Association between Ready-to-Eat Cereal Consumption and Nutrient Intake, Nutritional Adequacy, and Diet Quality among Infants, Toddlers, and Children in the National Health and Nutrition Examination Survey 2015–2016

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Population
2.2. RTE Cereal Consumption
2.3. Outcome Variables
2.3.1. Macro- and Micro-nutrients
2.3.2. Percent Contribution of RTE Cereal to Daily Nutrient Intake
2.3.3. Food Group Intake
2.3.4. Healthy Eating Index 2015 Scores
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Prevalence of RTE Cereal Consumption and Demographic Characteristics of RTE Cereal Eaters
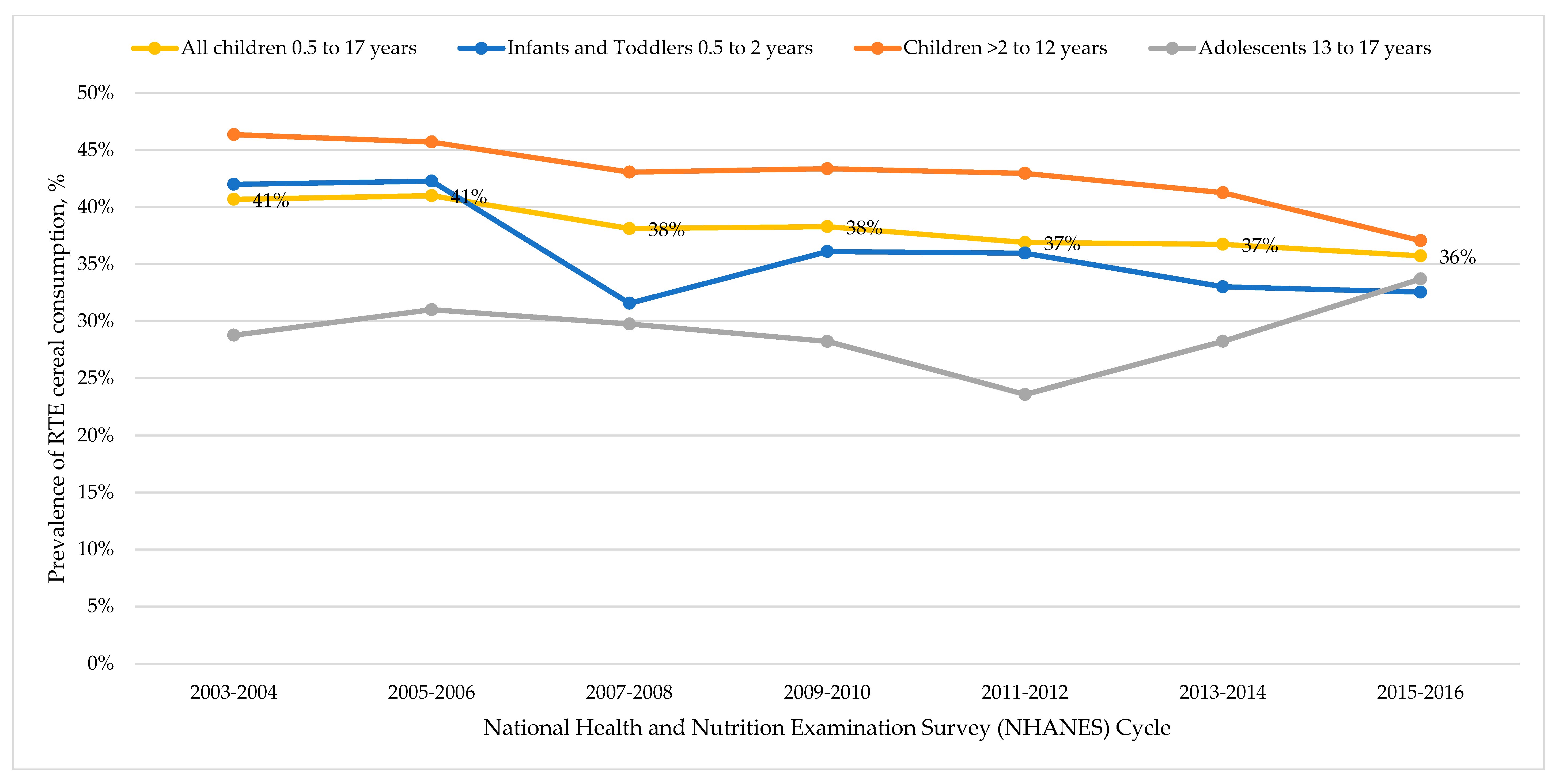
3.2. Trends in RTE Cereal Consumption
3.3. Differences in Nutrient Intakes for the Total Day between RTE Cereal Eaters and RTE Cereal Non-Eaters
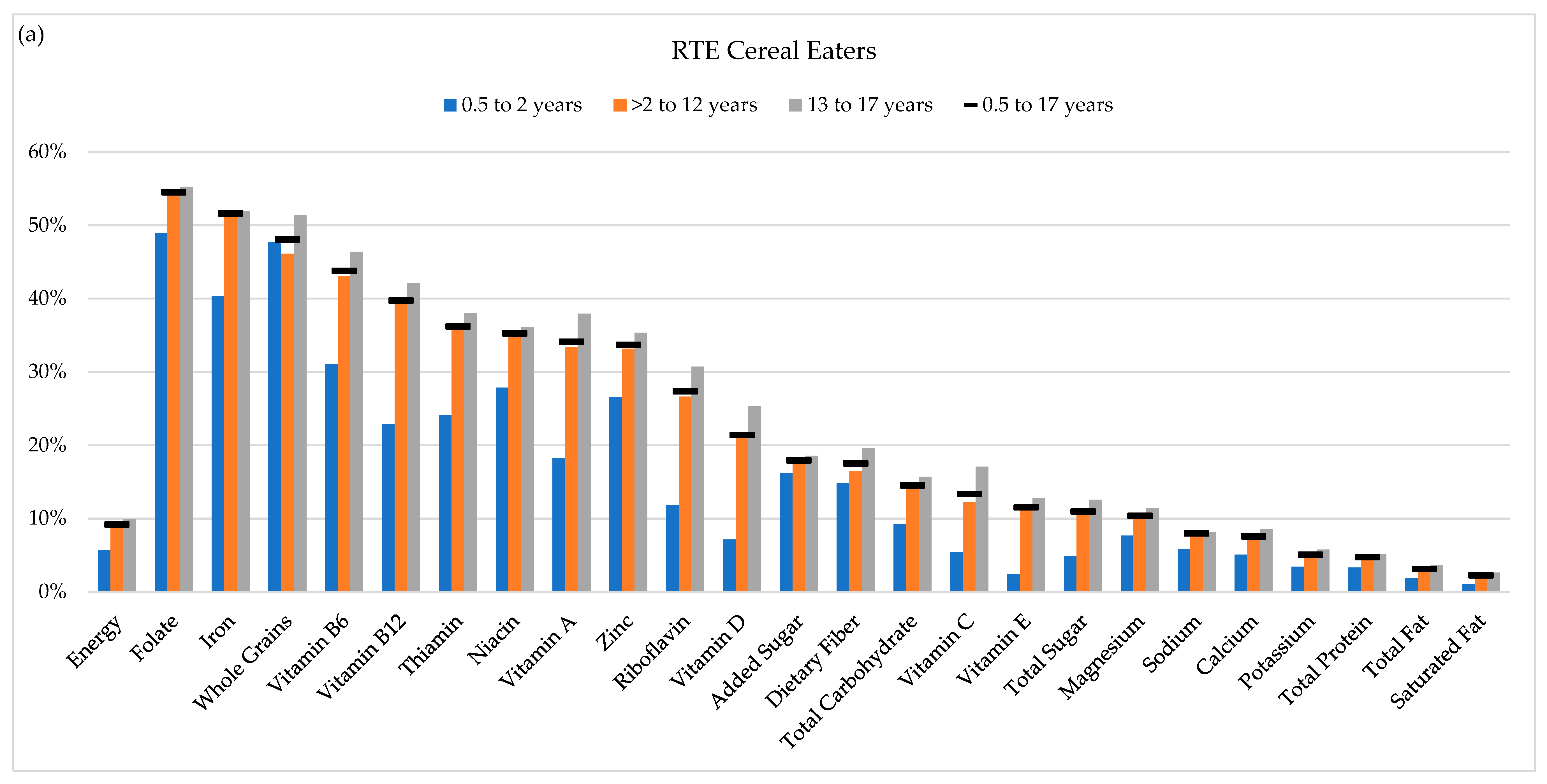
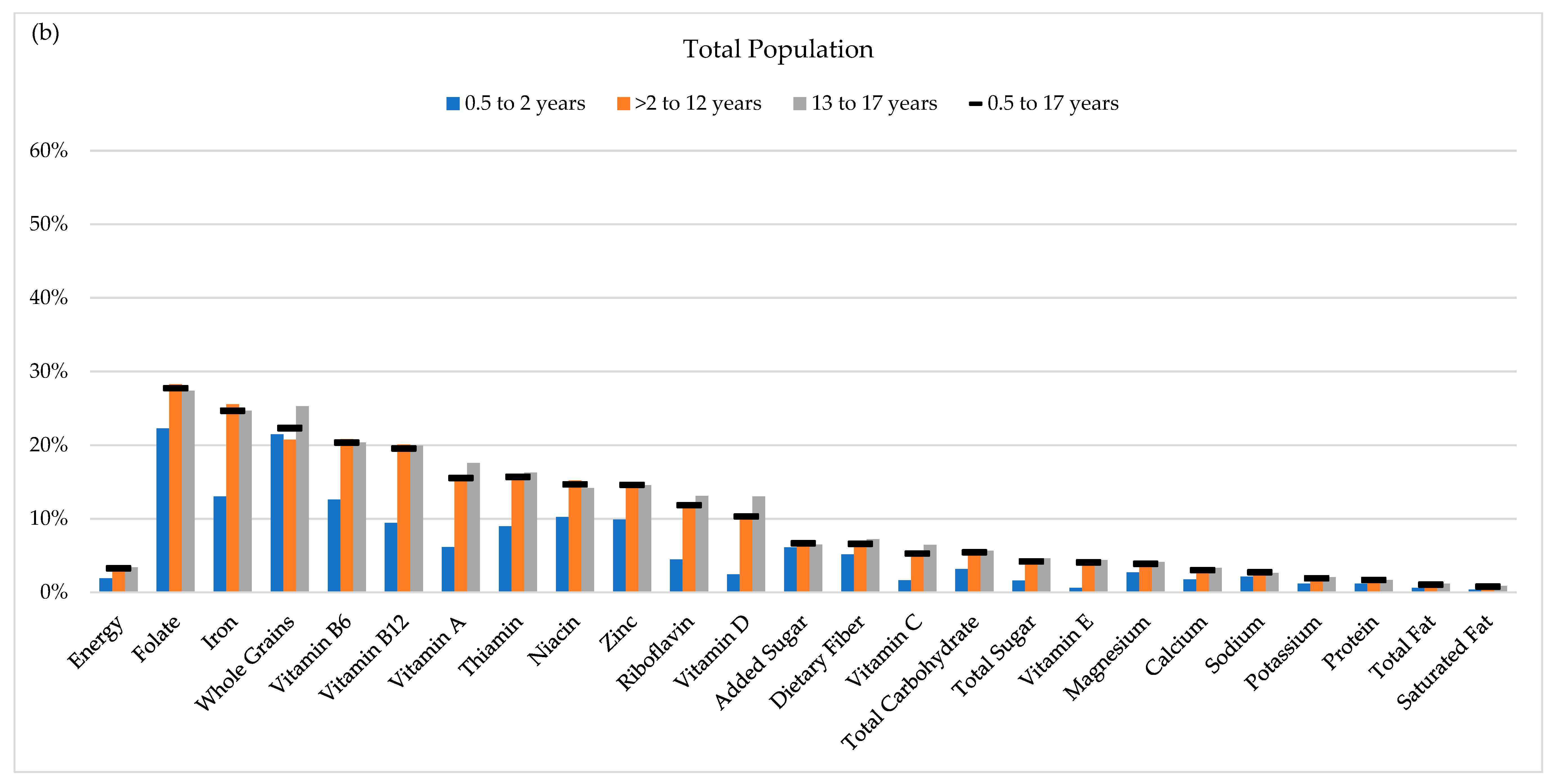
3.4. Contribution of RTE Cereal to Daily Nutrient Intakes
3.5. Food Group Intake for RTE Cereal Eaters and RTE Cereal Non-Eaters
3.6. Healthy Eating Index for RTE Cereal Eaters and RTE Cereal Non-Eaters
4. Discussion
4.1. Cereal Consumption over Time
4.2. Nutrient and Food Group Intakes in Infants and Toddlers
4.3. Nutrient and Food Group Intakes in Children and Adolescents
4.4. Nutrient Intakes across All Age Groups
4.5. Public Health Implication
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- 2015–2020 Dietary Guidelines for Americans. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 25 June 2019).
