A Randomized, Double-Blind, Placebo-Controlled Clinical Trial Assessing the Effects of Angelica Gigas Nakai Extract on Blood Triglycerides


Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Subjects
- 1)
- Adult male and female participants aged 19–80 years at the time of screening
- 2)
- Participants with a blood TG range of 130~200 mg/dL at screening.
- 3)
- Participants who fully understood the test and decided to participate of their own free will and agreed to the written consent document.
- 1)
- Subjects who were treated with a lipid-lowering agent within six months of undergoing treatment
- 2)
- History of severe CVD, such as heart attack and/or stroke
- 3)
- History of genetic hyperlipidemia and kidney diseases, such as acute or chronic renal failure; autoimmune disease, cancer, respiratory disease (asthma, chronic obstructive pulmonary disease); or diagnosis of diabetes
- 4)
- History of clinically significant hypersensitivity reaction
- 5)
- History of gastrointestinal disease (e.g., Crohn’s disease) or surgery (excluding appendectomy and herniotomy)
- 6)
- Antipsychotic therapy within two months prior to screening
- 7)
- History of alcoholism or drug abuse
- 8)
- Participation in other clinical trials within two months prior to screening
- 9)
- Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) concentrations over three times the upper limit of the reference range or serum creatinine > 2.0 mg/dL
- 10)
- Pregnant or nursing women
- 11)
- No use of appropriate birth control methods among fertile women (except surgery for female infertility)
- 12)
- Deemed unfit by the principle investigator due to other complications.
2.3. Test Supplements
2.4. Standard Meal
2.5. Outcome Measurements
2.6. Safety Outcome Measurements
2.7. Evaluation of Diet and Physical Activity
2.8. Statistical Analysis
2.9. Sample Size
3. Results
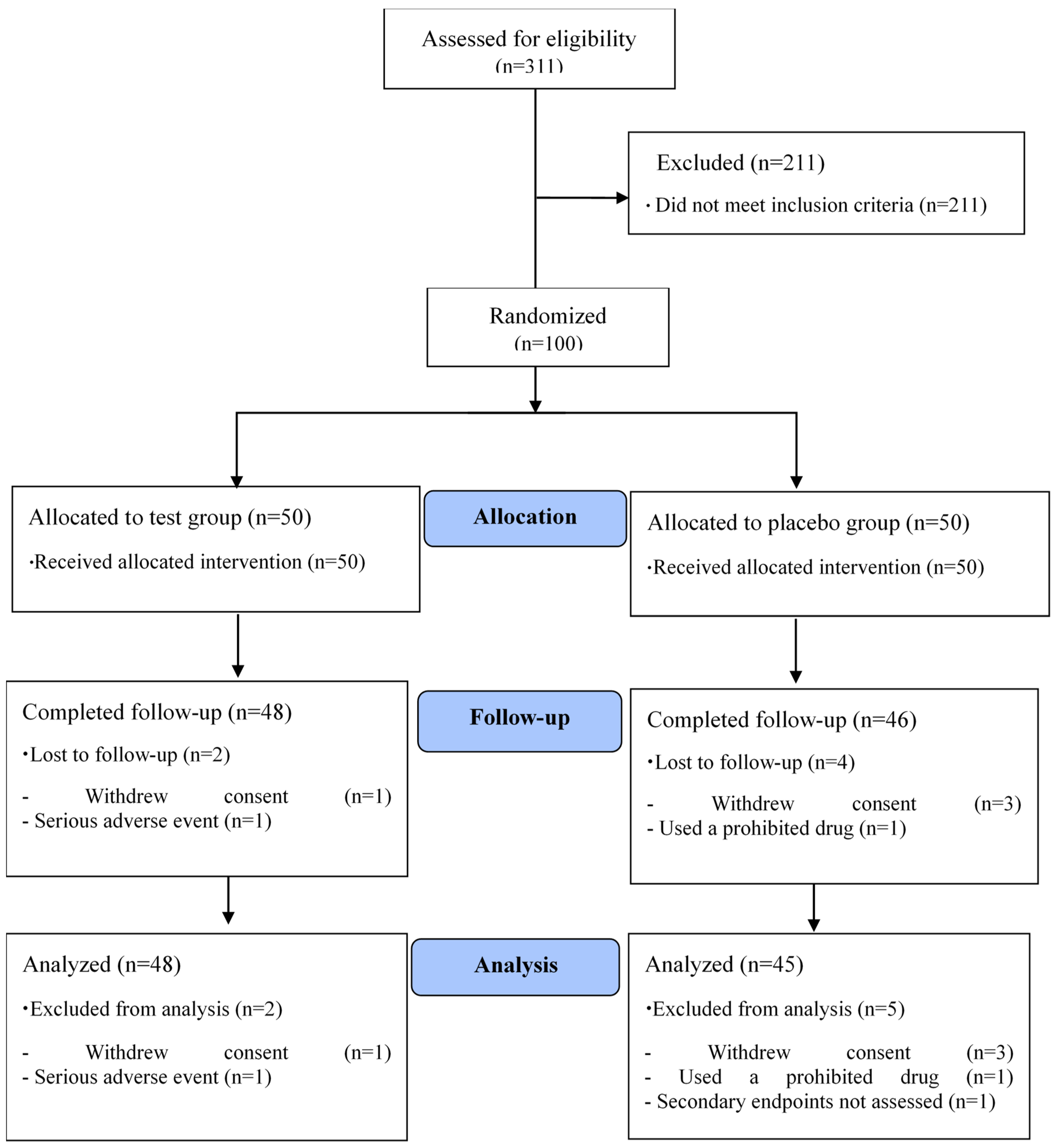
3.1. Participant Demographic Characteristics
3.2. Diet Intake and Physical Activity
3.3. Efficacy Evaluation
3.3.1. Primary Outcome
3.3.2. Secondary Outcome
3.4. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Korean National Health and Nutrition Examination Surveys VII, 1st ed.; Korea Centers for Disease Control and Prevention & Ministry of Health & Welfare: heongu-si, Chungcheongbuk-do, Korea, 2016.
- Braunwald Isselbacher. Harrison’s Principles of Internal Medicine, 13th ed.; McGraw-Hill, Inc.: Richmond, TX, USA, 1994. [Google Scholar]
