Animal Source Food Consumption in Young Children from Four Regions of Ethiopia: Association with Religion, Livelihood, and Participation in the Productive Safety Net Program


Abstract
:1. Introduction
2. Methods
2.1. Study Setting
2.2. Study Design
2.3. Sample Size
2.4. Sampling
2.5. Data Collection Methods and Tools
2.6. Ethics
2.7. Measures
2.7.1. Outcomes
2.7.2. Independent Variables
2.8. Analysis
3. Results
3.1. Participant Characteristics
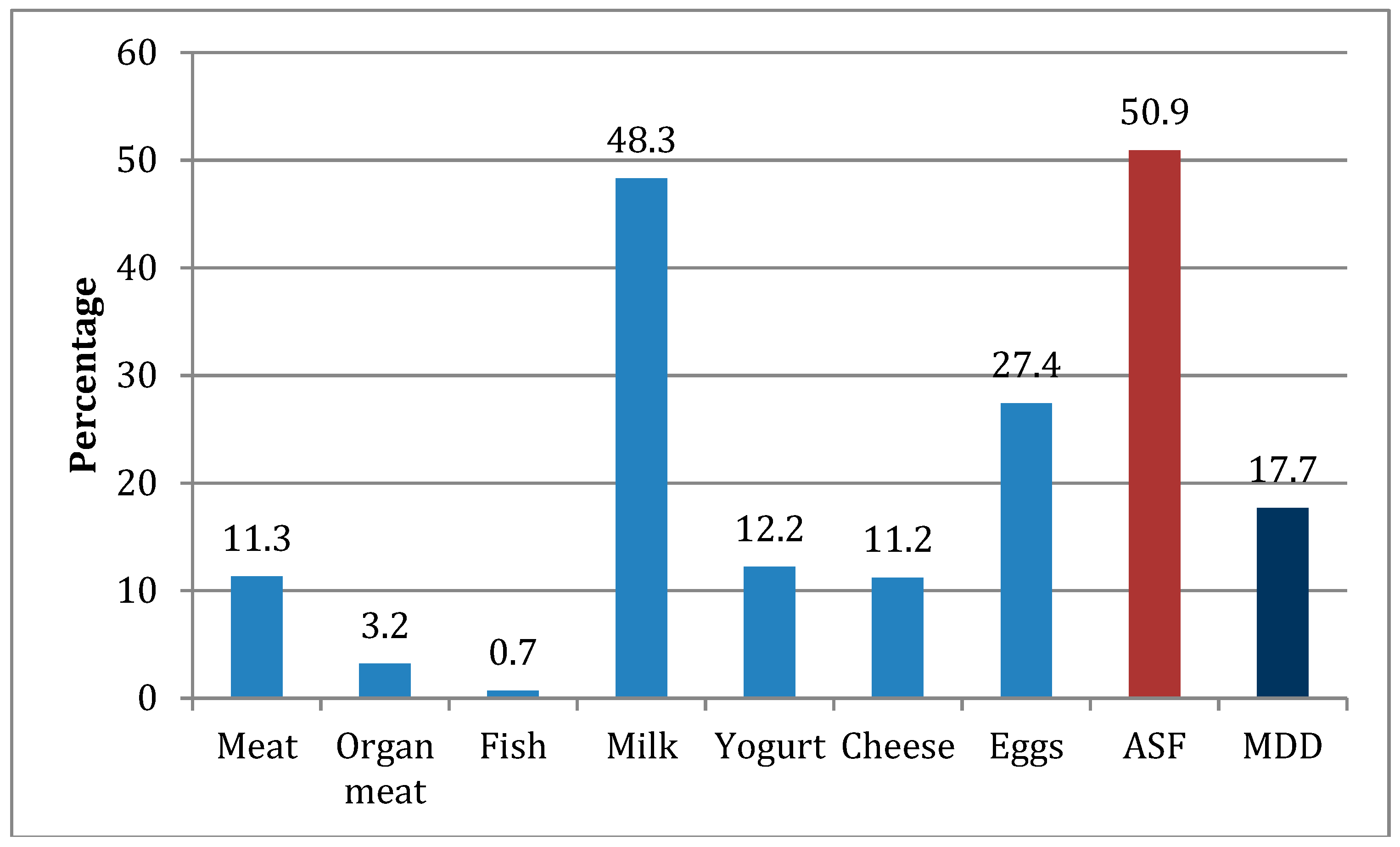
3.2. ASF and MDD
3.3. Unadjusted Associations
3.4. Adjusted Associations
4. Discussion
Strengths and Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund (UNICEF); World Health Organization; The World Bank Group. Levels and Trends in Child Malnutrition: Key Findings of the 2018 Edition of the Joint Child Malnutrition Estimates; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Victora, C.G.; Sibbritt, D.; Horta, B.L.; Lima, R.C.; Cole, T.; Wells, J. Weight gain in childhood and body composition at 18 years of age in Brazilian males. Acta Paediatr. 2007, 96, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Begum, K. Long-term consequences of stunting in early life. Matern. Child Nutr. 2011, 7, 5–18. [Google Scholar] [CrossRef]
- United Nations. Sustainable Development Goals: 17 Goals to Transform Our World. Available online: https://www.un.org/sustainabledevelopment/sustainable-development-goals/ (accessed on 18 July 2018).
