Human Milk Adiponectin and Leptin and Infant Body Composition over the First 12 Months of Lactation

 , , , , ,
, , , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Session
2.3. Anthropometric Measurements
2.4. Body Composition with Bioelectrical Impedance Spectroscopy
2.5. Ultrasound Skinfold Measurements
2.6. Body Composition Indices
2.7. 24-h Milk Intake and Feeding Frequency
2.8. Calculated Daily Intakes of Adipokines
2.9. Sample Preparation
2.10. Leptin
2.11. Adiponectin
2.12. Statistical Analyses
3. Results
3.1. Subjects
3.2. Breastfeeding Parameters and Milk Components
3.3. Maternal Body Composition and Adipokines
3.4. Infant Body Composition and Concentrations of Adipokines
3.5. Infant Body Composition and Calculated Daily Intakes of Adipokines
3.6. Breastfeeding Parameters and Adipokines
3.7. Changes in Infant Characteristics and Calculated Daily Intakes of Adipokines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Predictor | 2 Months | 5 Months | 9 Months | 12 Months | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| Whole milk leptin (ng/mL) | |||||||||||
| BMI d (kg/m2) | 0.35 (0.09) a | 0.006 (0.003) | 0.33 (0.08) | 0.006 (0.003) | 0.41 (0.08) | 0.006 (0.003) | 0.39 (0.08) | 0.006 (0.003) | 0.045 b | 0.17 | 0.15 c |
| Weight (kg) | 0.35 (0.08) | 0.002 (0.001) | 0.33 (0.07) | 0.002 (0.001) | 0.42 (0.07) | 0.002 (0.001) | 0.39 (0.07) | 0.002 (0.001) | 0.023 | 0.18 | 0.44 |
| FM d (kg) | 0.42 (0.05) | 0.003 (0.002) | 0.40 (0.05) | 0.003 (0.002) | 0.49 (0.05) | 0.003 (0.002) | 0.46 (0.04) | 0.003 (0.002) | 0.024 | 0.16 | 0.45 |
| FFM d (kg) | 0.22 (0.08) | 0.002 (0.002) | 0.16 (0.08) | 0.002 (0.002) | 0.11 (0.08) | 0.002 (0.002) | 0.12 (0.08) | 0.002 (0.002) | 0.041 | 0.23 | 0.46 |
| FMI d (kg/m2) | 0.42 (0.06) | 0.010 (0.005) | 0.39 (0.05) | 0.010 (0.005) | 0.48 (0.05) | 0.010 (0.005) | 0.46 (0.05) | 0.010 (0.005) | 0.038 | 0.15 | 0.30 |
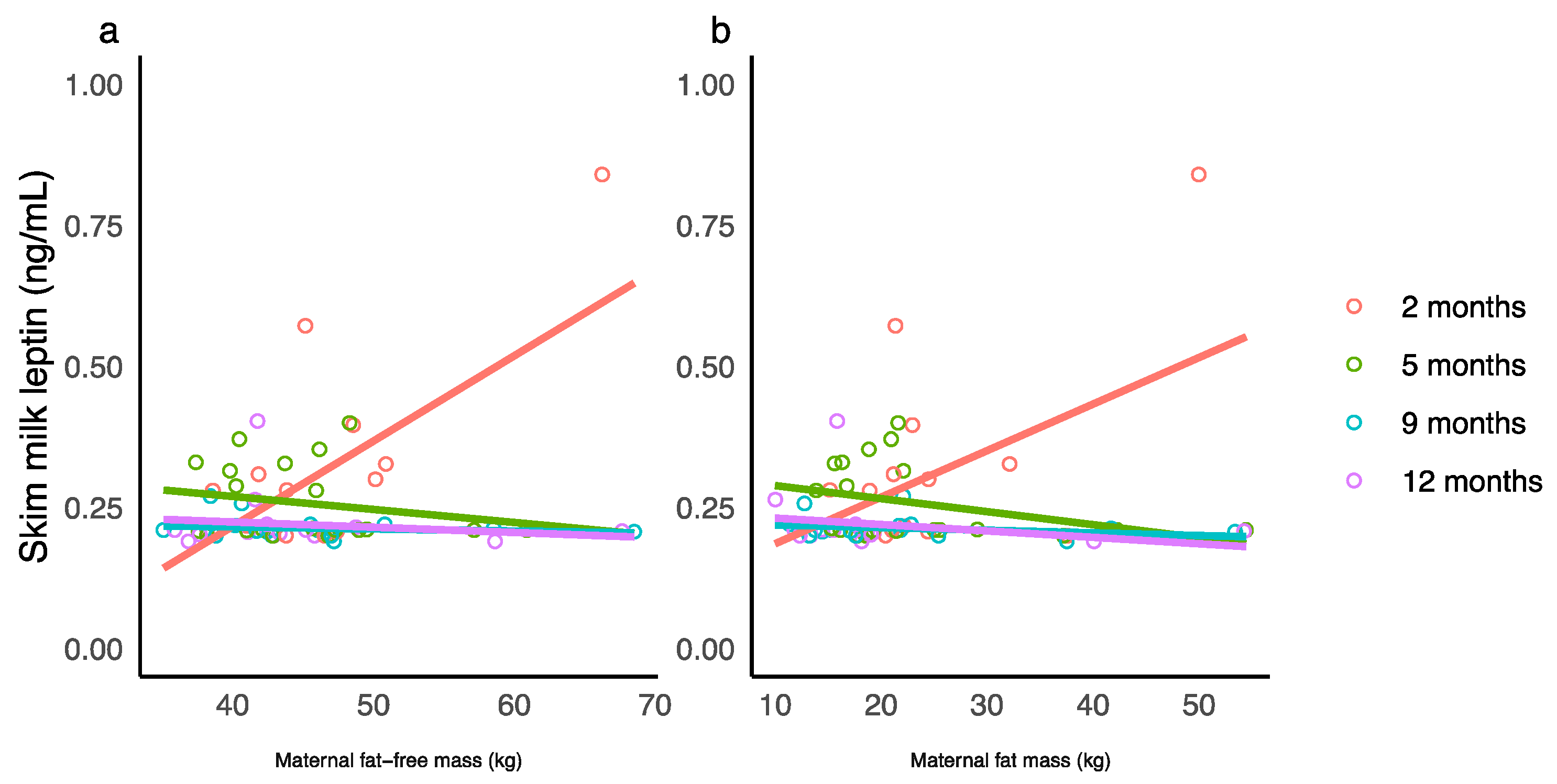
| Skim milk leptin (ng/mL) | |||||||||||
| Weight (kg) | −0.11 (0.11) | 0.006 (0.001) | 0.35 (0.09) | −0.001 (0.001) | 0.23 (0.08) | −0.0002 (0.001) | 0.26 (0.08) | −0.001 (0.001) | 0.44 | 0.001 | <0.001 |
| FM (kg) | 0.10 (0.07) | 0.008 (0.003) | 0.31 (0.05) | −0.002 (0.002) | 0.22 (0.05) | −0.001 (0.002) | 0.24 (0.05) | −0.001 (0.002) | 0.79 | 0.002 | 0.003 |
| FFM (kg) | −0.39 (0.14) | 0.015 (0.003) | 0.36 (0.14) | −0.002 (0.003) | 0.23 (0.12) | −0.0004 (0.003) | 0.26 (0.12) | −0.001 (0.003) | 0.14 | 0.001 | <0.001 |
| Predictor (Concentration, ng/mL) | 2 Months | 5 Months | 9 Months | 12 Months | p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | ||||
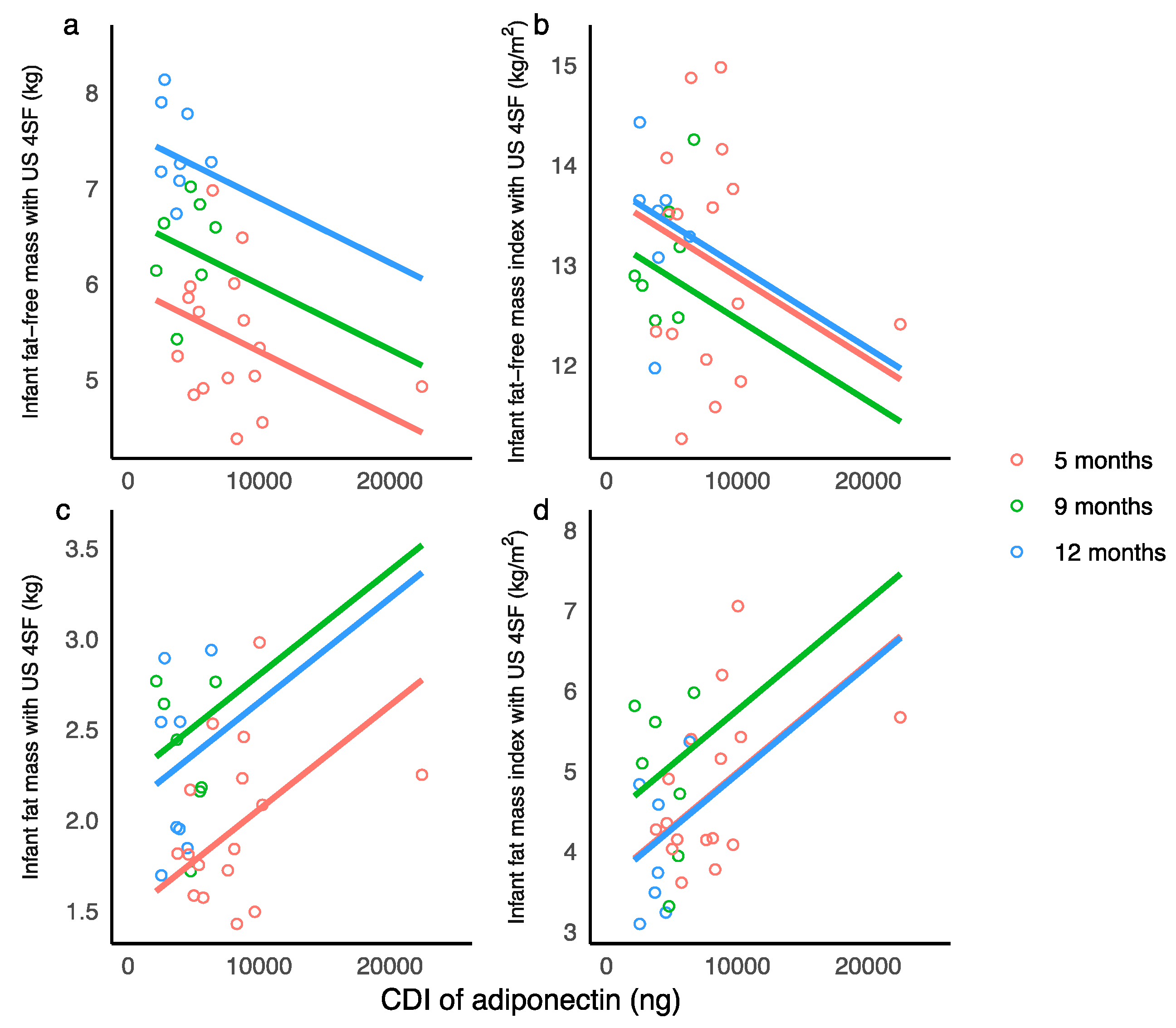
| Infant fat-free mass with ultrasound 4 skinfolds (kg) | ||||||||||||||
| Whole milk adiponectin | 4.53 (0.22) a | −0.032 (0.015) | 5.76 (0.21) | −0.032 (0.015) | 6.77 (0.20) | −0.032 (0.015) | 7.58 (0.23) | −0.032 (0.015) | 0.025 b | <0.001 | 0.052 c | |||
| Infant fat-free mass with bioelectrical impedance spectroscopy (kg) | ||||||||||||||
| Whole milk leptin | 4.53 (0.42) | −0.33 (0.76) | 5.49 (0.30) | −0.44 (0.55) | 5.01 (0.57) | 2.64 (0.55) | 5.62 (0.59) | 2.77 (1.04) | 0.24 | <0.001 | 0.016 | |||
| Infant head circumference (cm) | ||||||||||||||
| Skim milk leptin | 40.30 (0.44) | −1.85 (0.84) | 43.30 (0.40) | −1.85 (0.84) | 45.80 (0.39) | −1.85 (0.84) | 46.80 (0.39) | −1.85 (0.84) | 0.028 | <0.001 | 0.37 | |||
| Predictor (CDI d, ng) | Between 2 and 5 Months | 9 Months | 12 Months | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| Infant head circumference (cm) | |||||||||
| Whole milk adiponectin | 43.00 (0.40) a | −0.00002 (0.00002) | 44.60 (0.56) | 0.0002 (0.0001) | 46.80 (0.59) | −0.0001 (0.0001) | 0.27 | <0.001 | 0.026 |
| Infant body mass index (kg/m2) | |||||||||
| Whole milk adiponectin | 16.90 (0.54) | 0.0001 (0.0001) | 19.0 (0.96) | −0.0002 (0.0002) | 20.10 (1.04) | −0.0006 (0.0002) | 0.18 b | 0.46 | 0.016 c |
| Skim milk leptin | 15.60 (0.77) | 0.001 (0.003) | 18.20 (0.95) | −0.002 (0.008) | 19.40 (0.84) | −0.016 (0.007) | 0.060 | 0.21 | 0.004 |
| Infant fat-free mass with ultrasound 4 skinfolds (kg) | |||||||||
| Whole milk adiponectin | 5.97 (0.24) | −0.0001 (0.00002) | 6.68 (0.20) | −0.0001 (0.00002) | 7.58 (0.20) | −0.0001 (0.00002) | 0.005 | <0.001 | 0.80 |
| Infant fat-free mass index with ultrasound 4 skinfolds (kg/m2) | |||||||||
| Whole milk adiponectin | 13.70 (0.42) | −0.0001 (0.00004) | 13.30 (0.36) | −0.0001 (0.00004) | 13.80 (0.35) | −0.0001 (0.00004) | 0.009 | 0.060 | 0.056 |
