Micronutrient Status of Recreational Runners with Vegetarian or Non-Vegetarian Dietary Patterns

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Analytical Methods
2.3. References Values
2.4. Data Analysis and Statistical Methods
3. Results
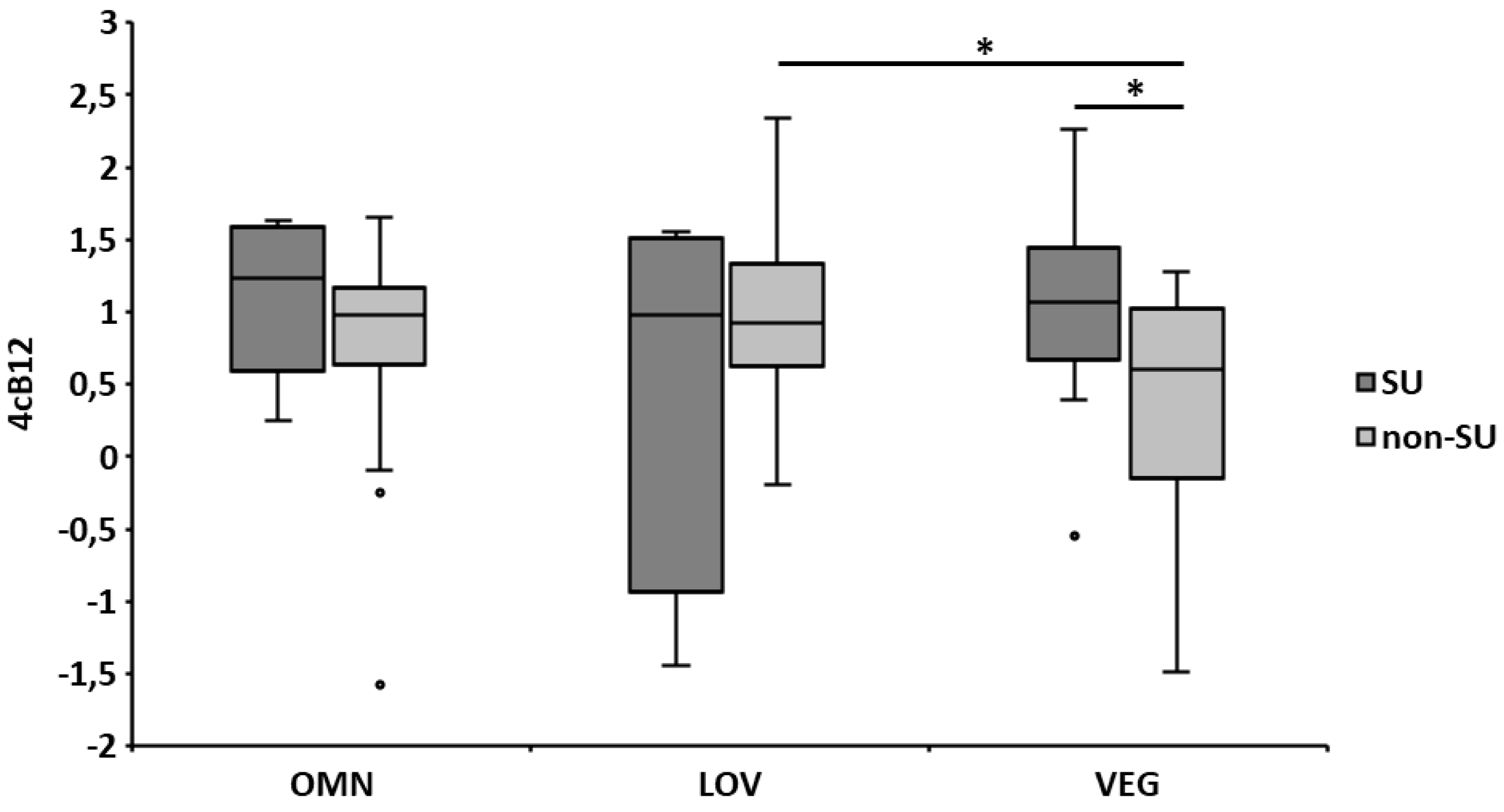
3.1. Biomarkers of Vitamin B12 Status
3.2. Biomarkers of Folate Status
3.3. Biomarkers of Vitamin D Status
3.4. Biomarkers of Iron Status and Hematological Parameters
3.5. Serum Levels of Calcium, Zinc, and Magnesium
4. Discussion
4.1. Vitamin B12
4.2. Red Blood Cell (RBC) Folate
4.3. 25-Hydroxyvitamin D (25(OH)D)
4.4. Iron
4.5. Calcium, Zinc, and Magnesium
4.6. Limitations
4.7. Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Melvin, H.H. Sports Nutrition. In Modern Nutrition in Health and Disease; Shils, M.E., Shike, M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 1723–1737. ISBN 978-0-7817-4133-0. [Google Scholar]
- Baranauskas, M.; Stukas, R.; Tubelis, L.; Žagminas, K.; Šurkienė, G.; Švedas, E.; Giedraitis, V.R.; Dobrovolskij, V.; Abaravičius, J.A. Nutritional habits among high-performance endurance athletes. Medicina 2015, 51, 351–362. [Google Scholar] [CrossRef]
- Faude, O.; Fuhrmann, M.; Herrmann, M.; Kindermann, W.; Urhausen, A. Ernährungsanalysen und Vitaminstatus bei deutschen Spitzenathleten. Leistungssport 2005, 35, 4–9. [Google Scholar]
- Owens, D.J.; Sharples, A.P.; Polydorou, I.; Alwan, N.; Donovan, T.; Tang, J.; Fraser, W.D.; Cooper, R.G.; Morton, J.P.; Stewart, C.; et al. A systems-based investigation into vitamin D and skeletal muscle repair, regeneration, and hypertrophy. Am. J. Physiol. Endocrinol. Metab. 2015, 309, E1019–E1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukaski, H.C. Vitamin and mineral status: Effects on physical performance. Nutrition 2004, 20, 632–644. [Google Scholar] [CrossRef]
- Sabetta, J.R.; DePetrillo, P.; Cipriani, R.J.; Smardin, J.; Burns, L.A.; Landry, M.L. Serum 25-hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS ONE 2010, 5, e11088. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef]
- Agnoli, C.; Baroni, L.; Bertini, I.; Ciappellano, S.; Fabbri, A.; Papa, M.; Pellegrini, N.; Sbarbati, R.; Scarino, M.L.; Siani, V.; et al. Position paper on vegetarian diets from the working group of the Italian Society of Human Nutrition. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1037–1052. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar]
- Phillips, F. Vegetarian nutrition. Nutr. Bull. 2005, 30, 132–167. [Google Scholar] [CrossRef]
- Silva, S.C.G.; Pinho, J.P.; Borges, C.; Santos, C.T.; Santos, A.; Graça, P. Guidelines for A Healthy Vegetarian Diet; Direção-Geral da Saúde: Lisbon, Portugal, 2015. [Google Scholar]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013; ISBN 1-86496-577-0. [Google Scholar]
- Wirnitzer, K.; Seyfart, T.; Leitzmann, C.; Keller, M.; Wirnitzer, G.; Lechleitner, C.; Rüst, C.A.; Rosemann, T.; Knechtle, B. Prevalence in running events and running performance of endurance runners following a vegetarian or vegan diet compared to non-vegetarian endurance runners: The NURMI Study. SpringerPlus 2016, 5, 458. [Google Scholar] [CrossRef] [PubMed]
