Insufficient Nutrition and Mortality Risk in Septic Patients Admitted to ICU with a Focus on Immune Dysfunction



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Definitions
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics between 28-Day Survivors and Non-Survivors.
3.2. Risk Factors of Lower Day 7 Caloric Meet
3.3. Impact of Immune Dysfunction and Day 7 Caloric Meet on Survival Outcome
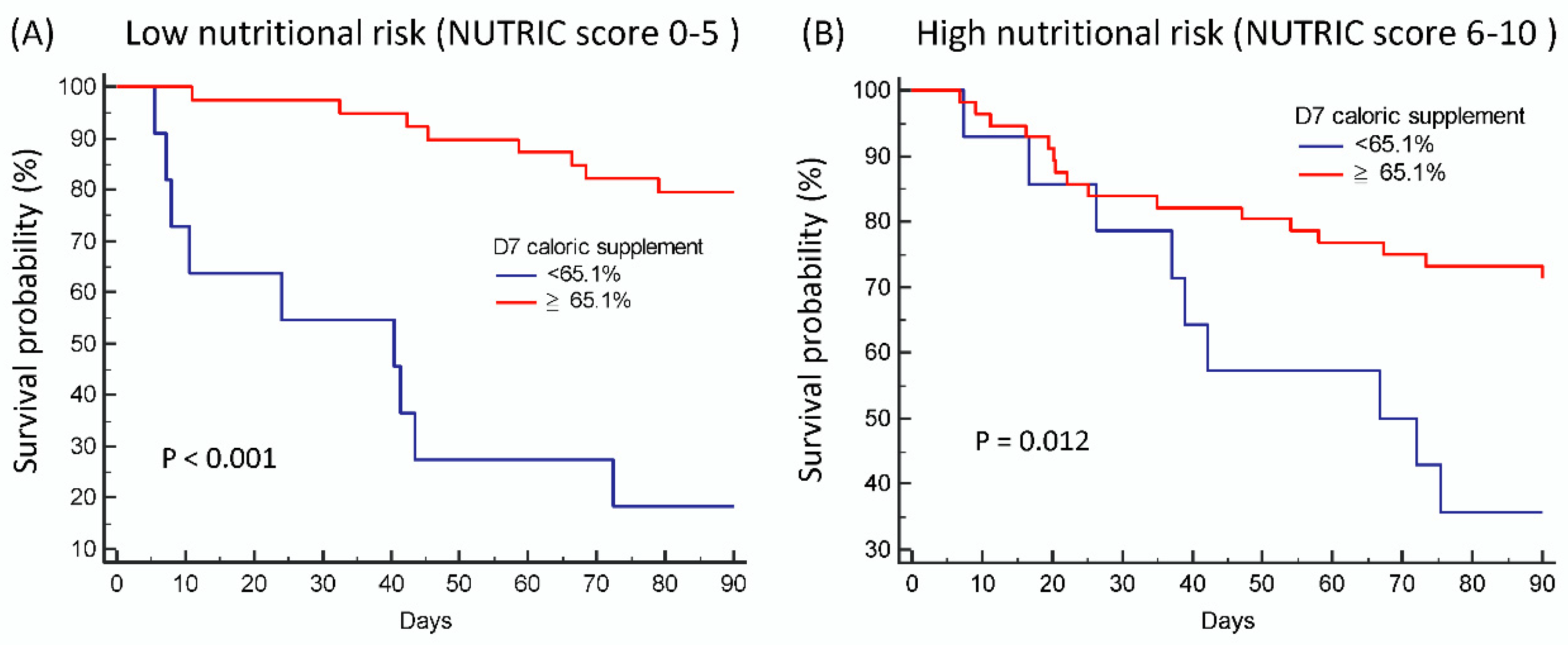
3.4. Impact of NUTRIC Score and Day 7 Caloric Meet on Survival Outcome
3.5. Multivariate Analysis of Clinical Characteristics and Immune Status and Their Impact on Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reintam Blaser, A.; Berger, M.M. Early or Late Feeding after ICU Admission? Nutrients 2017, 9, 1278. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.M.; Doig, G.S.; Heyland, D.K.; Morrison, T.; Sibbald, W.J.; Southwestern Ontario Critical Care Research Network. Multicentre, cluster-randomized clinical trial of algorithms for critical-care enteral and parenteral therapy (ACCEPT). CMAJ 2004, 170, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Finfer, S.; Delaney, A.; Davies, A.R.; Mitchell, I.; Dobb, G.; Nutrition Guidelines Investigators of the ANZICS Clinical Trials Group. Effect of evidence-based feeding guidelines on mortality of critically ill adults: A cluster randomized controlled trial. JAMA 2008, 300, 2731–2741. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Sweetman, E.A.; Finfer, S.R.; Cooper, D.J.; Heighes, P.T.; Davies, A.R.; O’Leary, M.; Solano, T.; Peake, S.; et al. Early parenteral nutrition in critically ill patients with short-term relative contraindications to early enteral nutrition: A randomized controlled trial. JAMA 2013, 309, 2130–2138. [Google Scholar] [CrossRef] [PubMed]
- Casaer, M.P.; Mesotten, D.; Hermans, G.; Wouters, P.J.; Schetz, M.; Meyfroidt, G.; Van Cromphaut, S.; Ingels, C.; Meersseman, P.; Muller, J.; et al. Early versus late parenteral nutrition in critically ill adults. N. Engl. J. Med. 2011, 365, 506–517. [Google Scholar] [CrossRef] [PubMed]
- Rubinson, L.; Diette, G.B.; Song, X.; Brower, R.G.; Krishnan, J.A. Low caloric intake is associated with nosocomial bloodstream infections in patients in the medical intensive care unit. Crit. Care Med. 2004, 32, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, J.A.; Parce, P.B.; Martinez, A.; Diette, G.B.; Brower, R.G. Caloric intake in medical ICU patients: Consistency of care with guidelines and relationship to clinical outcomes. Chest 2003, 124, 297–305. [Google Scholar] [CrossRef]
