Assessing the Lifetime Cost-Effectiveness of Low-Protein Infant Formula as Early Obesity Prevention Strategy: The CHOP Randomized Trial


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Methods
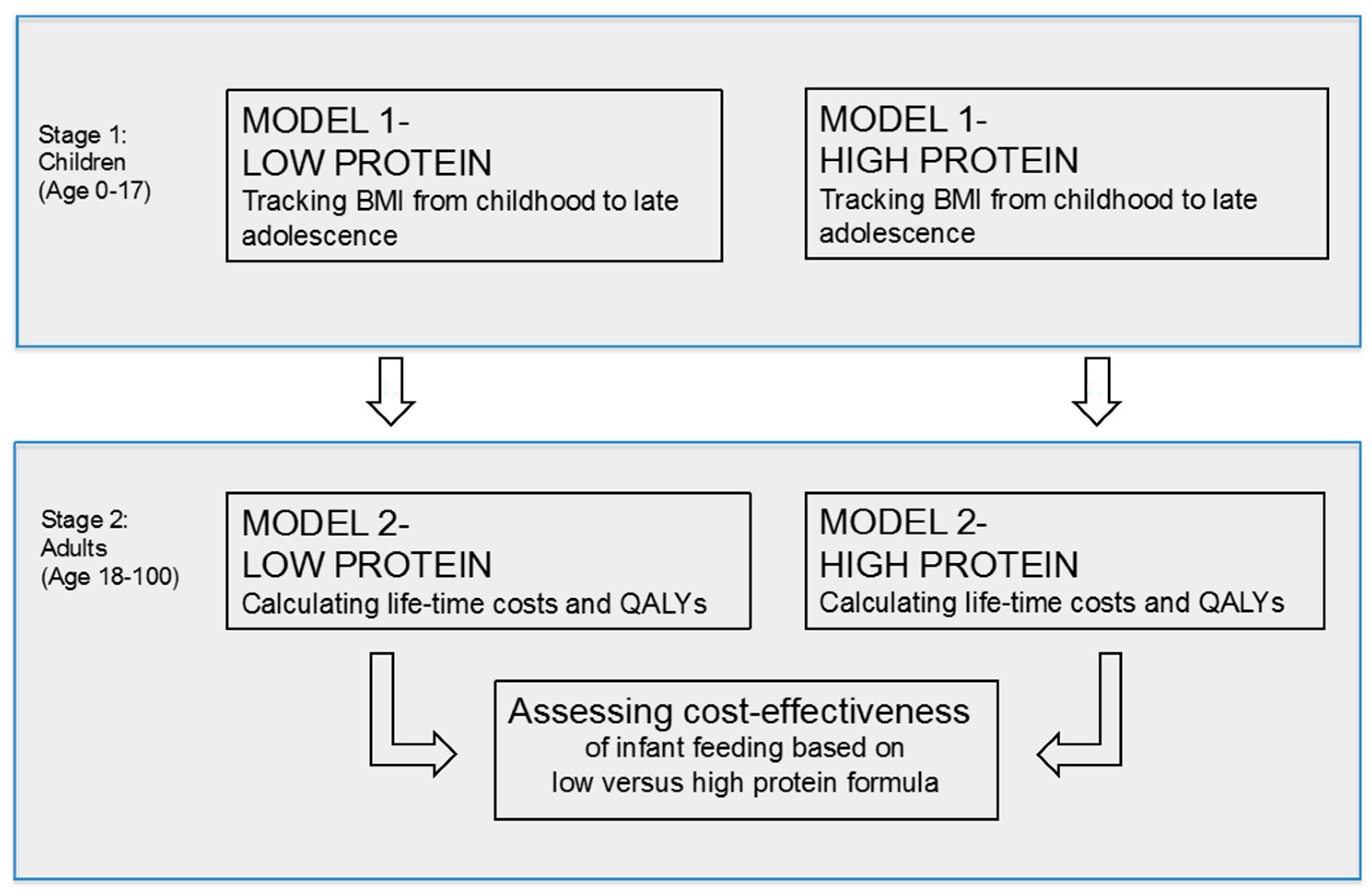
2.2. Model Structure
2.3. Model Parameters
2.3.1. State Transition Probabilities between BMI States
2.3.2. Risk of Mortality
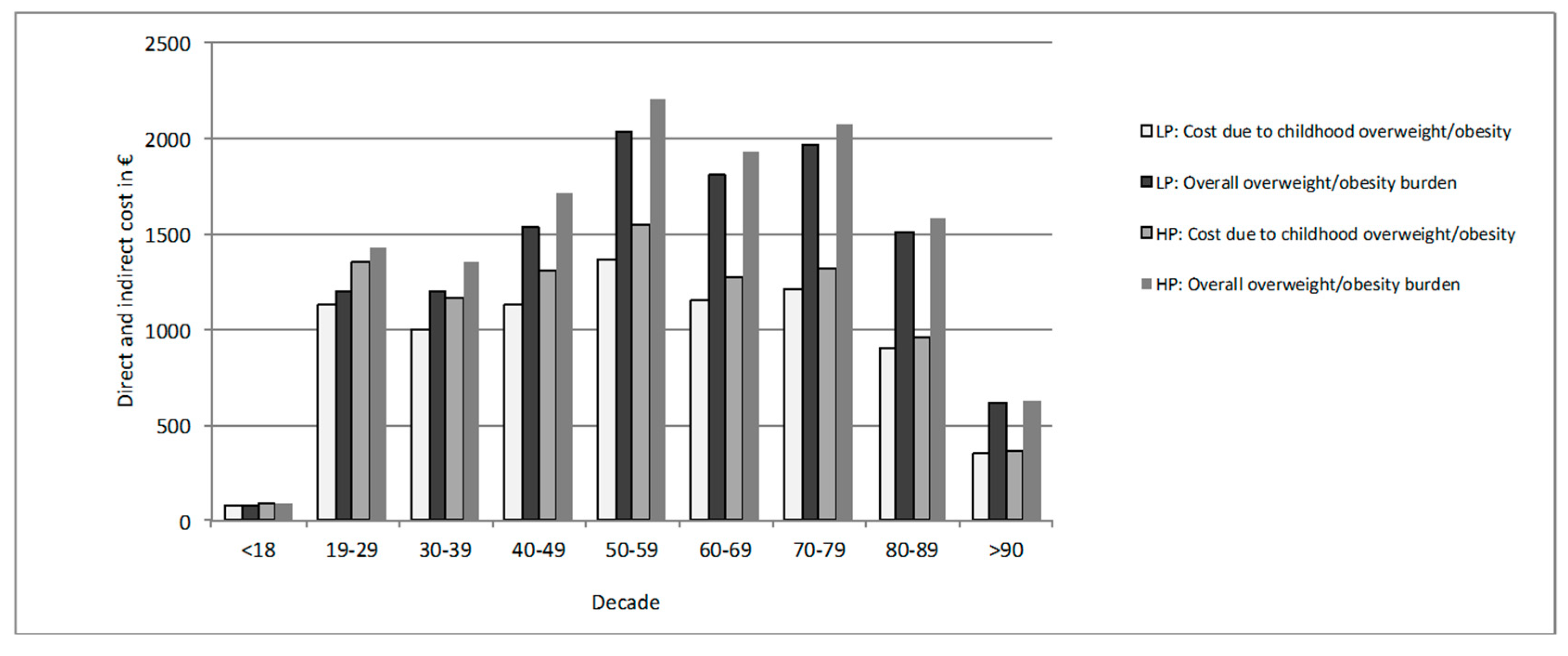
2.3.3. Intervention Costs and Costs Associated with Overweight and Obesity
2.3.4. Quality of Life
2.3.5. Sensitivity and Scenario Analyses
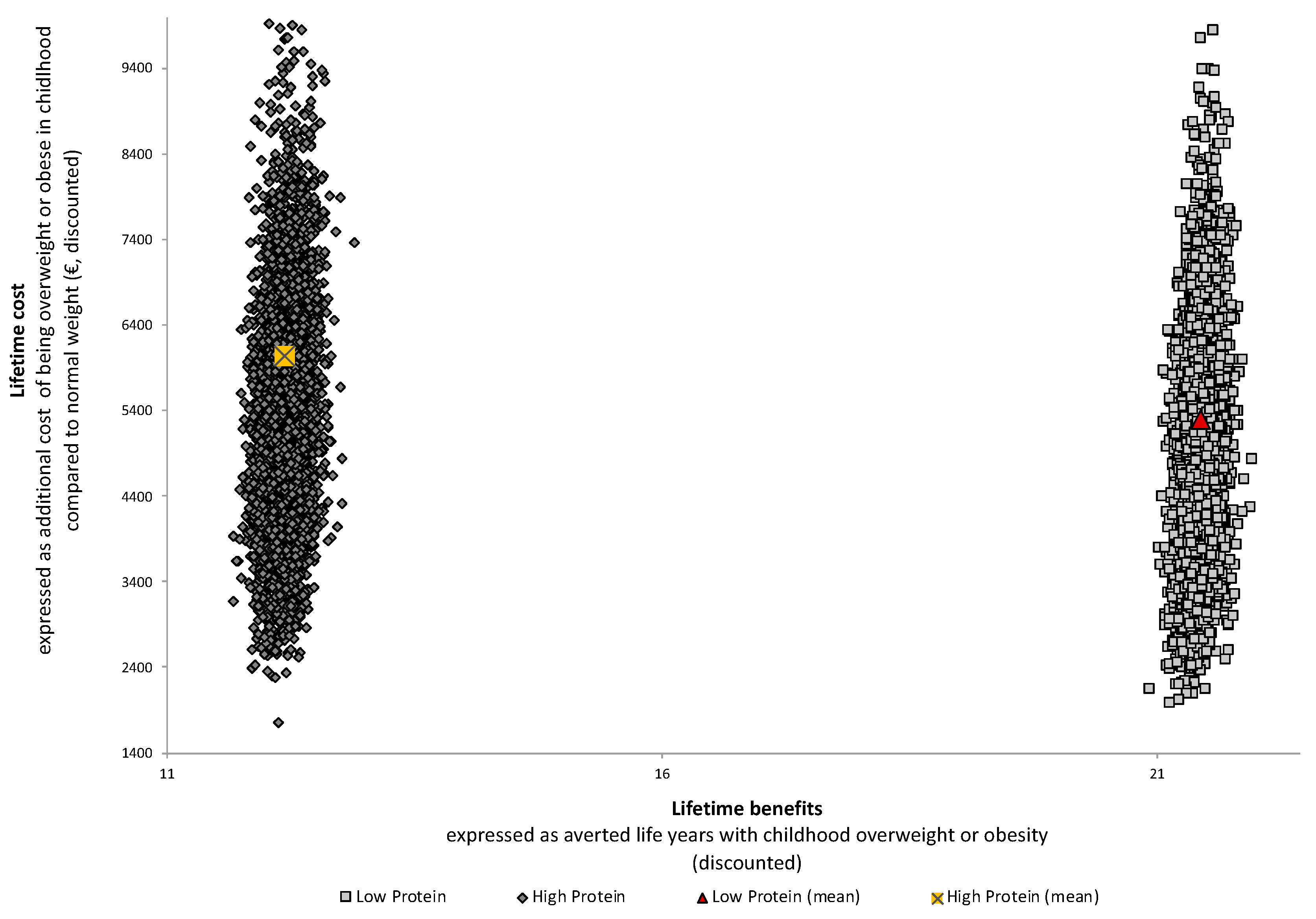
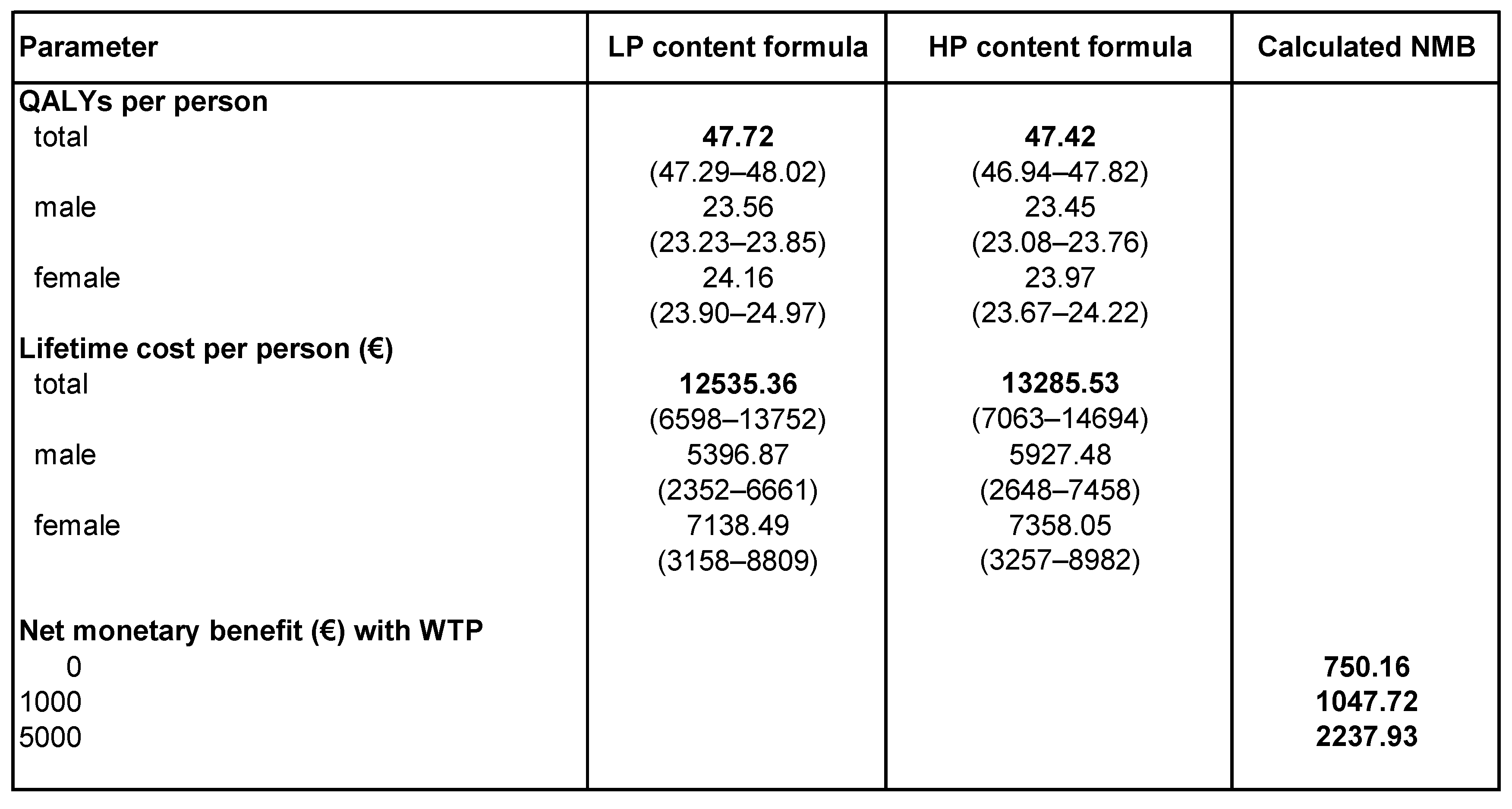
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; van Mechelen, W.; Chinapaw, M.J.M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, D.; Ali, S.; Lehnert, T.; Konnopka, A.; Riedel-Heller, S.; Koenig, H.H. Modelling the lifetime cost of child obesity in Germany: Results of a Markov Model. Pediatr. Obes. 2015, 10, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, D.; Ali, S.; De Bock, F. Lifetime indirect cost of childhood overweight and obesity: A decision analytic model. Obes. Silver Spring 2016, 24, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.M. Estimating the Lifecycle Costs Associated with Childhood Obesity in Evaluating the Impacts of School Nutrition and Physical Activity Policies on Child Health. Ph.D. Thesis, Pardee RAND Graduate School, Santa Monica, CA, USA, 2010. [Google Scholar]