- Affenito, S.G.; Thompson, D.; Dorazio, A.; Albertson, A.M.; Loew, A.; Holeschuh, N.M. Ready-to-eat cereal consumption and the School Breakfast Program: Relationship to nutrient intake and weight. J. Sch. Health 2013, 83, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Albertson, A.M.; Anderson, G.H.; Crockett, S.J.; Goebel, M.T. Ready-to-eat cereal consumption: Its relationship with BMI and nutrient intake of children aged 4 to 12 years. J. Am. Diet. Assoc. 2003, 103, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Alberston, A.M.; Affenito, S.G.; Bauserman, R.; Holschuh, N.M.; Eldridge, A.L.; Barton, B.A. The relationship of ready-to-eat cereal consumption to nutrient intake, blood lipids, and body mass index of children as they age through adolescence. J. Am. Diet. Assoc. 2009, 109, 1557–1565. [Google Scholar] [CrossRef]
- Deshmukh-Taskar, P.R.; Nicklas, T.A.; O’Neil, C.E.; Keast, D.R.; Radcliffe, J.D.; Cho, S. The relationship of breakfast skipping and type of breakfast consumption with nutrient intake and weight status in children and adolescents: The National Health and Nutrition Examination Survey 1999–2006. J. Am. Diet. Assoc. 2010, 110, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L.; Buckley, R.B. The contribution of fortified ready-to-eat cereal to vitamin and mineral intake in the U.S. population, NHANES 2007–2010. Nutrients 2015, 7, 3949–3958. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, Y.; Fulgoni, V.L. Certain grain foods can be meaningful contributors to nutrient density in the diets of U.S. children and adolescents: Data from the National Health and Nutrition Examination Survey, 2009–2012. Nutrients 2017, 9, 160. [Google Scholar] [CrossRef]
- Song, W.O.; Chun, O.K.; Kerver, J.; Cho, S.; Chung, C.E.; Chung, S.J. Ready-to-eat breakfast cereal consumption enhances milk and calcium intake in the US population. J. Am. Diet. Assoc. 2006, 106, 1783–1789. [Google Scholar] [CrossRef]
- Williams, B.M.; O’Neil, C.E.; Keast, D.R.; Cho, S.; Nicklas, T.A. Are breakfast consumption patterns associated with weight status and nutrient adequacy in African-American children? Public Health Nutr. 2009, 12, 489–496. [Google Scholar] [CrossRef]
- Priebe, M.G.; McMonagle, J.R. Effects of ready-to-eat cereals on key nutritional and health outcomes: A systematic review. PLoS ONE 2016, 11, E0164931. [Google Scholar] [CrossRef]
- Xu, M.; Huang, T.; Lee, A.W.; Qi, L.; Cho, S. Ready-to-eat cereal consumption with total and cause-specific mortality: Prospective analysis of 367,442 individuals. J. Am. Coll. Nutr. 2016, 35, 217–223. [Google Scholar] [CrossRef]
- Topics and Questions to Be Examined by the Dietary Guidelines Advisory Committee. Available online: https://www.dietaryguidelines.gov/work-under-way/review-science/topics-and-questions-under-review (accessed on 25 June 2019).