- Marik, P.E.; Hooper, M.H. Normocaloric versus hypocaloric feeding on the outcomes of ICU patients: A systematic review and meta-analysis. Intensive Care Med. 2016, 42, 316–323. [Google Scholar] [CrossRef]
- Petros, S.; Horbach, M.; Seidel, F.; Weidhase, L. Hypocaloric vs Normocaloric Nutrition in Critically Ill Patients: A Prospective Randomized Pilot Trial. JPEN J. Parenter Enteral Nutr. 2016, 40, 242–249. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Aldawood, A.S.; Haddad, S.H.; Al-Dorzi, H.M.; Tamim, H.M.; Jones, G.; Mehta, S.; McIntyre, L.; Solaiman, O.; Sakkijha, M.H.; et al. Permissive Underfeeding or Standard Enteral Feeding in Critically Ill Adults. N. Engl. J. Med. 2015, 372, 2398–2408. [Google Scholar] [CrossRef]
- Target Investigators for the ANZICS Clinical Trials Group; Chapman, M.; Peake, S.L.; Bellomo, R.; Davies, A.; Deane, A.; Horowitz, M.; Hurford, S.; Lange, K.; Little, L.; et al. Energy-Dense versus Routine Enteral Nutrition in the Critically III. N. Engl. J. Med. 2018, 379, 1823–1834. [Google Scholar] [CrossRef]
- Hernandez-Socorro, C.R.; Saavedra, P.; Lopez-Fernandez, J.C.; Ruiz-Santana, S. Assessment of Muscle Wasting in Long-Stay ICU Patients Using a New Ultrasound Protocol. Nutrients 2018, 10, 1849. [Google Scholar] [CrossRef] [PubMed]
- Thiessen, S.E.; Derde, S.; Derese, I.; Dufour, T.; Vega, C.A.; Langouche, L.; Goossens, C.; Peersman, N.; Vermeersch, P.; Vander Perre, S.; et al. Role of Glucagon in Catabolism and Muscle Wasting of Critical Illness and Modulation by Nutrition. Am. J. Respir. Crit. Care Med. 2017, 196, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Boomer, J.S.; To, K.; Chang, K.C.; Takasu, O.; Osborne, D.F.; Walton, A.H.; Bricker, T.L.; Jarman, S.D., 2nd; Kreisel, D.; Krupnick, A.S.; et al. Immunosuppression in patients who die of sepsis and multiple organ failure. JAMA 2011, 306, 2594–2605. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Immunosuppression in sepsis: A novel understanding of the disorder and a new therapeutic approach. Lancet Infect. Dis. 2013, 13, 260–268. [Google Scholar] [CrossRef]
- Alcock, J. The Emperor Has No Clothes? Searching for Dysregulation in Sepsis. J. Clin. Med. 2018, 7, 247. [Google Scholar] [CrossRef]
- Martin, L.; Koczera, P.; Simons, N.; Zechendorf, E.; Hoeger, J.; Marx, G.; Schuerholz, T. The Human Host Defense Ribonucleases 1, 3 and 7 Are Elevated in Patients with Sepsis after Major Surgery–A Pilot Study. Int. J. Mol. Sci. 2016, 17, 294. [Google Scholar] [CrossRef]
