
A Positive Association of Overactivated Immunity with Metabolic Syndrome Risk and Mitigation of Its Association by a Plant-Based Diet and Physical Activity in a Large Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Basal Characteristics and Anthropometric and Biochemical Parameters of the Participants
2.3. Definition of Immunity Status, MetS, and Immune-Related Diseases
2.4. Usual Food-Intake Measurement by a Semi-Quantitative Food Frequency Questionnaire (SQFFQ)
2.5. Dietary Patterns by Principal Components Analysis
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of the Participants according to Immunity Groups
3.2. Metabolic Parameters According to Immunity Groups
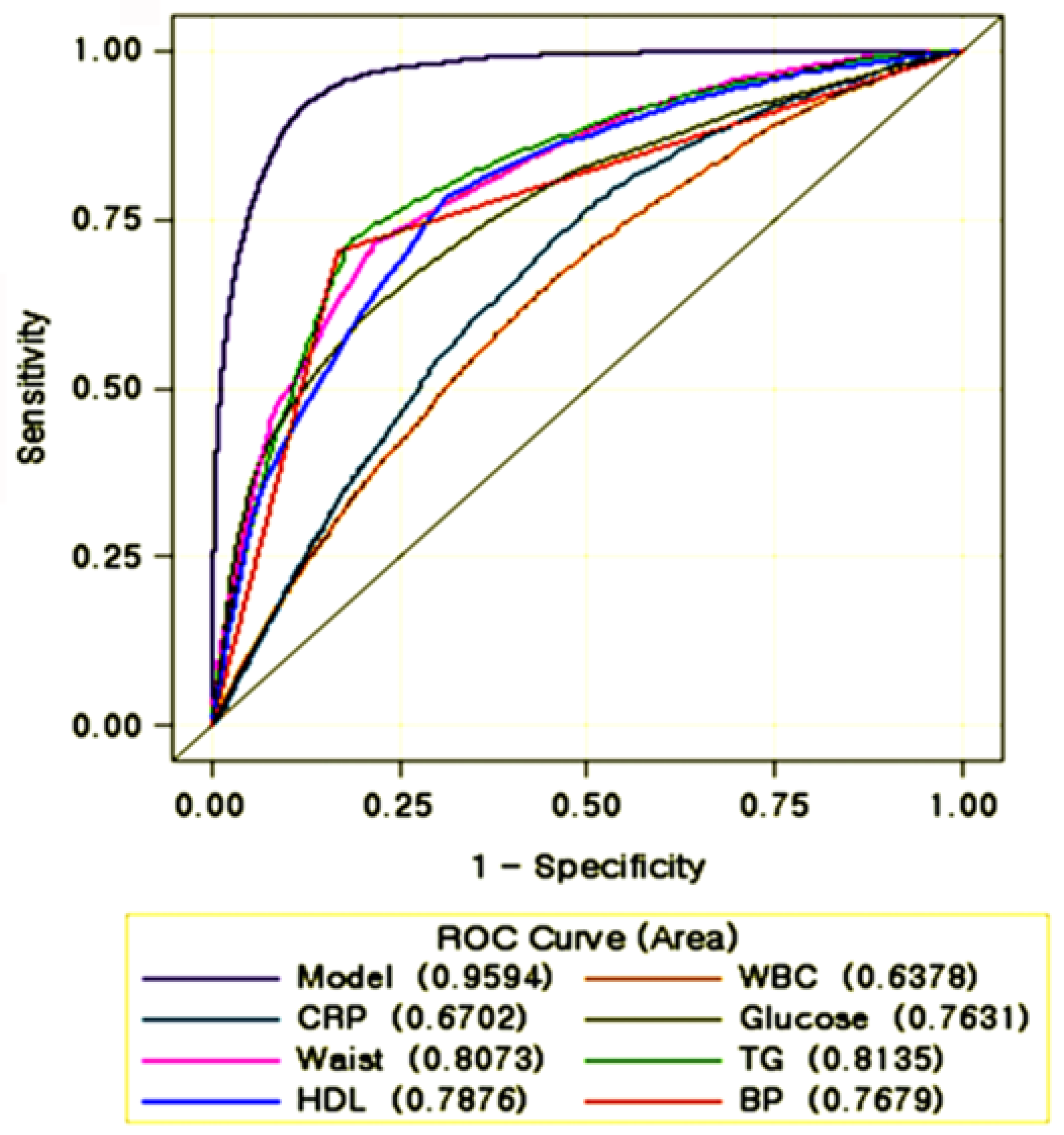
3.3. Association of the Risk of Various Metabolic Diseases with Immunity Status
3.4. Nutrient Intake Among the Immunity Groups
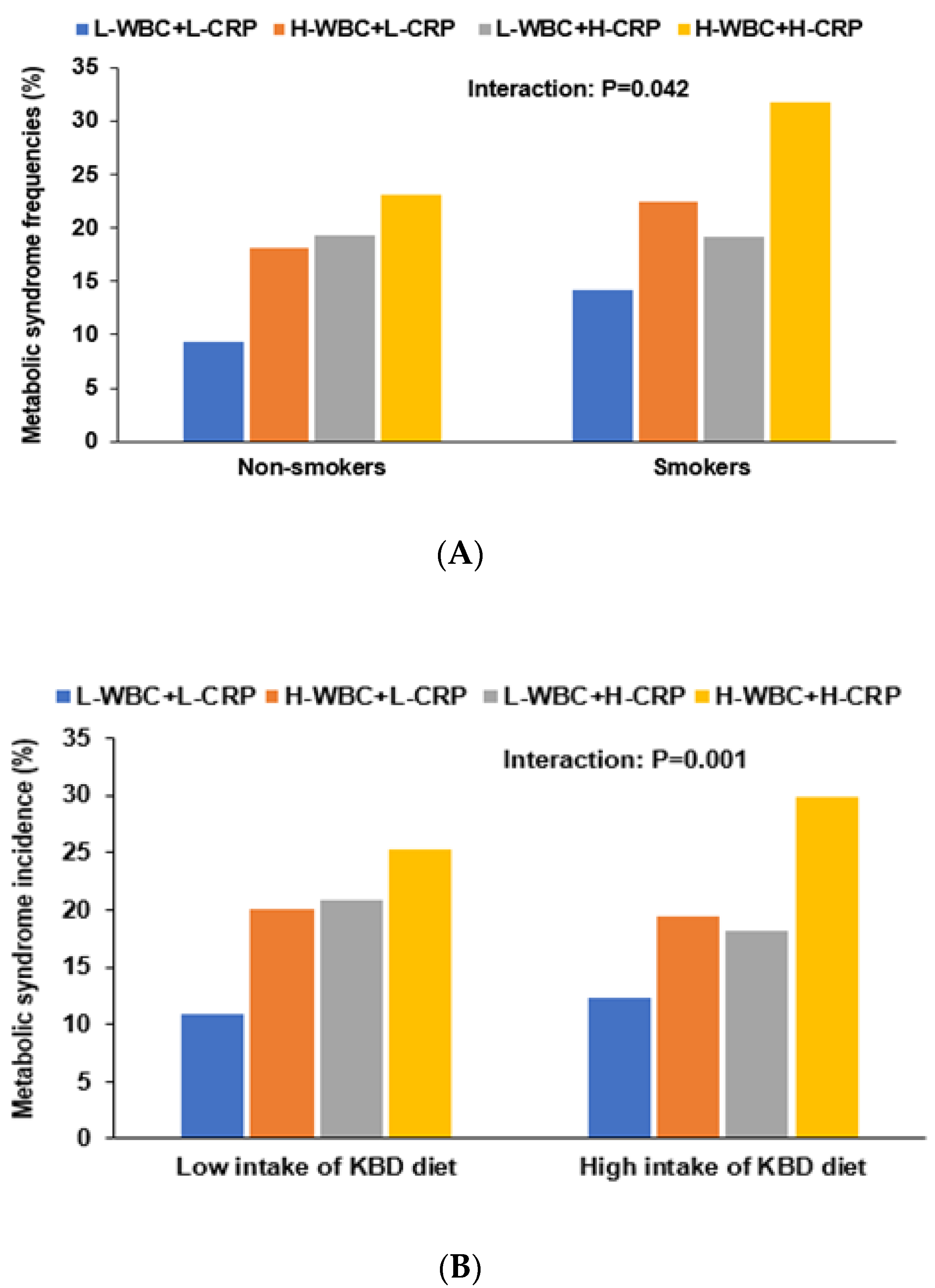
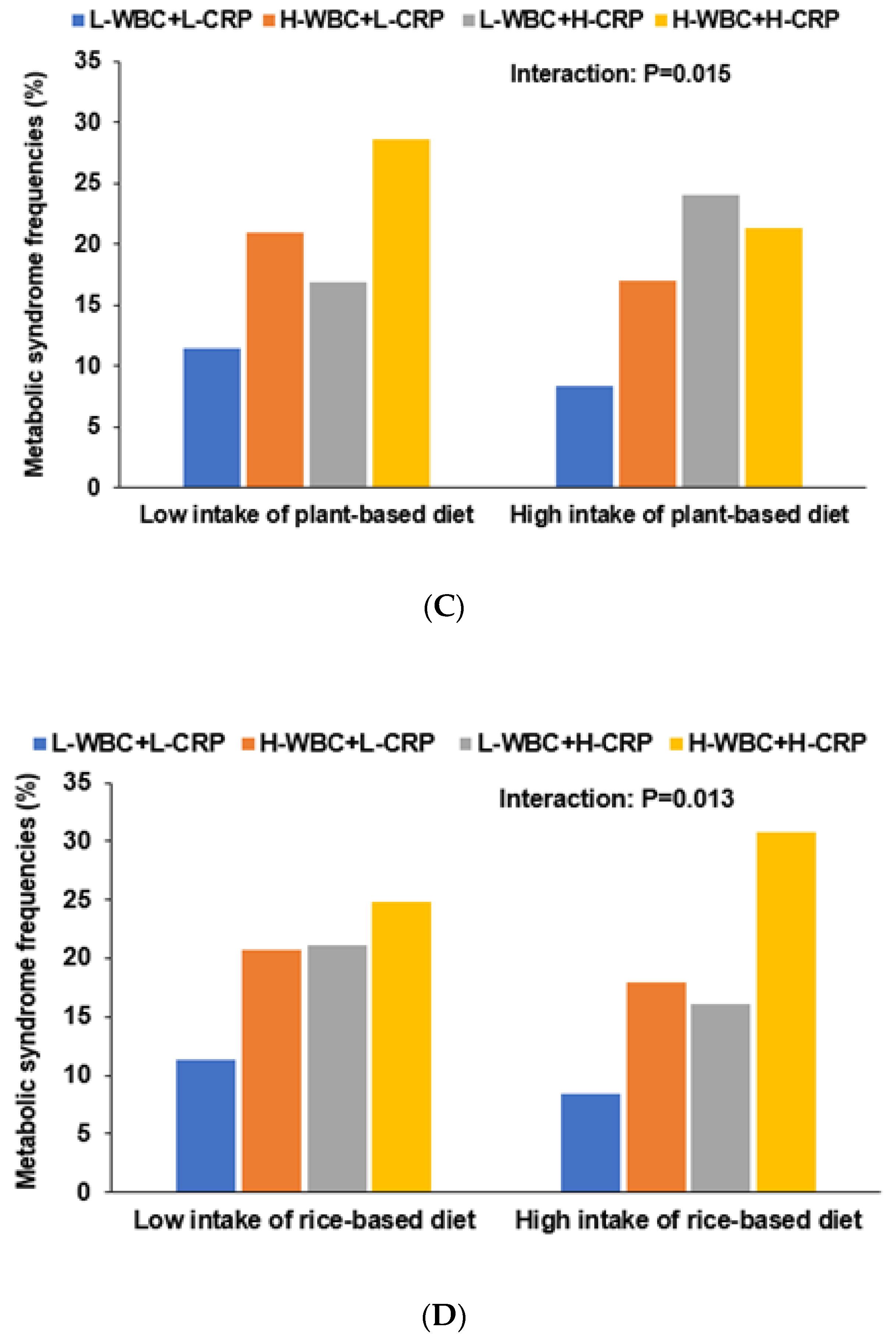
3.5. Interactions of Nutrient Intake and Dietary Patterns with Immunity for Mets Risk
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Tavladaki, T.; Spanaki, A.M.; Dimitriou, H.; Kondili, E.; Choulaki, C.; Georgopoulos, D.; Briassoulis, G. Similar Metabolic, Innate Immunity, and Adipokine Profiles in Adult and Pediatric Sepsis Versus Systemic Inflammatory Response Syndrome—A Pilot Study. Pediatr. Crit. Care Med. 2017, 18, e494–e505. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.J.; Barrientos, R.M. The impact of nutrition on COVID-19 susceptibility and long-term consequences. Brain Behav. Immun. 2020, 87, 53–54. [Google Scholar] [CrossRef] [PubMed]
- Fani, L.; van der Willik, K.D.; Bos, D.; Leening, M.J.G.; Koudstaal, P.J.; Rizopoulos, D.; Ruiter, R.; Stricker, B.H.C.; Kavousi, M.; Ikram, M.A.; et al. The association of innate and adaptive immunity, subclinical atherosclerosis, and cardiovascular disease in the Rotterdam Study: A prospective cohort study. PLoS Med. 2020, 17, e1003115. [Google Scholar] [CrossRef]
- Janeway, C.; Travers, P.; Walport, M.; Capra, D.J. Immunobiology, 5th ed.; Garland Science: New York, NY, USA; London, UK, 2001. [Google Scholar]
- Schloss, M.J.; Swirski, F.K.; Nahrendorf, M. Modifiable Cardiovascular Risk, Hematopoiesis, and Innate Immunity. Circ. Res. 2020, 126, 1242–1259. [Google Scholar] [CrossRef]
