Current Recommendations for Nutritional Management of Overweight and Obesity in Children and Adolescents: A Structured Framework

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Evidence Selection, Extraction and Analysis
2.2. Development of the Structured Framework
2.3. Usability Evaluation
3. Results
3.1. Evidence Selection
3.2. Guidelines Extraction and Analysis
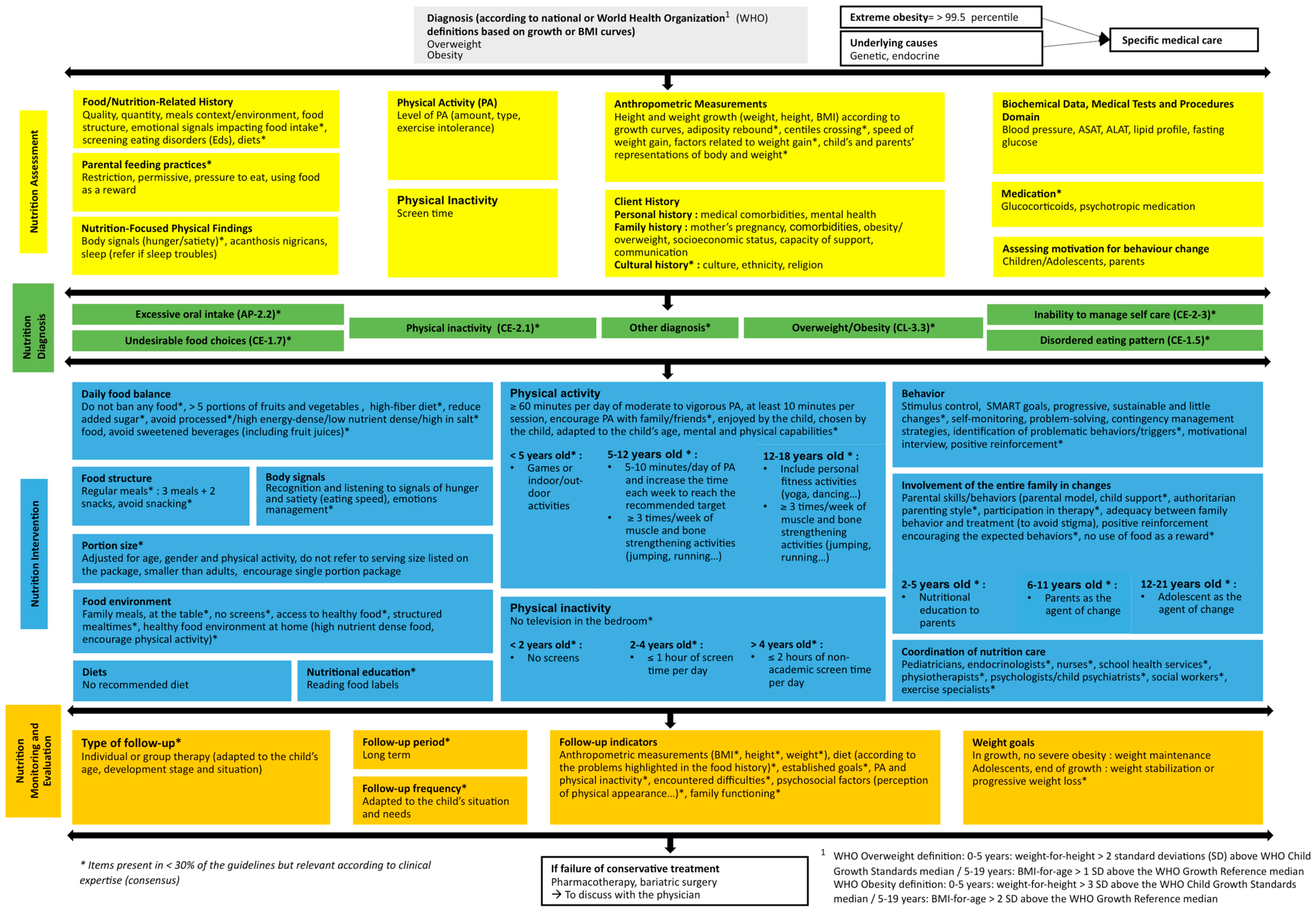
3.3. Development of the Structured Framework
3.4. Usability Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Taking Action on Childhool Obesity; World Health Organization. Available online: https://www.who.int/end-childhood-obesity/publications/taking-action-childhood-obesity-report/en/ (accessed on 8 February 2019).
