Prevalence of Carnitine Deficiency and Decreased Carnitine Levels in Patients on Peritoneal Dialysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ramsay, R.R.; Arduini, A. The Carnitine Acyltransferases and Their Role in Modulating Acyl-CoA Pools. Arch. Biochem. Biophys. 1993, 302, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Bonomini, M.; Zammit, V.; Pusey, C.D.; Vecchi, A.; Arduini, A. Pharmacological use of l-carnitine in uremic anemia: Has its full potential been exploited? Pharm. Res. 2011, 63, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Tanphaichitr, V.; Leelahagul, P. Carnitine metabolism and human carnitine deficiency. Nutrition 1993, 9, 246–254. [Google Scholar] [PubMed]
- Ramsay, R. The carnitine acyltransferases: Modulators of acyl-CoA-dependent reactions. Biochem. Soc. Trans. 2000, 28, 182–186. [Google Scholar] [CrossRef]
- Flanagan, J.L.; Simmons, P.A.; Vehige, J.; Willcox, M.D.; Garrett, Q. Role of carnitine in disease. Nutr. Metab. 2010, 7, 30. [Google Scholar] [CrossRef]
- Kudoh, Y.; Aoyama, S.; Torii, T.; Chen, Q.; Nagahara, D.; Sakata, H.; Nozawa, A. Hemodynamic stabilizing effects of L-carnitine in chronic hemodialysis patients. Cardiorenal Med. 2013, 3, 200–207. [Google Scholar] [CrossRef]
- Yang, S.K.; Xiao, L.; Song, P.A.; Xu, X.; Liu, F.Y.; Sun, L. Effect of L-carnitine therapy on patients in maintenance hemodialysis: A systematic review and meta-analysis. J. Nephrol. 2014, 27, 317–329. [Google Scholar] [CrossRef]
- Hatanaka, Y.; Higuchi, T.; Akiya, Y.; Horikami, T.; Tei, R.; Furukawa, T.; Takashima, H.; Tomita, H.; Abe, M. Prevalence of carnitine deficiency and decreased carnitine levels in patients on hemodialysis. Blood Purif. 2019, 47, 38–44. [Google Scholar] [CrossRef]
- Moorthy, A.V.; Rosenblum, M.; Rajaram, R.; Shug, A.L. A comparison of plasma and muscle carnitine levels in patients on peritoneal or hemodialysis for chronic renal failure. Am. J. Nephrol. 1983, 3, 205–208. [Google Scholar] [CrossRef]
- Constantin-Teodosiu, D.; Kirby, D.P.; Short, A.H.; Burden, R.P.; Morgan, A.G.; Greenhaff, P.L. Free and esterified carnitine in continuous ambulatory peritoneal dialysis patients. Kidney Int. 1996, 49, 158–162. [Google Scholar] [CrossRef] [Green Version]
- Sotirakopoulos, N.; Athanasiou, G.; Tsitsios, T.; Mavromatidis, K. The influence of L-carnitine supplementation on hematocrit and hemoglobin levels in patients with end stage renal failure on CAPD. Ren. Fail. 2002, 24, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.M.; Faull, R.J.; Nation, R.L.; Prasad, S.; Elias, T.; Reuter, S.E.; Fornasini, G. Impact of hemodialysis on endogenous plasma and muscle carnitine levels in patients with end-stage renal disease. Kidney Int. 2004, 66, 1527–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, A. Dialysis-related carnitine disorder and levocarnitine pharmacology. Am. J. Kidney Dis. 2003, 41, 13–26. [Google Scholar] [CrossRef]
- Grzegorzewska, A.E.; Mariak, I.; Dobrowolska-Zachwieja, A. Continuous ambulatory peritoneal dialysis (CAPD) adequacy influences serum free carnitine level. Int. Urol. Nephrol. 1999, 31, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Eknoyan, G.; Latos, D.L.; Lindberg, J. Practice recommendations for the use of L-carnitine in dialysis-related carnitine disorder. National Kidney Foundation Carnitine Consensus Conference. Am. J. Kidney Dis. 2003, 41, 868–876. [Google Scholar] [CrossRef]
- Takahashi, M.; Ueda, S.; Misaki, H.; Sugiyama, N.; Matsumoto, K.; Matsuo, N.; Murao, S. Carnitine determination by an enzymatic cycling method with carnitine dehydrogenase. Clin. Chem. 1994, 40, 817–821. [Google Scholar]
- Japan Pediatric Society. Available online: http://www.jpeds.or.jp/uploads/files/20181207_shishin.pdf (accessed on 21 September 2019).