- Grimes, C.A.; Szymlek-Gay, E.A.; Campbell, K.J.; Nicklas, T.A. Food sources of total energy and nutrients among U.S. infants and toddlers: National Health and Nutrition Examination Survey 2005–2012. Nutrients 2015, 7, 6797–6836. [Google Scholar] [CrossRef] [PubMed]
- National Health and Nutrition Examination Survey Data. Available online: https://wwwn.cdc.gov/nchs/nhanes/ContinuousNhanes/Default.aspx?BeginYear=2015 (accessed on 24 June 2019).
- Food Patterns Equivalents Database 2015–2016: Methodology and User Guide. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 24 June 2019).
- National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 13 August 2019).
- Blanton, C.A.; Moshfegh, A.J.; Baer, D.J.; Kretsch, M.J. The USDA Automated Multiple-Pass Method accurately estimates group total energy and nutrient intake. J. Nutr. 2006, 136, 2594–2599. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- National Health and Nutrition Examination Survey (NHANES): MEC In-Person Dietary Interviewers Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2015-2016/manuals/2016_MEC_In-Person_Dietary_Interviewers_Procedures_Manual.pdf (accessed on 25 June 2019).
- USDA Food and Nutrient Database for Dietary Studies 2015–2016. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 25 June 2019).
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Food and Nutrition Service. Child Nutrition Programs: Income Eligibility Guidelines; Federal Register: Washington, DC, USA, 2018; Volume 83, pp. 20788–20789.
- Ogden, C.L.; Lamb, M.M.; Carroll, M.D.; Flegal, K.M. Obesity and socioeconomic status in adults: United States, 2005–2008. NCHS Data Brief 2010, 50, 1–7. [Google Scholar]
- A Short History of Cereal. The New York Times. Available online: https://www.nytimes.com/interactive/2016/02/22/dining/history-of-cereal.html (accessed on 25 June 2019).
- Lepicard, E.M.; Maillot, M.; Vieux, F.; Viltard, M.; Bonnet, F. Quantitative and qualitative analysis of breakfast nutritional composition in French schoolchildren aged 9–11 years. J. Hum. Nutr. Diet. 2017, 30, 151–158. [Google Scholar] [CrossRef]
- Michels, N.; De Henauw, S.; Breidenassel, C.; Censi, L.; Cuenca-Garcia, M.; Gonzalez-Gross, M.; Gottrand, F.; Hallstrom, L.; Kafatos, A.; Kresting, M.; et al. European adolescent ready-to-eat cereal (RTEC) consumers have a healthier dietary intake and body composition compared with non-RTEC consumers. Eur. J. Nutr. 2015, 54, 653–664. [Google Scholar] [CrossRef]
- Barr, S.I.; DiFrancesco, L.; Fulgoni, V.L., 3rd. Breakfast consumption is positively associated with nutrient adequacy in Canadian children and adolescents. Br. J. Nutr. 2014, 112, 1373–1383. [Google Scholar] [CrossRef] [Green Version]
- Grieger, J.A.; Cobiac, L. Comparison of dietary intakes according to breakfast choice in Australian boys. Eur. J. Clin. Nutr. 2012, 66, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Koo, H.C.; Abdul Jalil, S.N.; Ruzita, A.T. Breakfast eating pattern and ready-to-eat cereals consumption among schoolchildren in Kuala Lumpur. Malays. J. Med. Sci. 2015, 22, 32–39. [Google Scholar] [PubMed]