- Sonnenberg, G.F.; Hepworth, M.R. Functional interactions between innate lymphoid cells and adaptive immunity. Nat. Rev. Immunol. 2019, 19, 599–613. [Google Scholar] [CrossRef]
- Jung, S.J.; Jung, E.S.; Choi, E.K.; Sin, H.S.; Ha, K.C.; Chae, S.W. Immunomodulatory effects of a mycelium extract of Cordyceps (Paecilomyces hepiali; CBG-CS-2): A randomized and double-blind clinical trial. BMC Complement. Altern. Med. 2019, 19, 77. [Google Scholar] [CrossRef]
- Lee, M.H.; Kim, M.; Kim, M.; Kwak, J.H.; Chang, D.H.; Yu, W.K.; Lee, S.H.; Lee, J.H. Consumption of dairy yogurt with the polysaccharide rhamnogalacturonan from the peel of the Korean citrus hallabong enhances immune function and attenuates the inflammatory response. Food Funct. 2016, 7, 2833–2839. [Google Scholar] [CrossRef]
- Bennett, J.M.; Reeves, G.; Billman, G.E.; Sturmberg, J.P. Inflammation-Nature’s Way to Efficiently Respond to All Types of Challenges: Implications for Understanding and Managing “the Epidemic” of Chronic Diseases. Front. Med. 2018, 5, 316. [Google Scholar] [CrossRef] [Green Version]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Abaspour, A.R.; Taghikhani, M.; Parizadeh, S.M.R.; Seyedi, S.M.R.; Ghazizadeh, H.; Kazemi, E.; Moohebati, M.; Ghafoori, F.; Mardannik, M.; Avan, A.; et al. HSP27 expression in the human peripheral blood mononuclear cells as an early prognostic biomarker in coronary artery disease patients. Diabetes Metab. Syndr. 2019, 13, 1791–1795. [Google Scholar] [CrossRef]
- Young, R.P.; Hopkins, R.J.; Marsland, B. The Gut-Liver-Lung Axis. Modulation of the Innate Immune Response and Its Possible Role in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Cell Mol. Biol. 2016, 54, 161–169. [Google Scholar] [CrossRef]
- Brandsma, E.; Houben, T.; Fu, J.; Shiri-Sverdlov, R.; Hofker, M.H. The immunity-diet-microbiota axis in the development of metabolic syndrome. Curr. Opin. Lipidol. 2015, 26, 73–81. [Google Scholar] [CrossRef]
- Ryu, J.; Lee, C. Association of glycosylated hemoglobin with the gene encoding CDKAL1 in the Korean Association Resource (KARE) study. Hum. Mutat. 2012, 33, 655–659. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Lee, B.K. Self-rated Subjective Health Status Is Strongly Associated with Sociodemographic Factors, Lifestyle, Nutrient Intakes, and Biochemical Indices, but Not Smoking Status: KNHANES 2007–2012. J. Korean Med. Sci. 2015, 30, 1279–1287. [Google Scholar] [CrossRef] [Green Version]