- Kosan, C.; Sever, L.; Arisoy, N.; Caliskan, S.; Kasapcopur, O. Carnitine supplementation improves apolipoprotein B levels in pediatric peritoneal dialysis patients. Pediatric Nephrol. 2003, 18, 1184–1188. [Google Scholar] [CrossRef]
- Pliakogiannis, T.; Chatzidimitriou, C.; Evabgelious, A.; Boyles, H.J.; Kalaitzidis, K. Serum carnitine levels, lipid profile, and metabolic status of patients on continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 1993, 13, 440–443. [Google Scholar]
- Guarnieri, G.; Situlin, R.; Biolo, G. Carnitine metabolism in uremia. Am. J. Kidney Dis. 2001, 38, 63–67. [Google Scholar] [CrossRef]
- Guarnieri, G.; Biolo, G.; Vinci, P.; Massolino, B.; Barazzoni, R. Advances in carnitine in chronic uremia. J. Ren. Nutr. 2007, 17, 23–29. [Google Scholar] [CrossRef]
- Naseri, M.; Shahri, H.M.M.; Horri, M.; Esmaeeli, M.; Sherbaf, F.G.; Jahanshahi, S.; Moeenolroayaa, G.; Rasoli, Z.; Salemian, F.; Pour Hasan, M. Absolute and relative carnitine deficiency in patients on hemodialysis and peritoneal dialysis. Iran. J. Kidney Dis. 2016, 10, 36–43. [Google Scholar] [PubMed]
- Leschke, M.; Rumpf, K.W.; Eisenhauer, T.; Fuchs, C.; Becker, K.; Köthe, U.; Scheler, F. Quantitative assessment of carnitine loss during hemodialysis and hemofiltration. Kidney Int. Suppl. 1983, 16, 143–146. [Google Scholar]
- Di Liberato, L.; Arduini, A.; Rossi, C.; Di Castelnuovo, A.; Posari, C.; Sacchetta, P.; Urbani, A.; Bonomini, M. L-carnitine status in end-stage renal disease patients on automated peritoneal dialysis. J. Nephrol. 2014, 27, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, T. Effects of levocarnitine on cardiac function and renal anemia in hemodialysis patients. Contrib. Nephrol. 2018, 196, 96–100. [Google Scholar] [PubMed]
- Higuchi, T.; Abe, M.; Yamazaki, T.; Mizuno, M.; Okawa, E.; Ando, H.; Oikawa, O.; Okada, K.; Kikuchi, F.; Soma, M. Effects of levocarnitine on brachial-ankle pulse wave velocity in hemodialysis patients: A randomized controlled trial. Nutrients 2014, 6, 5992–6004. [Google Scholar] [CrossRef]
- Maruyama, T.; Maruyama, N.; Higuchi, T.; Nagura, C.; Takashima, H.; Kitai, M.; Utsunomiya, K.; Tei, R.; Furukawa, T.; Yamazaki, T.; et al. Efficacy of L-carnitine supplementation for improving lean body mass and physical function in patients on hemodialysis: A randomized controlled trial. Eur. J. Clin. Nutr. 2019, 73, 293–301. [Google Scholar] [CrossRef]