| Skim milk leptin | 13.20 (0.59) | −0.0008 (0.003) | 13.40 (0.76) | −0.004 (0.006) | 15.50 (0.65) | −0.019 (0.006) | 0.11 | 0.10 | 0.012 |
| Whole milk leptin | 13.00 (0.47) | 0.0002 (0.001) | 13.50 (1.08) | −0.002 (0.004) | 15.40 (0.79) | −0.008 (0.003) | 0.75 | 0.15 | 0.036 |
| Infant fat mass with ultrasound 2 skinfolds (kg) | |||||||||
| Skim milk leptin | 1.06 (0.21) | 0.004 (0.001) | 2.74 (0.27) | −0.002 (0.002) | 2.15 (0.21) | 0.004 (0.002) | <0.001 | <0.001 | 0.007 |
| Infant fat mass with ultrasound 4 skinfolds (kg) | |||||||||
| Whole milk adiponectin | 1.48 (0.16) | 0.0001 (0.00002) | 2.23 (0.14) | 0.0001 (0.00002) | 2.07 (0.14) | 0.0001 (0.00002) | <0.001 | <0.001 | 0.19 |
| Skim milk leptin | 1.12 (0.21) | 0.004 (0.001) | 1.99 (0.16) | 0.004 (0.001) | 1.90 (0.14) | 0.004 (0.001) | <0.001 | <0.001 | 0.17 |
| Infant fat mass with bioelectrical impedance spectroscopy (kg) | |||||||||
| Skim milk leptin | 1.57 (0.26) | 0.003 (0.001) | 1.76 (0.20) | 0.003 (0.001) | 2.15 (0.19) | 0.003 (0.001) | 0.025 | 0.016 | 0.67 |
| Infant fat mass with ultrasound 2 skinfolds (%) | |||||||||
| Skim milk leptin | 20.40 (2.13) | 0.029 (0.009) | 23.80 (1.60) | 0.029 (0.009) | 22.90 (1.44) | 0.029 (0.009) | 0.001 | 0.067 | 0.13 |
| Infant fat mass with ultrasound 4 skinfolds (%) | |||||||||
| Whole milk adiponectin | 20.80 (1.54) | 0.0007 (0.0002) | 24.80 (1.30) | 0.0007 (0.0002) | 21.00 (1.24) | 0.0007 (0.0002) | <0.001 | <0.001 | 0.12 |
| Skim milk leptin | 20.00 (2.17) | 0.031 (0.009) | 23.80 (1.63) | 0.031 (0.009) | 20.50 (1.47) | 0.031 (0.009) | 0.002 | 0.032 | 0.032>0.43 |
| Infant fat mass index with ultrasound 2 skinfolds (kg/m2) | |||||||||
| Whole milk adiponectin | 4.04 (0.41) | 0.0001 (0.00004) | 4.63 (0.34) | 0.0001 (0.00004) | 4.24 (0.34) | 0.0001 (0.00004) | 0.039 | 0.20 | 0.51 |
| Skim milk leptin | 3.08 (0.48) | 0.008 (0.002) | 4.09 (0.35) | 0.008 (0.002) | 3.82 (0.33) | 0.008 (0.002) | <0.001 | 0.002 | 0.032>0.065 |
| Infant fat mass index with ultrasound 4 skinfolds (kg/m2) | |||||||||
| Whole milk adiponectin | 3.62 (0.38) | 0.0001 (0.00004) | 4.40 (0.32) | 0.0001 (0.00004) | 3.60 (0.32) | 0.0001 (0.00004) | <0.001 | 0.002 | 0.10 |
| Skim milk leptin | 3.10 (0.50) | 0.008 (0.002) | 4.01 (0.37) | 0.008 (0.002) | 3.31 (0.35) | 0.008 (0.002) | <0.001 | 0.012 | 0.29 |
| Infant fat mass index with bioelectrical impedance spectroscopy (kg/m2) | |||||||||
| Skim milk leptin | 3.97 (0.58) | 0.005 (0.003) | 3.64 (0.43) | 0.005 (0.003) | 3.88 (0.41) | 0.005 (0.003) | 0.038 | 0.71 | 0.55 |
| Predictor (Concentration of Adipokine or Breastfeeding Parameter) | Between 2 and 5 Months | 9 Months | 12 Months | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| Infant feeding frequency (feeds/24-h) d | |||||||||
| Whole milk adiponectin (ng/mL) | 8.02 (0.82) a | 0.010 (0.08) | 7.21 (2.36) | −0.23 (0.28) | 10.01 (1.90) | −0.63 (0.21) | 0.53 b | <0.001 | 0.009 c |
| Infant 24-h milk intake (g) d | |||||||||
| Whole milk adiponectin (ng/mL) | 645 (80.40) | 17.8 (6.83) | 244 (210) | 31.5 (24.50) | 1120 (161) | −75.3 (16.80) | 0.18 | <0.001 | <0.001 |
| CDI of whole milk leptin (ng) d | |||||||||
| Feeding frequency (24-h MP) f | 1.77 (129.0) | 45.0 (15.40) | 13.50 (92.60) | 45.0 (15.40) | 13.60 (80.10) | 45.0 (15.40) | 0.004 | 0.98 | 0.74 |
| Changes in Infant Characteristic | Months after Birth | |||||
|---|---|---|---|---|---|---|
| 5 and 2 | 9 and 2 | 12 and 2 | 9 and 5 | 12 and 5 | 12 and 9 | |
| Calculated daily intake of whole milk leptin (ng) between 2 and 5 months e | ||||||
| ΔLength (cm) | 0.003 (0.031) a 0.29 b,c | 0.008 (0.003) 0.022 | 0.003 (0.005) 0.57 | −0.0002 (0.002) 0.93 | −0.002 (0.003) 0.57 | −0.001 (0.003) 0.75 |
| Calculated daily intake of whole milk leptin (ng) at 9 months e | ||||||
| ΔLength (cm) | n/a f | −0.014 (0.022) 0.60 | 0.041 (0.004) 0.007 | −0.005 (0.011) 0.65 | 0.005 (0.011) 0.67 | 0.01 (0.012) 0.45 |
| Calculated daily intake of whole milk leptin (ng) at 12 months e | ||||||
| ΔBMI d (kg/m2) | n/a f | n/a f | 0.002 (0.01)0.86 | n/a f | −0.008 (0.006) 0.22 | −0.007 (0.002) 0.019 |
| ΔFat-free mass index US 2SF (kg/m2) | n/a | n/a | −0.011 (0.009) 0.34 | n/a | −0.012 (0.004) 0.040 | −0.005 (0.003) 0.12 |
| ΔFat-free mass index US 4SF (kg/m2) | n/a | n/a | −0.011 (0.011) 0.39 | n/a | −0.012 (0.002) 0.007 | −0.007 (0.004) 0.13 |
| ΔFat mass US 2SF (kg) | n/a | n/a | 0.005 (0.0003) 0.0006 *** | n/a | 0.002 (0.002) 0.22 | 0.0001 (0.0009) 0.89 |
| ΔFat mass US BIS (kg) | n/a | n/a | 0.005 (0.001) 0.046 | n/a | −0.001 (0.002) 0.66 | −0.0003 (0.002) 0.90 |
