A Dietary Intervention of Bioactive Enriched Foods Aimed at Adults at Risk of Metabolic Syndrome: Protocol and Results from PATHWAY-27 Pilot Study

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Participants
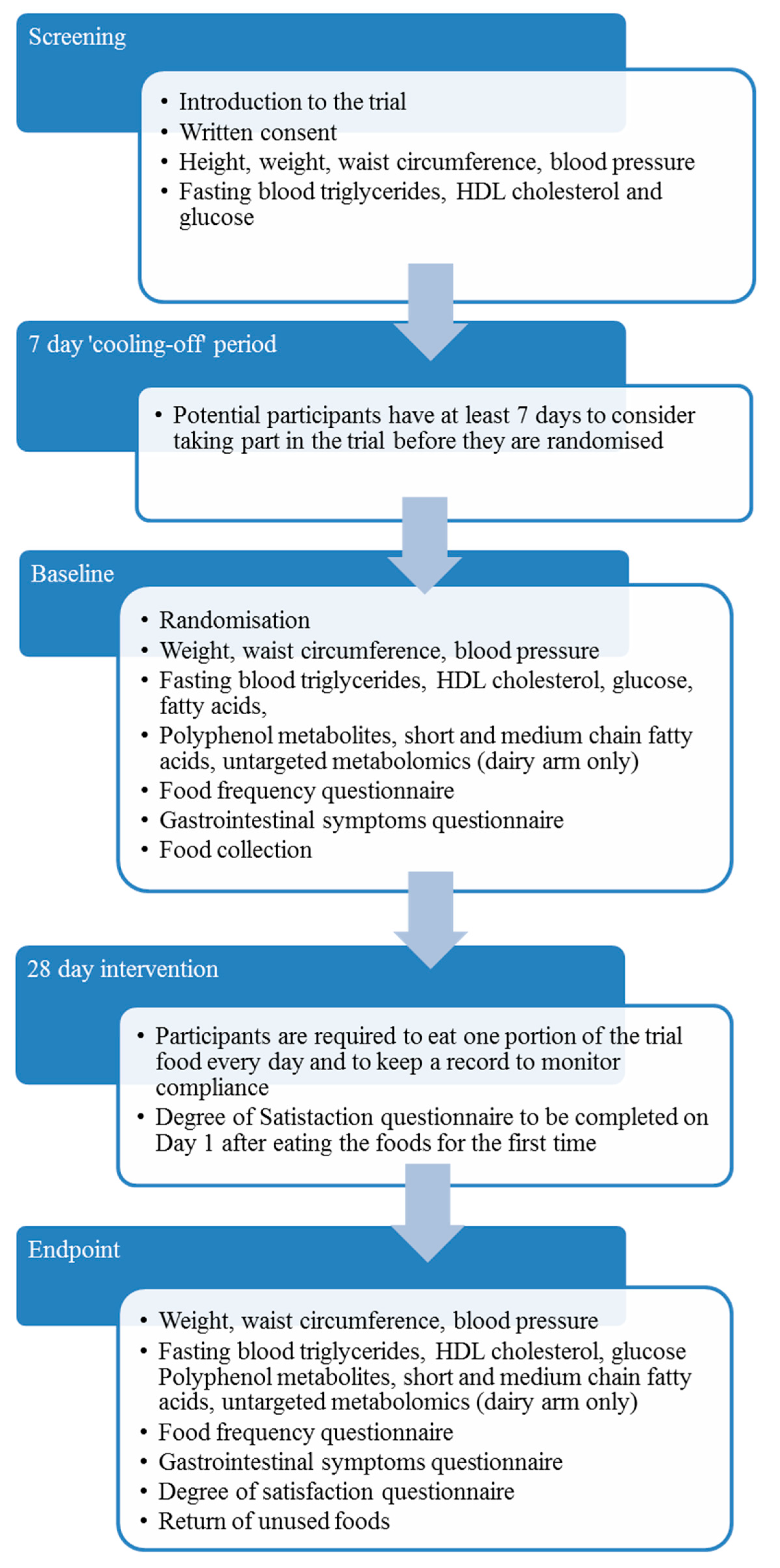
2.3. Pilot Trial Design
2.4. Test Foods
2.5. Randomization
2.6. Blinding
2.7. Blood Pressure and Anthropometric Measurements
2.8. Blood Collection, Processing and Analysis
2.9. Dietary Assessment
2.10. Compliance
2.11. Clinical Data Collection and Management
2.12. Serum Fatty Acid Composition
2.13. Quantification of Short and Medium Chain Fatty Acids, and Polyphenol Metabolites in Serum
2.14. Untargeted Metabolomics Analysis of Serum
2.15. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Acceptance of BEF and Compliance
3.3. Primary Outcomes
3.4. Secondary Outcomes
3.5. Serum Fatty Acid Composition and Quantification of SCFAs, MCFAs and Polyphenol Metabolites
3.6. Adverse and Serious Adverse Effects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Statement
References
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; american heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsen, B.; Lahti, K.; Nissen, M.; Taskinen, M.R.; Groop, L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.P.; Williams, K.; Gonzalez-Villalpando, C.; Hunt, K.J.; Haffner, S.M. Does the metabolic syndrome improve identification of individuals at risk of type 2 diabetes and/or cardiovascular disease? Diabetes Care 2004, 27, 2676–2681. [Google Scholar] [CrossRef] [PubMed]
- Plumb, J.; Pigat, S.; Bompola, F.; Cushen, M.; Pinchen, H.; Nørby, E.; Astley, S.; Lyons, J.; Kiely, M.; Finglas, P. Ebasis (bioactive substances in food information systems) and bioactive intakes: Major updates of the bioactive compound composition and beneficial bioeffects database and the development of a probabilistic model to assess intakes in europe. Nutrients 2017, 9, 320. [Google Scholar] [CrossRef] [PubMed]
- Grimsgaard, S.; Bonaa, K.H.; Hansen, J.B.; Nordoy, A. Highly purified eicosapentaenoic acid and docosahexaenoic acid in humans have similar triacylglycerol-lowering effects but divergent effects on serum fatty acids. Am. J. Clin. Nutr. 1997, 66, 649–659. [Google Scholar] [CrossRef]
- Qin, Y.; Xia, M.; Ma, J.; Hao, Y.; Liu, J.; Mou, H.; Cao, L.; Ling, W. Anthocyanin supplementation improves serum ldl-and hdl-cholesterol concentrations associated with the inhibition of cholesteryl ester transfer protein in dyslipidemic subjects. Am. J. Clin. Nutr. 2009, 90, 485–492. [Google Scholar] [CrossRef]