- Higuchi, T.; Abe, M.; Yamazaki, T.; Okawa, E.; Ando, H.; Hotta, S.; Oikawa, O.; Kikuchi, F.; Okada, K.; Soma, M. Levocarnitine improves cardiac function in hemodialysis patients with left ventricular hypertrophy: A randomized controlled trial. Am. J. Kidney Dis. 2016, 67, 260–270. [Google Scholar] [CrossRef]
- Maruyama, T.; Higuchi, T.; Yamazaki, T.; Okawa, E.; Ando, H.; Oikawa, O.; Inoshita, A.; Okada, K.; Abe, M. Levocarnitine injections decrease the need for erythropoiesis-stimulating agents in hemodialysis patients with renal anemia. Cardiorenal Med. 2017, 7, 188–197. [Google Scholar] [CrossRef]
- Lilien, M.R.; Duran, M.; Quak, J.M.; Frankhuisen, J.J.; Schroder, C.H. Oral L-carnitine does not decrease erythropoietin requirement in pediatric dialysis. Pediatric Nephrol. 2000, 15, 17–20. [Google Scholar] [CrossRef]
- Davies, S.J.; Phillips, L.; Griths, A.; Russell, L.H.; Naish, P.F.; Russell, G.I. What really happens to people on long-term peritoneal dialysis? Kidney Int. 1998, 54, 2207–2217. [Google Scholar] [CrossRef] [Green Version]
- Burkart, J. Metabolic consequences of peritoneal dialysis. Semin. Dial. 2004, 17, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Krediet, R.T.; Balafa, O. Cardiovascular risk in the peritoneal dialysis patients. Nat. Rev. Nephrol. 2010, 6, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Wang, I.K.; Lin, C.L.; Chen, H.C.; Lin, S.Y.; Chang, C.T.; Yen, T.H.; Sung, F.C. Risk of new-onset diabetes in end-stage renal disease patients undergoing dialysis: Analysis from registry data of Taiwan. Nephrol. Dial. Transpl. 2018, 33, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Hagen, T.; Boyle, C.A.; Vonesh, E.; Hamburger, R.; Charytan, C.; Sandroni, S.; Bernard, D.; Piraino, B.; Schreiber, M.; et al. Treatment of malnutrition with 1.1% amino acid peritoneal dialysis solution: Results of a multicenter outpatient study. Am. J. Kidney Dis. 1998, 32, 761–769. [Google Scholar] [CrossRef]
- Johnson, D.W.; Agar, J.; Collins, J.; Disney, A.; Harris, D.C.; Ibels, L.; Irish, A.; Saltissi, D.; Suranyi, M. Recommendations for the use of icodextrin in peritoneal dialysis patients. Nephrology 2003, 8, 1–7. [Google Scholar] [CrossRef]