- Decker, S.O.; Sigl, A.; Grumaz, C.; Stevens, P.; Vainshtein, Y.; Zimmermann, S.; Weigand, M.A.; Hofer, S.; Sohn, K.; Brenner, T. Immune-Response Patterns and Next Generation Sequencing Diagnostics for the Detection of Mycoses in Patients with Septic Shock-Results of a Combined Clinical and Experimental Investigation. Int. J. Mol. Sci. 2017, 18, 1796. [Google Scholar] [CrossRef]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; Martin-Fernandez, M.; Lopez-Mestanza, C.; Duque, P.; Almansa, R. Shared Features of Endothelial Dysfunction between Sepsis and Its Preceding Risk Factors (Aging and Chronic Disease). J. Clin. Med. 2018, 7, 400. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; Tamayo, E.; Andaluz-Ojeda, D.; Martin-Fernandez, M.; Almansa, R. Characterizing Systemic Immune Dysfunction Syndrome to Fill in the Gaps of SEPSIS-2 and SEPSIS-3 Definitions. Chest 2017, 151, 518–519. [Google Scholar] [CrossRef] [PubMed]
- Hamers, L.; Kox, M.; Pickkers, P. Sepsis-induced immunoparalysis: Mechanisms, markers, and treatment options. Minerva Anestesiol. 2015, 81, 426–439. [Google Scholar] [PubMed]
- Bourke, C.D.; Berkley, J.A.; Prendergast, A.J. Immune Dysfunction as a Cause and Consequence of Malnutrition. Trends Immunol. 2016, 37, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]
- Monneret, G.; Venet, F. Monocyte HLA-DR in sepsis: Shall we stop following the flow? Crit. Care 2014, 18, 102. [Google Scholar] [CrossRef]
- Fang, W.F.; Douglas, I.S.; Chen, Y.M.; Lin, C.Y.; Kao, H.C.; Fang, Y.T.; Huang, C.H.; Chang, Y.T.; Huang, K.T.; Wang, Y.H.; et al. Development and validation of immune dysfunction score to predict 28-day mortality of sepsis patients. PLoS ONE 2017, 12, e0187088. [Google Scholar] [CrossRef]
- Fang, W.F.; Chen, Y.M.; Lin, C.Y.; Huang, K.T.; Kao, H.C.; Fang, Y.T.; Huang, C.H.; Chang, Y.T.; Wang, Y.H.; Wang, C.C.; et al. Immune profiles and clinical outcomes between sepsis patients with or without active cancer requiring admission to intensive care units. PLoS ONE 2017, 12, e0179749. [Google Scholar] [CrossRef]
- National Heart, L. Blood Institute Acute Respiratory Distress Syndrome Clinical Trials, N.; Rice, T.W.; Wheeler, A.P.; Thompson, B.T.; Steingrub, J.; Hite, R.D.; Moss, M.; Morris, A.; Dong, N.; et al. Initial trophic vs full enteral feeding in patients with acute lung injury: The EDEN randomized trial. JAMA 2012, 307, 795–803. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Tamim, H.M.; Dhar, G.S.; Al-Dawood, A.; Al-Sultan, M.; Sakkijha, M.H.; Kahoul, S.H.; Brits, R. Permissive underfeeding and intensive insulin therapy in critically ill patients: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 93, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Jafar, N.; Edriss, H.; Nugent, K. The Effect of Short-Term Hyperglycemia on the Innate Immune System. Am. J. Med. Sci. 2016, 351, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Waitzberg, D.L.; Caiaffa, W.T.; Correia, M.I. Hospital malnutrition: The Brazilian national survey (IBRANUTRI): A study of 4000 patients. Nutrition 2001, 17, 573–580. [Google Scholar] [CrossRef]