- Daily, J.W.; Park, S. Interaction of BDNF rs6265 variants and energy and protein intake in the risk for glucose intolerance and type 2 diabetes in middle-aged adults. Nutrition 2017, 33, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Daily, J.W.; Zhang, X.; Jin, H.S.; Lee, H.J.; Lee, Y.H. Interactions with the MC4R rs17782313 variant, mental stress and energy intake and the risk of obesity in Genome Epidemiology Study. Nutr. Metab. 2016, 13, 38. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Kim, D.S.; Kang, S. Carrying minor allele of FADS1 and haplotype of FADS1 and FADS2 increased the risk of metabolic syndrome and moderate but not low fat diets lowered the risk in two Korean cohorts. Eur. J. Nutr. 2019, 58, 831–842. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Ahn, J.; Lee, B.K. Very-low-fat diets may be associated with increased risk of metabolic syndrome in the adult population. Clin. Nutr. 2016, 35, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Zhang, X.; Lee, N.R.; Jin, H.S. TRPV1 Gene Polymorphisms Are Associated with Type 2 Diabetes by Their Interaction with Fat Consumption in the Korean Genome Epidemiology Study. J. Nutr. Nutr. 2016, 9, 47–61. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Steel, R.G.; Torrie, J.H.; Dickey, D.A. Principles and Procedures of Statistics: A Biological Approach; McGraw-Hill: New York, NY, USA, 1997. [Google Scholar]
- Kim, J.O.; Mueller, C.W. Factor Analysis. Statistical Methods and Practical Issues; Sage Publications: Thousand Oaks, CA, USA, 1978. [Google Scholar]
- Bianchi, L.; Volpato, S. Muscle dysfunction in type 2 diabetes: A major threat to patient’s mobility and independence. Acta Diabetol. 2016, 53, 879–889. [Google Scholar] [CrossRef]
- Robert, G.D.; Richardson, P.J. Illustrative Logistic Regression Examples Using PROC LOGISTIC: New Features in SAS/STAT® 9.2; SAS Institute: Cary, NC, USA, 2009. [Google Scholar]
- Charles-Messance, H.; Sheedy, F.J. Train to Lose: Innate Immune Memory in Metaflammation. Mol. Nutr. Food Res. 2020, 65, e1900480. [Google Scholar] [CrossRef]