- Central Statistical Agency Ethiopia; ICF International. Ethiopia Demographic and Health Survey 2016; The DHS Program: Rockville, MD, USA, 2016.
- African Union Commission; NEPAD Planning and Coordinating Agency; UN Economic Commission for Africa; UN World Food Programme. The Cost of Hunger in Africa: Social and Economic Impact of Child Undernutrition in Egypt, Ethiopia, Swaziland and Uganda; UNECA: Addis Ababa, Ethiopia, 2014. [Google Scholar]
- Begin, F.; Aguayo, V.M. First foods: Why improving young children’s diets matter. Matern. Child Nutr. 2017, 13 (Suppl. 2). [Google Scholar] [CrossRef] [PubMed]
- Ruel, M.T.; Menon, P. Child feeding practices are associated with child nutritional status in Latin America: Innovative uses of the demographic and health surveys. J. Nutr. 2002, 132, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Arimond, M.; Ruel, M.T. Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. J. Nutr. 2004, 134, 2579–2585. [Google Scholar] [CrossRef]
- Marriott, B.P.; White, A.; Hadden, L.; Davies, J.C.; Wallingford, J.C. World Health Organization (WHO) infant and young child feeding indicators: Associations with growth measures in 14 low-income countries. Matern. Child Nutr. 2012, 8, 354–370. [Google Scholar] [CrossRef]
- World Health Organization; Akre, J. Infant Feeding: The Physiological Basis. In Bulletin of the World Health Organization; World Health Organization: Geneva, Switzerland, 1989; Volume 67. [Google Scholar]
- Murphy, S.P.; Allen, L.H. Nutritional Importance of Animal Source Foods. J. Nutr. 2003, 133, 3932S–3935S. [Google Scholar] [CrossRef]
- Ruel, M.T. Operationalizing dietary diversity: A review of measurement issues and research priorities. J. Nutr. 2003, 133, 3911s–3926s. [Google Scholar] [CrossRef]
- Darapheak, C.; Takano, T.; Kizuki, M.; Nakamura, K.; Seino, K. Consumption of animal source foods and dietary diversity reduce stunting in children in Cambodia. Int. Arch. Med. 2013, 6, 29. [Google Scholar] [CrossRef]
- Zhang, Z.; Goldsmith, P.D.; Winter-Nelson, A. The Importance of Animal Source Foods for Nutrient Sufficiency in the Developing World: The Zambia Scenario. Food Nutr. Bull. 2016, 37, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K.; Allen, L.H. The Importance of Milk and other Animal-Source Foods for Children in Low-Income Countries. Food Nutr. Bull. 2011, 32, 227–243. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices. Part. I: Definitions; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Herrador, Z.; Perez-Formigo, J.; Sordo, L.; Gadisa, E.; Moreno, J.; Benito, A.; Aseffa, A.; Custodio, E. Low Dietary Diversity and Intake of Animal Source Foods among School Aged Children in Libo Kemkem and Fogera Districts, Ethiopia. PLoS ONE 2015, 10, e0133435. [Google Scholar] [CrossRef]
- Gashu, D.; Stoecker, B.J.; Adish, A.; Haki, G.D.; Bougma, K.; Marquis, G.S. Ethiopian pre-school children consuming a predominantly unrefined plant-based diet have low prevalence of iron-deficiency anaemia. Public Health Nutr. 2016, 19, 1834–1841. [Google Scholar] [CrossRef] [PubMed]
- Workicho, A.; Belachew, T.; Feyissa, G.T.; Wondafrash, B.; Lachat, C.; Verstraeten, R.; Kolsteren, P. Household dietary diversity and Animal Source Food consumption in Ethiopia: Evidence from the 2011 Welfare Monitoring Survey. BMC Public Health 2016, 16, 1192. [Google Scholar] [CrossRef] [PubMed]
- Ali, D.; Saha, K.K.; Nguyen, P.H.; Diressie, M.T.; Ruel, M.T.; Menon, P.; Rawat, R. Household Food Insecurity Is Associated with Higher Child Undernutrition in Bangladesh, Ethiopia, and Vietnam, but the Effect Is Not Mediated by Child Dietary Diversity. J. Nutr. 2013, 143, 2015–2021. [Google Scholar] [CrossRef]
- Chotard, S.; Mason, J.B.; Oliphant, N.P.; Mebrahtu, S.; Hailey, P. Fluctuations in wasting in vulnerable child populations in the Greater Horn of Africa. Food Nutr. Bull. 2010, 31, S219–S233. [Google Scholar] [CrossRef]
- Central Statistical Agency Ethiopia; ICF International. Ethiopia Demographic and Health Survey 2011; Central Statistical Agency and ICF International: Calverton, MD, USA, 2012.