- Jeong, M.H.; Cha, K.S.; Park, J.C.; Seo, J.P.; Park, J.H.; Cho, J.G.; Park, J.G.; Suh, S.P.; Park, J.C.; Kang, J.C. Clinical Effects of Simvastatin in Patients with Hypercholesterolemia. Korean Circ. J. 1997, 27, 417–425. [Google Scholar] [CrossRef]
- Kim, S.; Choe, S.; Min, C.; Lee, S.; Koo, J.; Sun, S.; Lee, N. The Pharmaceutical Composition Comprising Losartan for Treating or Preventing Statin-Induced Muscle Toxicity. U.S. Patent 1020130074808, 5 July 2013. [Google Scholar]
- Choi, H.J.; Park, J.N. Management of Risk of Statin therapy. J. Korean Acad. Fam. Med. 2004, 25, 713–720. [Google Scholar]
- Brown, S.L. Lowered serum cholesterol and low mood. BMJ 1996, 313, 637–638. [Google Scholar] [CrossRef] [PubMed]
- Hertog, M.G.; Feskens, E.J.; Hollman, P.C.; Katan, M.B.; Kromhout, D. Dietary antioxidant flavonoids and risk of coronary heart disease: The Zutphen Elderly Study. Lancet 1993, 342, 1007–1011. [Google Scholar] [CrossRef]
- Jung, U.J.; Lee, M.-K.; Jeong, K.-S.; Choi, M.-S. The Hypoglycemic effects of hesperidin and naringin are partly mediated by hepatic glucose-regulating enzymes in C57BL/KsJ-db/db mice. J. Nutr. 2004, 134, 2499–2503. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, M.K.; Ha, T.Y.; Bok, S.H.; Park, H.M.; Jeong, K.S.; Woo, M.N.; Do, G.M.; Yeo, J.Y.; Choi, M.S. Supplementation of whole persimmon leaf improves lipid profiles and suppresses body weight gain in rats fed high-fat diet. Food Chem. Toxicol. 2006, 44, 1875–1883. [Google Scholar] [CrossRef]
- Son, C.-Y.; Song, G.-Y.; Kang, J.-S.; Kwon, K.-I.; Baek, I.-H. Pharmacological Effect of Decursin and Decursinol Angelate from Angelica gigas Nakai. Yakhak Hoeji 2009, 53, 303–313. [Google Scholar]
- Han, D.S. Dong-Myoung publicating company, Seoul. Herbology 1998, 201–202. [Google Scholar]
- Kim, K.-M.; Jung, J.-Y.; Hwang, S.-W.; Kim, M.-J.; Kang, J.-S. Isolation and Purification of Decursin and Decursinol Angelate in Angelica gigas Nakai. J. Korean Soc. Food Sci. Nutr. 2009, 38, 653–656. [Google Scholar] [CrossRef]
- Jo, S.K.; Moon, H.S.; Yun, Y.S.; Hong, S.I.; Ham, Y.H.; Chung, I.S.; Park, E.K. Influence of Angelicae gigantis Radix on the Immune System I. T—Independent B Cell Proliferation. Korean J. Immunol. 1990, 12, 113–118. [Google Scholar]
- Lee, S.; Lee, Y.S.; Jung, S.H.; Shin, K.H.; Kim, B.K.; Kang, S.S. Anti-Tumor Activities of Decursinol Angelate and Decursin from Angelica gigas. Arch. Pharmacal Res. 2003, 26, 727–730. [Google Scholar] [CrossRef]
- Park, K.W.; Choi, S.R.; Hong, H.R.; Kim, J.Y.; Shon, M.Y.; Seo, K.I. Biological Activities of Methanol Extract of Angelica gigas Nakai. Korean J. Food Preserv. 2007, 14, 655–661. [Google Scholar]