- Correia, M.I.; Campos, A.C.; Study, E.C. Prevalence of hospital malnutrition in Latin America: The multicenter ELAN study. Nutrition 2003, 19, 823–825. [Google Scholar] [CrossRef]
- Kamath, S.K.; Lawler, M.; Smith, A.E.; Kalat, T.; Olson, R. Hospital malnutrition: A 33-hospital screening study. J. Am. Diet. Assoc. 1986, 86, 203–206. [Google Scholar]
- O’Flynn, J.; Peake, H.; Hickson, M.; Foster, D.; Frost, G. The prevalence of malnutrition in hospitals can be reduced: Results from three consecutive cross-sectional studies. Clin. Nutr. 2005, 24, 1078–1088. [Google Scholar] [CrossRef]
- Fowler, R.A.; Adhikari, N.K.; Bhagwanjee, S. Clinical review: Critical care in the global context--disparities in burden of illness, access, and economics. Crit. Care 2008, 12, 225. [Google Scholar] [CrossRef]
- Nguyen, Y.L.; Angus, D.C.; Boumendil, A.; Guidet, B. The challenge of admitting the very elderly to intensive care. Ann. Intensive Care 2011, 1, 29. [Google Scholar] [CrossRef]
- Pirlich, M.; Schutz, T.; Kemps, M.; Luhman, N.; Burmester, G.R.; Baumann, G.; Plauth, M.; Lubke, H.J.; Lochs, H. Prevalence of malnutrition in hospitalized medical patients: Impact of underlying disease. Dig. Dis. 2003, 21, 245–251. [Google Scholar] [CrossRef]
- Gellrich, N.C.; Handschel, J.; Holtmann, H.; Kruskemper, G. Oral cancer malnutrition impacts weight and quality of life. Nutrients 2015, 7, 2145–2160. [Google Scholar] [CrossRef] [PubMed]
- Barr, J.; Hecht, M.; Flavin, K.E.; Khorana, A.; Gould, M.K. Outcomes in critically ill patients before and after the implementation of an evidence-based nutritional management protocol. Chest 2004, 125, 1446–1457. [Google Scholar] [CrossRef] [PubMed]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Artinian, V.; Krayem, H.; DiGiovine, B. Effects of early enteral feeding on the outcome of critically ill mechanically ventilated medical patients. Chest 2006, 129, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Pichard, C.; Lochs, H.; Pirlich, M. Prognostic impact of disease-related malnutrition. Clin. Nutr. 2008, 27, 5–15. [Google Scholar] [CrossRef] [PubMed]