- Phongnarisorn, B.; Orfila, C.; Holmes, M.; Marshall, J.L. Enrichment of biscuits with matcha green tea powder: Its impact on consumer acceptability and acute metabolic response. Foods 2018, 7, 17. [Google Scholar] [CrossRef]
- Lenssen, K.G.M.; Bast, A.; de Boer, A. Clarifying the health claim assessment procedure of efsa will benefit functional food innovation. J. Funct. Foods 2018, 47, 386–396. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to docosahexaenoic acid (DHA) and maintenance of normal (fasting) blood concentrations of triglycerides (ID 533, 691, 3150), protection of blood lipids from oxidative damage (ID 630), contribution to the maintenance or achievement of a normal body weight (ID 629), brain, eye and nerve development (ID 627, 689, 704, 742, 3148, 3151), maintenance of normal brain function (ID 565, 626, 631, 689, 690, 704, 742, 3148, 3151), maintenance of normal vision (ID 627, 632, 743, 3149) and maintenance of normal spermatozoa motility (ID 628) pursuant to article 13(1) of regulation (ec) no 1924/2006. EFSA J. 2010, 8, 1734. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to beta glucans and maintenance of normal blood cholesterol concentrations (ID 754, 755, 757, 801, 1465, 2934) and maintenance or achievement of a normal body weight (ID 820, 823) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2009, 7, 1254. [Google Scholar]
- Brandenburger, S.; Birringer, M. European health claims for small and medium-sized companies-utopian dream or future reality? Funct. Foods Health D 2015, 5, 44–56. [Google Scholar]
- Brown, L.; Caligiuri, S.P.B.; Brown, D.; Pierce, G.N. Clinical trials using functional foods provide unique challenges. J. Funct. Foods 2018, 45, 233–238. [Google Scholar] [CrossRef]
- Eldridge, S.; Bond, C.; Campbell, M.; Hopewell, S.; Thabane, L.; Lancaster, G.; Coleman, C. Defining feasibility and pilot studies in preparation for randomised controlled trials: Using consensus methods and validation to develop a conceptual framework. Trials 2015, 16, O87. [Google Scholar] [CrossRef]
- Marsaux, C.; Storcksdieck, S.; Putz, P.; Orfila, C.; Sutulic, S.; Kertesz, Z.; Grabler, C.; Ricciardiello, L.; Garelli, S.; Tomás, L.; et al. Scientific Guidelines for the Substantiation of Health Benefits from a (Bioactive-Enriched) Food; 2017; ISBN 978-88-943424-1-3. Available online: https://www.pathway27.eu/download (accessed on 5 August 2019).