- Hu, W.S.; Lee, S.J.; Pyo, J.H.; Kim, S.H.; Sung, N.J. Hypoglycemic and Hypolipidemic Effects of Jerusalem artichoke Composites in Streptozotocin induced Diabetic Rats. J. Life Sci. 2018, 28, 671–680. [Google Scholar] [CrossRef]
- Kang, S.A.; Han, J.A.; Jang, K.-H.; Choue, R. DPPH Radical Scavenger Activity and Antioxidant Effects of Cham - Dang - Gui (Angelica gigas). J Korean Soc. Food Sci. Nutr. 2004, 33, 1112–1118. [Google Scholar]
- Bae, U.-J.; Oh, M.-R.; Jung, T.-S.; Chae, S.-W.; Park, B.-H. Decursin and decursinol angelate-rich Angelica gigas Nakai extract suppresses de novo lipogenesis and alleviates nonalcoholic fatty liver disease and dyslipidemia in mice fed a high fat diet. J. Funct. Foods 2017, 31, 208–216. [Google Scholar] [CrossRef]
- Park, B.; Chae, S.; Jung, T.; Oh, S.; Park, J. Composition Containing Extract of Angelica gigas for Preventing and Treating Dyslipidemia. U.S. Patent 1020180042035, 2018. [Google Scholar]
- Triglyceride, high density lipoprotein, and coronary heart disease. Consensus statement. National Institutes of Health Consensus Development Conference. Consens Statement 1992, 10, 1–28.
- Park, H.S.; Shin, E.S.; Kim, J.J. Effect of Diet Therapy in Patients with Hypertriglyceridemia. J. Lipid Atherosclerosis 1995, 5, 85–94. [Google Scholar]
- Madjd, A.; Taylor, M.A.; Shafiei Neek, L.; Delavari, A.; Malekzadeh, R.; Macdonald, I.A.; Farshchi, H.R. Effect of weekly physical activity frequency on weight loss in healthy overweight and obese women attending a weight loss program: a randomized controlled trial. Am. J. Clin. Nutr. 2016, 104, 1202–1208. [Google Scholar] [CrossRef]
- Cha, K.-S.; Hong, S.-I.; Lee, Y.-S. The Relation between Total Volume of Physical Activity and Metabolic Syndrome - Prevalence at Community Health Center in Seoul, Korea. J. Korean soc. Wellness 2016, 11, 243–252. [Google Scholar] [CrossRef]
- Suliburska, J.; Bogdanski, P.; Szulinska, M.; Stepien, M.; Pupek-Musialik, D.; Jablecka, A.J.B.t.e.r. Effects of green tea supplementation on elements, total antioxidants, lipids, and glucose values in the serum of obese patients. Biol. Trace Elem. Res. 2012, 149, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Irudayaraj, S.S.; Sunil, C.; Duraipandiyan, V.; Ignacimuthu, S. In vitro antioxidant and antihyperlipidemic activities of Toddalia asiatica (L) Lam. leaves in Triton WR-1339 and high fat diet induced hyperlipidemic rats. Food Chem. Toxicol. 