- Schüpbach, R.; Wegmüller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P.K.; Sabaté, J. Nutritional Implications for Vegetarian Diets. In Modern Nutrition in Health and Disease; Shils, M.E., Shike, M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 1638–1652. ISBN 978-0-7817-4133-0. [Google Scholar]
- McAfee, A.J.; McSorley, E.M.; Cuskelly, G.J.; Moss, B.W.; Wallace, J.M.W.; Bonham, M.P.; Fearon, A.M. Red meat consumption: An overview of the risks and benefits. Meat Sci. 2010, 84, 1–13. [Google Scholar] [CrossRef]
- Iannotti, L.L.; Lutter, C.K.; Bunn, D.A.; Stewart, C.P. Eggs: The uncracked potential for improving maternal and young child nutrition among the world’s poor. Nutr. Rev. 2014, 72, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Sioen, I.; De Henauw, S.; Van Camp, J. Evaluation of benefits and risks related to seafood consumption. Verhandelingen-Koninklijke Academie voor Geneeskunde van Belgie 2007, 69, 249–289. [Google Scholar] [PubMed]
- Weaver, C.M. Should dairy be recommended as part of a healthy vegetarian diet? Point. Am. J. Clin. Nutr. 2009, 89, 1634S–1637S. [Google Scholar] [CrossRef] [Green Version]
- Ströhle, A.; Hahn, A. Kritische Mikronährstoffe bei veganer Ernährung—Ein Update. MMP 2018, 41, 113–121. [Google Scholar]
- Hanne, N.; Dlin, R.; Rotstein, A. Physical fitness, anthropometric and metabolic parameters in vegetarian athletes. J. Sports Med. Phys. Fit. 1986, 26, 180–185. [Google Scholar]
- Williams, P.T. Interactive effects of exercise, alcohol, and vegetarian diet on coronary artery disease risk factors in 9242 runners: The National Runners’ Health Study. Am. J. Clin. Nutr. 1997, 66, 1197–1206. [Google Scholar] [CrossRef]
- Schilling, K.A.; Wiesgigl, M. The Elecsys® Vitamin B12 assay is not affected by anti-intrinsic factor antibodies. Clin. Chem. Lab. Med. 2013, 51, e251–e252. [Google Scholar] [CrossRef]
- Harrington, D.J. Laboratory Assessment of Vitamin Status; Academic Press: Cambridge, MA, USA, 2019; ISBN 978-0-12-813051-3. [Google Scholar]
- Mineva, E.M.; Zhang, M.; Rabinowitz, D.J.; Phinney, K.W.; Pfeiffer, C.M. An LC-MS/MS method for serum methylmalonic acid suitable for monitoring vitamin B12 status in population surveys. Anal. Bioanal. Chem. 2015, 407, 2955–2964. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, A.; Olejarz, P.; Borowczyk, K.; Głowacki, R.; Chwatko, G. Simultaneous determination of total homocysteine, cysteine, glutathione, and N-acetylcysteine in brain homogenates by HPLC. J. Sep. Sci. 2018, 41, 3241–3249. [Google Scholar] [CrossRef]
- Fedosov, S.N.; Brito, A.; Miller, J.W.; Green, R.; Allen, L.H. Combined indicator of vitamin B12 status: Modification for missing biomarkers and folate status and recommendations for revised cut-points. Clin. Chem. Lab. Med. 2015, 53, 1215–1225. [Google Scholar] [CrossRef]