- Hesketh, K.D.; Campbell, K.J. Interventions to prevent obesity in 0–5 year olds: An updated systematic review of the literature. Obes. Silver Spring 2010, 18, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.D. Long-Term Effects of Nutritional Supplementation in Childhood. J. Nutr. 2018, 148, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Patro-Gołąb, B.; Zalewski, B.M.; Kouwenhoven, S.M.P.; Karaś, J.; Koletzko, B.; van Goudoever, J.B.; Szajewska, H. Protein Concentration in Milk Formula, Growth, and Later Risk of Obesity: A Systematic Review. J. Nutr. 2016, 146, 551–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, M.; Grote, V.; Closa-Monasterolo, R.; Escribano, J.; Langhendries, J.P.; Dain, E.; Giovannini, M.; Verduci, E.; Gruszfeld, D.; Socha, P.; et al. Lower protein content in infant formula reduces BMI and obesity risk at school age: Follow-up of a randomized trial. Am. J. Clin. Nutr. 2014, 99, 1041–1051. [Google Scholar] [CrossRef]
- Doering, N.; Mayer, S.; Rasmussen, F.; Sonntag, D. Economic Evaluation of Obesity Prevention in Early Childhood: Methods, Limitations and Recommendations. Int. J. Environ. Res. Public Health 2016, 13, 911. [Google Scholar] [CrossRef]
- Hollinghurst, S.; Hunt, L.P.; Banks, J.; Sharp, D.J.; Shield, J.P. Cost and effectiveness of treatment options for childhood obesity. Pediatr. Obes. 2013, 9, 26–34. [Google Scholar] [CrossRef]