- Bordoni, A.; Boesch, C.; Malpuech-Brugère, C.; Orfila, C.; Tomás-Cobos, L. The role of bioactives in energy metabolism and metabolic syndrome. Proc. Nutr. Soc. 2019, 10, 1–11. [Google Scholar] [CrossRef]
- Sutulic, S.; Holmes, M.J.; Garelli, S.; Herrmann, M.; Seifert, S.; Amat, J.; Blot, A.; Marcato, E.; Malpuech-Brugère, C.; Bub, A.; et al. Dietary intake of food bioactives in a cohort of european adults with metabolic syndrome enrolled in the pathway-27 trial. Proc. Nutr. Soc. 2018, 77, E133. [Google Scholar] [CrossRef]
- Sutulic, S.; Amat, J.; Blot, A.; Nemeth, I.; Kertész, Z.; Marshall, L.; Seifert, S.; Ricciardiello, L.; Malpuech-Brugère, C.; Bordoni, A.; et al. Protocol for pilot studies: effectiveness of bioactive enriched foods (bef) on markers of metabolic syndrome. White Rose Res. Online 2019. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J. 2010, 8, 1461. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of a health claim related to oat beta glucan and lowering blood cholesterol and reduced risk of (coronary) heart disease pursuant to article 14 of Regulation (EC) No 1924/2006. EFSA J. 2010, 8, 1885. [Google Scholar]
- WHO. Waist Circumference and Waist-Hip Ratio Report of a WHO Expert Consultation, Geneva, 8–11 December 2008; WHO: Geneva, Switzerland, 2011; ISBN 978-92-4-150149-1. Available online: https://apps.Who.Int/ (accessed on 5 August 2019).
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar]
- Stoffel, W.; Chu, F.; Ahrens, E.H. Analysis of long-chain fatty acids by gas-liquid chromatography. Anal. Chem. 1959, 31, 307–308. [Google Scholar] [CrossRef]
- Ghini, V.; Di Nunzio, M.; Tenori, L.; Valli, V.; Danesi, F.; Capozzi, F.; Luchinat, C.; Bordoni, A. Evidence of a DHA signature in the lipidome and metabolome of human hepatocytes. Int. J. Mol. Sci. 2017, 18, 359. [Google Scholar] [CrossRef] [PubMed]
- Lotti, C.; Rubert, J.; Fava, F.; Tuohy, K.; Mattivi, F.; Vrhovsek, U. Development of a fast and cost-effective gas chromatography-mass spectrometry method for the quantification of short-chain and medium-chain fatty acids in human biofluids. Anal. Bioanal. Chem. 2017, 409, 5555–5567. [Google Scholar] [CrossRef] [PubMed]
- Gasperotti, M.; Masuero, D.; Guella, G.; Mattivi, F.; Vrhovsek, U. Development of a targeted method for twenty-three metabolites related to polyphenol gut microbial metabolism in biological samples, using spe and uhplc-esi-ms/ms. Talanta 2014, 128, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Ancillotti, C.; Ulaszewska, M.; Mattivi, F.; Del Bubba, M. Untargeted metabolomics analytical strategy based on liquid chromatography/electrospray ionization linear ion trap quadrupole/orbitrap mass spectrometry for discovering new polyphenol metabolites in human biofluids after acute ingestion of vaccinium myrtillus berry supplement. J. Am. Soc. Mass Spectrom. 2019, 30, 381–402. [Google Scholar] [PubMed]