2013, 60, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Keaney, J.F., Jr.; Vita, J.A. Cholesterol reduction in cardiovascular disease. Clinical benefits and possible mechanisms. New England J. Med. 1995, 332, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the Metabolic Syndrome Among US Adults: Findings From the Third National Health and Nutrition Examination Survey. J. Am. Med Assoc. 2002, 287, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Bae, U.J.; Choi, E.K.; Oh, M.R.; Jung, S.J.; Park, J.; Jung, T.S.; Park, T.S.; Chae, S.W.; Park, B.H. Angelica gigas Ameliorates Hyperglycemia and Hepatic Steatosis in C57BL/KsJ-db/db Mice via Activation of AMP-Activated Protein Kinase Signaling Pathway. Am. J. Chin. Med. 2016, 44, 1627–1638. [Google Scholar] [CrossRef] [PubMed]
- Goliasch, G.; Wiesbauer, F.; Blessberger, H.; Demyanets, S.; Wojta, J.; Huber, K.; Maurer, G.; Schillinger, M.; Speidl, W.S. Premature myocardial infarction is strongly associated with increased levels of remnant cholesterol. J. Clin. Lipidol. 2015, 9, 801–806. [Google Scholar] [CrossRef]
- Sniderman, A.D.; Williams, K.; Contois, J.H.; Monroe, H.M.; McQueen, M.J.; de Graaf, J.; Furberg, C.D. A meta-analysis of low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, and apolipoprotein B as markers of cardiovascular risk. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 337–345. [Google Scholar] [CrossRef]
- Cai, G.; Shi, G.; Xue, S.; Lu, W. The atherogenic index of plasma is a strong and independent predictor for coronary artery disease in the Chinese Han population. Medicine (Baltimore) 2017, 96, 1–6. [Google Scholar] [CrossRef]
- Jeppesen, J.; Hein, H.O.; Suadican, P.; Gyntelberg, F. Triglyceride concentration and ischemic heart disease: an eight-year follow-up in the Copenhagen Male Study. Circulation 1998, 97, 1029–1036. [Google Scholar] [CrossRef]
- Dobiasova, M.; Frohlich, J. The plasma parameter log (TG/HDL-C) as an atherogenic index: correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-depleted plasma (FERHDL). Clin. Biochem. 2001, 34, 583–588. [Google Scholar] [CrossRef]
- Seo, J.-K.; Park, S.-H. The effect of exercise intervention program on the insulin resistance and the atherogenic index of the obese children. Korea J. Sports Sci. 2014, 23, 1195–1209. [Google Scholar]


{kind=link}
| Component | Test Capsule A. Gigas Nakai Extract Supplement (%) | Placebo Supplement (%) |
|---|---|---|
| A. gigas Nakai extract | 20 | - |
| Soybean oil | 73 | 93 |
| Beeswax | 7 | 7 |
| Total | 100 | 100 |
| AGNE Group (n = 50) | Placebo Group (n = 50) | Total (n = 100) | P Value 1) | |
|---|---|---|---|---|