| ΔFat mass index US 2SF (kg/m2) | n/a | n/a | 0.012 (0.002) 0.018 | n/a | 0.004 (0.004) 0.35 | −0.002 (0.002) 0.43 |
| ΔFat mass US 2SF (%) | n/a | n/a | 0.073 (0.004) 0.0004 *** | n/a | 0.024 (0.017) 0.20 | −0.002 (0.013) 0.90 |
| ΔFat mass BIS (%) | n/a | n/a | 0.065 (0.015) 0.049 | n/a | −0.01 (0.021) 0.66 | −0.006 (0.028) 0.84 |
| Changes in Infant Characteristic | Months after Birth | |||||
|---|---|---|---|---|---|---|
| 5 and 2 | 9 and 2 | 12 and 2 | 9 and 5 | 12 and 5 | 12 and 9 | |
| Calculated daily intake of skim milk leptin (ng) between 2 and 5 months e | ||||||
| ΔWeight (kg) | 0.002 (0.001) a 0.097 b,c | 0.005 (0.002) 0.015 | 0.005 (0.002) 0.026 | 0.001 (0.001) 0.46 | 0.001 (0.002) 0.75 | −0.0001 (0.001) 0.84 |
| ΔBMI d (kg/m2) | 0.006 (0.002) 0.021 | 0.004 (0.004) 0.31 | 0.002 (0.005) 0.63 | −0.003 (0.003) 0.33 | −0.005 (0.004) 0.23 | −0.002 (0.003) 0.53 |
| ΔFat-free mass US 2SF d (kg) | −0.001 (0.002) 0.47 | 0.003 (0.001) 0.012 | 0.003 (0.002) 0.16 | 0.002 (0.001) 0.25 | 0.002 (0.002) 0.31 | −0.0001 (0.001) 0.89 |
| ΔFat-free mass US 4SF d (kg) | 0.001 (0.001) 0.67 | 0.004 (0.001) 0.010 | 0.005 (0.002) 0.018 | 0.002 (0.001) 0.090 | 0.003 (0.002) 0.096 | 0.001 (0.001) 0.40 |
| ΔFat-free mass BIS d (kg) | 0.001 (0.001) 0.21 | 0.004 (0.002) 0.055 | 0.005 (0.001) 0.013 | 0.002 (0.001) 0.098 | 0.002 (0.002) 0.22 | 0.0004 (0.002) 0.81 |
| ΔFat mass US 2SF (kg) | 0.003 (0.001) 0.029 | 0.001 (0.001) 0.30 | 0.002 (0.002) 0.25 | −0.001 (0.001) 0.50 | −0.001 (0.001) 0.39 | 0.0002 (0.001) 0.76 |
| ΔFat mass BIS (kg) | 0.002 (0.001) 0.044 | 0.001 (0.002) 0.71 | 0.001 (0.001) 0.58 | −0.002 (0.001) 0.18 | −0.002 (0.001) 0.14 | −0.0001 (0.002) 0.96 |
| ΔFat mass index US 2SF (kg/m2) | 0.007 (0.003) 0.047 | 0.001 (0.003) 0.76 | 0.001 (0.004) 0.88 | −0.004 (0.003) 0.22 | −0.005 (0.003) 0.13 | −0.001 (0.002) 0.69 |
| ΔFat mass index US 4SF (kg/m2) | 0.002 (0.001) 0.18 | −0.002 (0.004) 0.61 | −0.004 (0.005) 0.47 | −0.005 (0.003) 0.13 | −0.007 (0.003) 0.026 | −0.002 (0.001) 0.23 |
| ΔFat mass US 4SF (%) | 0.007 (0.009) 0.48 | −0.015 (0.017) 0.39 | −0.020 (0.020) 0.36 | −0.021 (0.014) 0.15 | −0.027 (0.012) 0.036 | −0.007 (0.008) 0.38 |
| Calculated daily intake of skim milk leptin (ng) at 9 months e | ||||||
| ΔWeight (kg) | n/a f | 0.026 (0.004) 0.007 | 0.033 (0.008) 0.025 | −0.005 (0.006) 0.41 | −0.006 (0.006) 0.39 | −0.0006 (0.002) 0.81 |
| ΔBMI d (kg/m2) | n/a | 0.12 (0.04) 0.11 | 0.10 (0.02) 0.035 | −0.01 (0.02) 0.50 | −0.02 (0.01) 0.34 | −0.004 (0.01) 0.70 |
| ΔFat mass BIS (kg) | n/a | 0.052 (0.012) 0.046 | 0.016 (0.026) 0.60 | −0.005 (0.007) 0.47 | −0.008 (0.005) 0.13 | −0.003 (0.005) 0.60 |
| Calculated daily intake of skim milk leptin (ng) at 12 months e | ||||||
| ΔFat-free mass index US 2SF (kg/m2) | n/a f | n/a f | −0.025 (0.010) 0.13 | n/a f | −0.031 (0.007) 0.005 | −0.013 (0.006) 0.081 |
| ΔFat-free mass index US 4SF (kg/m2) | n/a | n/a | −0.022 (0.017) 0.32 | n/a | −0.025 (0.002) 0.0004 *** | −0.011 (0.009) 0.27 |
| ΔFat mass US 2SF (kg) | n/a | n/a | 0.010 (0.002) 0.022 | n/a | 0.005 (0.004) 0.23 | 0.002 (0.002) 0.32 |
| ΔFat mass US 2SF (%) | n/a | n/a | 0.135 (0.041) 0.046 | n/a | 0.061 (0.037) 0.14 | 0.022 (0.029) 0.49 |
| Changes in Infant Characteristic | Months after Birth | |||||
|---|---|---|---|---|---|---|
| 5 and 2 | 9 and 2 | 12 and 2 | 9 and 5 | 12 and 5 | 12 and 9 | |
| Calculated daily intake of adiponectin (ng) between 2 and 5 months e | ||||||
| ΔLength (cm) | −0.0001 (0.0001) a 0.074 b,c | 0.0002 (0.0001) 0.079 | 0.00004 (0.0001) 0.76 | 0.0002 (0.0001) 0.010 | 0.0001 (0.0001) 0.47 | −0.0001 (0.0001) 0.39 |
| ΔFat-free mass US 4SF d (kg) | −0.00002 (0.00002) 0.43 | 0.0001 (0.00002) 0.036 | 0.0001 (0.00003) 0.043 | −0.0001 (0.00002) 0.011 | 0.0001 (0.00003) 0.018 | 0.00001 (0.00002) 0.41 |
| ΔFat-free mass index US 2SF (kg/m2) | 0.00004 (0.0001) 0.42 | 0.0001 (0.00004) 0.28 | 0.0001 (0.00004) 0.026 | −0.00002 (0.0001) 0.77 | 0.00004 (0.0001) 0.54 | 0.00001 (0.00004) 0.17 |
| ΔFat-free mass index US 4SF (kg/m2) | 0.00002 (0.0001) 0.67 | 0.0001 (0.00001) 0.092 | 0.0002 (0.00004) 0.009 | 0.0001 (0.00001) 0.27 | 0.0001 (0.0001) 0.057 | 0.00001 (0.0001) 0.22 |
| ΔFat-free mass index BIS (kg/m2) | 0.0001 (0.00003) 0.098 | 0.0001 (0.0001) 0.23 | 0.0001 (0.00004) 0.029 | 0.00002 (0.0001) 0.67 | 0.00004 (0.0001) 0.54 | 0.00004 (0.0001) 0.44 |
| ΔFat mass US 4SF (kg) | 0.00001 (0.00001) 0.50 | −0.00003 (0.00002) 0.22 | −0.00004 (0.00003) 0.22 | −0.00004 (0.00003) 0.17 | −0.0001 (0.00002) 0.049 | −0.00001 (0.00001) 0.68 |