- Altman, M.; Wilfley, D.E. Evidence Update on the Treatment of Overweight and Obesity in Children and Adolescents. J. Clin. Child Adolesc. Psychol. 2014, 44, 521–537. [Google Scholar] [CrossRef] [PubMed]
- Colquitt, J.L.; Loveman, E.; O’Malley, C.; Azevedo, L.B.; Mead, E.; Al-Khudairy, L.; Ells, L.J.; Metzendorf, M.-I.; Rees, K. Diet, physical activity, and behavioural interventions for the treatment of overweight or obesity in preschool children up to the age of 6 years. Cochrane Database Syst. Rev. 2016, 3. [Google Scholar] [CrossRef]
- Mead, E.; Brown, T.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; Beardsmore, E.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Al-Khudairy, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Coppock, J.H.; Ridolfi, D.R.; Hayes, J.F.; Paul, M.S.; Wilfley, D.E. Current Approaches to the Management of Pediatric Overweight and Obesity. Curr. Treat. Options Cardio. Med. 2014, 16, 343. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Garnett, S.P.; Baur, L.; Burrows, T.; Stewart, L.; Neve, M.; Collins, C. Effectiveness of Lifestyle Interventions in Child Obesity: Systematic Review With Meta-analysis. Pediatrics 2012, 130, e1647–e1671. [Google Scholar] [CrossRef]
- Barlow, S.E.; Ervin, C.; Ludwig, D.S.; Saelens, B.E.; Schetzina, K.E.; Taveras, E.M.; Spear, B.A. Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Pediatrics 2007, 120, 254. [Google Scholar] [CrossRef]
- Sun, Y.; You, W.; Almeida, F.; Estabrooks, P.; Davy, B. The Effectiveness and Cost of Lifestyle Interventions Including Nutrition Education for Diabetes Prevention: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2017, 117, 404–421. [Google Scholar] [CrossRef]
- Final Report of the International Confederation of Dietetic Associations (ICDA) Evidence-based Practice Working Group. Available online: https://www.internationaldietetics.org/Downloads/ICDA-Report-Evidence-based-Dietetics-Practice-2010.aspx (accessed on 8 February 2019).
- Timmermans, S.; Mauck, A. The Promises And Pitfalls Of Evidence-Based Medicine. Health Affairs 2005, 24, 18–28. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. Clinical Practice Guidelines We Can Trust; National Academies Press (US): Washington, DC, USA, 2011.
- Blumberg, J.; Heaney, R.P.; Huncharek, M.; Scholl, T.; Stampfer, M.; Vieth, R.; Weaver, C.M.; Zeisel, S.H. Evidence-based criteria in the nutritional context. Nutr. Rev. 2010, 68, 478–484. [Google Scholar] [CrossRef]
- Byham-Gray, L.D.; Gilbride, J.A.; Dixon, L.B.; Stage, F.K. Evidence-Based Practice: What Are Dietitians’ Perceptions, Attitudes, and Knowledge? J. Am. Diet. Assoc. 2005, 105, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.E.; Kukuruzovic, R.; Martino, B.; Chauhan, S.S.; Elliott, E.J. Knowledge and use of evidence-based nutrition: a survey of paediatric dietitians. J. Hum. Nutr. Diet. 2003, 16, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Toman, C.; Harrison, M.B.; Logan, J. Clinical practice guidelines: necessary but not sufficient for evidence-based patient education and counseling. Patient Educ. Couns. 2001, 42, 279–287. [Google Scholar] [CrossRef]
- Légaré, F.; Fervers, B.; Harrison, M.B.; Graham, I.D. Adapting clinical practice guidelines to local context and assessing barriers to their use. CMAJ 2009, 182, E78–E84. [Google Scholar]
- Harrison, M.B.; Graham, I.D.; Fervers, B.; Hoek, J.V.D. Adapting knowledge to local context. In Knowledge Translation in Health Care; Wiley: Hoboken, NJ, USA, 2013; pp. 110–120. [Google Scholar]
- Writing Group of the Nutrition Care Process/Standardized Language Committee. Nutrition care process and model part I: the 2008 update. J. Am. Diet. Assoc. 2008, 108, 1113–1117. [Google Scholar] [CrossRef] [PubMed]
- Writing Group of the Nutrition Care Process/Standardized Language Committee. Nutrition care process part II: using the International Dietetics and Nutrition Terminology to document the nutrition care process. J. Am. Diet. Assoc. 2008, 108, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, M.; Kho, M.; Browman, G.; Burgers, J.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in healthcare. CMAJ 2010, 182, E839–E842. [Google Scholar] [CrossRef] [PubMed]
- Academy of Nutrition and Dietetics. Pediatric Weight Management. Major recommendations (2007). Available online: https://www.andeal.org/vault/pq57.pdf (accessed on 10 December 2018).