- Mahdiani, A.; Kheirandish, M.; Bonakdaran, S. Correlation Between White Blood Cell Count and Insulin Resistance in Type 2 Diabetes. Curr. Diabetes Rev. 2019, 15, 62–66. [Google Scholar] [CrossRef]
- Płaczkowska, S.; Pawlik-Sobecka, L.; Kokot, I.; Sowiński, D.; Wrzosek, M.; Piwowar, A. Associations between basic indicators of inflammation and metabolic disturbances. Postepy Hig. Med. Dosw. 2014, 68, 1374–1382. [Google Scholar] [CrossRef]
- Yang, H.; Youm, Y.H.; Vandanmagsar, B.; Ravussin, A.; Gimble, J.M.; Greenway, F.; Stephens, J.M.; Mynatt, R.L.; Dixit, V.D. Obesity increases the production of proinflammatory mediators from adipose tissue T cells and compromises TCR repertoire diversity: Implications for systemic inflammation and insulin resistance. J. Immunol. 2010, 185, 1836–1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilainam, P.; Nintasen, R.; Viriyavejakul, P. Mast cell activation in the skin of Plasmodium falciparum malaria patients. Malar. J. 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, G.B.; Gao, P.C.; Chen, Y.Y.; Xia, Y.; Ke, X.S.; Shao, X.F.; Xiong, C.X.; Chen, H.S.; Xiao, H.; Ning, J.; et al. High-Sensitivity C-Reactive Protein Leads to Increased Incident Metabolic Syndrome in Women but Not in Men: A Five-Year Follow-Up Study in a Chinese Population. Diabetes Metab. Syndr. Obes. 2020, 13, 581–590. [Google Scholar] [CrossRef] [Green Version]
- Siedlinski, M.; Jozefczuk, E.; Xu, X.; Teumer, A.; Evangelou, E.; Schnabel, R.B.; Welsh, P.; Maffia, P.; Erdmann, J.; Tomaszewski, M.; et al. White Blood Cells and Blood Pressure: A Mendelian Randomization Study. Circulation 2020, 141, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xiong, C.; Shao, X.; Ning, J.; Gao, P.; Xiao, H.; Chen, Y.; Zou, Z.; Hong, G.; Li, X.; et al. Lymphocyte To High-Density Lipoprotein Ratio As A New Indicator Of Inflammation And Metabolic Syndrome. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2117–2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, H.; Adams-Huet, B.; Smith, G.; Jialal, I. Increased neutrophil count in nascent metabolic syndrome. Metab. Syndr. Relat. Disord. 2013, 11, 128–131. [Google Scholar] [CrossRef]
- Hoyas, I.; Leon-Sanz, M. Nutritional Challenges in Metabolic Syndrome. J. Clin. Med. 2019, 8, 1301. [Google Scholar] [CrossRef] [Green Version]