- Watters, C.A.; Edmonds, C.M.; Rosner, L.S.; Sloss, K.P. A cost analysis of epa and dha in fish, supplements, and foods. Nutr. Food Sci. 2012, 2, 159–163. [Google Scholar] [CrossRef]
- Carrero, J.J.; Baró, L.; Fonollá, J.; González-Santiago, M.; Martínez-Férez, A.; Castillo, R.; Jiménez, J.; Boza, J.J.; López-Huertas, E. Cardiovascular effects of milk enriched with ω-3 polyunsaturated fatty acids, oleic acid, folic acid, and vitamins e and b6 in volunteers with mild hyperlipidemia. Nutrition 2004, 20, 521–527. [Google Scholar] [CrossRef]
- Dawczynski, C.; Martin, L.; Wagner, A.; Jahreis, G. N-3 lc-pufa-enriched dairy products are able to reduce cardiovascular risk factors: A double-blind, cross-over study. Clin. Nutr. 2010, 29, 592–599. [Google Scholar] [CrossRef]
- Goncalves, A.; Margier, M.; Tagliaferri, C.; Lebecque, P.; George, S.; Wittrant, Y.; Coxam, V.; Amiot, M.J.; Reboul, E. Pinoresinol of olive oil decreases vitamin d intestinal absorption. Food Chem. 2016, 206, 234–238. [Google Scholar] [CrossRef]
- Reboul, E.; Thap, S.; Perrot, E.; Amiot, M.J.; Lairon, D.; Borel, P. Effect of the main dietary antioxidants (carotenoids, gamma-tocopherol, polyphenols, and vitamin c) on alpha-tocopherol absorption. Eur. J. Clin. Nutr. 2007, 61, 1167–1173. [Google Scholar] [CrossRef]
- Chen, T.Y.; Ferruzzi, M.G.; Wu, Q.L.; Simon, J.E.; Talcott, S.T.; Wang, J.; Ho, L.; Todd, G.; Cooper, B.; Pasinetti, G.M.; et al. Influence of diabetes on plasma pharmacokinetics and brain bioavailability of grape polyphenols and their phase ii metabolites in the zucker diabetic fatty rat. Mol. Nutr. Food Res. 2017, 61, 1700111. [Google Scholar] [CrossRef] [PubMed]
- Karakaya, S.; Simsek, S.; Eker, A.T.; Pineda-Vadillo, C.; Dupont, D.; Perez, B.; Viadel, B.; Sanz-Buenhombre, M.; Rodriguez, A.G.; Kertesz, Z.; et al. Stability and bioaccessibility of anthocyanins in bakery products enriched with anthocyanins. Food Funct. 2016, 7, 3488–3496. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Vadillo, C.; Nau, F.; Dubiard, C.G.; Cheynier, V.; Meudec, E.; Sanz-Buenhombre, M.; Guadarrama, A.; Tóth, T.; Csavajda, É.; Hingyi, H.; et al. In vitro digestion of dairy and egg products enriched with grape extracts: Effect of the food matrix on polyphenol bioaccessibility and antioxidant activity. Food Res. Int. 2016, 88, 284–292. [Google Scholar] [CrossRef]
- Calder, P.C. Mechanisms of action of (n-3) fatty acids. J. Nutr. 2012, 142, 592S–599S. [Google Scholar] [CrossRef] [PubMed]
- Bjork, C.; Wilhelm, U.; Mandrup, S.; Larsen, B.D.; Bordoni, A.; Heden, P.; Ryden, M.; Arner, P.; Laurencikiene, J. Effects of selected bioactive food compounds on human white adipocyte function. Nutr. Metab. 2016, 13, 4. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Wang, D.; Yang, Y.; Xia, M.; Li, D.; Li, G.; Zhu, Y.; Xiao, Y.; Ling, W. Cyanidin-3-o-beta-glucoside improves obesity and triglyceride metabolism in kk-ay mice by regulating lipoprotein lipase activity. J. Sci. Food Agric. 2011, 91, 1006–1013. [Google Scholar] [CrossRef]