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Dewey, K.G.; Adu-Afarwuah, S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern. Child Nutr. 2008, 4, 24–85. [Google Scholar] [CrossRef]
- Federal Democratic Republic of Ethiopia. Food and Nutrition Policy; Government of Ethiopia: Addis Ababa, Ethiopia, 2018.
- Federal Democratic Republic of Ethiopia; National Nutrition Coordinating Body. National Nutrition Programme 2016–2020; Government of Ethiopia: Addis Ababa, Ethiopia, 2016.
- Federal Democratic Republic of Ethiopia; Ministry of Agriculture and Livestock Resources. National Nutrition Sensitive Agriculture Strategy; Government of Ethiopia: Addis Ababa, Ethiopia, 2017.
- Federal Democratic Republic of Ethiopia. Seqota Declaration, Implementation Plan. (2016–2030): Summary Programme Approach Document; Government of Ethiopia: Addis Ababa, Ethiopia, 2016.
- Federal Democratic Republic of Ethiopia; Ministry of Agriculture. Productive Safety Net Programme Phase IV Programme Implementation Manual; Government of Ethiopia: Addis Ababa, Ethiopia, 2014.
- White, J.; Mason, J.B. Assessing the impact on child nutrition of the Ethiopia Community-based Nutrition Program; Tulane University: New Orleans, LA, USA, 2012. [Google Scholar]
- Kim, S.S.; Rawat, R.; Mwangi, E.M.; Tesfaye, R.; Abebe, Y.; Baker, J.; Frongillo, E.A.; Ruel, M.T.; Menon, P. Exposure to Large-Scale Social and Behavior Change Communication Interventions Is Associated with Improvements in Infant and Young Child Feeding Practices in Ethiopia. PLoS ONE 2016, 11, e0164800. [Google Scholar] [CrossRef] [PubMed]
- Central Intelligence Agency. The World Factbook, Country Profiles: Ethiopia. Available online: https://www.cia.gov/library/publications/the-world-factbook/geos/et.html (accessed on 19 July 2018).
- Sadler, K.; Catley, A. Milk Matters: The Role and Value of Milk in the Diets of Somali Pastoralist Children in Liben and Shinile, Ethiopia; Feinstein International Center, Tufts University and Save the Children, Addis Ababa: Sommerville, MA, USA, 2009. [Google Scholar]
- Ali, D.; Tedla, M.; Subandoro, A.; Bamezai, A.; Rawat, R.; Menon, P. Alive & Thrive Baseline Survey Report: Ethiopia; Alive & Thrive: Washington, DC, USA, 2011. [Google Scholar]
- Fabrizio, C.S.; Van Liere, M.; Pelto, G. Identifying determinants of effective complementary feeding behaviour change interventions in developing countries. Matern. Child Nutr. 2014, 10, 575–592. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.; Potts, K.; Crum, J.; Hofer, R.; Saldanha, L. Analysis of the Nutrition Sector in Ethiopia. A Report to UNICEF and EU; Tulane School of Public Health and Tropical Medicine, Department of Global Community Health and Behavioral Sciences: New Orleans, LA, USA, July 2015. [Google Scholar]
- Reich, N.G.; Myers, J.A.; Obeng, D.; Milstone, A.M.; Perl, T.M. Empirical Power and Sample Size Calculations for Cluster-Randomized and Cluster-Randomized Crossover Studies. PLoS ONE 2012, 7, e35564. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide (v. 3); FHI 360, Food and Nutrition Technical Assistance Project: Washington, DC, USA, 2007. [Google Scholar]
- Swindale, A.; Bilinsky, P. Development of a universally applicable household food insecurity measurement tool: Process, current status, and outstanding issues. J. Nutr. 2006, 136, 1449s–1452s. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2000. [Google Scholar]
- Alive & Thrive. IYCF Practices, Beliefs, and Influences in Tigray Region, Ethiopia; Alive & Thrive: Addis Ababa, Ethiopia, 2010. [Google Scholar]
- The Ethiopian Orthodox Tewahedo Church Faith and Order. Worship in the Ethiopian Orthodox Church. Available online: http://www.ethiopianorthodox.org/english/ethiopian/worship.html (accessed on 8 June 2018).