- Leino, A.; Turpeinen, U.; Koskinen, P. Automated Measurement of 25-OH Vitamin D3 on the Roche Modular E170 Analyzer. Clin. Chem. 2008, 54, 2059–2062. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.; Chanarin, I.; Slavin, G.; Levi, A.J. Folate Deficiency in the Alcoholic—Its Relationship to Clinical and Haematological Abnormalities, Liver Disease and Folate Stores. Br. J. Haematol. 1975, 29, 469–478. [Google Scholar] [CrossRef]
- Roche Diagnostics International Ltd. Elecsys® Folate RBC—Electrochemiluminescence Immunoassay (ECLIA) for the in vitro Quantitative Determination of Folate in Erythrocytes (Red Blood Cells, RBC). 2014. Available online: https://www.google.com.tw/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=2ahUKEwiq3oCkyqviAhXSfXAKHSV_BugQFjAAegQIAxAC&url=https%3A%2F%2Fdiagnostics.roche.com%2Fcontent%2Fdam%2Fdiagnostics%2Fch%2Fde%2Fgesundheitsthemen%2Fanaemia%2FAnemia_Factsheet_FolateRBC.pdf&usg=AOvVaw0gfL3lcLP6WENudhxG7OBx (accessed on 9 April 2019).
- Bauer, P.J. Affinity and stoichiometry of calcium binding by arsenazo III. Anal. Biochem. 1981, 110, 61–72. [Google Scholar] [CrossRef]
- Mann, C.K.; Yoe, J.H. Spectrophotometric Determination of Magnesium with Sodium 1-Azo-2-hydroxy-3-(2,4-dimethylcarboxanilido)-naphthalene-1′-(2-hydroxybenzene-5-sulfonate). Anal. Chem. 1956, 28, 202–205. [Google Scholar] [CrossRef]
- Beaty, R.D.; Kerber, J. Concepts, Instrumentation and Techniques in Atomic Absorption Spectrophotometry, 2nd ed.; The Perkin Elmer Corporation: Norwalk, CT, USA, 1993. [Google Scholar]
- Strzelak, K.; Rybkowska, N.; Wiśniewska, A.; Koncki, R. Photometric flow analysis system for biomedical investigations of iron/transferrin speciation in human serum. Anal. Chim. Acta 2017, 995, 43–51. [Google Scholar] [CrossRef]
- Kaplan, L.A.; Pesce, A.J.; Kazmierczak, S.C. Principles for Competitive-Binding Assays. In Clinical Chemistry: Theory, Analysis, Correlation, 4th ed.; Mosby: St. Louis, MO, USA, 2003; ISBN 978-0-323-01716-9. [Google Scholar]
- Bernard, A.; Lauwerys, R. Turbidimetric latex immunoassay for serum ferritin. J. Immunol. Methods 1984, 71, 141–147. [Google Scholar] [CrossRef]
- Kiese, M. Empfindliche photometrische Verfahren zur Bestimmung von Hämiglobin und Hämoglobin. Naunyn-Schmiedebergs Arch. 1947, 204, 190–202. [Google Scholar] [CrossRef]
- van Kampen, E.; Zijlstra, W.G. Standardization of hemoglobinometry. II. The hemiglobincyanide method. Clin. Chim. Acta 1961, 6, 538–544. [Google Scholar] [CrossRef]
- Singh, A.K.; Shinton, N.K. International Committee for Standardization in Haematology of the European Society of Haematology: Recommendations and Requirements for Haemoglobinometry in Human Blood. J. Clin. Pathol. 1965, 18, 353–355. [Google Scholar]
- Camaschella, C. Iron deficiency: New insights into diagnosis and treatment. Hematology 2015, 2015, 8–13. [Google Scholar] [CrossRef]
- World Health Organization. Iron Deficiency Anaemia: Assessment, Prevention, and Control: A Guide for Programme Managers; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Sarma, P.R. Red Cell Indices. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990; ISBN 978-0-409-90077-4. [Google Scholar]
