Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System

Abstract
:1. Introduction
2. Materials and Methods
2.1. Score Participants and Approach
2.2. Creating the Score
3. Results
3.1. Healthy Weight Sub-Score
3.2. Physical Activity Sub-Score
3.3. Wholegrains, Vegetables, Fruit, and Beans Sub-Score
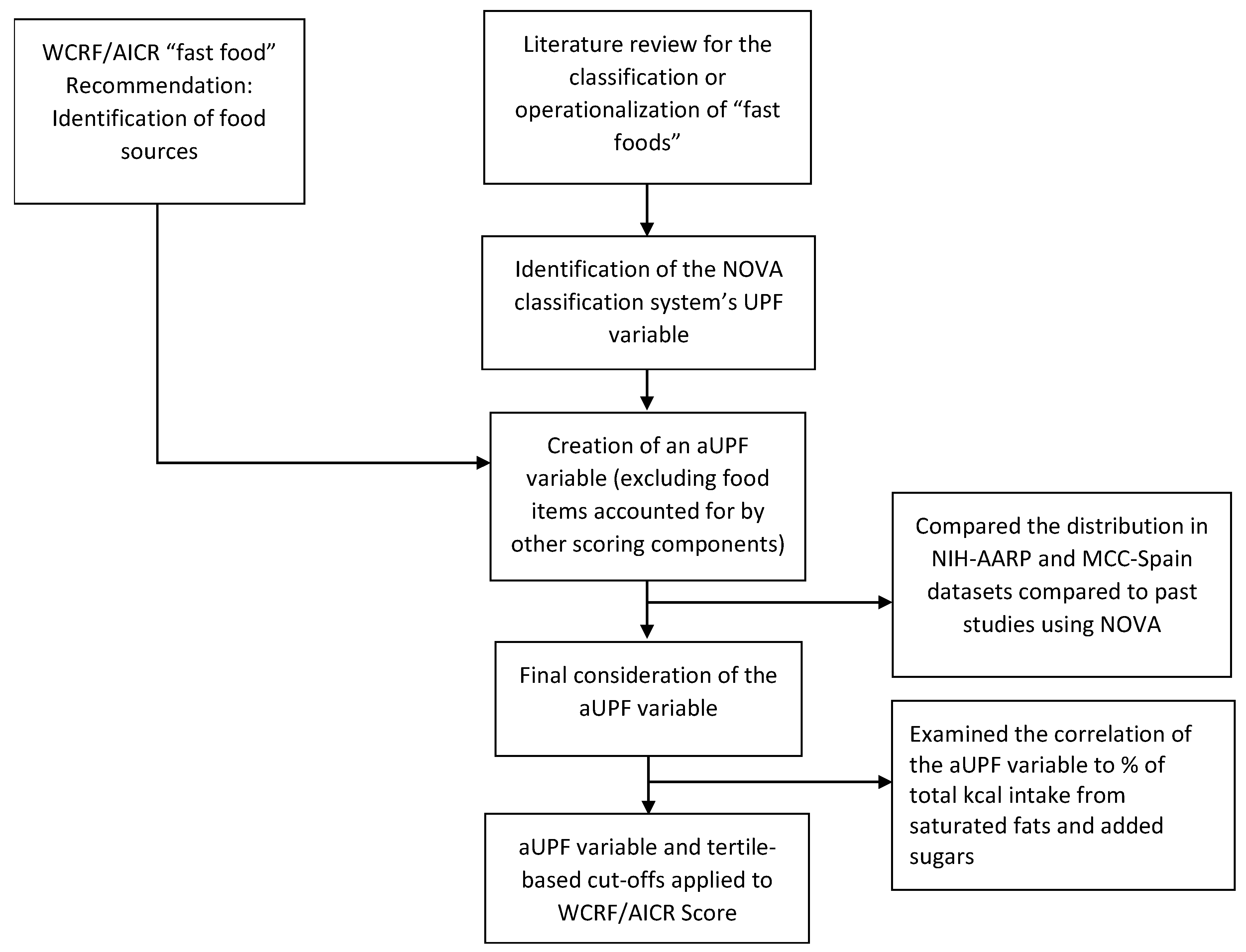
3.4. “Fast-foods” Sub-Score
3.5. Red and Processed Meat Sub-Score
3.6. Sugar-Sweetened Drinks Sub-Score
3.7. Alcohol Consumption Sub-Score
3.8. Breastfeeding Sub-Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. Available online: http://dietandcancerreport.org (accessed on 11 March 2019).