- Vatanparast, H.; Islam, N.; Patil, R.P.; Shamloo, A.; Keshavarz, P.; Smith, J.; Chu, L.M.; Whiting, S. Consumption of ready-to-eat cereal in Canada and its contribution to nutrient intake and nutrient density among Canadians. Nutrients 2019, 11, 1009. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; De Henauw, S.; Beghin, L.; Cuenca-Garcia, M.; Gonzalez-Gross, M.; Hallstrom, L.; Kafatos, A.; Kersting, M.; Manios, Y.; Marcos, A.; et al. Ready-to-eat cereals improve nutrient, milk and fruit intake at breakfast in European adolescents. Eur. J. Nutr. 2016, 55, 771–779. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals; World Health Organization: Geenva, Switzerland, 2009; pp. 19–28. ISBN 9789241597494. [Google Scholar]
- Roess, A.A.; Jacquier, E.F.; Catellier, D.J.; Carvalho, R.; Lutes, A.C.; Anater, A.S.; Dietz, W.H. Food consumption patterns of infants and toddlers: Findings from the Feeding Infants and Toddlers Study (FITS) 2016. J. Nutr. 2018, 148, 1525s–1535s. [Google Scholar] [CrossRef] [PubMed]
- Grantham-McGregor, S.; Ani, C. A review of studies on the effect of iron deficiency on congitive development in children. J. Nutr. 2001, 131, 639S–666S. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Tucker, K.L. Dietary quality of the US child and adolescent population: Treands from 1999 to 2012 and associations with the use of federal nutrition assistance programs. Am. J. Clin. Nutr. 2017, 105, 194–202. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005; ISBN 978-0-309-08525-0. [Google Scholar]
- Global Burden of Diseases Diet Collaborators. Health effects of dietary risks in 195 countries, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Infants and Toddlers (0.5 to 2 Years) | Children (>2 to 12 Years) | Adolescents (13 to 17 Years) | All Children (0.5 to 17 Years) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RTE Cereal Eaters | RTE Cereal Non-Eaters | p2 | RTE Cereal Eaters | RTE Cereal Non-Eaters | p2 | RTE Cereal Eaters | RTE Cereal Non-Eaters | p2 | RTE Cereal Eaters | RTE Cereal Non-Eaters | p2 | ||
| n | 88 | 236 | 688 | 1169 | 242 | 546 | 1018 | 1951 | |||||
| Mean Age years ± SE | 1.4 ± 0.07 | 1.2 ± 0.03 | 0.007 | 6.7 ± 0.2 | 7.3 ± 0.1 | 0.007 | 14.7 ± 0.1 | 15.2 ± 0.1 | 0.002 | 8.7 ± 0.2 | 9.4 ± 0.2 | 0.06 | |
| Female, n (weighted %) | 39 (41%) | 113 (42%) | 0.89 | 341 (50%) | 593 (49%) | 0.65 | 103 (49%) | 279 (51%) | 0.71 | 483 (49%) | 985 (49%) | 0.81 | |
| Race/Ethnicity, n (weighted %) | Mexican American | 15 (15%) | 45 (15%) | 0.007 | 161 (18%) | 232 (14%) | 0.36 | 51 (17%) | 121 (16%) | 0.85 | 227 (17%) | 398 (15%) | 0.56 |
| Other Hispanic | 12 (8%) | 30 (9%) | 89 (9%) | 153 (9%) | 33 (10%) | 59 (7%) | 134 (9%) | 242 (8%) | |||||
| Non-Hispanic White | 43 (65%) | 69 (45%) | 192 (48%) | 356 (52%) | 77 (53%) | 157 (54%) | 312 (50%) | 582 (52%) | |||||
| Non-Hispanic Black | 14 (8%) | 55 (16%) | 148 (14%) | 266 (15%) | 50 (13%) | 123 (14%) | 212 (13%) | 444 (14%) | |||||
| Other | 4 (4%) | 37 (15%) | 98 (11%) | 162 (10%) | 31 (8%) | 86 (9%) | 133 (9%) | 285 (10%) | |||||
| PIR ≤1.85, n (weighted %) | 56 (60%) | 152 (61%) | 0.76 | 419 (53%) | 662 (44%) | 0.10 | 138 (46%) | 332 (47%) | 0.99 | 613 (51%) | 1146 (46%) | 0.25 | |
| PIR >1.85 and ≤3.5, n (weighted %) | 14 (18%) | 43 (20%) | 164 (27%) | 268 (27%) | 55 (25%) | 113 (25%) | 233 (26%) | 424 (26%) | |||||