- Briggs, A.; Sculpher, M.; Claxton, K. Decision Modelling for Health Economic Evaluation; Oxford University Press: Oxford, UK, 2006; ISBN 9780198526629. [Google Scholar]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben (Percentiles for the Body-Mass-Index in childhood and adolescence using German samples). Mon. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.K.; Homan, S.M. Determining transition probabilities: Confusion and suggestions. Med. Decis. Mak. 1994, 14, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Bärbel-Maria, K.; Angelika Schaffrath, R. Die Verbreitung von Übergewicht und Adipositas bei Kinden und Jugendlichen in Deutschland. Ergebnisse des bundesweiten Kinder- und Jugendgesundheitssurveys (KiGGS) (The prevalence of overweight and obese children and adolescents living in Germany. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS)). Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 736–743. [Google Scholar] [CrossRef]
- Statistisches Bundesamt. Mikrozensus-Fragen zur Gesundheit. Körpermaße der Bevölkerung (Microcensus: Anthroprometric measurements); Statistisches Bundesamt: Wiesbaden, Germany, 2011.
- Statistisches Bundesamt. Periodensterbetafeln für Deutschland. Allgemeine Sterbetafeln, Abgekürzte Sterbetafeln und Sterbetafeln (Life Tables–Germany); Statistisches Bundesamt: Wiesbaden, Germany, 2012.
- Pischon, T.; Boeing, H.; Hoffmann, K.; Bergmann, M.; Schulze, M.B.; Overvad, K.; van der Schouw, Y.T.; Spencer, E.; Moons, K.G.; Tjonneland, A.; et al. General and abdominal adiposity and risk of death in Europe. N. Engl. J. Med. 2008, 359, 2105–2120. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, D.; Ali, S.; de Bock, F. Langfristige gesellschaftliche Kosten von heutigem Übergewicht und Adipositas im Jugendalter und Präventionspotentiale für Deutschland (Long-term social costs of todays overweight and obesity in adolescence and prevention potential in Germany). Adipositas 2016, 10. [Google Scholar] [CrossRef]
- König, H.H.; Bernert, S.; Angermeyer, M.C. Gesundheitszustand der deutschen Bevölkerung: Ergebnisse einer repräsentativen Befragung mit dem EuroQol-Instrument (The health status of the German population: results of the EuroQoL instrument). Gesundheitswesen 2005, 67. [Google Scholar] [CrossRef] [PubMed]
- Dolan, P. Modeling valuations for EuroQol health states. Med. Care 1997, 35, 1095–1108. [Google Scholar] [CrossRef] [PubMed]
- Clayton, H.B.; Li, R.; Perrine, C.G.; Scanlon, K.S. Prevalence and Reasons for Introducing Infants Early to Solid Foods: Variations by Milk Feeding Type. Pediatrics 2013, 131, e1108–e1114. [Google Scholar] [CrossRef] [Green Version]
- Weissenborn, A.; Abou-Dakn, M.; Bergmann, R.; Both, D.; Gresens, R.; Hahn, B.; Hecker, A.; Koletzko, B.; Krawinkel, M.; Kroll, D.; et al. Stillhäufigkeit und Stilldauer in Deutschland—Eine systematische Übersicht [Breastfeeding Rates and Duration in Germany—A Systematic Review]. Gesundheitswesen 2015, 78, 695–707. [Google Scholar] [CrossRef]
- Sonntag, D.; Schneider, S.; Mdege, N.; Ali, S.; Schmidt, B. Beyond Food Promotion: A Systematic Review on the Influence of the Food Industry on Obesity-Related Dietary Behaviour among Children. Nutrients 2015, 7, 8565–8576. [Google Scholar] [CrossRef] [Green Version]