- Sabaté, J.; Wien, M. A perspective on vegetarian dietary patterns and risk of metabolic syndrome. Br. J. Nutr. 2015, 113 (Suppl. 2), S136–S143. [Google Scholar] [CrossRef] [Green Version]
- Glick-Bauer, M.; Yeh, M.C. The health advantage of a vegan diet: Exploring the gut microbiota connection. Nutrients 2014, 6, 4822–4838. [Google Scholar] [CrossRef] [Green Version]
- Eichelmann, F.; Schwingshackl, L.; Fedirko, V.; Aleksandrova, K. Effect of plant-based diets on obesity-related inflammatory profiles: A systematic review and meta-analysis of intervention trials. Obes. Rev. 2016, 17, 1067–1079. [Google Scholar] [CrossRef]
- Tomova, A.; Bukovsky, I.; Rembert, E.; Yonas, W.; Alwarith, J.; Barnard, N.D.; Kahleova, H. The Effects of Vegetarian and Vegan Diets on Gut Microbiota. Front. Nutr. 2019, 6, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, E.; Gálvez, I.; Martín-Cordero, L. Adrenergic Regulation of Macrophage-Mediated Innate/Inflammatory Responses in Obesity and Exercise in this Condition: Role of β2 Adrenergic Receptors. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Walsh, N.P.; Blannin, A.K.; Robson, P.J.; Gleeson, M. Glutamine, exercise and immune function. Links and possible mechanisms. Sports Med. 1998, 26, 177–191. [Google Scholar] [CrossRef]
- Cerqueira, É.; Marinho, D.A.; Neiva, H.P.; Lourenço, O. Inflammatory Effects of High and Moderate Intensity Exercise—A Systematic Review. Front. Physiol. 2019, 10, 1550. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| L-WBC+L-CRP (n = 25,604) | H-WBC+L-CRP (n = 13,880) | L-WBC+H-CRP (n = 464) | H-WBC+H-CRP (n = 820) | |
|---|---|---|---|---|
| Age (years) | 53.9 ± 7.8 b | 53.2 ± 8.4 c | 55.2 ± 7.9 a | 54.5±8.2 ab *** |
| Gender (Male N, Yes %) | 7234 (28.3) | 6084 (48.8) | 168 (36.2) | 370 (45.1) ††† |
| Physical activity (N, Yes %) | 13,726 (56.4) | 6895 (51.6) | 242 (56.0) | 372 (47.6) ††† |
| Smoker (N, %) | 1541 (6.16) | 2666 (19.7) | 35 (7.79) | 174 (3.96) ††† |
| Metabolic syndrome (N, Yes %) | 2541(10.4) | 2663 (19.8) | 83 (19.4) | 212 (26.7) ††† |
| Obesity (N, %) | 6985 (28.4) | 5209 (38.6) | 168 (39.2) | 356 (44.8) ††† |
| Type 2 diabetes (N, %) | 1722 (7.05) | 1879 (14.0) | 63 (14.5) | 163 (20.8) ††† |
| Hypertension (N, %) | 5157 (21.1) | 3973 (29.7) | 133 (30.6) | 275 (35.4) ††† |
| Cardiovascular disease (N, %) | 894 (3.66) | 635 (4.74) | 20 (4.63) | 40 (5.10) ††† |