- de Benoist, B. Conclusions of a WHO Technical Consultation on folate and vitamin B12 deficiencies. Food Nutr. Bull. 2008, 29, S238–S244. [Google Scholar] [CrossRef]
- Herrmann, W.; Schorr, H.; Bodis, M.; Knapp, J.P.; Müller, A.; Stein, G.; Geisel, J. Role of homocysteine, cystathionine and methylmalonic acid measurement for diagnosis of vitamin deficiency in high-aged subjects. Eur. J. Clin. Investig. 2000, 30, 1083–1089. [Google Scholar] [CrossRef]
- Herrmann, W.; Obeid, R.; Schorr, H.; Geisel, J. Functional vitamin B12 deficiency and determination of holotranscobalamin in populations at risk. Clin. Chem. Lab. Med. 2003, 41, 1478–1488. [Google Scholar] [CrossRef]
- Hvas, A.-M.; Nexo, E. Holotranscobalamin as a predictor of vitamin B12 status. Clin. Chem. Lab. Med. 2003, 41, 1489–1492. [Google Scholar] [CrossRef]
- Malinow, M.R.; Bostom, A.G.; Krauss, R.M. Homocyst(e)ine, diet, and cardiovascular diseases: A statement for healthcare professionals from the Nutrition Committee, American Heart Association. Circulation 1999, 99, 178–182. [Google Scholar] [CrossRef]
- Obersby, D.; Chappell, D.C.; Dunnett, A.; Tsiami, A.A. Plasma total homocysteine status of vegetarians compared with omnivores: A systematic review and meta-analysis. Br. J. Nutr. 2013, 109, 785–794. [Google Scholar] [CrossRef]
- Zittermann, A.; Gummert, J.F. Nonclassical Vitamin D Actions. Nutrients 2010, 2, 408–425. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US); Committee to Review Dietary Reference Intakes for Vitamin D and Calcium Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Thomas, L. Calcium (Ca). In Clinical Laboratory Diagnostics: Use and Assessment of Clinical Laboratory Results; Thomas, L., Andert, S.E., Ansorg, R., Eds.; Th-Books Verlagsgesellschaft mbH: Frankfurt/Mainz, Germany, 1998; pp. 231–234. ISBN 978-3-9805215-4-3. [Google Scholar]
- Dörner, K. Magnesium (Mg). In Clinical Laboratory Diagnostics: Use and Assessment of Clinical Laboratory Results; Thomas, L., Andert, S.E., Ansorg, R., Eds.; Th-Books Verlagsgesellschaft mbH: Frankfurt/Mainz, Germany, 1998; pp. 339–340. ISBN 978-3-9805215-4-3. [Google Scholar]
- Gibson, R.S.; Hess, S.Y.; Hotz, C.; Brown, K.H. Indicators of zinc status at the population level: A review of the evidence. Br. J. Nutr. 2008, 99 (Suppl. S3), S14–S23. [Google Scholar] [CrossRef]
- Aparicio-Ugarriza, R.; Palacios, G.; Alder, M.; González-Gross, M. A review of the cut-off points for the diagnosis of vitamin B12 deficiency in the general population. Clin. Chem. Lab. Med. 2014, 53, 1149–1159. [Google Scholar] [CrossRef]
- Pawlak, R.; Lester, S.E.; Babatunde, T. The prevalence of cobalamin deficiency among vegetarians assessed by serum vitamin B12: A review of literature. Eur. J. Clin. Nutr. 2014, 68, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Wright, Z.; Hvas, A.-M.; Møller, J.; Sanders, T.A.B.; Nexø, E. Holotranscobalamin as an indicator of dietary vitamin B12 deficiency. Clin. Chem. 2003, 49, 2076–2078. [Google Scholar] [CrossRef]