- Surampudi, P.; Enkhmaa, B.; Anuurad, E.; Berglund, L. Lipid lowering with soluble dietary fiber. Curr. Atheroscler. Rep. 2016, 18, 75. [Google Scholar] [CrossRef]
- Gunness, P.; Michiels, J.; Vanhaecke, L.; De Smet, S.; Kravchuk, O.; Van de Meene, A.; Gidley, M.J. Reduction in circulating bile acid and restricted diffusion across the intestinal epithelium are associated with a decrease in blood cholesterol in the presence of oat beta-glucan. FASEB J. 2016, 30, 4227–4238. [Google Scholar] [CrossRef]
- Jayachandran, M.; Chen, J.; Chung, S.S.M.; Xu, B. A critical review on the impacts of beta-glucans on gut microbiota and human health. J. Nutr. Biochem. 2018, 61, 101–110. [Google Scholar] [CrossRef]
- Tomas-Barberan, F.A.; Selma, M.V.; Espin, J.C. Interactions of gut microbiota with dietary polyphenols and consequences to human health. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 471–476. [Google Scholar] [CrossRef]
- Garcia-Villalba, R.; Vissenaekens, H.; Pitart, J.; Romo-Vaquero, M.; Espin, J.C.; Grootaert, C.; Selma, M.V.; Raes, K.; Smagghe, G.; Possemiers, S.; et al. Gastrointestinal simulation model twin-shime shows differences between human urolithin-metabotypes in gut microbiota composition, pomegranate polyphenol metabolism, and transport along the intestinal tract. J. Agric. Food Chem. 2017, 65, 5480–5493. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Bioactive | Treatment Arm | ||||
|---|---|---|---|---|---|
| DHA | OBG | AC | DHA + OBG | DHA + AC | |
| DHA (mg) | 250 | - | - | 250 | 250 |
| OBG (mg) | - | 3000 | - | 3000 | - |
| AC (mg) | - | - | 320 | - | 320 |
| Bakery | Dairy | Egg | |
|---|---|---|---|
| Energy (kJ) | 828 (657–966) | 904 (653–929) | 854 (711–983) |
| Energy (kcal) | 198 (157–231) | 216 (156–222) | 204 (170–235) |
| Protein (g) | 6.1 (4.1–6.2) | 13.9 (9.6–16.3) | 5.6 (4.3–6.5) |
| Carbohydrate (g) | 35.2 (22.2–36.9) | 26.7 (25.2–28.9) | 17.7 (14.1–22.0) |
| of which sugars (g) | 9.3 (6.7–10.0) | 22.1 (20.0–22.7) | 1.9 (1.7–11.4) |
| Fat (g) | 7.6 (4.6–7.7) | 4.4 (1.8–4.6) | 13.1 (9.3–14.3) |
| of which SFA (g) | 1.6 (0.9–1.7) | 1.5 (1.0–1.6) | 2.2 (1.3–2.4) |
| Fibre (g) | 0.8 (0.7–5.2) | 0.8 (0.7–5.2) | 0.7 (0.7–4.5) |
| Sodium (mg) | 10.9 (4.0–13.5) | 135.3 (123.7–139.6) | 413.0 (397.7–617.7) |
| Matrix | ||||||
|---|---|---|---|---|---|---|
| Dairy | Egg | Bakery | ||||
| Gender | M | F | M | F | M | F |
| N | 38 | 28 | 14 | 21 | 22 | 44 |
| Age (years) | 61.6 (9.0) | 58.9 (7.8) | 45.5 (10.7) | 44.6 (14.2) | 51.8 (13.1) | 56.4 (12.6) |
| Weight (kg) | 91.2 (13.6) | 80.9 (12.9) | 99.3 (18.3) | 87.3 (22.0) | 91.4 (16.0) | 80.8 (12.4) |
| BMI (kg/m2) | 29.26 | 29.97 | 31.11 | 31.68 | 29.31 | 30.80 |
| Waist circumference (cm) | 105.3 (11.2) | 98.2 (10.5) | 110.1 (9.4) | 104.8 (16.0) | 101.6 (12.1) | 93.2 (8.3) |