- Bonomini, M.; Di Liberato, L.; Zammit, V.; Arduini, A. Current opinion on usage of L-carnitine in end-stage renal disease patients on peritoneal dialysis. Molecules 2019, 24, 3449. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | PD Group | HD Group | p Value |
|---|---|---|---|
| N (Male/Female) | 34 (25/9) | 34 (25/9) | 1.000 |
| Age (years) | 61.5 ± 16.4 | 64.2 ± 12.8 | 0.467 |
| Duration of dialysis(m) | 13.0 (8.5–29.5) | 19.0 (8.0–54.0) | 0.122 |
| History of CVD n (%) | 5 (14.7) | 6 (17.6) | 0.742 |
| Smoking, n (%) | 6 (17.7) | 7 (20.6) | 0.758 |
| Alcohol use, n (%) | 5 (14.7) | 7 (20.6) | 0.524 |
| Systolic BP (mmHg) | 141 ± 15 | 143 ± 14 | 0.661 |
| Diastolic BP (mmHg) | 81 ± 10 | 80 ± 10 | 0.752 |
| Heart rate (bpm) | 72 ± 10 | 73 ± 10 | 0.706 |
| Body mass index (kg/m2) | 23.1 ± 4.0 | 22.2 ± 4.0 | 0.402 |
| Anuria, n (%) | 9 (26.5) | 15 (44.1) | 0.128 |
| Causes of ESKD, n (%) | 0.694 | ||
| Diabetes mellitus | 10 (29.5) | 8 (23.5) | |
| Chronic glomerular nephritis | 8 (23.5) | 9 (26.5) | |
| Nephrosclerosis | 13 (38.2) | 11 (32.3) | |
| Others | 3 (8.8) | 6 (17.7) | |
| Medications, n (%) | |||
| RAS inhibitor | 25 (73.5) | 28 (82.3) | 0.380 |
| Active vitamin D | 22 (64.7) | 25 (73.5) | 0.431 |
| Phosphate binders | 29 (85.3) | 31 (91.2) | 0.452 |
| Statin | 12 (35.2) | 15 (44.1) | 0.461 |
| Variables | PD Group | HD Group | p Value |
|---|---|---|---|
| sUN (mg/dL) | 51 ± 15 | 56 ± 13 | 0.180 |
| Creatinine (mg/dL) | 8.9 ± 3.8 | 10.1 ± 3.3 | 0.214 |
| Total protein (g/dL) | 6.3 ± 0.7 | 6.6 ± 0.5 | 0.038 * |
| Albumin (g/dL) | 3.3 ± 0.5 | 3.5 ± 0.5 | 0.018 * |
| Sodium (mEq/L) | 138 ± 4.0 | 141 ± 3.1 | 0.001 ** |
| Potassium (mEq/L) | 4.3 ± 0.6 | 4.8 ± 0.7 | 0.002 ** |
| Calcium (mg/dL) | 9.0 ± 0.6 | 9.0 ± 0.8 | 0.788 |
| Phosphate (mg/dL) | 5.6 ± 1.4 | 5.2 ± 1.1 | 0.211 |
| CRP (md/dL) | 0.11 (0.1–0.6) | 0.11 (0.1–0.5) | 0.976 |
| Total-cholesterol (mg/dL) | 180 ± 40 | 153 ± 32 | 0.004 ** |
| HDL-cholesterol (mg/dL) | 55 ± 16 | 36 ± 15 | <0.001 |
| Triglyceride (mg/dL) | 94 (70–140) | 115 (88–163) | 0.300 |
| Hemoglobin (g/dL) | 10.9 ± 1.3 | 10.8 ± 0.9 | 0.735 |
| Iron (μg/dL) | 83 ± 32 | 84 ± 33 | 0.906 |
| TSAT (%) | 33.1 ± 16.5 | 35.4 ± 14.7 | 0.752 |
| Ferritin (ng/mL) | 114 (37–185) | 94 (50–151) | 0.622 |
| Zinc (μg/dL) | 58 ± 10 | 56 ± 8 | 0.413 |
| ESA (μg/m) | 120 (50–172) | 120 (80–160) | 0.065 |
| β2-MG (mg/L) | 25 ± 11 | 26 ± 8 | 0.816 |