- Kumera, G.; Tsedal, E.; Ayana, M. Dietary diversity and associated factors among children of Orthodox Christian mothers/caregivers during the fasting season in Dejen District, North West Ethiopia. Nutr. Metabol. 2018, 15, 16. [Google Scholar] [CrossRef]
- Alive & Thrive. Alive & Thrive Engages Church Leaders to Improve Nutrition in Ethiopia’s Amhara Region. Available online: https://www.aliveandthrive.org/resources/alive-thrive-engages-church-leaders-to-improve-nutrition-in-ethiopias-amhara-region/ (accessed on 16 July 2018).
- Disha, A.; Tharaney, M.; Abebe, Y.; Alayon, S.; Winnard, K. Factors Associated with Infant and Young Child Feeding Practices in Amhara Region and Nationally in Ethiopia: Analysis of the 2005 and 2011 Demographic and Health Surveys; Alive & Thrive: Washington, DC, USA, 2015. [Google Scholar]
- Webb, P.; Braun, J.V. The Pastoral Experience. Famine and food Security in Ethiopia: Lessons for Africa; Wiley & Sons Ltd.: Chichester, UK, 1994; pp. 85–98. [Google Scholar]
- Save the Children UK; Mayer, A.-M. The Causes of Malnutrition in Children under 3 in the Somali Region of Ethiopia Related to Household Caring Practices: Preliminary Report; Report on research findings from Somali Caring Practices research project in Shinile and Dambal districts of Shinile zone, Somali region, Ethiopia; Save the Children: Addis Ababa, Ethiopia, 2007. [Google Scholar]
- Disaster Prevention and Preparedness Bureau Ethiopia; Save the Children UK. Filtu-Dolow Pastoral Livelihood Zone: An HEA Baseline Study; Disaster Prevention and Preparedness Bureau Ethiopia, Save the Children: Addis Ababa, Ethiopia, 2002. [Google Scholar]
- Sadler, K.; Mitchard, E.; Abdi, A.; Shiferaw, Y.; Bekele, G.; Catley, A. Milk Matters: The Impact of Dry Season Livestock Support on Milk Supply and Child Nutrition in Somali Region, Ethiopia; Feinstein International Center, Tufts University, Save the Children: Sommerville, MA, USA, 2012. [Google Scholar]
- Devereux, S. Vulnerable Livelihoods in the Somali Regio, Ethiopia; Institute of Development Studies: Brighton, UK, 2006. [Google Scholar]
- Mengistu, G.; Moges, T.; Samuel, A.; Baye, K. Energy and nutrient intake of infants and young children in pastoralist communities of Ethiopia. Nutrition 2017, 41, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization of the United Nations. Nutrition and Social Proetction; Food and Agriculture Organization of the United Nations: Rome, Italy, 2015. [Google Scholar]
- Save the Children. A Chance to Grow: How Social Protection Can Tackle Child Malnutrition and Promote Economic Opportunities; Save the Children UK: London, UK, 2012. [Google Scholar]
- Alderman, H.; Hoogeveen, H.; Rossi, M. Reducing child malnutrition in Tanzania combined effects of income growth and program interventions. Econ. Hum. Biol. 2006, 4, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Ruel, M.T.; Alderman, H. Nutrition-sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? Lancet 2013, 382, 536–551. [Google Scholar] [CrossRef]