| Fasting TG (mg/dL) | 187.0 (94.9) | 162.4 (53.3) | 155.6 (54.0) | 136.6 (84.5) | 167.7 (50.89) | 195.41 (122.26) |
| Fasting HDL-C (mg/dL) | 44.0 (10.0) | 53.5 (10.9) | 40.3 (6.7) | 55.2 (16.6) | 40.0 (11.63) | 48.1 (13.3) |
| Fasting Glucose (mg/dL) | 96.8 (10.2) | 91.6 (8.1) | 93.3 (14.4) | 91.1 (9.7) | 104.4 (16.3) | 97.6 (9.9) |
| Systolic BP (mmHg) | 144.1 (19.8) | 140.3 (16.2) | 134.7 (21.3) | 130.7 (17.0) | 139.4 (17.0) | 133.7 (11.2) |
| Diastolic BP (mmHg) | 91.9 (11.5) | 93.6 (10.8) | 79.5 (14.1) | 82.1 (11.4) | 86.9 (8.2) | 85.3 (9.8) |
| Bioactive | Germany (Dairy Arm) | UK (Egg Arm) | France (Bakery Arm) |
|---|---|---|---|
| DHA (mg/d) | 0.31 (0.24) | 0.34 (0.28) | 0.36 (0.50) |
| OBG (mg/d) | 290.5 (473.78) | 716.5 (1153.41) | 154.1 (387.83) |
| AC (mg/d) | 46.3 (39.39) | 102.2 (92.67) | 49.2 (74.49) |
| Attribute | Matrix | ||
|---|---|---|---|
| Dairy | Egg | Bakery | |
| Appearance | 6.80 | 5.84 | 5.37 |
| Odour | 6.86 | 5.72 | 5.79 |
| Taste | 6.98 | 5.65 | 5.18 |
| Texture | 6.80 | 5.42 | 4.22 |
| Overall acceptability | 7.03 | 5.88 | 4.75 |
| Compliance to trial (%) | 93.3 | 90.6 | 85.2 |
| TG (mg/dL) | HDL-C (mg/dL) | |||
|---|---|---|---|---|
| Matrix | Enrichment | N | Mean (SD) | Mean (SD) |
| Dairy | DHA | 14 | 10.36 (60.33) | −2.36 (7.96) |
| OBG | 12 | −31.00 (128.64) | −0.17 (8.36) | |
| AC | 15 | −7.60 (50.39) | 2.53 * (3.89) | |
| DHA + OBG | 13 | −41.69 * (50.77) | 1.08 (4.21) | |
| DHA + AC | 12 | −4.83 (49.76) | 0.17 (6.09) | |
| Egg | DHA | 7 | −6.34 (45.96) | 4.97 * (5.34) |
| OBG | 8 | 21.04 (89.28) | 0.46 (5.62) | |
| AC | 8 | −13.16 (28.65) | −0.46 (6.02) | |
| DHA + OBG | 6 | 0.00 (36.72) | −1.92 (5.33) | |
| DHA + AC | 6 | −11.83 (37.84) | 5.80 * (4.04) | |
| Bakery | DHA | 12 | −7.75 (51.34) | 2.83 (2.66) |
| OBG | 14 | −6.86 (49.96) | 1.00 (6.15) | |
| AC | 13 | 32.00 (115.00) | 4.82 (1.34) | |
| DHA + OBG | 13 | −27.54 (46.13) | 1.15 (5.65) | |
| DHA + AC | 14 | −36.64 (82.32) | 1.43 (4.52) | |
| Systolic BP (mmHg) | Diastolic BP (mmHg) | Fasting Glucose (units) | WC (cm) | |||
|---|---|---|---|---|---|---|
| Matrix | Enrichment | N | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) |
| Dairy | DHA | 14 | 0 (11) | −2 (7) | −0.9 (7.8) | −0.6 (1.7) |
| OBG | 12 | −9 (11) | −7 (12) | 1.3 (4.9) | 0.4 (1.6) | |
| AC | 15 | 2 (11) | 2 (7) | −2.2 (5.1) | −0.6 (2.2) | |
| DHA + OBG | 13 | −3 (12) | −4 (8) | 0.8 (3.0) | −1.3 (2.3) | |
| DHA + AC | 12 | −3 (16) | −1 (10) | 0.5 (6.9) | 1.1 (2.0) | |
| Egg | DHA | 7 | 3 (10) | 1 (7) | 4.5 (6.5) | −4.2 (9.0) |
| OBG | 8 | 0 (9) | 2 (10) | 0.0 (7.5) | −0.8 (7.1) | |
| AC | 8 | 6 (9) | 6 (2) | −4.2 (7.9) | −2.7 (4.6) | |
| DHA + OBG | 6 | −3 (11) | 0 (13) | −2.4 (4.1) | −1.8 (2.5) | |
| DHA + AC | 6 | −12 (10) | 5 (8) | −2.2 (15.1) | −3.6 (5.5) | |
| Bakery | DHA | 12 | 1 (9) | −5 (5) | −1.17 (5.18) | −0.83 (2.41) |
