 8.3 4.8 ± 2.6 11.6 ± 6.1 | 13.6 ± 7.2 3.9 ± 2.2 9.6 ± 5.4 | 14.2 ± 7.1 4.6 ± 2.4 9.5 ± 5.4 |
| Ratio soluble to insoluble dietary fiber | 0.3 ± 0.1 | 0.4 ± 0.2 | 0.4 ± 0.2 | 0.6 ± 0.3 |
| Meeting 14 g/1000 kcal (n, %) | 208 (42.5) | 35 (8.7) | 28 (5.8) | 14 (3.2) |
| Ghana | Jamaica | Seychelles | USA | Across All Sites | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 246 | n = 200 | n = 242 | n = 222 | n = 942 | ||||||
| Q1 | Q4 b | Q1 | Q4 c | Q1 | Q4 d | Q1 | Q4 e | Q1 | Q4 f | |
| Metabolic syndrome | 9 (7.3) | 8 (6.5) | 10 (10.0) | 6 (6.0) | 8 (6.6) | 12 (9.9) | 30 (27.0) | 15 (13.5) * | 57 (12.5) | 41 (9.0) |
| Inflammation | 26 (23.0) | 29 (24.8) | 27 (30.3) | 34 (36.6) | 33 (31.1) | 22 (19.5) * | 51 (51.0) | 39 (37.5) * | 154 (38.0) | 103 (23.8) * |
| Obesity | 12 (9.8) | 10 (8.1) | 34 (34.0) | 27 (27.0) | 39 (32.2) | 30 (24.8) | 56 (50.5) | 54 (48.7) | 173 (38.0) | 80 (17.6) * |
| Quartiles of Total Fiber | Metabolic Syndrome | Inflammation | Obesity |
|---|---|---|---|
| 0.0–10.3 g (Q1) | 1 | 1 | 1 |
| 10.3–15.1 g (Q2) | 1.0 (0.7–1.5) | 0.9 (0.7–1.3) | 0.9 (0.7–1.2) |
| 15.1–22.1 g (Q3) | 0.5 (0.3–0.8) * | 0.7 (0.5–0.9) * | 0.6 (0.4–0.8) * |
| >22.1 g (Q4) | 0.7 (0.4–1.2) | 0.5 (0.4–0.8) * | 0.4 (0.2–0.5) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lie, L.; Brown, L.; Forrester, T.E.; Plange-Rhule, J.; Bovet, P.; Lambert, E.V.; Layden, B.T.; Luke, A.; Dugas, L.R. The Association of Dietary Fiber Intake with Cardiometabolic Risk in Four Countries across the Epidemiologic Transition. Nutrients 2018, 10, 628. https://doi.org/10.3390/nu10050628
Lie L, Brown L, Forrester TE, Plange-Rhule J, Bovet P, Lambert EV, Layden BT, Luke A, Dugas LR. The Association of Dietary Fiber Intake with Cardiometabolic Risk in Four Countries across the Epidemiologic Transition. Nutrients. 2018; 10(5):628. https://doi.org/10.3390/nu10050628
Chicago/Turabian StyleLie, Louise, Laquita Brown, Terrence E. Forrester, Jacob Plange-Rhule, Pascal Bovet, Estelle V. Lambert, Brian T. Layden, Amy Luke, and Lara R. Dugas. 2018. "The Association of Dietary Fiber Intake with Cardiometabolic Risk in Four Countries across the Epidemiologic Transition" Nutrients 10, no. 5: 628. https://doi.org/10.3390/nu10050628