- Ströhle, A.; Richter, M.; González-Gross, M.; Neuhäuser-Berthold, M.; Wagner, K.-H.; Leschik-Bonnet, E.; Egert, S. The Revised D-A-CH-Reference Values for the Intake of Vitamin B12: Prevention of Deficiency and Beyond. Mol. Nutr. Food Res. 2019, e1801178. [Google Scholar] [CrossRef]
- Pawlak, R.; Parrott, S.J.; Raj, S.; Cullum-Dugan, D.; Lucus, D. How prevalent is vitamin B12 deficiency among vegetarians? Nutr. Rev. 2013, 71, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Damayanti, D.; Jaceldo-Siegl, K.; Beeson, W.L.; Fraser, G.; Oda, K.; Haddad, E.H. Foods and Supplements Associated with Vitamin B12 Biomarkers among Vegetarian and Non-Vegetarian Participants of the Adventist Health Study-2 (AHS-2) Calibration Study. Nutrients 2018, 10, 722. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Narbón, A.; Zapatera, B.; Barrios, L.; Vaquero, M.P. Vitamin B12 and folate status in Spanish lacto-ovo vegetarians and vegans. J. Nutr. Sci. 2019, 8, e7. [Google Scholar] [CrossRef] [PubMed]
- Miles, F.L.; Lloren, J.I.C.; Haddad, E.; Jaceldo-Siegl, K.; Knutsen, S.; Sabate, J.; Fraser, G.E. Plasma, Urine, and Adipose Tissue Biomarkers of Dietary Intake Differ Between Vegetarian and Non-Vegetarian Diet Groups in the Adventist Health Study-2. J. Nutr. 2019, 149, 667–675. [Google Scholar] [CrossRef]
- Pilz, S.; Zittermann, A.; Trummer, C.; Schwetz, V.; Lerchbaum, E.; Keppel, M.; Grübler, M.; Maerz, W.; Pandis, M. Vitamin D testing and treatment: A narrative review of current evidence. Endocr. Connect. 2019, 8, R27–R43. [Google Scholar] [CrossRef]
- de Koning, L.; Al-Turkmani, M.R.; Berg, A.H.; Shkreta, A.; Law, T.; Kellogg, M.D. Variation in clinical vitamin D status by DiaSorin Liaison and LC-MS/MS in the presence of elevated 25-OH vitamin D2. Clin. Chim. Acta 2013, 415, 54–58. [Google Scholar] [CrossRef] [PubMed]
- van den Ouweland, J.M.W.; Beijers, A.M.; Demacker, P.N.M.; van Daal, H. Measurement of 25-OH-vitamin D in human serum using liquid chromatography tandem-mass spectrometry with comparison to radioimmunoassay and automated immunoassay. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2010, 878, 1163–1168. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Jaceldo-Siegl, K.; Fraser, G.E. Serum 25-hydroxyvitamin D status of vegetarians, partial vegetarians, and nonvegetarians: The Adventist Health Study-2. Am. J. Clin. Nutr. 2009, 89, 1686S–1692S. [Google Scholar] [CrossRef]
- Farrokhyar, F.; Tabasinejad, R.; Dao, D.; Peterson, D.; Ayeni, O.R.; Hadioonzadeh, R.; Bhandari, M. Prevalence of vitamin D inadequacy in athletes: A systematic-review and meta-analysis. Sports Med. 2015, 45, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Wentz, L.M.; Liu, P.-Y.; Ilich, J.Z.; Haymes, E.M. Female Distance Runners Training in Southeastern United States Have Adequate Vitamin D Status. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 397–403. [Google Scholar] [CrossRef]