| ΔFat mass US 4SF (%) | 0.0001 (0.0002) 0.62 | −0.001 (0.0002) 0.044 | −0.001 (0.0003) 0.099 | −0.001 (0.0003) 0.044 | −0.001 (0.0002) 0.007 | −0.0001 (0.0002) 0.047 |
| ΔFat mass index US 4SF (kg/m2) | 0.00003 (0.00003) 0.36 | −0.0001 (0.0001) 0.10 | −0.0001 (0.0001) 0.25 | −0.0001 (0.0001) 0.059 | −0.0001 (0.0001) 0.044 | 0.000 (0.00003) 0.99 |
| Calculated daily intake of adiponectin (ng) at 9 months e | ||||||
| ΔHead circumference (cm) | n/a f | 0.0004 (0.0004) 0.42 | −0.0002 (0.0004) 0.64 | 0.0001 (0.0001) 0.32 | −0.0002 (0.0001) 0.066 | −0.0003 (0.0001) 0.017 |
| Calculated daily intake of adiponectin (ng) at 12 months e | ||||||
| ΔFat-free mass index US 4SF (kg/m2) | n/a f | n/a f | −0.001 (0.001) 0.39 | n/a | −0.001 (0.0002) 0.020 | −0.0004 (0.0003) 0.23 |
| ΔFat mass index US 2SF (kg/m2) | n/a | n/a | 0.001 (0.0001) 0.005 | n/a f | 0.00002 (0.0003) 0.95 | 0.00002 (0.0002) 0.90 |
| ΔFat mass US 2SF (kg) | n/a | n/a | 0.001 (0.0001) 0.012 | n/a | −0.00003 (0.0001) 0.82 | 0.0001 (0.0001) 0.26 |
| ΔFat mass BIS (kg) | n/a | n/a | 0.001 (0.0001) 0.018 | n/a | −0.0002 (0.0001) 0.17 | −0.0001 (0.0002) 0.59 |
| ΔFat mass US 2SF (%) | n/a | n/a | 0.009 (0.002) 0.013 | n/a | 0.001 (0.001) 0.63 | 0.001 (0.001) 0.46 |
| ΔFat mass BIS (%) | n/a | n/a | 0.007 (0.001) 0.011 | n/a | −0.002 (0.001) 0.26 | −0.001 (0.002) 0.63 |
References
- Koletzko, B.; Brands, B.; Chourdakis, M.; Cramer, S.; Grote, V.; Hellmuth, C.; Kirchberg, F.; Prell, C.; Rzehak, P.; Uhl, O.; et al. The power of programming and the early nutrition project: Opportunities for health promotion by nutrition during the first thousand days of life and beyond. Ann. Nutr. Metab. 2014, 64, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Geddes, D.; Prescott, S. Developmental origins of health and disease: The role of human milk in preventing disease in the 21(st) century. J. Hum. Lact. 2013, 29, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Chomoto, S.; Fewtrell, M.S. Programming of body composition by early growth and nutrition. Proc. Nutr. Soc. 2007, 66, 423–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hypponen, E.; Kenward, M.; Virtanen, S.; Piitulainen, A.; Virta-Autio, P.; Tuomilehto, J.; Knip, M.; Akerblom, H. Infant feeding, early weight gain, and risk of type 1 diabetes. Childhood diabetes in Finland (DiMc) study group. Diab. Care 1999, 22, 1961–1965. [Google Scholar] [CrossRef]
- Andersson, S.; Bengtsson, C.; Hallberg, L.; Lapidus, L.; Niklasson, A.; Wallgren, A.; Hulthen, L. Cancer risk in Swedish women: The relation to size at birth. Br. J. Cancer 2001, 84, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Stettler, N.; Kumanyika, S.; Katz, S.; Zemel, B.; Stallings, V. Rapid weight gain during infancy and obesity in young adulthood in a cohort of African Americans. Am. J. Clin. Nutr. 2003, 77, 1374–1378. [Google Scholar] [CrossRef] [PubMed]
- Stettler, N.; Stallings, V.; Troxel, A.; Zhao, J.; Schinnar, R.; Nelson, S.; Ziegler, E.; Strom, B. Weight gain in the first week of life and overweight in adulthood: A cohort study of European American subjects fed infant formula. Circulation 2005, 111, 1897–1903. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.; Wong, W.; Hopkinson, J.; Smith, E.; Ellis, K. Infant feeding mode affects early growth and body composition. Pediatrics 2000, 16, 1355–1366. [Google Scholar] [CrossRef]
- Luque, V.; Closa-Monasterolo, R.; Escribano, J.; Ferre, N. Early programming by protein intake: The effect of protein on adiposity development and the growth and functionality of vital organs. Nutr. Metab. Insights 2015, 8, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Kon, I.Y.; Shilina, N.M.; Gmoshinskaya, M.V.; Ivanushkina, T.A. The study of breast milk IGF-1, leptin, ghrelin and adiponectin levels as possible reasons of high weight gain in breast-fed infants. Ann. Nutr. Metab. 2014, 65, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Sievers, E.; Oldigs, H.D.; Santer, R.; Schaub, J. Feeding patterns in breast-fed and formula-fed infants. Ann. Nutr. Metab. 2002, 46, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Savino, F.; Liguori, S.A.; Fissore, M.F.; Oggero, R. Breast milk hormones and their protective effect on obesity. Int. J. Pediatr. Endocrinol. 2009, 2009, 327505. [Google Scholar] [CrossRef] [PubMed]