- Academy of Nutrition and Dietetics. Pediatric Weight Management. Major recommendations (2015). Available online: https://www.andeal.org/vault/pq140.pdf (accessed on 10 December 2018).
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L.; Academy Positions Committee. Position of the Academy of Nutrition and Dietetics: Interventions for the Prevention and Treatment of Pediatric Overweight and Obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef]
- Lau, D.C.; Douketis, J.D.; Morrison, K.M.; Hramiak, I.M.; Sharma, A.M.; Ur, E.; Obesity Canada Clinical Practice Guidelines Expert Panel. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. CMAJ 2007, 176, S1–S13. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity—Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef]
- Baker, J.L.; Farpour-Lambert, N.J.; Nowicka, P.; Pietrobelli, A.; Weiss, R. Evaluation of the Overweight/Obese Child—Practical Tips for the Primary Health Care Provider: Recommendations from the Childhood Obesity Task Force of the European Association for the Study of Obesity. Obes. Facts 2010, 3, 5. [Google Scholar] [CrossRef]
- Haute Autorité de Santé. Surpoids et obésité de l’enfant et de l’adolescent. Available online: https://www.has-sante.fr/portail/jcms/c_964941/fr/surpoids-et-obesite-de-l-enfant-et-de-l-adolescent-actualisation-des-recommandations-2003 (accessed on 22 December 2018).
- Institute for Clinical Systems Improvement. Prevention and Management of Obesity for Children and Adolescents. 2013. Available online: https://www.ohcoop.org/wp-content/uploads/Clinical-Guidelines-Prevention-and-Management-Obesity-in-Children-and-Adolscent.pdf (accessed on 8 February 2019).
- Institut national d’excellence en santé et en services sociaux. Traitement de l’obésité des enfants et des adolescents en 1re et 2e ligne: guide de pratique clinique. Volet I; INESSS: Montreal, QC, Canada, 2012. [Google Scholar]
- Turner, L.R.; Harris, M.F.; Mazza, D. Obesity management in general practice: does current practice match guideline recommendations? Med. J. Aust. 2015, 202, 370–372. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health Care Excellence. Obesity: Identification, assessment and management. Available online: https://www.nice.org.uk/guidance/cg189/resources/obesity-identification-assessment-and-management-pdf-35109821097925 (accessed on 22 December 2018).
- Ministry of Health; Clinical Trials Research Unit. Clinical Guidelines for Weight Management in New Zealand Children and Young People; Ministry of Health: Wellington, New Zealand, 2009.
- Ministry of Health. Clinical Guidelines for Weight Mangagement in New Zealand Children and Young People; Ministry of Health: Wellington, New Zealand, 2016.
- Scottish Intercollegiate Guidelines Network. Handbook of Disease Burdens and Quality of Life Measures; Springer-Verlag: New York, NY, USA, 2010; p. 4315. [Google Scholar]
- Società Italiana di Pediatria; Società Italiana di Endocrinologia e Diabetologia Pediatrica. Consensus su diagnosi, trattamento e prevenzione dell’obesita del’bambino e dell’adolescente. Available online: https://docs.sip.it/Consensus_Obesita_2017.pdf (accessed on 22 December 2018).