- Rabenberg, M.; Scheidt-Nave, C.; Busch, M.A.; Rieckmann, N.; Hintzpeter, B.; Mensink, G.B.M. Vitamin D status among adults in Germany—Results from the German Health Interview and Examination Survey for Adults (DEGS1). BMC Public Health 2015, 15, 641. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Webb, A.R. Who, what, where and when—influences on cutaneous vitamin D synthesis. Prog. Biophys. Mol. Biol. 2006, 92, 17–25. [Google Scholar] [CrossRef] [PubMed]
- WHO. Serum Ferritin Concentrations for the Assessment of Iron Status and Iron Deficiency in Populations; Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Goodnough, L.T.; Nemeth, E.; Ganz, T. Detection, evaluation, and management of iron-restricted erythropoiesis. Blood 2010, 116, 4754–4761. [Google Scholar] [CrossRef]
- Craig, W.J. Iron status of vegetarians. Am. J. Clin. Nutr. 1994, 59, 1233S–1237S. [Google Scholar] [CrossRef] [Green Version]
- Elorinne, A.-L.; Alfthan, G.; Erlund, I.; Kivimäki, H.; Paju, A.; Salminen, I.; Turpeinen, U.; Voutilainen, S.; Laakso, J. Food and Nutrient Intake and Nutritional Status of Finnish Vegans and Non-Vegetarians. PLoS ONE 2016, 11, e0148235. [Google Scholar] [CrossRef] [PubMed]
- Haider, L.M.; Schwingshackl, L.; Hoffmann, G.; Ekmekcioglu, C. The effect of vegetarian diets on iron status in adults: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 58, 1359–1374. [Google Scholar] [CrossRef]
- Waldmann, A.; Koschizke, J.W.; Leitzmann, C.; Hahn, A. Dietary Iron Intake and Iron Status of German Female Vegans: Results of the German Vegan Study. Ann. Nutr. Metab. 2004, 48, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Snyder, A.C.; Dvorak, L.L.; Roepke, J.B. Influence of dietary iron source on measures of iron status among female runners. Med. Sci. Sports Exerc. 1989, 21, 7. [Google Scholar] [CrossRef] [PubMed]
- Alaunyte, I.; Stojceska, V.; Plunkett, A. Iron and the female athlete: A review of dietary treatment methods for improving iron status and exercise performance. J. Int. Soc. Sports Nutr. 2015, 12, 38. [Google Scholar] [CrossRef]


{kind=link}
| Measure | Omnivores (n = 27) | Lacto-Ovo (n = 26) | Vegan (n = 28) | p value |
|---|---|---|---|---|
| Age, years | 27.4 ± 4.03 | 27.6 ± 4.31 | 27.5 ± 4.24 | 0.968 a |
| Sex | m = 11, f = 16 | m = 10, f = 16 | m = 10, f = 18 | 0.929 b |
| BMI, kg/m2 | 22.3 ± 1.74 | 21.6 ± 1.98 | 22.1 ± 2.09 | 0.436 a |
| Duration of diet | 0.001 b | |||
| 0.5–1 year, n (%) | 0 (0) | 4 (15) | 6 (21) | |
| 1–2 years, n (%) | 1 (4) | 3 (12) | 4 (14) | |
| 2–3 years, n (%) | 0 (0) | 2 (8) | 7 (25) | |
| >3 years, n (%) | 26 (96) | 17 (65) | 11 (39) | |
| Vitamin B12 SU, n (%) | 4 (19) | 4 (15) | 15 (54) | 0.005 b |
| Vitamin D SU, n (%) | 5 (22) | 1 (4) | 7 (25) | 0.078 b |
| Folate SU, n (%) | 3 (11) | 1 (4) | 5 (18) | 0.262 b |
| Iron SU, n (%) | 3 (11) | 4 (15) | 5 (18) | 0.689 b |
| Calcium SU, n (%) | 3 (11) | 1 (4) | 2 (7) | 0.210 b |
| Zinc SU, n (%) | 4 (15) | 3 (12) | 2 (7) | 0.662 b |