- Arab, L.; Su, J.; Steck, S.E.; Ang, A.; Fontham, E.T.; Bensen, J.T.; Mohler, J.L. Adherence to World Cancer Research Fund/American Institute for Cancer Research lifestyle recommendations reduces prostate cancer aggressiveness among African and Caucasian Americans. Nutr. Cancer 2013, 65, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Castello, A.; Martin, M.; Ruiz, A.; Casas, A.M.; Baena-Canada, J.M.; Lope, V.; Antolin, S.; Sanchez, P.; Ramos, M.; Anton, A.; et al. Lower Breast Cancer Risk among Women following the World Cancer Research Fund and American Institute for Cancer Research Lifestyle Recommendations: EpiGEICAM Case-Control Study. PLoS ONE 2015, 10, e0126096. [Google Scholar] [CrossRef] [PubMed]
- Catsburg, C.; Miller, A.B.; Rohan, T.E. Adherence to cancer prevention guidelines and risk of breast cancer. Int. J. Cancer 2014, 135, 2444–2452. [Google Scholar] [CrossRef] [PubMed]
- Er, V.; Lane, J.A.; Martin, R.M.; Emmett, P.; Gilbert, R.; Avery, K.N.; Walsh, E.; Donovan, J.L.; Neal, D.E.; Hamdy, F.C.; et al. Adherence to dietary and lifestyle recommendations and prostate cancer risk in the prostate testing for cancer and treatment (ProtecT) trial. Cancer Epidemiol. Biomark. 2014, 23, 2066–2077. [Google Scholar] [CrossRef] [PubMed]
- Fanidi, A.; Ferrari, P.; Biessy, C.; Ortega, C.; Angeles-Llerenas, A.; Torres-Mejia, G.; Romieu, I. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and breast cancer risk in the Cancer de Mama (CAMA) study. Public Health Nutr. 2015, 18, 3337–3348. [Google Scholar] [CrossRef] [PubMed]
- Harris, H.R.; Bergkvist, L.; Wolk, A. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and breast cancer risk. Int. J. Cancer 2016, 138, 2657–2664. [Google Scholar] [CrossRef] [PubMed]
- Hastert, T.A.; Beresford, S.A.; Patterson, R.E.; Kristal, A.R.; White, E. Adherence to WCRF/AICR cancer prevention recommendations and risk of postmenopausal breast cancer. Cancer Epidemiol. Prev. Biomark. 2013, 22, 1498–1508. [Google Scholar] [CrossRef]
- Jankovic, N.; Geelen, A.; Winkels, R.M.; Mwungura, B.; Fedirko, V.; Jenab, M.; Illner, A.K.; Brenner, H.; Ordonez-Mena, J.M.; Kiefte de Jong, J.C.; et al. Adherence to the WCRF/AICR Dietary Recommendations for Cancer Prevention and Risk of Cancer in Elderly from Europe and the United States: A Meta-Analysis within the CHANCES Project. Cancer Epidemiol. Prev. Biomark. 2017, 26, 136–144. [Google Scholar] [CrossRef]
- Kohler, L.N.; Garcia, D.O.; Harris, R.B.; Oren, E.; Roe, D.J.; Jacobs, E.T. Adherence to Diet and Physical Activity Cancer Prevention Guidelines and Cancer Outcomes: A Systematic Review. Cancer Epidemiol. Prev. Biomark. 2016, 25, 1018–1028. [Google Scholar] [CrossRef] [Green Version]
- Lohse, T.; Faeh, D.; Bopp, M.; Rohrmann, S. Adherence to the cancer prevention recommendations of the World Cancer Research Fund/American Institute for Cancer Research and mortality: A census-linked cohort. Am. J. Clin. Nutr. 2016, 104, 678–685. [Google Scholar] [CrossRef]
- Lucas, A.L.; Bravi, F.; Boffetta, P.; Polesel, J.; Serraino, D.; La Vecchia, C.; Bosetti, C. Adherence to World Cancer Research Fund/American Institute for Cancer Research recommendations and pancreatic cancer risk. Cancer Epidemiol. 2016, 40, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Makarem, N.; Lin, Y.; Bandera, E.V.; Jacques, P.F.; Parekh, N. Concordance with World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) guidelines for cancer prevention and obesity-related cancer risk in the Framingham Offspring cohort (1991-2008). Cancer Causes Control. 2015, 26, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.J.; Inoue-Choi, M.; Lazovich, D.; Robien, K. WCRF/AICR recommendation adherence and breast cancer incidence among postmenopausal women with and without non-modifiable risk factors. Int. J. Cancer 2016, 138, 2602–2615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romaguera, D.; Vergnaud, A.C.; Peeters, P.H.; Van Gils, C.H.; Chan, D.S.; Ferrari, P.; Romieu, I.; Jenab, M.; Slimani, N.; Clavel-Chapelon, F.; et al. Is concordance with World Cancer Research Fund/American Institute for Cancer Research guidelines for cancer prevention related to subsequent risk of cancer? Results from the EPIC study. Am. J. Clin. Nutr. 2012, 96, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Ward, H.; Wark, P.A.; Vergnaud, A.C.; Peeters, P.H.; Van Gils, C.H.; Ferrari, P.; Fedirko, V.; Jenab, M.; Boutron-Ruault, M.C.; et al. Pre-diagnostic concordance with the WCRF/AICR guidelines and survival in European colorectal cancer patients: A cohort study. BMC Med. 2015, 13, 107. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Bravi, F.; Di Maso, M.; Bosetti, C.; Polesel, J.; Serraino, D.; Dalmartello, M.; Giacosa, A.; Montella, M.; Tavani, A.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and colorectal cancer risk. Eur. J. Cancer 2017, 85, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Vergnaud, A.C.; Romaguera, D.; Peeters, P.H.; Van Gils, C.H.; Chan, D.S.; Romieu, I.; Freisling, H.; Ferrari, P.; Clavel-Chapelon, F.; Fagherazzi, G.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research guidelines and risk of death in Europe: Results from the European Prospective Investigation into Nutrition and Cancer cohort study1,4. Am. J. Clin. Nutr. 2013, 97, 1107–1120. [Google Scholar] [CrossRef]
- Inoue-Choi, M.; Robien, K.; Lazovich, D. Adherence to the WCRF/AICR guidelines for cancer prevention is associated with lower mortality among older female cancer survivors. Cancer Epidemiol. Prev. Biomark. 2013, 22, 792–802. [Google Scholar] [CrossRef]
- Nomura, S.J.; Dash, C.; Rosenberg, L.; Yu, J.; Palmer, J.R.; Adams-Campbell, L.L. Is adherence to diet, physical activity, and body weight cancer prevention recommendations associated with colorectal cancer incidence in African American women? Cancer Causes Control. 2016, 27, 869–879. [Google Scholar] [CrossRef] [Green Version]
- Nomura, S.J.; Dash, C.; Rosenberg, L.; Yu, J.; Palmer, J.R.; Adams-Campbell, L.L. Adherence to diet, physical activity and body weight recommendations and breast cancer incidence in the Black Women’s Health Study. Int. J. Cancer 2016, 139, 2738–2752. [Google Scholar] [CrossRef]
- Hastert, T.A.; Beresford, S.A.; Sheppard, L.; White, E. Adherence to the WCRF/AICR cancer prevention recommendations and cancer-specific mortality: Results from the Vitamins and Lifestyle (VITAL) Study. Cancer Causes Control. 2014, 25, 541–552. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Recommendations and Public Health and Policy Implications. Available online: http//dietandcancerreport.org (accessed on 23 April 2019).
- Center for Disease Control and Prevention (CDC). Healthy Weight: Assessing Your Weight. Available online: https://www.cdc.gov/healthyweight/assessing/index.html (accessed on 18 October 2011).
- National Heart, Lung, and Blood Institute. Assessing Your Weight and Health Risk. Available online: https://www.nhlbi.nih.gov/health/educational/lose_wt/risk.htm (accessed on 26 April 2019).
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Figure D-1; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. NOVA. The start shines bright. World Nutr. 2016, 7, 28–38. Available online: http://archive.wphna.org/wp-content/uploads/2016/01/WN-2016-7-1-3-28-38-Monteiro-Cannon-Levy-et-al-NOVA.pdf (accessed on 19 November 2018).
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- World Health Organization (WHO). Factsheet: Physical Activity and Adults. Available online: https://www.who.int/dietphysicalactivity/factsheet_adults/en/ (accessed on 4 January 2017).
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Figure D-2; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Martinez Steele, E.; Baraldi, L.G.; Louzada, M.L.; Moubarac, J.C.; Mozaffarian, D.; Monteiro, C.A. Ultra-processed foods and added sugars in the US diet: Evidence from a nationally representative cross-sectional study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [PubMed]
- Martinez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; De Castro, I.R.; Cannon, G. Increasing consumption of ultra-processed foods and likely impact on human health: Evidence from Brazil. Public Health Nutr. 2011, 14, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Moubarac, J.C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of ultra-processed foods predicts diet quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Alcoholic Drinks and the Risk of Cancer. Available online: http//dietandcancerreport.org (accessed on 23 April 2019).