| PIR >3.5, n (weighted %) | 18 (22%) | 41 (19%) | 105 (21%) | 239 (29%) | 49 (29%) | 101 (28%) | 172 (23%) | 381 (28%) | |||||
| Breakfast skipping 3, n (weighted %) | 19 (25%) | 85 (30%) | 0.55 | 17 (3%) | 206 (17%) | <0.0001 | 20 (8%) | 210 (36%) | <0.0001 | 56 (6%) | 501 24% | <0.0001 | |
| Infants and Toddlers (0.5 to 2 Years) | Children (>2 to 12 Years) | Adolescents (13 to 17 Years) | All Children (0.5 to 17 Years) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 2 | Model 2 3 | Model 1 2 | Model 2 3 | Model 1 2 | Model 2 3 | Model 1 2 | Model 2 3 | |||||||||
| % diff | p4 | % diff | p4 | % diff | p4 | % diff | p4 | % diff | p4 | % diff | p4 | % diff | p4 | % diff | p4 | |
| Energy | −1.8 | 0.79 | NA | NA | –0.2 | 0.93 | NA | NA | −0.1 | 0.99 | NA | NA | 0.8 | 0.74 | NA | NA |
| Total Carbohydrate | 0.3 | 0.97 | 2.0 | 0.51 | 7.9 | 0.01 | 8.2 | <0.0001 | 10.0 | 0.04 | 10.1 | <0.0001 | 9.7 | 0.0008 | 9.0 | <0.0001 |
| Total Sugar | −0.1 | 0.99 | 1.2 | 0.78 | 13.0 | 0.006 | 13.3 | 0.0004 | 12.9 | 0.06 | 13.0 | 0.001 | 13.1 | 0.002 | 12.4 | 0.0001 |
| Added sugar | −3.4 | 0.79 | −0.8 | 0.94 | 11.2 | 0.08 | 11.6 | 0.04 | 3.9 | 0.59 | 4.1 | 0.39 | 10.7 | 0.04 | 9.9 | 0.02 |
| Fiber | −4.6 | 0.52 | −2.8 | 0.59 | 6.9 | 0.04 | 7.1 | 0.005 | 14.6 | 0.002 | 14.7 | 0.0008 | 10.4 | 0.0004 | 9.9 | <0.0001 |
| Total Fat | −4.7 | 0.51 | −2.7 | 0.35 | −10.1 | 0.003 | −9.9 | <0.0001 | −9.2 | 0.11 | −9.2 | 0.0004 | −9.0 | 0.006 | −10.0 | <0.0001 |
| Saturated Fat | −2.8 | 0.70 | −0.9 | 0.86 | −9.8 | 0.02 | −9.6 | <0.0001 | −3.8 | 0.54 | −3.7 | 0.31 | −7.0 | 0.05 | −8.0 | 0.0001 |
| Protein | -0.3 | 0.98 | 1.5 | 0.82 | −0.9 | 0.76 | −0.6 | 0.69 | −8.0 | 0.16 | −8.0 | 0.02 | −1.9 | 0.54 | −2.7 | 0.15 |
| Calcium | 3.9 | 0.65 | 5.2 | 0.50 | 14.7 | 0.002 | 15.0 | <0.0001 | 26.3 | 0.0002 | 26.5 | <0.0001 | 18.3 | <0.0001 | 17.7 | <0.0001 |
| Iron | 15.9 | 0.20 | 16.7 | 0.14 | 70.3 | <0.0001 | 70.8 | <0.0001 | 77.2 | <0.0001 | 77.6 | <0.0001 | 70.1 | <0.0001 | 69.6 | <0.0001 |
| Magnesium | 2.6 | 0.76 | 4.3 | 0.41 | 6.4 | 0.08 | 6.6 | 0.003 | 11.0 | 0.10 | 11.1 | 0.02 | 9.2 | 0.01 | 8.5 | 0.0003 |
| Potassium | −0.7 | 0.93 | 0.8 | 0.84 | 7.6 | 0.03 | 7.8 | 0.0002 | 7.3 | 0.20 | 7.4 | 0.02 | 8.0 | 0.02 | 7.4 | 0.0002 |
| Sodium | −6.1 | 0.54 | −3.6 | 0.61 | −6.4 | 0.005 | −6.2 | 0.003 | −6.9 | 0.19 | −6.9 | 0.06 | −5.4 | 0.05 | −6.2 | 0.02 |
| Zinc | 26.6 | 0.03 | 27.6 | 0.008 | 42.9 | <0.0001 | 43.4 | <0.0001 | 38.2 | 0.002 | 38.3 | 0.0001 | 42.4 | <0.0001 | 42.1 | <0.0001 |
| Vitamin A | 14.3 | 0.08 | 15.0 | 0.05 | 51.8 | <0.0001 | 52.2 | <0.0001 | 68.9 | <0.0001 | 69.3 | <0.0001 | 53.0 | <0.0001 | 52.7 | <0.0001 |
| Thiamin | 20.0 | 0.03 | 22.1 | 0.0007 | 37.9 | <0.0001 | 37.1 | <0.0001 | 45.6 | <0.0001 | 46.6 | <0.0001 | 42.1 | <0.0001 | 41.6 | <0.0001 |
| Riboflavin | 19.0 | 0.02 | 20.1 | 0.001 | 36.6 | <0.0001 | 37.5 | <0.0001 | 49.7 | <0.0001 | 49.1 | <0.0001 | 40.4 | <0.0001 | 40.3 | <0.0001 |
| Niacin | 18.7 | 0.11 | 19.9 | 0.02 | 34.2 | <0.0001 | 34.5 | <0.0001 | 28.2 | 0.0005 | 28.4 | <0.0001 | 33.2 | <0.0001 | 32.7 | <0.0001 |
| Vitamin B6 | 35.6 | 0.008 | 35.9 | 0.0002 | 62.7 | <0.0001 | 62.7 | <0.0001 | 56.6 | <0.0001 | 57.6 | <0.0001 | 61.1 | <0.0001 | 60.8 | <0.0001 |