- Bartok, C. Babies fed breastmilk by breast versus by bottle: A pilot study evaluating early growth patterns. Breastfeed. Med. 2011, 6, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Rea, A.; Hepworth, A.R.; Ward, L.C.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. Relationships between breastfeeding patterns and maternal and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 45. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Hepworth, A.R.; Prime, D.K.; Lai, C.T.; Trengove, N.J.; Hartmann, P.E. Variation in fat, lactose, and protein composition in breast milk over 24 hours: Associations with infant feeding patterns. J. Hum. Lact. 2013, 29, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Hennet, T.; Borsig, L. Breastfed at Tiffany’s. Trends Biochem. Sci. 2016, 41, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Guerrero, M.; Altaye, M.; Ruiz-Palacios, G.; Martin, L.; Dubert-Ferrandon, A.; Newburg, D.; Morrow, A. Human milk adiponectin is associated with growth in two independent cohorts. Breastfeed. Med. 2009, 4, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Guerrero, M.; Guo, F.; Martin, L.; Davidson, B.; Ortega, H.; Ruiz-Palacios, G.; Morrow, A. Human milk adiponectin affects infant weight trajectory during the second year of life. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Miralles, O.; Sanchez, J.; Palou, A.; Pico, C. A physiological role of breast milk leptin in body weight control in developing infants. Obesity 2006, 14, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.; Demerath, E. Relationship of insulin, glucose, leptin, IL-6 and TNF-a in human breast milk with infant growth and body composition. Pediatr. Obes. 2012, 7, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Kugananthan, S.; Lai, C.T.; Gridneva, Z.; Mark, P.J.; Geddes, D.T.; Kakulas, F. Leptin levels are higher in whole compared to skim human milk, supporting a cellular contribution. Nutrients 2016, 8, 711. [Google Scholar] [CrossRef] [PubMed]
- Kugananthan, S.; Gridneva, Z.; Lai, C.T.; Hepworth, A.R.; Mark, P.J.; Kakulas, F.; Geddes, D.T. Associations between maternal body composition and appetite hormones and macronutrients in human milk. Nutrients 2017, 9, 252. [Google Scholar] [CrossRef] [PubMed]
- Uysal, F.; Onal, E.; Aral, Y.; Adam, B.; Dilmen, U.; Ardicolu, Y. Breast milk leptin: Its relationship to maternal and infant adiposity. Clin. Nutr. 2002, 21, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.M.; Jebb, S.A. Beyond body mass index. Obes. Rev. 2001, 2, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Hepworth, A.R.; Ward, L.C.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. Determinants of body composition in breastfed infants using bioimpedance spectroscopy and ultrasound skinfolds—methods comparison. Pediatr. Res. 2016, 81, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreas, N.J.; Hyde, M.J.; Gale, C.; Parkinson, J.R.C.; Jeffries, S.; Holmes, E.; Modi, N. Effect of maternal body mass index on hormones in breast milk: A systematic review. PLoS ONE 2014, 9, e115043. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Schneider, C.R.; Pavela, G. A narrative review of the associations between six bioactive components in breast milk and infant adiposity. Obesity 2016, 24, 1213–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, L.J.; Woo, J.G.; Geraghty, S.R.; Altaye, M.; Davidson, B.S.; Banach, W.; Dolan, L.M.; Ruiz-Palacios, G.M.; Morrow, A.L. Adiponectin is present in human milk and is associated with maternal factors. Am. J. Clin. Nutr. 2006, 83, 1106–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigro, E.; Scudiero, O.; Monaco, M.L.; Palmieri, A.; Mazzarella, G.; Costagliola, C.; Bianco, A.; Daniele, A. New insight into adiponectin role in obesity and obesity-related diseases. BioMed Res. Int. 2014, 2014, 658913. [Google Scholar] [CrossRef] [PubMed]
- Catli, G.; Dundar, N.O.; Dundar, B.N. Adipokines in breast milk: An update. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Weyermann, M.; Beermann, C.; Brenner, H.; Dietrich, R. Adiponectin and leptin in maternal serum, cord blood, and breast milk. Clin. Chem. 2006, 52, 2095–2102. [Google Scholar] [CrossRef] [PubMed]
- Arita, Y.; Kihara, S.; Ouchi, N.; Takahashi, M.; Maeda, K.; Miyagawa, S.; Hotta, K.; Shimomura, I.; Nakamura, T.; Miyaoka, K.; et al. Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem. Biophys. Res. Commun. 1999, 257, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Savino, F.; Lupica, M.M.; Benetti, S.; Petrucci, E.; Liguori, S.A.; Cordero Di Montezemolo, L. Adiponectin in breast milk: Relation to serum adiponectin concentration in lactating mothers and their infants. Acta Pediatr. 2012, 101, 1058–1062. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, A.M.; Algendy, Y.G.; Shaaban, M.A.; El Shalabi, A.M. Relation of breast milk adiponectin level to infant growth. Egypt. J. Hosp. Med. 2017, 69, 3036–3041. [Google Scholar] [CrossRef]