| Magnesium SU, n (%) | 5 (22) | 4 (15) | 5 (18) | 0.770 b |
| Training frequency per week | 3.04 ± 0.98 | 3.24 ± 0.88 | 3.00 ± 0.85 | 0.502 a |
| Running time per week, h | 2.72 ± 1.11 | 3.38 ± 1.43 | 2.65 ± 1.38 | 0.079 b |
| Parameter | Supplementation | Omnivores n = 27 | p value Omnivores vs. Lacto-Ovo | Lacto-Ovo n = 26 | p value Lacto-Ovo vs. Vegan | Vegan n = 28 | p value Omnivores vs. Vegan | p value |
|---|---|---|---|---|---|---|---|---|
| nSU | 5 | 4 | 15 | |||||
| nnon-SU | 22 | 22 | 13 | |||||
| Vitamin B12, pmol/L | 323 ± 121 | - | 316 ± 146 | - | 320 ± 247 | - | 0.586 b | |
| SU | 350 ± 112 | - | 261 ± 149 | - | 396 ± 318 | - | 0.590 b | |
| non-SU | 316 ± 124 | - | 326 ± 148 | - | 244 ± 115 | - | 0.118 b | |
| Deficient (<150 pmol/L), n (%) | 1 (4) | 2 (8) | 3 (11) | 0.349 d | ||||
| SU | 0 (0) | 1 (4) | 1 (4) | |||||
| non-SU | 1 (4) | 1 (4) | 2 (7) | |||||
| Holo-TC, pmol/L | 80.4 ± 30.1 | - | 85.9 ± 36.9 | 67.8 ± 39.4 | - | 0.168 a | ||
| SU | 92.4 ± 37.7 | - | 80.5 ± 53.5 | 82.0 ± 37.9 | - | 0.871 a | ||
| non-SU | 76.1 ± 28.9 | n.s. | 86.8 ± 34.7 | 0.013 c | 52.1 ± 37.9 | n.s. | 0.016 a | |
| Deficient (<35 pmol/L), n (%) | 1 (4) | 2 (8) | 6 (21) | 0.043 d | ||||
| SU | 0 (0) | 1 (4) | 1 (4) | |||||
| non-SU | 1 (4) | 1 (4) | 5 (18) | |||||
| MMA, nmol/L | 264 ± 174 | - | 266 ± 176 | - | 363 ± 570 | - | 0.693 b | |
| SU | 261 ± 177 | - | 400 ± 362 | - | 216 ± 161 | - | 0.186 b | |
| non-SU | 264 ± 177 | - | 234 ± 123 | - | 535 ± 801 | - | 0.226 b | |
| Deficient (>271 nmol/L), n (%) | 6 (22) | 7 (27) | 8 (29) | 0.720 d | ||||
| SU | 1 (4) | 2 (8) | 1 (4) | |||||
| non-SU | 5 (19) | 5 (19) | 7 (25) | |||||
| tHcy, µmol/L | 12.2 ± 2.93 | - | 13.2 ± 6.47 | - | 12.8 ± 4.26 | - | 0.920 b | |
| >10 µmol/L, n (%) | 19 (82) | 15 (58) | 22 (79) | - | 0.266 d | |||
| 4cB12 | 0.91 ± 0.50 | - | 0.91 ± 0.75 | - | 0.70 ± 0.76 | - | 0.442 a | |
| SU | 1.12 ± 0.56 | - | 0.52 ± 1.37 | - | 1.10 ± 0.67 | - | 0.490 a | |
| non-SU | 0.86 ± 0.49 | n.s. | 0.98 ± 0.60 | 0.020 c | 0.35 ± 0.75 | n.s. | 0.021 a |
| Parameter | Omnivores n = 27 | Lacto-Ovo n = 26 | Vegan n = 28 | p value | |
|---|---|---|---|---|---|
| nSU | 3 | 1 | 5 | ||
| nnon-SU | 24 | 25 | 23 | ||
| RBC folate, nmol/L | 2213 ± 444 | 2236 ± 596 | 2354 ± 639 | 0.577 a | |
| SU | 2254 ± 776 | 1456 ± 0 | 2903 ± 494 | 0.134 a | |
| non-SU | 2207 ± 413 | 2246 ± 586 | 2233 ± 609 | 0.966 a | |
| Deficient (<340 nmol/L), n (%) | 0 | 0 | 0 | - | |
| nSU | 6 | 1 | 7 | ||
| nnon-SU | 21 | 25 | 21 | ||
| 25(OH)D, nmol/L | 90.6 ± 32.1 | 76.8 ± 33.7 | 86.2 ± 39.5 | 0.354 a | |
| SU | 120 ± 40.4 | 152 ± 0 | 117 ± 26.3 | 0.619 a | |
| non-SU | 82.2 ± 24.6 | 73.8 ± 30.6 | 73.8 ± 37.3 | 0.592 a | |
| Optimal | 18 (67) | 11 (42) | 16 (57) | 0.219 b | |
| (≥75 nmol), n (%) | SU | 5 (19) | 1 (4) | 7 (25) | |
| non-SU | 13 (48) | 10 (39) | 9 (32) | ||
| Sufficient | 6 (22) | 10 (39) | 5 (18) | ||
| (50–74.9 nmol/L), n (%) | SU | 1 (4) | 0 (0) | 1 (4) | |
| non-SU | 5 (19) | 10 (39) | 4 (14) | ||
| Insufficient | 3 (11) | 5 (19) | 5 (18) | ||