| OBG | 14 | −2 (10) | −2 (8) | −1.21 (3.31) | 0.43 (1.60) | |
| AC | 13 | 3 (14) | 2 (6) | 0.15 (6.62) | −0.36 (2.10) | |
| DHA + OBG | 13 | 0 (10) | 0.3 (7) | −2.62 (7.40) | −0.62 (1.98) | |
| DHA + AC | 14 | 3 (11) | −4 (10) | −1.15 (4.86) | 0.15 (2.08) | |
| Dairy BEF (Milkshake) | ||||||||||
| DHA | AC | OBG | DHA + AC | DHA + OBG | ||||||
| T0 | T28 | T0 | T28 | T0 | T28 | T0 | T28 | T0 | T28 | |
| 14:0 | 0.9 ± 0.5 | 0.9 ± 0.5 | 1.1 ± 0.4 | 1.2 ± 0.6 | 1.2 ± 0.4 | 1.1 ± 0.4 | 0.9 ± 0.4 | 0.9 ± 0.4 | 1.4 ± 0.6 | 1.1 ± 0.6 |
| 16:0 | 27.9 ± 1.8 | 30.5 ± 8.9 | 28.8 ± 3.4 | 29.2 ± 3.2 | 28.2 ± 2.3 | 31.7 ± 8.5 | 28.9 ± 4 | 28 ± 3.2 | 27.7 ± 2.3 | 28.3 ± 2.4 |
| 16:1 | 1.5 ± 0.6 | 2 ± 0.9 | 1.8 ± 0.5 | 1.9 ± 0.8 | 2.1 ± 1 | 2.2 ± 1.4 | 1.3 ± 0.5 | 1.4 ± 0.6 | 2.4 ± 1.1 | 2.3 ± 2.4 |
| 18:0 | 10.4 ± 2.2 | 10.4 ± 3.4 | 9.3 ± 2.1 | 9.0 ± 1.3 | 9.5 ± 2.4 | 10.2 ± 2.1 | 10.1 ± 2.1 | 10.5 ± 2.8 | 9.1 ± 2.1 | 9.9 ± 1.5 |
| 18:1 | 22.7 ± 2.2 | 25.1 ± 7.3 | 23.5 ± 2.8 | 23.9 ± 1.8 | 25.5 ± 2.8 | 28.1 ± 7 | 22.3 ± 3.1 | 22.6 ± 3.5 | 24.9 ± 3.8 | 22.4 ± 4 |
| 18:2 | 24.9 ± 3.3 | 26.3 ± 9.5 | 23.6 ± 3.8 | 23.9 ± 3.7 | 23.5 ± 4 | 25.3 ± 6.7 | 24.3 ± 4.9 | 24.3 ± 3 | 23.7 ± 4.8 | 23.8 ± 5.2 |
| 18:3 | 0.3 ± 0.3 | 0.2 ± 0.2 | 0.2 ± 0.3 | 0.2 ± 0.2 | 0.1 ± 0.1 | 0.3 ± 0.3 | 0.2 ± 0.2 | 0.4 ± 0.7 | 0.2 ± 0.2 | 0.1 ± 0.2 |
| 20:4 | 7.3 ± 1.6 | 6.3 ± 2 | 7.1 ± 1.6 | 6.6 ± 1.4 | 5.5 ± 1.4 | 7 ± 2.5 | 7.1 ± 1.8 | 6.9 ± 1.5 | 6.5 ± 1.8 | 7 ± 1.3 |
| 20:5n-3 | 0.5 ± 0.4 | 0.5 ± 0.6 | 0.4 ± 0.4 | 0.5 ± 0.5 | 0.3 ± 0.4 | 0.3 ± 0.4 | 0.6 ± 0.4 | 1.1 ± 2 | 0.5 ± 0.5 | 0.6 ± 0.7 |
| 22:6n-3 | 3.6 ± 0.8 | 5.3 ± 2.8 * | 4.1 ± 1.2 | 3.7 ± 1.1 | 4.1 ± 0.9 | 3.7 ± 1 | 4.2 ± 1.1 | 3.9 ± 0.9 | 3.6 ± 1.0 | 4.4 ± 1.4 * |
| Egg-based BEF (Pancake) | ||||||||||
| DHA | AC | OBG | DHA + AC | DHA + OBG | ||||||
| T0 | T28 | T0 | T28 | T0 | T28 | T0 | T28 | T0 | T28 | |
| 14:0 | 0.4 ± 0.4 | 0.30 ± 0.3 | 0.736 ± 0.63 | 0.4 ± 0.3 | 0.8 ± 0.1 | 0.9 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.2 | 0.3 ± 0.2 | 0.4 ± 0.2 |
| 16:0 | 25.5 ± 4.0 | 27.0 ± 3.5 | 27.1 ± 4.1 | 24.6 ± 2.9 | 27.2 ± 2.6 | 27.2 ± 2.6 | 26.1 ± 0.3 | 26.1 ± 0.4 | 26.9 ± 1.7 | 27.3 ± 1.8 |
| 16:1 | 1.4 ± 0.7 | 1.2 ± 0.8 | 1.7 ± 0.0 | 1.3 ± 0.7 | 0.9 ± 0.8 | 0.6 ± 0.2 | 1.1 ± 0.5 | 0.8 ± 0.1 | 1.5 ± 0.3 | 1.3 ± 1.3 |
| 18:0 | 9.1 ± 1.3 | 10.4 ± 2.4 | 8.4 ± 1.8 | 10.0 ± 1.3 | 10.0 ± 0.1 | 10.2 ± 0.2 | 8.6 ± 1.8 | 8.9 ± 0.9 | 9.2 ± 1.1 | 11.3 ± 2.9 |
| 18:1 | 24.7 ± 0.7 | 22.3 ± 2.3 | 24.0 ± 1.4 | 23.7 ± 1.5 | 22.9 ± 2.5 | 20.4 ± 0.4 | 24.8 ± 1.9 | 22.4 ± 0.9 | 24.8 ± 5.5 | 19.3 ± 2.0 |
| 18:2 | 28.9 ± 4.3 | 28.7 ± 7.2 | 28.0 ± 0.2 | 28.9 ± 1.7 | 27.3 ± 3.3 | 28.9 ± 3.7 | 28.6 ± 0.9 | 30.8 ± 1.1 | 26.7 ± 2.4 | 25.3 ± 3.8 |
| 18:3 | 0.1 ± 0.1 | n.d. | n.d. | n.d. | n.d | n.d. | 0.1 ± 0.2 | n.d. | 0.1 ± 0.1 | 0.1 ± 0.2 |
| 20:4 | 6.2 ± 0.7 | 5.1 ± 2.1 | 6.1 ± 3.8 | 7.3 ± 4.6 | 6.3 ± 0.7 | 7.3 ± 0.2 | 6.3 ± 0.1 | 5.9 ± 0.4 | 6.9 ± 1.2 | 8.8 ± 0.9 |