| Folate | 70.7 | 0.0005 | 71.2 | <0.0001 | 89.1 | <0.0001 | 89.8 | <0.0001 | 92.1 | <0.0001 | 92.6 | <0.0001 | 92.5 | <0.0001 | 92.5 | <0.0001 |
| Vitamin B12 | 39.2 | 0.004 | 39.7 | 0.003 | 79.6 | <0.0001 | 79.9 | <0.0001 | 83.2 | <0.0001 | 83.5 | <0.0001 | 81.2 | <0.0001 | 80.8 | <0.0001 |
| Vitamin C | −2.4 | 0.86 | −1.2 | 0.91 | 17.4 | 0.002 | 17.6 | 0.002 | 16.3 | 0.16 | 16.4 | 0.10 | 15.5 | 0.01 | 15.1 | 0.005 |
| Vitamin D | 14.9 | 0.13 | 15.7 | 0.09 | 59.3 | <0.0001 | 59.7 | <0.0001 | 113.3 | <0.0001 | 113.3 | <0.0001 | 63.8 | <0.0001 | 63.6 | <0.0001 |
| Vitamin E | −20.4 | 0.09 | −18.8 | 0.04 | 0.6 | 0.90 | 0.9 | 0.80 | 1.4 | 0.89 | 1.6 | 0.84 | −0.6 | 0.92 | −1.4 | 0.71 |
| Infants and Toddlers (0.5 to 2 Years) | Children (>2 to 12 Years) | Adolescents (13 to 17 Years) | All Children (0.5 to 17 Years) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | |
| Total dairy (cup eq.) | 2.1 ± 0.18 | 1.7 ± 0.13 | 0.15 | 2.2 ± 0.18 | 1.8 ± 0.14 | <0.0001 | 2.3 ± 0.09 | 1.6 ± 0.08 | <0.0001 | 2.2 ± 0.17 | 1.7 ± 0.15 | <0.0001 |
| Fluid milk (cup eq.) | 1.8 ± 0.10 | 1.3 ± 0.21 | 0.05 | 1.5 ± 0.13 | 1.0 ± 0.09 | <0.0001 | 1.4 ± 0.15 | 0.7 ± 0.12 | <0.0001 | 1.5 ± 0.09 | 1.0 ± 0.08 | <0.0001 |
| Total fruit (cup eq.) | 1.0 ± 0.10 | 0.9 ± 0.08 | 0.76 | 1.1 ± 0.14 | 1.0 ± 0.12 | 0.33 | 1.1 ± 0.15 | 0.9 ± 0.12 | 0.03 | 1.1 ± 0.07 | 1.0 ± 0.06 | 0.01 |
| Whole fruit (cup eq.) | 0.6 ± 0.06 | 0.6 ± 0.06 | 0.32 | 0.7 ± 0.13 | 0.7 ± 0.12 | 0.36 | 0.8 ± 0.15 | 0.5 ± 0.12 | 0.03 | 0.7 ± 0.06 | 0.6 ± 0.06 | 0.04 |
| Fruit juice (cup eq.) | 0.3 ± 0.08 | 0.3 ± 0.05 | 0.86 | 0.4 ± 0.03 | 0.4 ± 0.03 | 0.98 | 0.3 ± 0.07 | 0.3 ± 0.07 | 0.83 | 0.4 ± 0.03 | 0.3 ± 0.03 | 0.65 |
| Vegetables (cup eq.) | 0.5 ± 0.09 | 0.6 ± 0.10 | 0.06 | 0.9 ± 0.07 | 0.9 ± 0.07 | 0.50 | 0.9 ± 0.13 | 1.0 ± 0.11 | 0.03 | 0.8 ± 0.06 | 0.9 ± 0.07 | 0.27 |
| Total protein foods including legumes (oz eq.) | 1.3 ± 0.14 | 1.8 ± 0.10 | 0.02 | 3.7 ± 0.15 | 4.3 ± 0.12 | 0.009 | 4.1 ± 0.24 | 5.7 ± 0.25 | <0.0001 | 3.6 ± 0.11 | 4.4 ± 0.10 | 0.0001 |
| Total Grains (oz eq.) | 2.7 ± 0.17 | 2.6 ± 0.14 | 0.7 | 6.2 ± 0.15 | 6.5 ± 0.12 | 0.15 | 7.9 ± 0.23 | 7.7 ± 0.20 | 0.50 | 6.3 ± 0.13 | 6.4 ± 0.11 | 0.55 |
| Whole grains (oz eq.) | 0.7 ± 0.07 | 0.4 ± 0.05 | 0.006 | 1.1 ± 0.10 | 0.8 ± 0.09 | <0.0001 | 1.4 ± 0.20 | 0.7 ± 0.13 | 0.002 | 1.2 ± 0.10 | 0.7 ± 0.07 | <0.0001 |
| Refined Grains (oz eq.) | 2.0 ± 0.16 | 2.2 ± 0.12 | 0.33 | 5.1 ± 0.16 | 5.7 ± 0.11 | 0.002 | 6.5 ± 0.22 | 7.0 ± 0.17 | 0.05 | 5.2 ± 0.12 | 5.7 ± 0.08 | 0.002 |
| Maximum Score | Infants and Toddlers (0.5 to 2 Years) | Children (>2 to 12 Years) | Adolescents (13 to 17 Years) | All Children (0.5 to 17 Years) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | RTEC Eaters 2 | RTEC Non-Eaters | p-Value 3 | |||
| Total vegetables | 5 | 1.9 ± 0.22 | 2.4 ± 0.16 | 0.03 | 2.3 ± 0.10 | 2.2 ± 0.07 | 0.62 | 2.2 ± 0.11 | 2.4 ± 0.10 | 0.15 | 2.2 ± 0.07 | 2.3 ± 0.05 | 0.42 | |
| Greens and beans | 5 | 0.6 ± 0.36 | 1.0 ± 0.10 | 0.32 | 1.0 ± 0.11 | 1.1 ± 0.10 | 0.66 | 0.9 ± 0.15 | 1.0 ± 0.11 | 0.59 | 1.0 ± 0.09 | 1.0 ± 0.06 | 0.39 | |
| Total fruit | 5 | 3.7 ± 0.21 | 3.4 ± 0.17 | 0.39 | 2.8 ± 0.14 | 2.7 ± 0.09 | 0.77 | 2.6 ± 0.15 | 2.1 ± 0.10 | 0.02 | 2.8 ± 0.10 | 2.6 ± 0.07 | 0.08 | |