- Mantilla Herrera, A.M.; Crino, M.; Erskine, H.E.; Sacks, G.; Ananthapavan, J.; Mhurchu, C.N.; Lee, Y.Y. Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia. Nutrients 2018, 10, 614. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; Franca, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- European Commission. Commission Directive 2006/141/EC of Infant Formula and Follow-on Formulae and Amendments to Directive 1999/21/EC; European Commission: Brussels, Belgium, 2006; pp. L401–L402. [Google Scholar]
- Barrett, J.L.; Gortmaker, S.L.; Long, M.W.; Ward, Z.J.; Resch, S.C.; Moodie, M.L.; Carter, R.; Sacks, G.; Swinburn, B.A.; Wang, Y.C.; et al. Cost Effectiveness of an Elementary School Active Physical Education Policy. Am. J. Prev. Med. 2015, 49, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.; Lung, T.; Wen, L.M.; Baur, L.; Rissel, C.; Howard, K. Economic evaluation of “healthy beginnings” an early childhood intervention to prevent obesity. Obes. Silver Spring 2014, 22, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Frick, K.D. A simulation of affordability and effectiveness of childhood obesity interventions. Acad. Pediatr. 2011, 11, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.R.; Kenney, E.L.; Giles, C.M.; Long, M.W.; Ward, Z.J.; Resch, S.C.; Moodie, M.L.; Carter, R.C.; Wang, Y.C.; Sacks, G.; et al. Modeling the Cost Effectiveness of Child Care