| Sex (M/F) | 17/33 | 16/34 | 33/67 | 0.832 2) |
| Age (years) | 49.1 ± 10.5 | 50.5 ± 10.3 | 49.8 ± 10.4 | 0.497 |
| Height (cm) | 162.4 ± 8.1 | 163.2 ± 9.4 | 162.8 ± 8.8 | 0.634 |
| Weight (kg) | 67.9 ± 11.9 | 69.1 ± 14.3 | 68.5 ± 13.1 | 0.631 |
| BMI (kg/m2) | 25.6 ± 3.3 | 25.8 ± 3.6 | 25.7 ± 3.4 | 0.809 |
| SBP (mmHg) | 124.2 ± 15.7 | 123.8 ± 13.0 | 124.0 ± 14.6 | 0.889 |
| DBP (mmHg) | 78.4 ± 11.9 | 78.0 ± 10.0 | 78.2 ± 10.9 | 0.856 |
| Pulse (bpm) | 77.2 ± 8.3 | 74.0 ± 11.3 | 76.7 ± 9.5 | 0.631 |
| Alcohol (Y/N) | 21/29 | 18/32 | 39/61 | 0.539 2) |
| Alcohol (unit 3)/week) | 4.1 ± 4.7 | 4.1 ± 5.7 | 4.1 ± 5.1 | 0.966 |
| Smoking (Y/N) | 5/45 | 5/45 | 10/90 | >0.999 2) |
| Smoking (n/day) | 9.2 ± 7.1 | 16.0 ± 5.5 | 12.6 ± 7.0 | 0.129 |
| AGNE Group (n = 48) | Placebo Group (n = 45) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | Change | P Value 1) | Baseline | Week 12 | Change | P Value 1) | P Value 2) | |
| Energy (Kcal) | 1595.3 ± 466.4 | 1627.0 ± 476.0 | 31.7 ± 10.0 | 0.662 | 1600.2 ± 399.2 | 1591.9 ± 428.9 | −8.3 ± 29.7 | 0.885 | 0.667 |
| Carbohydrates (g) | 249.3 ± 73.0 | 240.4 ± 68.1 | −8.9 ± 65.5 | 0.351 | 243.0 ± 68.4 | 249.1 ± 71.2 | 6.1 ± 2.8 | 0.549 | 0.281 |
| Lipids (g) | 38.4 ± 20.2 | 45.2 ± 23.3 | 6.8 ± 3.15 | 0.102 | 40.4 ± 15.6 | 39.1 ± 18.7 | −1.3 ± 3.1 | 0.677 | 0.117 |
| Protein (g) | 62.1 ± 19.5 | 63.8 ± 20.6 | 1.7 ± 1.1 | 0.582 | 62.5 ± 15.9 | 60.1 ± 17.8 | −2.4 ± 1.9 | 0.366 | 0.314 |
| Fiber (g) | 21.0 ± 8.6 | 20.1 ± 7.2 | −0.9 ± 1.4 | 0.377 | 19.8 ± 7.0 | 20.0 ± 7.1 | 0.3 ± 0.1 | 0.787 | 0.409 |
| MET value(min/week) | 2383.8 ± 3198.4 | 1490.0 ± 1840.1 | −893.8 ± 1358.3 | 0.051 | 1351.1 ± 2190.3 | 1947.6 ± 2779.3 | 596.4 ± 589 | 0.139 | 0.015 |
| AGNE Group (n = 48) | Placebo Group (n = 45) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | Change | P-Value 1) | Baseline | Week 12 | Change | P-Value 1) | P-Value 2) | P-Value 3) | |
| TG (mg/dL) | 158.2 ± 21.3 | 143.4 ± 37.4 | −14.8 ± 16.1 | 0.010 | 159.4 ± 20.3 | 179.4 ± 86.7 | 19.9 ± 66.4 | 0.131 | 0.013 | 0.009 |
| TC (mg/dL) | 213.1 ± 32.1 | 213.6 ± 29.7 | 0.5 ± 2.4 | 0.902 | 213.8 ± 34.6 | 209.3 ± 34.3 | −4.6± 0.3 | 0.330 | 0.403 | 0.527 |
| LDL-C (mg/dL) | 135.8 ± 26.7 | 133.5 ± 25.6 | − 2.3 ± 1.1 | 0.493 | 134.4 ± 30.3 | 126.1 ± 29.7 | −8.4 ± 24.2 | 0.025 | 0.218 | 0.304 |
| HDL-C (mg/dL) | 50.4 ± 8.5 | 51.4 ± 8.0 | 1.1 ± 0.5 | 0.178 | 50.6 ± 11.2 | 50.3 ± 11.8 | −0.29 ± 0.6 | 0.802 | 0.326 | 0.617 |
| Non-HDL-C (mg/dL) | 162.8 ± 27.8 | 162.2 ± 27.1 | −0.6 ± 0.7 | 0.875 | 163.2 ± 30.1 | 158.9 ± 30.1 | −4.3 ± 0.1 | 0.330 | 0.516 | 0.594 |