- World Health Organization (WHO). Session 2—The physiological basis of breastfeeding. In Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals; World Health Organization: Geneva, Switzerland, 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK148970/d (accessed on 23 April 2019).
- Moore, S.C.; Lee, I.M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; Berrington De Gonzalez, A.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]


{kind=link}
| Recommendations | Details | Goals |
|---|---|---|
| Keep your weight within the healthy range and avoid weight gain in adult life |
|
| Be physically active as part of everyday life and life—walk more and sit less |
|
| Make wholegrains, vegetables, fruit, and pulses (legumes) such as beans and lentils a major part of your usual diet |
|
| Limiting these foods helps control calorie intake and maintain a healthy weight | Limit consumption of processed foods high in fat, starches or sugars—including “fast foods”, many pre-pared dishes, snacks, bakery foods and desserts; and confectionery (candy) 2 |
| Eat no more than moderate amounts of red meat, such as beef, pork, and lamb. Eat little, if any, processed meat. | If you eat red meat, limit consumption to no more than about three portions per week. Three portions are equivalent to about 350 to 500 g (about 12 to 18 oz) cooked weight of red meat. Consume very little, if any, processed meat. 2 |
| Drink mostly water and unsweetened drinks | Do not consume sugar-sweetened drinks 2 |
| For cancer prevention, it’s best not to drink alcohol | For cancer prevention, it’s best not to drink alcohol 2 |
| Aim to meet nutritional needs through diet alone | High-dose dietary supplements are not recommended for cancer prevention—aim to meet nutritional needs through diet alone |
| Breastfeeding is good for both mother and baby | This Recommendation aligns with the advice of the WHO, which recommends infants are exclusively breastfed for 6 months, and then up to 2 years of age or beyond alongside appropriate complementary foods 2 |
| Check with your health professional what is right for you |
|
| 2018 WCRF/AICR Recommendations | Operationalization of Recommendations | Points |
|---|---|---|
| BMI (kg/m2):2 | |
| 18.5–24.9 | 0.5 | |
| 25–29.9 | 0.25 | |
| <18.5 or ≥30 | 0 | |
| Waist circumference (cm (in)):2,3 | ||
| Men: <94 (<37) Women: <80 (<31.5) | 0.5 | |
| Men: 94–<102 (37–<40) Women: 80–<88 (31.5–<35) | 0.25 | |
| Men: ≥102 (≥40) Women: ≥88 (≥35) | 0 | |
| Total moderate-vigorous physical activity (min/wk):4 | |
| ≥150 | 1 | |
| 75–<150 | 0.5 | |
| <75 | 0 | |
| Fruits and vegetables (g/day):5 | |
| ≥400 | 0.5 | |
| 200–<400 | 0.25 | |
| <200 | 0 | |
| Total fiber (g/day):5 | ||
| ≥30 | 0.5 | |
| 15–<30 | 0.25 | |
| <15 | 0 | |
| Percent of total kcal from ultra-processed foods (aUPFs):6 | |
| Tertile 1 | 1 | |
| Tertile 2 | 0.5 | |
| Tertile 3 | 0 | |
| Total red meat (g/wk) and processed meat (g/wk): | |
| Red meat <500 and processed meat <21 | 1 | |
| Red meat <500 and processed meat 21–<100 | 0.5 | |
| Red meat >500 or processed meat ≥100 | 0 | |
| Total sugar-sweetened drinks (g/day): | |
| 0 | 1 | |
| >0–≤250 | 0.5 | |
| >250 | 0 | |
| Total ethanol (g/day): | |
| 0 | 1 | |
| >0–≤28 (2 drinks) males and ≤14 (1 drink) females | 0.5 | |
| >28 (2 drinks) males and >14 (1 drink) females | 0 | |
| Exclusively breastfed over lifetime for a total of: | |
| 6+ months | 1 | |
| >0–<6 months | 0.5 | |
| Never | 0 | |
| Total Score Range | 0–7 (or 0–8) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. https://doi.org/10.3390/nu11071572
Shams-White MM, Brockton NT, Mitrou P, Romaguera D, Brown S, Bender A, Kahle LL, Reedy J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients. 2019; 11(7):1572. https://doi.org/10.3390/nu11071572
Chicago/Turabian StyleShams-White, Marissa M., Nigel T. Brockton, Panagiota Mitrou, Dora Romaguera, Susannah Brown, Alice Bender, Lisa L. Kahle, and Jill Reedy. 2019. "Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System" Nutrients 11, no. 7: 1572. https://doi.org/10.3390/nu11071572