| Myocardial infarction (N, Yes %) | 642 (2.63) | 457 (3.41) | 14 (3.24) | 26 (3.32) ††† |
| Stroke (N, %) | 266 (1.09) | 199 (1.48) | 6 (1.39) | 15 (1.91) †† |
| L-WBC+L-CRP (n = 25,604) | H-WBC+L-CRP (n = 13,880) | L-WBC+H-CRP (n = 464) | H-WBC+H-CRP (n = 820) | |
|---|---|---|---|---|
| WBC (109/L) | 4.83 (4.82–4.85) c | 7.18 (7.17–7.20) b | 4.84 (4.54–4.93) c | 7.97 (7.91–8.04) a***# |
| Serum CRP (mg/dL) | 0.08 (0.08–0.08) d | 0.11 (0.10-0.11) c | 1.2 (1.179–1.23) b | 1.39 (1.37–1.41) a***# |
| BMI (kg/m2) | 23.6 (23.6–23.6) c | 24.3 (24.2–24.3) b | 24.3 (24.1–24.6) a | 24.9 (24.7–25.1) a***# |
| Waist circumferences (cm) | 80.2 (80.2–80.3) b | 80.7 (80.7–80.8) a | 80.5 (80.0–80.9) ab | 80.9 (80.6–81.2) a***# |
| Serum glucose (mg/dL) | 94.2 | 96.9 | 97.4 | 100.2 |
| (93.9–94.4) c | (96.6–97.3) b | (95.6–99.2) b | (98.9–102) a***# | |
| Blood HbA1c (%) | 5.64 (5.63–5.65) c | 5.82 (5.81–5.83) b | 5.77 (5.70–5.83) b | 5.96 (5.92–6.01) a***# |
| Serum total cholesterol (mg/dL) | 197 (197–198) b | 200 (199–200) a | 193 (190–196) b | 196 (194–199) b***# |
| Serum HDL (mg/dL) | 55.2 (55.0–55.3) a | 53.5 (53.3–53.8) b | 53.1 (52.0–54.3) b | 52 (51.1–52.8) c***# |
| Serum LDL (mg/dL) | 118 (118–119) | 118 (117–119) | 116 (113–119) | 119 (116–122) |
| Serum TG (mg/dL) | 119 (118–120) b | 140 (138–141) a | 118 (111–126) b | 126 (119–131) b***# |
| SBP (mmHg) | 122 (122–122) b | 124 (123–124) a | 122 (121–123) ab | 123 (122–124) a** |
| DBP (mmHg) | 75.1 (75.0–75.2) b | 75.8 (75.1–76.4) ab | 75.3 (74.5–76.2) ab | 75.9 (75.7–76.1) a** |
| Serum AST | 23.4 | 23.9 | 24.7 | 30.7 |
| (IU/L) | (23.1–23.7) b | (23.4–23.9) b | (22.3–27.0) b | (28.9–32.4) a***# |
| Serum ALT | 21.4 | 22.8 | 23.1 | 27.8 |
| (IU/L) | (21.1–21.8) b | (22.5–23.2) b | (21.0–25.2) b | (26.3–29.4) a***# |
| L-WBC+L-CRP (n = 25,604) | H-WBC+L-CRP (n = 13,880) | L-WBC+H-CRP (n = 464) | H-WBC+H-CRP (n = 820) | |
|---|---|---|---|---|
| Age (≥55 years) | 1 | 0.90 (0.86–0.95) *** | 1.53 (1.23–1.89) *** | 1.21(1.03–1.42) * |
| Gender (Female) | 1 | 0.74 (0.62–0.87) * | 0.09 (0.01–0.70) * | 1.09 (0.70–1.70) |
| Metabolic syndrome (Yes) | 1 | 1.75 (1.64–1.88) *** | 1.37 (1.05–1.81) | 1.86 (1.54–2.24) ** |
| BMI (≥25 kg/m2) | 1 | 1.49 (1.42–1.56) *** | 1.57 (1.29–1.91) *** | 1.87 (1.62–2.17) *** |