| (25–49.9 nmol/L), n (%) | SU | 0 (0) | 0 (0) | 0 (0) | |
| non-SU | 3 (11) | 5 (19) | 5 (18) | ||
| Deficient | 0 (0) | 0 (0) | 2 (7) | ||
| (<25 nmol/L), n (%) | SU | 0 (0) | 0 (0) | 0 (0) | |
| non-SU | 0 (0) | 0 (0) | 2 (7) |
| Parameter | Omnivores n = 27, | p value Omnivores vs. Lacto-Ovo | Lacto-Ovo n = 26, | p value Lacto-Ovo vs. Vegan | Vegan n = 28 | p value Omnivores vs. Vegan | p value | |
|---|---|---|---|---|---|---|---|---|
| nSU nnon-SU | 3 24 | 4 22 | 5 23 | |||||
| Iron serum, µmol/L | f m | 14.5 ± 7.91 22.2 ± 6.37 | - - | 16.7 ± 7.03 20.0 ± 8.76 | - - | 15.7 ± 6.00 18.4 ± 6.80 | - - | 0.671 a 0.493 a |
| Deficiency (<10 µmol/L), n (%) | f m | 7 (26) 0 (0) | 4 (15) 1 (4) | 2 (7) 0 (0) | 0.353 d - | |||
| Ferritin, µg/L Depleted iron stores (<15 µg/L), n (%) | f m f m | 25.9 ± 23.0 115 ± 44.8 7 (26) 0 (0) | - 0.024 c | 23.9 ± 12.9 64.3 ± 40.7 6 (23) 0 (0) | - n.s. | 32.1 ± 22.8 64.6 ± 36.7 5 (18) 0 (0) | - 0.028 c | 0.441 b 0.010 b 0.619 d - |
| Transferrin, µmol/L Increased iron requirement (≥47.7 µmol/L), n (%) | f m f m | 46.4 ± 12.9 34.7 ± 4.27 6 (22) 0 (0) | - - | 41.6 ± 7.79 38.2 ± 4.40 3 (12) 1 (4) | - - | 40.2 ± 7.54 39.0 ± 6.16 3 (11) 0 (0) | - - | 0.316 b 0.092 b 0.306 d - |
| Transferrin saturation | f m | 17.2 ± 12.6 32.5 ± 10.2 | - - | 21.0 ± 9.97 26.8 ± 12.2 | - - | 20.4 ± 8.93 24.8 ± 11.6 | - - | 0.543 a 0.288 a |
| Insufficient iron supply (<16%), n (%) | f m | 10 (37) 0 (0) | 5 (19) 1 (4) | 7 (25) 3 (11) | 0.184 d 0.261 d | |||
| Hb, g/dL | f m | 13.0 ± 1.08 15.1 ± 0.64 | - - | 13.6 ± 0.78 14.8 ± 1.00 | - - | 13.4 ± 1.20 15.2 ± 0.84 | - - | 0.260 a 0.661 a |
| Anemia (<12.0 g/dL), n (%) (<13.0 g/dL), n (%) | f m | 3 (11) 0 (0) | 0 (0) 0 (0) | 4 (14) 0 (0) | 0.198 d - | |||
| Hct, L/L | f m | 0.39 ± 0.03 0.44 ± 0.03 | - - | 0.41 ± 0.03 0.43 ± 0.02 | - - | 0.41 ± 0.04 0.44 ± 0.03 | - - | 0.083 a 0.730 a |
| < 0.36 (f)/0.39 (m), n (%) | 0 (0) | 0 (0) | 0 (0) | - | ||||
| MCV, fl Iron deficiency anemia (<80 fl), n (%) | f m | 87.7 ± 3.34 87.2 ± 2.78 0 (0) | - - | 89.3 ± 5.06 88.8 ± 3.42 0 (0) | - - | 89.5 ± 3.59 87.3 ± 4.05 0 (0) | - - | 0.410 b 0.597 b - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nebl, J.; Schuchardt, J.P.; Ströhle, A.; Wasserfurth, P.; Haufe, S.; Eigendorf, J.; Tegtbur, U.; Hahn, A. Micronutrient Status of Recreational Runners with Vegetarian or Non-Vegetarian Dietary Patterns. Nutrients 2019, 11, 1146. https://doi.org/10.3390/nu11051146
Nebl J, Schuchardt JP, Ströhle A, Wasserfurth P, Haufe S, Eigendorf J, Tegtbur U, Hahn A. Micronutrient Status of Recreational Runners with Vegetarian or Non-Vegetarian Dietary Patterns. Nutrients. 2019; 11(5):1146. https://doi.org/10.3390/nu11051146
Chicago/Turabian StyleNebl, Josefine, Jan Philipp Schuchardt, Alexander Ströhle, Paulina Wasserfurth, Sven Haufe, Julian Eigendorf, Uwe Tegtbur, and Andreas Hahn. 2019. "Micronutrient Status of Recreational Runners with Vegetarian or Non-Vegetarian Dietary Patterns" Nutrients 11, no. 5: 1146. https://doi.org/10.3390/nu11051146