- van den Berk, J.M.; Oldenburger, R.H.; van den Berg, A.P.; Klompmaker, I.J.; Mesander, G.; van Son, W.J.; van der Bij, W.; Sloof, M.J.; The, T.H. Low HLA-DR expression on monocytes as a prognostic marker for bacterial sepsis after liver transplantation. Transplantation 1997, 63, 1846–1848. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 151) | Non-Survivor (n = 30) | Survivor (n = 121) | p | |
|---|---|---|---|---|
| Age (years), mean (SD) | 67.3 (15.1) | 67.1 (13.5) | 67.4 (15.5) | 0.758 |
| Male, n (%) | 60 (39.7) | 13 (43.3) | 47 (38.8) | 0.653 |
| Body Mass Index, mean (SD) | 23.2 (5.0) | 24.6 (4.6) | 22.8 (5.0) | 0.056 |
| Coronary artery disease, n (%) | 45 (29.8) | 8 (26.7) | 37 (30.6) | 0.675 |
| Hypertension, n (%) | 87 (57.6) | 18 (60.0) | 69 (57.0) | 0.768 |
| Diabetes mellitus, n (%) | 75 (49.7) | 16 (53.3) | 59 (48.8) | 0.654 |
| Stroke, n (%) | 32 (21.2) | 6 (20.0) | 26 (21.5) | 0.858 |
| Chronic kidney disease, n (%) | 34 (22.5) | 9 (30.0) | 25 (20.7) | 0.273 |
| Infection focus | 0.068 | |||
| Lung | 95 (62.9) | 16 (16.8) | 79 (83.2) | |
| Urinary tract | 20 (13.2) | 2 (10.0) | 18 (90.0) | |
| Intra-abdomen | 6 (4.0) | 1 (16.7) | 5 (83.3) | |
| Others | 30 (19.9) | 11 (36.7) | 19 (63.3) | |
| Hemodialysis, n (%) | 30 (19.9) | 8 (26.7) | 22 (73.3) | 0.297 |
| Cancer, n (%) | 29 (19.2) | 7 (23.3) | 22 (18.2) | 0.209 |
| Cirrhosis, n (%) | 6 (4) | 3 (10) | 3 (2.5) | 0.059 |
| SOFA score, mean (SD) | 9.5 (3.6) | 11.9 (4.2) | 8.9 (3.2) | <0.001 |
| APAHCE-II, mean (SD) | 26.01 (8.77) | 27.57 (7.77) | 25.62 (8.99) | 0.240 |
| Interleukin-6, pg/mL, mean (SD) | 313.2 (1351.4) | 134.1 (293.7) | 1035.8 (2901.0) | 0.100 |
| NUTRIC score, mean (SD) | 5.7 (1.9) | 6.3 (2.0) | 5.5 (1.8) | 0.023 |
| Day 1 caloric intake, mean (SD) | 617.7 (439.8) | 490.2 (444.6) | 649.1 (434.8) | 0.081 |
| Day 1 caloric meet, mean (SD) | 0.43 (0.30) | 0.34 (0.31) | 0.45 (0.30) | 0.069 |
| Day 1 protein intake, g, mean (SD) | 18.6 (17.7) | 13.5 (15.8) | 19.8 (18.0) | 0.089 |
| Day 1 HLA-DR (%), mean (SD) | 86.5 (15.8) | 79.1 (21.5) | 88.4 (13.5) | 0.045 |
| Day 3 caloric intake, mean (SD) ** | 1053.4 (496.1) | 882.0 (573.0) | 1087.1 (475.0) | 0.070 |
| Day 3 caloric meet, mean (SD) | 0.74 (0.36) | 0.62 (0.42) | 0.76 (0.34) | 0.072 |
| Day 3 protein intake, g, mean (SD) | 36.9 (22.4) | 37.9 (21.9) | 36.5 (22.7) | 0.737 |
| Day 3 HLA-DR (%), mean (SD) | 89.8 (12.2) | 85.1 (15.4) | 90.6 (11.4) | 0.052 |
| Day 7 caloric intake, mean (SD) *** | 869.8 (304.7) | 730.4 (310.3) | 890.8 (299.7) | 0.049 |
| Day 7 caloric meet, mean (SD) | 0.87 (0.30) | 0.73 (0.31) | 0.89 (0.30) | 0.042 |
| Day 7 protein intake, g, mean (SD) | 48.3 (20.7) | 43.8 (21.3) | 50.3 (20.3) | 0.114 |
| Day 7 HLA-DR (%), mean (SD) | 93.6 (9.9) | 83.9 (21.1) | 94.7 (7.1) | 0.085 |