| Waist circumference (>90 cm for men; >85 cm for women) | 1 | 1.15 (1.07–1.23) * | 1.09 (0.81–1.46) | 1.03 (0.82–1.29) |
| Plasma glucose (>126 mg/dL) | 1 | 1.94 (1.80–2.09) *** | 1.74 (1.32–2.01) *** | 2.6 (2.15–3.14) *** |
| HbA1c (>7.5% ) | 1 | 2.56 (2.20–2.96) *** | 2.87 (1.80–4.58) *** | 4.72(3.52–6.33) *** |
| Serum total cholesterol (>240 mg/dL) | 1 | 1.26 (1.19–1.32) *** | 0.89 (0.71–1.13) | 1 (0.84–1.19) |
| Serum HDL (40 for men, 50 mg/dL for women) | 1 | 1.3 1.24–1.37) *** | 1.37 (1.11–1.69) * | 1.69 (1.45–1.97) *** |
| Serum LDL (>160 mg/dL) | 1 | 1.2 (1.13–1.27) *** | 1.04 (0.81–1.35) | 1.02 (0.84–1.24) |
| Serum TG (>200 mg/dL) | 1 | 1.55 (1.45–1.66) *** | 1 (0.77–1.30) | 0.95 (0.79–1.15) |
| SBP (>140 mmHg) | 1 | 1.15 (1.09–1.22) *** | 0.94(0.75–1.18) | 1.18 (1.01–1.38) * |
| DBP (>90 mmHg) | 1 | 1.30 (1.19–1.43) *** | 0.98(0.69–1.41) | 1.43 (1.14–1.81) ** |
| Serum ALT (>40 IU) | 1 | 1.38 (1.26–1.50) | 1.61 (1.15–2.24) | 1.32 (1.03–1.69) |
| Serum AST (>40 IU) | 1 | 1.24 (1.11–1.39) | 1.49 (0.98–2.27) | 2.12 (1.63–2.77) *** |
| Physical activity | 1 | 0.82 (0.78–0.85) *** | 0.94 (0.77–1.16) | 0.67 (0.57–0.78) *** |
| L-WBC+L-CRP | H-WBC+L-CRP | L-WBC+H-CRP | H-WBC+H-CRP | |
|---|---|---|---|---|
| (n = 25,604) | (n = 13,880) | (n = 464) | (n = 820) | |
| Energy (% EER) | 96.0 ± 0.19 | 96.1 ± 0.26 | 92.7 ± 1.41 | 95.2 ± 1.06 |
| CHO (% En) | 71.7 ± 0.04 a | 71.4 ± 0.06 b | 71.5 ± 0.32 ab | 71.5 ± 0.24 ab** |
| Fat (% En) | 13.9 ± 0.03 b | 14.2 ± 0.05 a | 14.1 ± 0.25 ab | 14.0 ± 0.19 ab** |
| Protein (% En) | 13.3 ± 0.02 | 13.4 ± 0.02 | 13.4 ± 0.12 | 13.4 ± 0.09 |
| V-A (μg RE) | 476 ±2.13 | 477 ± 2.92 | 460 ± 15.6 | 459 ± 11.7 |
| Carotene (mg) | 2362 ± 11.5 | 2367 ± 15.8 | 2262 ± 84.1 | 2280 ± 63.2 |
| V-C (mg) | 104 ± 0.41 a | 102 ± 0.56 b | 98.4 ± 2.99 ab | 97.9 ± 2.25 ab* |
| Fiber (g) | 5.65 ± 0.02 a | 5.61 ± 0.02 b | 5.33 ± 0.13 ab | 5.41 ± 0.10 ab* |
| Coffee (cups/week) | 3.7 ± 0.02 b | 3.9 ± 0.03 a | 3.5 ± 0.14 b | 3.9 ± 0.10 a*** |
| Alcohol (g) | 17.4 ± 0.31 a | 14.9 ± 0.42 b | 16.6 ± 2.24 a | 15.8 ± 1.69 ab* |
| KBD (scores) | −0.033 ± 0.006 | −0.014 ± 0.008 | −0.089 ± 0.044 | −0.029 ± 0.034 |
| PBD (scores) | 0.022 ± 0.006 a | −0.011 ± 0.008 b | −0.002 ± 0.045 ab | −0.084 ± 0.033 c** |