- Gilligan, D.O.; Hoddinot, J.; Taffesse, A.S. The Impact of Ethiopia’s Productive Safety Net Programme and its Linkages; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2008. [Google Scholar]
- Debela, B.L.; Shively, G.; Holden, S.T. Does Ethiopia’s Productive Safety Net Program improve child nutrition? Food Secur. 2015, 7, 1273–1289. [Google Scholar] [CrossRef]
- Berhane, G.; Hoddinott, J.; Kumar, N. The Impact of Ethiopia’s Productive Safety Net Programme on the Nutritional Status of Children: 2008–2012; The International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2016. [Google Scholar]
- Gebrehiwot, T.; Castilla, C. Do Safety Net Transfers Improve Diets and Reduce Undernutrition? Evidence from Rural Ethiopia. J. Dev. Stud. 2018, 1–20. [Google Scholar] [CrossRef]


{kind=link}
| ASF Consumption | ||||
|---|---|---|---|---|
| Variable (Missing) | No | Yes | Total | |
| n (row %) a | n (row %) a | p-Value | n (col %) a | |
| Child Characteristics | ||||
| Sex of child (6) | 0.6995 b | |||
| Male | 257 (48.7) | 271 (51.3) | 528 (52.6) | |
| Female | 237 (49.9) | 238 (50.1) | 475 (47.4) | |
| Age of child in months (0) | ||||
| Mean (SD) | 18.6 (8.84) | 20.7 (8.45) | 0.0001 c | 19.6 (8.7) |
| Median (Q1, Q3) | 17 (10, 25) | 21 (13, 27) | 20 (12, 26) | |
| Caretaker and Household Characteristics | ||||
| Respondent age in years (39) | ||||
| Mean (SD) | 29.0 (6.3) | 29.6 (6.3) | 0.0979 c | 29.3 (6.3) |
| Median (Q1, Q3) | 28 (25, 32) | 30 (25, 34) | 29 (25, 33) | |
| Total number of children (168) | ||||
| Mean (SD) | 4.0 (1.9) | 3.9 (2.0) | 0.8391 c | 4.0 (1.9) |
| Median (Q1, Q3) | 4 (3, 5) | 4 (2.5, 5) | 0.5721 d | 4 (3, 5) |
| Respondent Education (8) | 0.2367 b | |||
| No education | 322 (47.9) | 351 (52.2) | 673 (67.2) | |
| Any education | 170 (51.8) | 158 (48.2) | 328 (32.8) | |
| Number of household assets (29) | ||||
| Mean (SD) | 1.3 (1.4) | 1.5 (1.6) | 0.0261 c | 1.4 (1.5) |
| Median (Q1, Q3) | 1 (0, 2) | 1 (0, 2) | 0.0395 d | 1 (0, 2) |
| 0 | 186 (51.1) | 178 (48.9) | 0.0336 b | 364 (37.1) |
| 1 | 135 (53.2) | 119 (46.9) | 254 (25.9) | |
| 2–4 | 137 (43.8) | 176 (56.2) | 313 (31.9) | |
| 5–8 | 18 (36.7) | 31 (63.3) | 49 (5.0) | |
| Religion (3) | <0.0001 b | |||
| Muslim | 220 (40.2) | 327 (59.8) | 547 (54.4) | |
| Orthodox | 246 (59.6) | 167 (40.4) | 413 (41.1) | |
| Other e | 28 (60.9) | 18 (39.1) | 46 (4.6) | |
| Livelihood/Occupation (0) | <0.0001 b | |||
| Pastoral | 30 (15.2) | 167 (84.8) | 197 (19.5) | |
| Agro-pastoral | 155 (53.1) | 137 (46.9) | 292 (28.9) | |
| Agricultural/Farmer | 272 (63.9) | 154 (36.2) | 426 (42.2) | |
| Housewife | 16 (45.7) | 19 (54.3) | 35 (3.5) | |
| Other f | 22 (37.3) | 37 (62.7) | 59 (5.8) | |
| Livestock ownership: number of animals owned (23) | ||||
| Mean (SD) | 6.2 (22.4) | 16.2 (27.5) | <0.0001 c | 11.3 (25.7) |
| Median (Q1, Q3) | 1 (1, 6) | 7 (1, 18) | <0.0001 d | 3 (1, 12) |
| 0 | 47 (59.5) | 32 (40.5) | <0.0001 b | 79 (8.0) |
| 1–4 | 279 (60.8) | 180 (39.2) | 459 (46.6) | |
| 5–10 | 70 (48.0) | 76 (52.1) | 146 (14.8) | |
| 10 or more | 83 (27.5) | 219 (72.5) | 302 (30.6) | |
| Food Insecurity and Aid | ||||
| Severe food insecurity score (12) | ||||