| VLDL-C (mg/dL) | 31.6 ± 4.3 | 28.7 ± 7.5 | −3.0 ± 3.2 | 0.010 | 31.9 ± 4.1 | 35.9 ± 17.3 | 4.0 ± 13.2 | 0.131 | 0.013 | 0.009 |
| Free fatty acid (uEq/L) | 596.1 ± 228.2 | 629.6 ± 209.7 | 33.5 ± 18.5 | 0.218 | 634.0 ± 219.5 | 572.1 ± 164.5 | −62.0 ± 55.0 | 0.025 | 0.013 | 0.033 |
| ApoA1 (g/L) | 1.45 ± 0.19 | 1.47 ± 0.17 | 0.01 ± 0.02 | 0.546 | 1.47 ± 0.23 | 1.46 ± 0.21 | −0.01 ± 0.02 | 0.707 | 0.498 | 0.423 |
| ApoB (g/L) | 1.21 ± 0.21 | 1.20 ± 0.21 | −0.01± 0.0 | 0.723 | 1.22 ± 0.23 | 1.1 ± 0.23 | −0.05 ±0.0 | 0.092 | 0.290 | 0.567 |
| hs-CRP (g/L) | 1.19 ± 1.81 | 1.20 ± 2.58 | 0.01 ± 0.8 | 0.984 | 0.57 ± 0.98 | 1.41 ± 5.18 | 0.8 ± 4.2 | 0.264 | 0.327 | 0.328 |
| TC/HDL-C | 4.28 ± 0.60 | 4.21 ± 0.62 | −0.08 ± 0.02 | 0.349 | 4.34 ± 0.77 | 4.30 ± 0.86 | −0.0 ± 0.09 | 0.640 | 0.812 | 0.710 |
| LDL-C/HDL-C | 2.74 ± 0.56 | 2.64 ± 0.56 | −0.10 ± 0.0 | 0.132 | 2.75 ± 0.73 | 2.61 ± 0.78 | −0.1 ± 0.05 | 0.060 | 0.658 | 0.497 |
| TG/HDL-C | 3.23 ± 0.70 | 2.87 ± 0.92 | −0.36 ± 0.03 | 0.013 | 3.34 ± 0.99 | 3.87 ± 2.23 | 0.5 ± 1.24 | 0.074 | 0.006 | 0.006 |
| (TC-HDL-C)/HDL-C | 3.28 ± 0.60 | 3.21 ± 0.62 | −0.08 ± 0.02 | 0.349 | 3.3 ± 0.77 | 3.3 ± 0.86 | − 0.0 ±0.09 | 0.640 | 0.812 | 0.710 |
| ApoB/ApoA1 | 0.84 ± 0.18 | 0.83 ± 0.16 | −0.02 ± 0.02 | 0.410 | 0.85 ± 0.19 | 0.82 ± 0.20 | −0.03 ± 0.01 | 0.131 | 0.597 | 0.646 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, S.-J.; Kim, W.-R.; Oh, M.-R.; Cha, Y.-S.; Park, B.-H.; Chae, S.-W. A Randomized, Double-Blind, Placebo-Controlled Clinical Trial Assessing the Effects of Angelica Gigas Nakai Extract on Blood Triglycerides. Nutrients 2020, 12, 377. https://doi.org/10.3390/nu12020377
Jung S-J, Kim W-R, Oh M-R, Cha Y-S, Park B-H, Chae S-W. A Randomized, Double-Blind, Placebo-Controlled Clinical Trial Assessing the Effects of Angelica Gigas Nakai Extract on Blood Triglycerides. Nutrients. 2020; 12(2):377. https://doi.org/10.3390/nu12020377
Chicago/Turabian StyleJung, Su-Jin, Woo-Rim Kim, Mi-Ra Oh, Youn-Soo Cha, Byung-Hyun Park, and Soo-Wan Chae. 2020. "A Randomized, Double-Blind, Placebo-Controlled Clinical Trial Assessing the Effects of Angelica Gigas Nakai Extract on Blood Triglycerides" Nutrients 12, no. 2: 377. https://doi.org/10.3390/nu12020377
APA StyleJung, S.-J., Kim, W.-R., Oh, M.-R., Cha, Y.-S., Park, B.-H., & Chae, S.-W. (2020). A Randomized, Double-Blind, Placebo-Controlled Clinical Trial Assessing the Effects of Angelica Gigas Nakai Extract on Blood Triglycerides. Nutrients, 12(2), 377. https://doi.org/10.3390/nu12020377