| WSD (scores) | 0.005 ± 0.006 c | 0.043 ± 0.009 b | 0.045 ±0.046 ab | 0.061 ± 0.035 a* |
| RBD (scores) | −0.001 ± 0.006 b | 0.021 ± 0.009 a | 0.068 ± 0.047 ab | 0.058 ± 0.035 ab* |
| L-WBC+L-CRP (n = 25,604) | H-WBC+L-CRP (n = 13,880) | L-WBC+H-CRP (n = 464) | H-WBC+H-CRP (n = 820) | Immunity, Lifestyle, and Diet Interaction | |
|---|---|---|---|---|---|
| Low physical activity | 1 | 1.805 (1.637–1.990) * | 1.628 (1.105–2.398) | 2.057 (1.582–2.675) * | 0.650 1 |
| High physical activity | 1 | 1.835 (1.677–2.008) ** | 1.396 (0.955–2.039) | 2.047 (1.561–2.684) ** | |
| Non-smokers | 1 | 1.86 | 1.59 | 1.64 | 0.042 |
| (1.71–2.02) *** | (1.16–2.16) | (1.28–2.12) | 0.081 2 | ||
| Smokers | 1 | 1.71 | 1.45 | 2.35 | |
| (1.52–1.91) | (0.90–2.35) | (1.77–3.11) *** | |||
| Low intake of a KBD | 1 | 1.94 | 1.49 | 1.86 | 0.001 |
| (1.79–2.11) *** | (1.08–2.05) | (1.47–2.34) * | 0.003 | ||
| High intake of a KBD | 1 | 1.39 | 1.11 | 1.84 | |
| (1.23–1.57) | (0.65–1.92) | (1.31–2.57) * | |||
| Low intake of plant-based diet | 1 | 1.79 | 1.25 | 2.04 | 0.015 |
| (1.66–1.94) *** | (0.89–1.75) | (1.65–2.52) *** | 0.045 | ||
| High intake of a plant-based diet | 1 | 1.48 | 1.66 | 1.03 | |
| (1.07–1.92) | (1.04–2.65) | (0.67–1.59) | |||
| Low intake of | 1 | 1.77 | 1.59 | 1.53 | 0.013 |
| rice-based diet | (1.63–1.91) *** | (1.16–2.18) | (1.22–1.94) | 0.039 | |
| High intake of | 1 | 1.95 | 1.53 | 3.13 | |
| rice-based diet | (1.73–2.21) | (0.95–2.44) | (2.29–4.29) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Zhang, T. A Positive Association of Overactivated Immunity with Metabolic Syndrome Risk and Mitigation of Its Association by a Plant-Based Diet and Physical Activity in a Large Cohort Study. Nutrients 2021, 13, 2308. https://doi.org/10.3390/nu13072308
Park S, Zhang T. A Positive Association of Overactivated Immunity with Metabolic Syndrome Risk and Mitigation of Its Association by a Plant-Based Diet and Physical Activity in a Large Cohort Study. Nutrients. 2021; 13(7):2308. https://doi.org/10.3390/nu13072308
Chicago/Turabian StylePark, Sunmin, and Ting Zhang. 2021. "A Positive Association of Overactivated Immunity with Metabolic Syndrome Risk and Mitigation of Its Association by a Plant-Based Diet and Physical Activity in a Large Cohort Study" Nutrients 13, no. 7: 2308. https://doi.org/10.3390/nu13072308