- Weyermann, M.; Brenner, H.; Rothenbacher, D. Adipokines in human milk and risk of overweight in early childhood: A prospective cohort study. Epidemiology 2007, 18, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Brunner, S.; Schmid, D.; Zang, K.; Much, D.; Knoeferl, B.; Kratzsch, J.; Amann-Gassner, U.; Bader, B.L.; Hauner, H. Breast milk leptin and adiponectin in relation to infant body composition up to 2 years. Pediatr. Obes. 2014, 10, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Bronsky, J.; Mitrova, K.; Karpisek, M.; Mazoch, J.; Durilova, M.; Fisarkova, B.; Stechova, K.; Prusa, R.; Nevoral, J. Adiponectin, AFABP, and leptin in human breast milk during 12 months of lactation. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Dundar, N.O.; Dundar, B.; Cesur, G.; Yilmaz, N.; Sutcu, R.; Ozguner, F. Ghrelin and adiponectin levels in colostrum, cord blood and maternal serum. Pediatr. Int. 2010, 52, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; McKinley, K.; Onugha, J.; Duazo, P.; Chernoff, M.; Quinn, E.A. Lower levels of human milk adiponectin predict offspring weight for age: A study in a lean population of Filipinos. Matern. Child. Nutr. 2016, 12, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Luoto, R.; Kalliomaki, M.; Laitinen, K.; Delzenne, N.M.; Cani, P.D.; Salmimen, S.; Isolauri, E. Initial dietary and microbiological environments deviate in normal-weight compared to overweight children at 10 years of age. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Khodabakhshi, A.; Ghayour-Mobarhan, M.; Rooki, H.; Vakili, R.; Hashemy, S.-I.; Mirhafez, S.R.; Shakeri, M.-T.; Kashanifar, R.; Pourbafarani, R.; Mirzaei, H.; et al. Comparative measurement of ghrelin, leptin, adiponectin, EGF and IGF-1 in breast milk of mothers with overweight/obese and normal-weight infants. Eur. J. Clin. Nutr. 2015, 69, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Quinn, E.A.; Childs, G. Ecological pressures and milk metabolic hormones of ethnic Tibetans living at different altitudes. Ann. Hum. Biol. 2016, 44, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Meyer, D.M.; Brei, C.; Stecher, L.; Much, D.; Brunner, S.; Hauner, H. The relationship between breast milk leptin and adiponectin with child body composition from 3 to 5 years: A follow-up study. Pediatr. Obes. 2017, 12, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Bieswal, F.; Ahn, M.T.; Reusens, B.; Holvoet, P.; Raes, M.; Rees, W.D.; Remacle, C. The importance of catch-up growth after early malnutrition for the programming of obesity in male rat. Obesity 2006, 14, 1330–1343. [Google Scholar] [CrossRef] [PubMed]
- Binns, C.W.; Fraser, M.L.; Lee, A.H.; Scott, J. Defining exclusive breastfeeding in Australia. J. Paediatr. Child Health 2009, 45, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Hepworth, A.; Ward, L.; Lai, C.T.; Hartmann, P.; Geddes, D.T. Bioimpedance spectroscopy in the infant: Effect of milk intake and extracellular fluid reservoirs on resistance measurements in term breastfed infants. Eur. J. Clin. Nutr. 2016, 70, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Van Itallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Arthur, P.; Hartmann, P.; Smith, M. Measurement of the milk intake of breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 1987, 6, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.C.; Mitoulas, L.R.; Cregan, M.D.; Ramsay, D.T.; Doherty, D.A.; Hartmann, P.E. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics 2006, 117, e387–e395. [Google Scholar] [CrossRef] [PubMed]
- Keller, R.; Neville, M. Determination of total protein in human milk: Comparison of methods. Clin. Chem. 1986, 32, 120–123. [Google Scholar] [PubMed]
- Cannon, A.; Kakulas, F.; Hepworth, A.; Lai, C.; Hartmann, P.; Geddes, D. The effects of leptin on breastfeeding behaviour. Int. J. Environ. Res. Public. Health 2015, 12, 12340–12355. [Google Scholar] [CrossRef] [PubMed]
- Curran-Everett, D. Multiple comparisons: Philosophies and illustrations. Am. J. Physiol. Reg Integr. Compar. Physiol. 2000, 279, R1–R8. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Pinheiro, J.B.; Bates, D.; DebRoy, S.; Sarkar, D.; R Development Core Team. nlme: Linear and Nonlinear Mixed Effects Models, R package version 3.1-102; R Foundation for Statistical Computing: Vienna, Austria, 2011. [Google Scholar]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. lme4: Linear Mixed-Efects Models Using Eigen and s4, R package version 1.1-7; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Gamer, M.; Lemon, J.; Fellows, I.; Singh, P. Various Coefficients of Interrater Reliability and Agreement; 0.84; R Foundation for Statistical Computing: Vienna, Austria, 2012. [Google Scholar]