| Kt/V renal | 0.15 (0.05–0.96) | - | - |
| Kt/V PD | 1.1 ± 0.4 | - | - |
| Kt/V total | 1.7 ± 0.7 | - | - |
| Kt/V HD | - | 1.3 ± 0.2 | - |
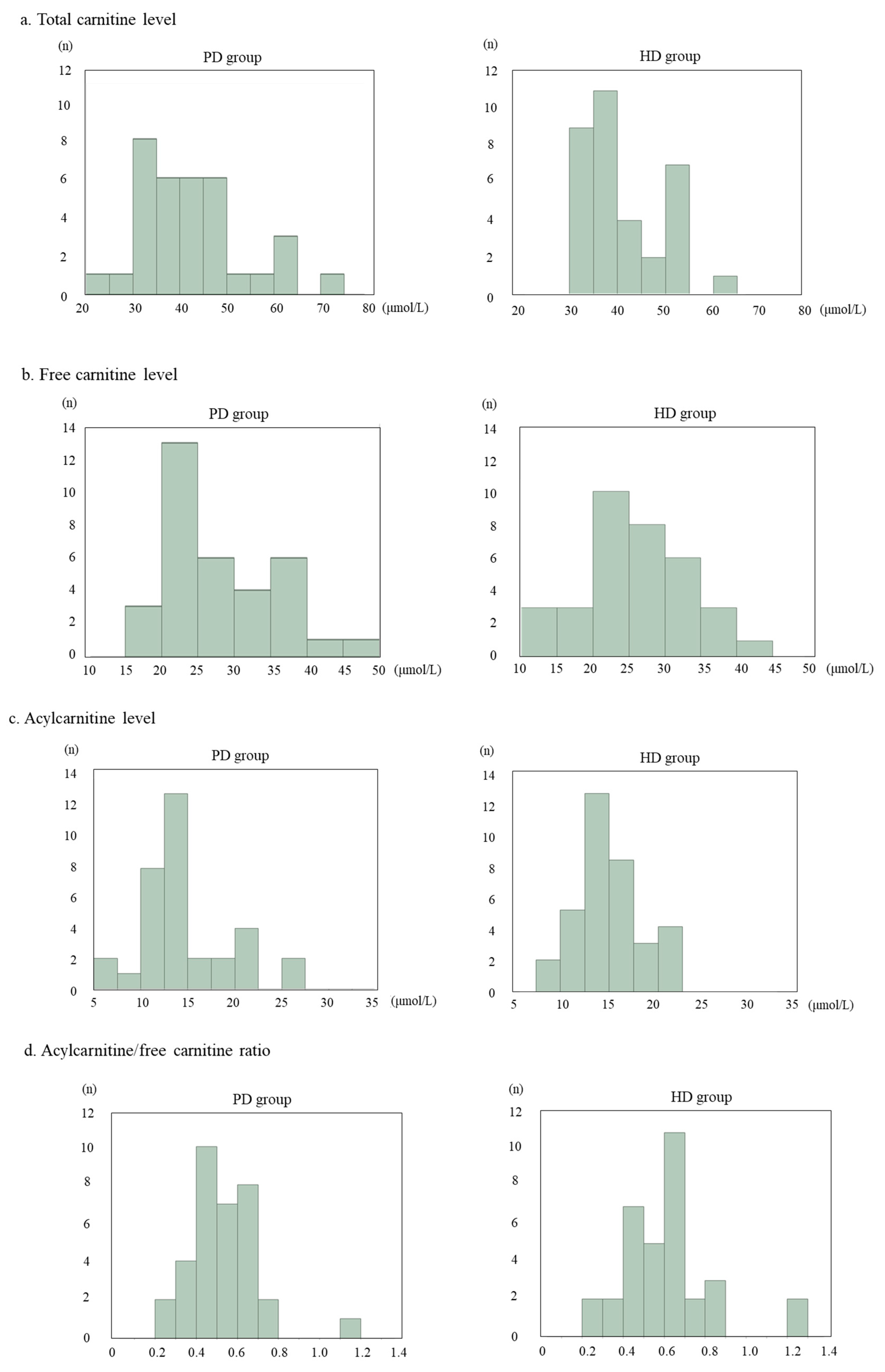
| Total carnitine (μmol/L) | 42.5 ± 11.2 | 41.0 ± 8.2 | 0.535 |
| Free carnitine (μmol/L) | 28.0 ± 7.8 | 25.6 ± 7.4 | 0.203 |
| Acyl carnitine (μmol/L) | 14.5 ± 4.8 | 15.0 ± 3.3 | 0.634 |
| Acyl/free carnitine ratio | 0.52 ± 0.16 | 0.62 ± 0.22 | 0.069 |
| Variables | Estimate | SE | t | 95%CI | p Value | |
|---|---|---|---|---|---|---|
| Age | −3.60 | 1.68 | −2.13 | −7.06 | −0.13 | 0.041 * |
| Female | −0.94 | 1.45 | −0.65 | −3.91 | 2.02 | 0.520 |
| Duration of dialysis | −0.15 | 0.06 | −2.53 | −0.28 | −0.03 | 0.016 * |
| Body mass index | −0.02 | 0.18 | −0.19 | −0.24 | 0.19 | 0.849 |
| Serum urea nitrogen | 0.05 | 0.12 | 0.37 | −0.21 | 0.31 | 0.716 |
| Creatinine | 0.60 | 0.71 | 0.85 | −0.82 | 2.08 | 0.398 |
| Hemoglobin | −0.78 | 1.50 | −0.55 | −3.82 | 2.25 | 0.603 |
| Albumin | 1.85 | 3.12 | 0.6 | −4.45 | 8.12 | 0.557 |
| Calcium | −0.94 | 1.72 | −0.55 | −4.41 | 2.53 | 0.587 |
| Phosphate | −0.93 | 1.90 | −0.49 | −4.47 | 2.9 | 0.625 |
| C-reactive protein | −0.67 | 1.42 | −0.47 | −3.55 | 2.22 | 0.472 |
| HDL-cholesterol | −0.06 | 0.09 | −0.73 | −0.25 | 0.11 | 0.468 |
| β2-MG | −0.28 | 0.18 | −1.57 | −0.65 | 0.08 | 0.123 |
| Kt/V total | 0.94 | 0.71 | 0.38 | −4.04 | 5.92 | 0.703 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, S.; Takashima, H.; Tei, R.; Furukawa, T.; Okamura, M.; Kitai, M.; Nagura, C.; Maruyama, T.; Higuchi, T.; Abe, M. Prevalence of Carnitine Deficiency and Decreased Carnitine Levels in Patients on Peritoneal Dialysis. Nutrients 2019, 11, 2645. https://doi.org/10.3390/nu11112645
Shimizu S, Takashima H, Tei R, Furukawa T, Okamura M, Kitai M, Nagura C, Maruyama T, Higuchi T, Abe M. Prevalence of Carnitine Deficiency and Decreased Carnitine Levels in Patients on Peritoneal Dialysis. Nutrients. 2019; 11(11):2645. https://doi.org/10.3390/nu11112645
Chicago/Turabian StyleShimizu, Satoshi, Hiroyuki Takashima, Ritsukou Tei, Tetsuya Furukawa, Makiyo Okamura, Maki Kitai, Chinami Nagura, Takashi Maruyama, Terumi Higuchi, and Masanori Abe. 2019. "Prevalence of Carnitine Deficiency and Decreased Carnitine Levels in Patients on Peritoneal Dialysis" Nutrients 11, no. 11: 2645. https://doi.org/10.3390/nu11112645