| Whole fruit | 5 | 3.7 ± 0.25 | 3.3 ± 0.20 | 0.32 | 2.7 ± 0.18 | 2.7 ± 0.12 | 0.87 | 2.5 ± 0.20 | 1.9 ± 0.11 | 0.01 | 2.7 ± 0.11 | 2.5 ± 0.10 | 0.09 | |
| Whole grains | 10 | 3.9 ± 0.31 | 2.3 ± 0.25 | 0.003 | 4.0 ± 0.16 | 2.6 ± 0.15 | <0.0001 | 4.2 ± 0.36 | 2.1 ± 0.26 | 0.002 | 4.0 ± 0.16 | 2.5 ± 0.14 | <0.0001 | |
| Dairy | 10 | 7.7 ± 0.30 | 6.4 ± 0.26 | 0.002 | 7.8 ± 0.22 | 6.3 ± 0.14 | <0.0001 | 7.3 ± 0.17 | 5.4 ± 0.14 | <0.0001 | 7.8 ± 0.16 | 6.1 ± 0.11 | <0.0001 | |
| Total protein foods | 5 | 2.1 ± 0.18 | 2.4 ± 0.15 | 0.11 | 3.4 ± 0.09 | 3.8 ± 0.08 | 0.01 | 3.4 ± 0.08 | 3.8 ± 0.09 | 0.007 | 3.4 ± 0.06 | 3.7 ± 0.07 | 0.008 | |
| Seafood and plant proteins | 5 | 0.6 ± 0.18 | 0.9 ± 0.12 | 0.25 | 1.7 ± 0.09 | 1.7 ± 0.12 | 0.80 | 1.8 ± 0.15 | 1.7 ± 0.14 | 0.69 | 1.7 ± 0.09 | 1.6 ± 0.10 | 0.66 | |
| Fatty acids | 10 | 1.2 ± 0.37 | 1.4 ± 0.18 | 0.66 | 3.8 ± 0.20 | 4.0 ± 0.12 | 0.33 | 3.6 ± 0.22 | 4.7 ± 0.19 | 0.002 | 3.5 ± 0.14 | 4.0 ± 0.07 | 0.02 | |
| Sodium | 10 | 8.4 ± 0.52 | 7.8 ± 0.27 | 0.35 | 5.4 ± 0.18 | 4.7 ± 0.14 | 0.001 | 4.8 ± 0.34 | 4.0 ± 0.18 | 0.04 | 5.5 ± 0.16 | 4.8 ± 0.14 | 0.005 | |
| Refined grains | 10 | 8.5 ± 0.35 | 7.8 ± 0.25 | 0.12 | 5.7 ± 0.20 | 4.7 ± 0.15 | 0.0005 | 5.2 ± 0.36 | 4.5 ± 0.23 | 0.09 | 5.7 ± 0.15 | 4.9 ± 0.11 | 0.0002 | |
| Saturated fat | 10 | 2.6 ± 0.53 | 2.6 ± 0.36 | 0.96 | 5.8 ± 0.17 | 4.7 ± 0.19 | 0.001 | 5.9 ± 0.34 | 5.4 ± 0.20 | 0.22 | 5.6 ± 0.15 | 4.7 ± 0.10 | 0.0004 | |
| Added sugar | 10 | 9.4 ± 0.14 | 9.2 ± 0.15 | 0.24 | 6.5 ± 0.18 | 7.1 ± 0.13 | 0.02 | 6.1 ± 0.34 | 6.3 ± 0.22 | 0.60 | 6.6 ± 0.15 | 7.1 ± 0.11 | 0.009 | |
| Total HEI 2015 Score | 100 | 54.2 ± 1.25 | 50.9 ± 0.94 | 0.06 | 52.9 ± 0.50 | 48.3 ± 0.73 | <0.0001 | 50.5 ± 0.79 | 45.3 ± 0.70 | <0.0001 | 52.6 ± 0.29 | 47.7 ± 0.57 | <0.0001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, J.D.; Zhu, Y.; Vanage, V.; Jain, N.; Holschuh, N.; Hermetet Agler, A. Association between Ready-to-Eat Cereal Consumption and Nutrient Intake, Nutritional Adequacy, and Diet Quality among Infants, Toddlers, and Children in the National Health and Nutrition Examination Survey 2015–2016. Nutrients 2019, 11, 1989. https://doi.org/10.3390/nu11091989
Smith JD, Zhu Y, Vanage V, Jain N, Holschuh N, Hermetet Agler A. Association between Ready-to-Eat Cereal Consumption and Nutrient Intake, Nutritional Adequacy, and Diet Quality among Infants, Toddlers, and Children in the National Health and Nutrition Examination Survey 2015–2016. Nutrients. 2019; 11(9):1989. https://doi.org/10.3390/nu11091989
Chicago/Turabian StyleSmith, Jessica D., Yong Zhu, Vipra Vanage, Neha Jain, Norton Holschuh, and Anne Hermetet Agler. 2019. "Association between Ready-to-Eat Cereal Consumption and Nutrient Intake, Nutritional Adequacy, and Diet Quality among Infants, Toddlers, and Children in the National Health and Nutrition Examination Survey 2015–2016" Nutrients 11, no. 9: 1989. https://doi.org/10.3390/nu11091989
APA StyleSmith, J. D., Zhu, Y., Vanage, V., Jain, N., Holschuh, N., & Hermetet Agler, A. (2019). Association between Ready-to-Eat Cereal Consumption and Nutrient Intake, Nutritional Adequacy, and Diet Quality among Infants, Toddlers, and Children in the National Health and Nutrition Examination Survey 2015–2016. Nutrients, 11(9), 1989. https://doi.org/10.3390/nu11091989