- Academy of Nutrition and Dietetics. Manuel de référence de la terminologie internationale de diététique et de nutrition (TIDN); Presses de l’Université de Laval: Québec, QC, Canada, 2013. [Google Scholar]
- Epstein, L.H.; Valoski, A.; Wing, R.R.; McCurley, J. Ten-Year Follow-up of Behavioral, Family-Based Treatment for Obese Children. JAMA 1990, 264, 2519. [Google Scholar] [CrossRef] [PubMed]
- Vanherle, K.; Werkman, A.; Baete, E.; Barkmeijer, A.; Kolm, A.; Gast, C.; Ramminger, S.; Höld, E.; Kohlenberg-Müller, K.; Ohlrich-Hahn, S.; et al. Proposed standard model and consistent terminology for monitoring and outcome evaluation in different dietetic care settings: Results from the EU-sponsored IMPECD project. Clin. Nutr. 2018, 37, 2206–2216. [Google Scholar] [CrossRef] [PubMed]
- Ford, I.; Norrie, J. Pragmatic Trials. N. Engl. J. Med. 2016, 375, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Database | Search Terms or Search Equation |
|---|---|
| Medline via PubMed | (terms in all fields): ((pediatric AND obesity) OR (pediatric obesity) OR (obesity AND child)) AND (guideline OR algorithms OR evidence-based medicine) AND (diet therapy OR nutrition therapy OR case management OR patient care management OR dietetics/education); filters: 10 years, Humans, Child: birth-18 years. |
| The Cochrane Library | pediatric obesity, pediatric obesity guidelines and treatment, obesity. |
| Grey literature research (Google, Bing) | guidelines, pediatric/childhood obesity, nutritional management, algorithm, the name of the country (Australia, Canada, Scotland, United States, France, Italy, New-Zealand, United Kingdom), the name of the scientific society (Academy of Nutrition and Dietetics, American Academy of Pediatrics, Canadian Medical Association, European Association for the Study of Obesity, Haute Autorité de Santé, Institute for Clinical Systems Improvement, Institute for Healthy Childhood Weight, Institut National d’Excellence en Santé et Services sociaux, National Health and Medical Research Council, National Institute for Health and Care Excellence, New Zealand Ministry of Health, Scottish Intercollegiate Guidelines Network, Società Italiana di Pediatrica, The Endocrine Society). |
| Theme | Recommendation | N of Citation | Reference |
|---|---|---|---|
| Nutritional Assessment | |||
| Food/Nutrition-related history | Assess eating patterns | 13 | [8,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] |
| Assess food quality and quantity (including portion sizes and overeating) | 7 | [8,22,23,24,27,28,31,33,34,36] | |
| Assess the presence of sugar-sweetened beverages and juices | 7 | [8,22,23,24,25,26,27,31,33,34] | |
| Assess meals structure and distribution | 7 | [8,22,23,24,25,27,28,31,33,34] | |
| Assess meals context and environment | 6 | [26,27,28,29,33,34,36] | |
| Assess the presence of snacking | 3 | [27,28,31] | |
| Anthropometric measurements | Calculate BMI | 13 | [8,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] |
| Analyze growth curves | 11 | [8,25,26,27,28,29,30,31,32,33,34,36] | |
| Assess the factors conducting to a weight gain | 2 | [30,31] | |
| Assess the precocity of the adiposity rebound | 1 | [28] | |
| Biochemical data, medical tests and procedures | Interpret of blood pressure | 10 | [8,25,26,27,28,29,31,32,33,34,36] |
| Interpret of blood lipids | 10 | [8,25,26,27,28,29,30,32,33,34,36] | |
| Analyze blood glucose | 9 | [8,25,26,27,28,29,30,32,36] | |
| Assess hepatic tests | 7 | [25,26,27,28,29,32,36] | |
| Nutrition-focused physical findings | Assess the presence of acanthosis nigricans | 7 | [8,26,27,29,31,33,34,35] |
| Assess sleep | 6 | [8,27,28,30,31,33,34] | |
| Assess food sensations | 1 | [28] | |
| Physical activity | Assess physical activity level | 12 | [8,22,23,24,25,26,28,29,30,31,32,33,34,35,36] |
| Assess sedentary behaviors (especially the screen time) | 11 | [8,22,23,24,25,26,27,28,29,30,31,33,34,35] | |
| Client history | Assess comorbidities | 11 | [8,25,26,27,29,30,31,32,33,34,35,36] |
| Assess family history | 12 | [8,25,26,27,28,29,30,31,32,33,34,35] | |
| Assess mental health | 8 | [8,22,23,24,26,30,31,32,33,34,35] | |
| Assess social/family environment | 8 | [22,23,24,25,26,28,30,31,32,35] | |
| Assess parental feeding practices (restrictive, permissive, pressure to eat, food as reward) | 3 | [22,23,24,26,28] | |
| Eating Disorders screening | Screen for eating disorders | 9 | [8,22,23,24,26,28,29,30,31,35,36] |
| Assess the presence of Binge Eating Disorders | 5 | [8,26,28,31,36] | |
| Change motivation | Assess motivation and readiness to change | 9 | [8,25,27,28,29,30,31,32,33,34,35] |
| Nutritional Diagnosis | |||
| No guideline referred to nutritional diagnosis. | 0 | ||