| Day 7 Caloric Meet | First Quartile (<71.0 %, n = 30) | Second Quartile (71.0%–93.8%, n = 31) | Third Quartile (93.8%–107.4%, n = 31) | Fourth Quartile (>107.4%, n = 30) | p |
|---|---|---|---|---|---|
| Age (years), mean (SD) | 69.6 (15.6) | 68.2 (15.5) | 69.7 (12.8) | 65.7 (16.6) | 0.710 |
| Male, n (%) | 11 (36.7) | 7 (22.6) | 11 (35.5) | 19 (63.3) | 0.011 |
| Body Mass Index, mean (SD) | 22.8 (4.7) | 23.0 (6.8) | 22.0 (4.7) | 23.8 (4.1) | 0.598 |
| Coronary artery disease, n (%) | 9 (30.0) | 4 (12.9) | 9 (29.0) | 13 (43.3) | 0.074 |
| Hypertension, n (%) | 14 (46.7) | 20 (64.5) | 18 (58.1) | 17 (56.7) | 0.568 |
| Diabetes mellitus, n (%) | 13 (43.3) | 12 (38.7) | 15 (48.4) | 18 (60.0) | 0.383 |
| Stroke, n (%) | 8 (26.7) | 8 (26.7) | 5 (16.1) | 4 (13.3) | 0.241 |
| Chronic kidney disease, n (%) | 11 (36.7) | 8 (25.8) | 3 (9.7) | 4 (13.3) | 0.041 |
| Cancer, n (%) | 12 (40.0) | 5 (16.1) | 5 (16.1) | 3 (10.0) | 0.021 |
| Cirrhosis, n (%) | 3 (10.0) | 0 (0.0) | 1 (3.2) | 1 (3.3) | 0.252 |
| SOFA score, mean (SD) | 10.7 (4.6) | 8.9 (3.2) | 9.0 (3.0) | 8.7 (2.8) | 0.105 |
| Interleukin-6, µ/mL, mean (SD) | 198.2 (326.0) | 163.2 (327.2) | 94.3 (159.8) | 56.2 (107.3) | 0.118 |
| NUTRIC score, mean (SD) | 5.7 (2.0) | 5.6 (1.9) | 5.7 (1.8) | 5.3 (1.8) | 0.783 |
| HLA-DR (%), mean (SD) | 81.9 (17.8) | 87.4 (13.8) | 90.4 (13.0) | 89.1 (13.4) | 0.122 |
| β | S.E. | Wals | df | sig | Exp(β) (95% C.I.) | |
|---|---|---|---|---|---|---|
| NUTRIC score | 0.004 | 0.147 | 0.001 | 1 | 0.976 | 1.004 (0.753–1.339) |
| Day 1 HLA-DR (≥87.2% vs. <87.2%) | 0.544 | 0.574 | 0.898 | 1 | 0.343 | 1.723 (0.559–5.307) |
| day 7 caloric meet (≥65.1% vs. <65.1%) | 1.280 | 0.560 | 5.220 | 1 | 0.022 | 3.596 (1.200–10.782) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, K.-Y.; Chen, Y.-M.; Wang, C.-C.; Wang, Y.-H.; Lin, C.-Y.; Chang, Y.-T.; Huang, K.-T.; Lin, M.-C.; Fang, W.-F. Insufficient Nutrition and Mortality Risk in Septic Patients Admitted to ICU with a Focus on Immune Dysfunction. Nutrients 2019, 11, 367. https://doi.org/10.3390/nu11020367
Hung K-Y, Chen Y-M, Wang C-C, Wang Y-H, Lin C-Y, Chang Y-T, Huang K-T, Lin M-C, Fang W-F. Insufficient Nutrition and Mortality Risk in Septic Patients Admitted to ICU with a Focus on Immune Dysfunction. Nutrients. 2019; 11(2):367. https://doi.org/10.3390/nu11020367
Chicago/Turabian StyleHung, Kai-Yin, Yu-Mu Chen, Chin-Chou Wang, Yi-Hsi Wang, Chiung-Yu Lin, Ya-Ting Chang, Kuo-Tung Huang, Meng-Chih Lin, and Wen-Feng Fang. 2019. "Insufficient Nutrition and Mortality Risk in Septic Patients Admitted to ICU with a Focus on Immune Dysfunction" Nutrients 11, no. 2: 367. https://doi.org/10.3390/nu11020367