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous inference in general parametric models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- Chan, D.; Goruk, S.; Becker, A.B.; Subbarao, P.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.; Sears, M.R.; the CHILD Study investigators; Field, C.J.; et al. Adiponectin, leptin and insulin in breast milk: Associations with maternal characteristics and infant body composition in the first year of life. Int. J. Obes. 2018, 42, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Cesur, G.; Ozguner, F.; Yilmaz, N.; Dundar, B. The relationship between ghrelin and adiponectin levels in breast milk and infant serum and growth of infants during early postnatal life. J. Physiol. Sci. 2012, 62, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.; Hechler, C.; Gebauer, C.; Kiess, W.; Kratzsch, J. Leptin in maternal serum and breast milk: Association with infants’ body weight gain in a longitudinal study over 6 months of lactation. Pediatr. Res. 2011, 70, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Quinn, E.A.; Largado, F.; Borja, J.B.; Kuzawa, C.W. Maternal characteristics associated with milk leptin content in a sample of Filipino women and associations with infant weight for age. J. Hum. Lact. 2015, 31, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; George, B.; Williams, M.; Whitaker, K.; Allison, D.B.; Teague, A.; Demerath, E.W. Associations between human breast milk hormones and adipocytokines and infant growth and body composition in the first 6 months of life. Pediatr. Obes. 2017, 12, 78–85. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Frasquet-Darrieux, M.; Gaud, M.A.; Christin, P.; Boquien, C.-Y.; Millet, C.; Herviou, M.; Darmaun, D.; Robins, R.J.; Ingrand, P.; et al. Higher leptin but not human milk macronutrient concentration distinguishes normal-weight from obese mothers at 1-month postpartum. PLoS ONE 2016, 11, e0168568. [Google Scholar] [CrossRef] [PubMed]
- Ucar, B.; Kirel, B.; Bor, O.; Kilic, F.S.; Dogruel, N.; Aydogdu, S.D.; Tekin, N. Breast milk leptin concentrations in initial and terminal milk samples: Relationships to maternal and infant plasma leptin concentrations, adiposity, serum glucose, insulin, lipid and lipoprotein levels. J. Pediatr. Endocrinol. Metab. 2000, 13, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Bielicki, J.; Huch, R.; von Mandach, U. Time-course of leptin levels in term and prteterm human milk. Eur. J. Endocrinol. 2004, 151, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, J.F.; Morley, P.; Willick, G.E. Bone growth stimulators: New tools for treating bone loss and mending fractures. Vitam. Horm. 2002, 65, 1–80. [Google Scholar] [PubMed]
- Smith-Kirwin, S.M.; O’Connor, D.M.; Johnston, J.; De Lancey, E.; Hassink, S.G.; Funanage, V.L. Leptin expression in human mammary epithelial cells and breast milk. J. Clin. Endocrinol. Metab. 1998, 83, 1810–1813. [Google Scholar] [CrossRef] [PubMed]
- Houseknecht, K.L.; McGuire, M.K.; Portocarrero, C.P.; McGuire, M.A.; Beerman, K. Leptin is present in human milk and is related to maternal plasma leptin concentration and adiposity. Biochem. Biophys. Res. Commun. 1997, 240, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Hassiotou, F.; Geddes, D.T. Programming of appetite control during breastfeeding as a preventative strategy against the obesity epidemic. J. Hum. Lact. 2014, 30, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Levek, C.; Reynolds, R.M.; Rudolph, M.C.; MacLean, P.; Hernandez, T.L.; Friedman, J.E.; Krebs, N.F. Bioactive components in human milk are differentially associated with rates of lean and fat mass deposition in infants of mothers with normal vs. elevated BMI. Pediatr. Obes. 2018. [Google Scholar] [CrossRef] [PubMed]




| Characteristic | 2 Months a | 5 Months b | 9 Months c | 12 Months d |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| (Range) | (Range) | (Range) | (Range) | |
| Mothers | ||||
| Weight (kg) | 78.8 ± 19.3 | 70.1 ± 17.8 | 63.0 ± 10.0 | 64.2 ± 17.3 |
| (57.5–116.2) | (53.7–115.3) | (50.4–121.9) | (51.4–121.9) | |
| BMI (kg/m2) | 27.2 ± 5.5 | 24.8 ± 5.0 | 22.7 ± 3.9 | 23.9 ± 5.9 |