Policy Changes in the U.S. Am. J. Prev. Med. 2015, 49, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Butte, N.F.; Taveras, E.M.; Lundeen, E.A.; Blanck, H.M.; Goodman, A.B.; Ogden, C.L. BMI z-scores are a poor indicator of adiposity among2-to 19-year-olds with very high BMIs, NHANES 1999-2000 to 2013-14. Obes. Silver Spring 2017, 25, 739–746. [Google Scholar] [CrossRef] [PubMed]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sonntag, D.; De Bock, F.; Totzauer, M.; Koletzko, B. Assessing the Lifetime Cost-Effectiveness of Low-Protein Infant Formula as Early Obesity Prevention Strategy: The CHOP Randomized Trial. Nutrients 2019, 11, 1653. https://doi.org/10.3390/nu11071653
Sonntag D, De Bock F, Totzauer M, Koletzko B. Assessing the Lifetime Cost-Effectiveness of Low-Protein Infant Formula as Early Obesity Prevention Strategy: The CHOP Randomized Trial. Nutrients. 2019; 11(7):1653. https://doi.org/10.3390/nu11071653
Chicago/Turabian StyleSonntag, Diana, Freia De Bock, Martina Totzauer, and Berthold Koletzko. 2019. "Assessing the Lifetime Cost-Effectiveness of Low-Protein Infant Formula as Early Obesity Prevention Strategy: The CHOP Randomized Trial" Nutrients 11, no. 7: 1653. https://doi.org/10.3390/nu11071653
APA StyleSonntag, D., De Bock, F., Totzauer, M., & Koletzko, B. (2019). Assessing the Lifetime Cost-Effectiveness of Low-Protein Infant Formula as Early Obesity Prevention Strategy: The CHOP Randomized Trial. Nutrients, 11(7), 1653. https://doi.org/10.3390/nu11071653