| Nutritional Intervention | |||
| Meal structure | Structure eating with 3 meals and 2 snacks per day | 5 | [2,8,31,35,36] |
| Avoid snacking | 3 | [8,26,36] | |
| Food balance | Promote fruit and vegetable consumption | 7 | [8,26,27,29,33,34,35,36] |
| Balance diet and eating habits | 6 | [25,28,30,32,33,34,36] | |
| Avoid high energy density and low nutritional density foods (fast-foods, take-out, sugar sweetened beverages and juices) | 5 | [2,26,29,33,34,36] | |
| Do not forbid any food | 3 | [28,31,35] | |
| Avoid sugar sweetened beverages and juices | 4 | [8,26,29,33,34] | |
| Limit sugar sweetened beverages and juices consumption | 3 | [27,35,36] | |
| Portion sizes | Follow national recommendations | 4 | [29,33,34,35,36] |
| Diets | Avoid any type of restrictive diet | 8 | [8,22,23,24,25,28,32,33,34,35,36] |
| Follow the “stop/traffic light diet” (The traffic light diet divides food groups into 3 categories: green (low-energy, high-nutrient foods, may be eaten often), yellow (moderate-energy foods, may be eaten in moderation), and red (high-energy, low-nutrient foods, should be eaten sparingly). [38] | 4 | [22,23,24,25,30,36] | |
| Meal environment | Eat as a family | 6 | [8,27,29,30,31,35] |
| Avoid screen during meals | 3 | [27,31,35] | |
| Offer healthy foods at home | 1 | [31] | |
| Food sensations | Work on the recognition and respect of the food sensations | 6 | [2,28,30,31,35,36] |
| Family implication | Families should be included in the treatment | 14 | [2,8,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] |
| Family behavior should not be different than the child with excess weight to avoid stigmatization | 8 | [2,8,27,28,30,32,33,34,35] | |
| Lifestyle intervention | Multifactorial treatment including the food balance, the physical activity and the behavior management | 10 | [2,22,23,24,26,28,29,30,31,32,33,34,35] |
| Physical activity | At least 60 min of moderate to vigorous activity per day (at least 10 min per session) | 10 | [2,8,27,28,29,30,31,32,35,36] |
| Importance of the child’s choice and pleasure in the activity | 8 | [8,25,27,29,30,32,33,34,35] | |
| Sedentarity | Reduce non-academic screen time to max. 2 h both in week days and weekend days | 8 | [2,8,26,27,29,30,33,34,35] |
| Behavior management | Practice stimulus control | 8 | [2,22,23,24,25,29,30,32,33,34,35] |
| Use motivational counseling | 8 | [2,8,25,26,27,28,29,30] | |
| Set SMART objectives with the child and/or the parents | 8 | [2,8,25,29,30,31,33,34,35] | |
| Introduce behavior and objectives self-monitoring | 7 | [2,8,25,29,30,33,34,35] | |
| Care coordination and implication | Dietitian | 7 | [8,22,23,24,25,26,27,28,30] |
| Pediatrician | 6 | [8,25,27,28,29,30] | |
| Other professionals | Details in Table S1 | ||
| Interdisciplinary teams | 3 | [24,25,30] | |
| Pharmacotherapy | Recommend to use Orlistat in specific conditions but warn about its low efficacy | 11 | [8,22,23,24,25,26,29,30,31,32,33,34,35,36] |
| Bariatric surgery | In general, not recommended. Indications and contraindications were different between guidelines. | Details in Table S1 | |
| Comorbidities | Consider comorbidities during the intervention | 9 | [8,26,27,28,29,30,32,35,36] |
| Nutritional Monitoring and evaluation | |||
| Follow-up | Individual or group follow-up depending on the child’s situation | 2 | [22,23,24,36] |
| Long-term follow-up | 4 | [2,25,31,32] | |
| Monitoring indicators | Monitor anthropometric measurements | 10 | [2,8,22,23,24,26,28,29,31,33,34,35,36] |
| Monitor food balance and physical activity | 4 | [8,29,31,36] | |
| Monitor changes according to the objectives | 1 | [28] | |
| Weight management | Weight stabilization for growing children | 7 | [22,23,24,26,27,28,29,31,32] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfeifflé, S.; Pellegrino, F.; Kruseman, M.; Pijollet, C.; Volery, M.; Soguel, L.; Bucher Della Torre, S. Current Recommendations for Nutritional Management of Overweight and Obesity in Children and Adolescents: A Structured Framework. Nutrients 2019, 11, 362. https://doi.org/10.3390/nu11020362
Pfeifflé S, Pellegrino F, Kruseman M, Pijollet C, Volery M, Soguel L, Bucher Della Torre S. Current Recommendations for Nutritional Management of Overweight and Obesity in Children and Adolescents: A Structured Framework. Nutrients. 2019; 11(2):362. https://doi.org/10.3390/nu11020362
Chicago/Turabian StylePfeifflé, Shawna, Fabien Pellegrino, Maaike Kruseman, Claire Pijollet, Magali Volery, Ludivine Soguel, and Sophie Bucher Della Torre. 2019. "Current Recommendations for Nutritional Management of Overweight and Obesity in Children and Adolescents: A Structured Framework" Nutrients 11, no. 2: 362. https://doi.org/10.3390/nu11020362