| (20.4–35.5) | (19.0–35.2) | (17.9–37.2) | (18.2–37.2) | |
| Infants | ||||
| Sex (M/F) | 9M/6F | 10M/10F | 10M/9F | 9M/9F |
| Age (months) | 2.04 ± 0.14 | 5.16 ± 0.22 | 9.22 ± 0.27 | 12.26 ± 0.28 |
| (1.87–2.33) | (4.77–5.47) | (8.83–9.77) | (11.63–12.67) | |
| Length (cm) | 58.1 ± 1.9 | 64.8 ± 2.3 | 71.7 ± 1.9 | 73.6 ± 3.2 |
| (54.2–60.0) | (60.5–69.5) | (66.0–74.0) | (69.0–78.5) | |
| Weight (kg) | 5.630 ± 0.660 | 7.431 ± 1.134 | 8.836 ± 0.975 | 9.650 ± 0.618 |
| (4.420–7.400) | (5.808–9.510) | (6.675–10.095) | (7.165–11.085) | |
| BMI (kg/m2) | 16.6 ± 1.2 | 17.6 ± 1.9 | 17.7 ± 1.7 | 17.8 ± 0.9 |
| (14.5–18.1) | (14.9–20.4) | (14.2–20.2) | (13.7–19.2) | |
| Head circumference (cm) | 39.7 ± 1.6 | 42.1 ± 1.5 | 45.6 ± 1.7 | 46.6 ± 1.7 |
| (37.0–42.0) | (40.0–45.9) | (43.0–48.5) | (44.2–49.5) | |
| Breastfeeding characteristics | ||||
| 24-h milk intake (g) | n/a e | 818.8 ± 204.9 | 478.3 ± 154.0 | 451.1 ± 215.7 |
| (498–1185) | (300–775) | (255–795) | ||
| 24-h feeding frequency (MP) | n/a e | 8.1 ± 1.4 | 5.4 ± 1.3 | 4.4 ± 2.1 |
| (6–11) | (4–7) | (2–8) | ||
| Feeding frequency (SR) | 2.3 ± 0.4 f | 2.8 ± 0.8 | 3.7 ± 1.2 | 5.4 ± 2.9 |
| (1.5–3.0) | (1.5–4.0) | (2.0–6.0) | (2.2–12.0) | |
| Components | 2 Months | 5 Months | 9 Months | 12 Months |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| (Range) | (Range) | (Range) | (Range) | |
| Concentrations b | ||||
| Whole milk adiponectin (ng/mL) | 11.14 ± 5.79 c | 8.42 ± 1.69 | 8.44 ± 1.33 | 11.22 ± 4.22 |
| (6.61–21.56) | (6.18–22.58) | (6.41–12.86) | (5.66–19.38) | |
| Whole milk leptin (ng/mL) | 0.50 ± 0.18 | 0.49 ± 0.17 | 0.56 ± 0.11 | 0.50 ± 0.11 |
| (0.24–0.77) | (0.23–0.71) | (0.42–0.67) | (0.34–0.74) | |
| Skim milk leptin (ng/mL) | 0.34 ± 0.20 | 0.26 ± 0.08 | 0.21 ± 0.02 | 0.21 ± 0.03 |
| (0.20–0.84) | (0.20–0.40) | (0.19–0.27) | (0.19–0.40) | |
| CDI d | ||||
| Whole milk adiponectin (ng) | n/a e | 7976 ± 4480 d | 4446 ± 1645 | 3922 ± 1431 |
| (3771–22,439) | (2142–6673) | (2511–6352) | ||
| Whole milk leptin (ng) | n/a | 362 ± 173 | 280 ± 73 | 219 ± 90 |
| (162–841) | (132–349) | (122–350) | ||
| Skim milk leptin (ng) | n/a | 200 ± 81 | 114 ± 38 | 93 ± 36 |
| (106–402) | (62–172) | (51–159) | ||
| Characteristic | Months after Birth | ||||||
|---|---|---|---|---|---|---|---|
| 5 and 2 | 9 and 2 | 12 and 2 | 9 and 5 | 12 and 5 | 12 and 9 | p Overall | |
| Milk components | |||||||
| Whole milk adiponectin (ng/mL) | −1.01 (0.96) b 0.72 | −1.81 (0.98) 0.25 | 0.32 (1.05) 0.99 | −0.80 (0.90) 0.81 | 1.33 (0.96) 0.51 | 2.13 (0.98) 0.13 | 0.13 c |
| Whole milk leptin (ng/mL) | −0.04 (0.05) 0.87 | 0.05 (0.06) 0.74 | 0.02 (0.05) 0.98 | 0.08 (0.04) 0.22 | 0.05 (0.05) 0.65 | −0.03 (0.05) 0.92 | 0.29 |
| Skim milk leptin (ng/mL) | −0.06 (0.03) 0.22 | −0.10 (0.003) d 0.009 | −0.10 (0.03) 0.024 | −0.04 (0.03) 0.52 | 0.04 (0.03) 0.68 | 0.01 (0.03) 1.00 | 0.012 c |
| Breastfeeding characteristics | |||||||
| Feeding frequency (SR) e | 0.46 (0.53) 0.82 | 1.40 (0.54) 0.045 | 3.14 (0.58) <0.001 | 0.94 (0.46) 0.17 | 2.69 (0.50) <0.001 | 1.75 (0.51) 0.003 | <0.001 |
| Feeding frequency (MP) f | n/a g | n/a g | n/a g | −2.81 (0.49) <0.001 | −3.71 (0.46) <0.001 | −0.90 (0.52) 0.19 | <0.001 |
| 24-h milk intake (g) f | n/a | n/a | n/a | −325 (64) <0.001 | −376 (64) <0.001 | −52 (69) 0.73 | <0.001 |
| CDI of milk components | |||||||
| Whole milk adiponectin (ng) f | n/a | n/a | n/a | −3902 (1390) 0.023 | −4370 (1390) 0.010 | −467 (1621) 0.96 | 0.004 |
| Whole milk leptin (ng) f | n/a | n/a | n/a | −100 (58) 0.22 | −147 (58) 0.044 | −47 (68) 0.77 | 0.039 |
| Skim milk leptin (ng) f | n/a | n/a | n/a | −103 (29) 0.004 | −119 (29) <0.001 | −16 (34) 0.89 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gridneva, Z.; Kugananthan, S.; Rea, A.; Lai, C.T.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human Milk Adiponectin and Leptin and Infant Body Composition over the First 12 Months of Lactation. Nutrients 2018, 10, 1125. https://doi.org/10.3390/nu10081125
Gridneva Z, Kugananthan S, Rea A, Lai CT, Ward LC, Murray K, Hartmann PE, Geddes DT. Human Milk Adiponectin and Leptin and Infant Body Composition over the First 12 Months of Lactation. Nutrients. 2018; 10(8):1125. https://doi.org/10.3390/nu10081125
Chicago/Turabian StyleGridneva, Zoya, Sambavi Kugananthan, Alethea Rea, Ching Tat Lai, Leigh C. Ward, Kevin Murray, Peter E. Hartmann, and Donna T. Geddes. 2018. "Human Milk Adiponectin and Leptin and Infant Body Composition over the First 12 Months of Lactation" Nutrients 10, no. 8: 1125. https://doi.org/10.3390/nu10081125