| 20:5n-3 | 0.3 ± 0.3 | 0.2 ± 0.2 | 0.2 ± 0.0 | n.d. | 0.6 ± 0.4 | 0.4 ± 0.2 | 0.1 ± 0.1 | 0.2 ± 0.3 | 0.7 ± 0.9 | 1.2 ± 0.4 |
| 22:6n-3 | 3.3 ± 0.7 | 4.9 ± 1.7 | 3.7 ± 1.1 | 3.9 ± 1.1 | 4.2 ± 0.1 | 4.0 ± 1.0 | 3.9 ± 0.1 | 4.4 ± 0.2 | 3.1 ± 0.9 | 4.9 ± 1.1 |
| Bakery BEF (Biscuits) | ||||||||||
| DHA | AC | OBG | DHA + AC | DHA + OBG | ||||||
| T0 | T28 | T0 | T28 | T0 | T28 | T0 | T28 | T0 | T28 | |
| 14:0 | 1.4 ± 0.3 | 1.5 ± 0.3 | 1.7 ± 0.4 | 1.7 ± 0.4 | 1.4 ± 0.6 | 1.3 ± 0.5 | 1.8 ± 0.7 | 1.6 ± 0.6 | 1.9 ± 0.6 | 1.6 ± 0.6 |
| 16:0 | 27.0 ± 0.8 | 25.9 ± 1.9 | 26.6 ± 2.0 | 26.5 ± 1.7 | 26.6 ± 2.0 | 25.9 ± 2.6 | 27.8 ± 1.8 | 27.3 ± 0.9 | 28.6 ± 3.1 | 26.7 ± 1.9 * |
| 16:1 | 3.1 ± 0.8 | 2.9 ± 0.7 | 3.0 ± 0.7 | 3.0 ± 0.6 | 2.6 ± 0.8 | 2.6 ± 0.9 | 3.3 ± 0.70 | 3.3 ± 0.56 | 3.6 ± 0.5 | 3.1 ± 1.0 |
| 18:0 | 9.4 ± 1.7 | 8.9 ± 1.2 | 9.3 ± 1.5 | 8.9 ± 1.1 | 8.6 ± 1.6 | 8.4 ± 0.9 | 9.0 ± 1.3 | 8.6 ± 1.9 | 9.0 ± 1.1 | 8.7 ± 0.9 |
| 18:1 | 25.2 ± 0.9 | 23.1 ± 2.4 | 23.4± 2.5 | 24.8 ± 3.4 | 24.2 ± 1.8 | 25.0 ± 2.4 | 24.6 ± 4.3 | 25.1 ± 3.0 | 24.1 ± 0.8 | 24.4 ± 2.7 |
| 18:2 | 28.6 ± 3.0 | 26.2 ± 2.1 | 26.0 ± 4.0 | 25.3 ± 3.3 | 26.3 ± 3.5 | 26.0 ± 4.0 | 23.8 ± 4.3 | 22.9 ± 2.4 | 22.7 ± 3.4 | 23.6 ± 4.2 |
| 18:3 | 1.3 ± 0.4 | 1.2 ± 0.1 | 1.1 ± 0.3 | 1.2 ± 0.3 | 1.0 ± 0.3 | 1.1 ± 0.3 | 1.1 ± 0.2 | 0.9 ± 0.1 | 1.1 ± 0.2 | 1.0 ± 0.3 |
| 20:4 | 6.3 ± 0.9 | 6.9 ± 1.3 | 6.2 ± 1.0 | 6.1 ± 1.1 | 6.3 ± 1.0 | 6.9 ± 1.4 | 6.1 ± 1.7 | 6.7 ± 1.3 | 6.1 ± 0.8 | 6.8 ± 1.2 |
| 20:5n-3 | 0.9 ± 0.3 | 0.9 ± 0.3 | 0.9 ± 0.5 | 0.8 ± 0.3 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.7 ± 0.1 | 0.9 ± 0.3 | 0.8 ± 0.2 | 1.0 ± 0.3 |
| 22:6n-3 | 2.3 ± 0.5 | 2.5 ± 0.7 | 1.9 ± 0.3 | 1.8 ± 0.3 | 2.1 ± 0.5 | 2.0 ± 0.5 | 1.8 ± 0.3 | 2.6 ± 0.5 ** | 1.9 ± 0.7 | 3.1 ± 1.1 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bub, A.; Malpuech-Brugère, C.; Orfila, C.; Amat, J.; Arianna, A.; Blot, A.; Di Nunzio, M.; Holmes, M.; Kertész, Z.; Marshall, L.; et al. A Dietary Intervention of Bioactive Enriched Foods Aimed at Adults at Risk of Metabolic Syndrome: Protocol and Results from PATHWAY-27 Pilot Study. Nutrients 2019, 11, 1814. https://doi.org/10.3390/nu11081814
Bub A, Malpuech-Brugère C, Orfila C, Amat J, Arianna A, Blot A, Di Nunzio M, Holmes M, Kertész Z, Marshall L, et al. A Dietary Intervention of Bioactive Enriched Foods Aimed at Adults at Risk of Metabolic Syndrome: Protocol and Results from PATHWAY-27 Pilot Study. Nutrients. 2019; 11(8):1814. https://doi.org/10.3390/nu11081814
Chicago/Turabian StyleBub, Achim, Corinne Malpuech-Brugère, Caroline Orfila, Julien Amat, Alice Arianna, Adeline Blot, Mattia Di Nunzio, Melvin Holmes, Zsófia Kertész, Lisa Marshall, and et al. 2019. "A Dietary Intervention of Bioactive Enriched Foods Aimed at Adults at Risk of Metabolic Syndrome: Protocol and Results from PATHWAY-27 Pilot Study" Nutrients 11, no. 8: 1814. https://doi.org/10.3390/nu11081814