| Mean (SD) | 0.6 (1.5) | 0.8 (1.6) | 0.0357 c | 0.7 (1.6) |
| Median (Q1, Q3) | 0 (0, 0) | 0 (0, 1) | 0.0055 d | 0 (0, 1) |
| 0 | 385 (51.5) | 362 (48.5) | 0.0008 b | 747 (74.9) |
| 1–3 | 83 (43.7) | 107 (56.3) | 190 (19.1) | |
| 4–6 | 10 (24.4) | 31 (75.6) | 41 (4.1) | |
| 7–9 | 13 (68.4) | 6 (31.6) | 19 (1.9) | |
| No food insecurity | 385 (51.4) | 362 (48.5) | 0.0124 b | |
| Any food insecurity | 106 (42.4) | 144 (57.6) | ||
| Food aid or PSNP participation (0) | <0.0001 b | |||
| No food aid or PSNP participation | 372 (59.4) | 254 (40.6) | 626 (62.0) | |
| Food aid (no PSNP) | 42 (39.3) | 65 (60.8) | 107 (10.6) | |
| PSNP (not direct support) | 68 (34.0) | 132 (66.0) | 200 (19.8) | |
| PSNP direct support | 13 (17.1) | 63 (82.9) | 76 (7.5) | |
| Dietary Diversity | ||||
| Minimum dietary diversity (28) | <0.0001 b | |||
| No (<= 3 food groups) | 464 (47.3) | 343 (35.0) | 807 (82.3) | |
| Yes (4–7 food groups) | 19 (1.9) | 155 (15.8) | 174 (17.7) | |
| Total | 495 (49.1) | 514 (50.9) | 1009 | |
| Age-Adjusted OR (95% CI) | Fully Adjusted a OR (95% CI) | |
|---|---|---|
| Age of child—per 3-month increase | 1.09 (1.04, 1.14) | 1.08 (1.03, 1.13) |
| Religion | ||
| Muslim | Referent group | Referent group |
| Orthodox | 0.45 (0.35, 0.59) | 0.70 (0.53, 0.94) |
| Other | 0.44 (0.24, 0.82) | 0.61 (0.31, 1.18) |
| Livelihood/Occupation | ||
| Pastoral | Referent group | Referent group |
| Agro-pastoral | 0.16 (0.10, 0.25) | 0.21 (0.13, 0.35) |
| Agricultural/Farmer | 0.10 (0.07, 0.16) | 0.15 (0.09, 0.23) |
| Housewife and other | 0.26 (0.15, 0.46) | 0.32 (0.18, 0.58) |
| Food aid or PSNP participation | ||
| No food aid or PSNP | Referent group | Referent group |
| Food aid (no PSNP) | 2.26 (1.482, 3.45) | 1.10 (0.68, 1.77) |
| PSNP (not direct support) | 2.82 (2.017, 3.94) | 1.74 (1.21, 2.52) |
| PSNP direct support | 6.89 (3.71, 12.82) | 4.47 (2.33, 8.56) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potts, K.S.; Mulugeta, A.; Bazzano, A.N. Animal Source Food Consumption in Young Children from Four Regions of Ethiopia: Association with Religion, Livelihood, and Participation in the Productive Safety Net Program. Nutrients 2019, 11, 354. https://doi.org/10.3390/nu11020354
Potts KS, Mulugeta A, Bazzano AN. Animal Source Food Consumption in Young Children from Four Regions of Ethiopia: Association with Religion, Livelihood, and Participation in the Productive Safety Net Program. Nutrients. 2019; 11(2):354. https://doi.org/10.3390/nu11020354
Chicago/Turabian StylePotts, Kaitlin S., Afework Mulugeta, and Alessandra N. Bazzano. 2019. "Animal Source Food Consumption in Young Children from Four Regions of Ethiopia: Association with Religion, Livelihood, and Participation in the Productive Safety Net Program" Nutrients 11, no. 2: 354. https://doi.org/10.3390/nu11020354
APA StylePotts, K. S., Mulugeta, A., & Bazzano, A. N. (2019). Animal Source Food Consumption in Young Children from Four Regions of Ethiopia: Association with Religion, Livelihood, and Participation in the Productive Safety Net Program. Nutrients, 11(2), 354. https://doi.org/10.3390/nu11020354