
Association of Daily Physical Activity and Sedentary Behaviour with Protein Intake Patterns in Older Adults: A Multi-Study Analysis across Five Countries

 , ,
, ,  , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Dietary Intake
2.3. Protein Intake
2.4. Physical Activity
2.5. Sedentary Behaviour
2.6. Socioeconomic, Lifestyle, and Health Factors
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Physical Activity and Protein Intake
3.3. Physical Activity and Number of Eating Occasions Providing Protein
3.4. Physical Activity and Reaching Protein Thresholds
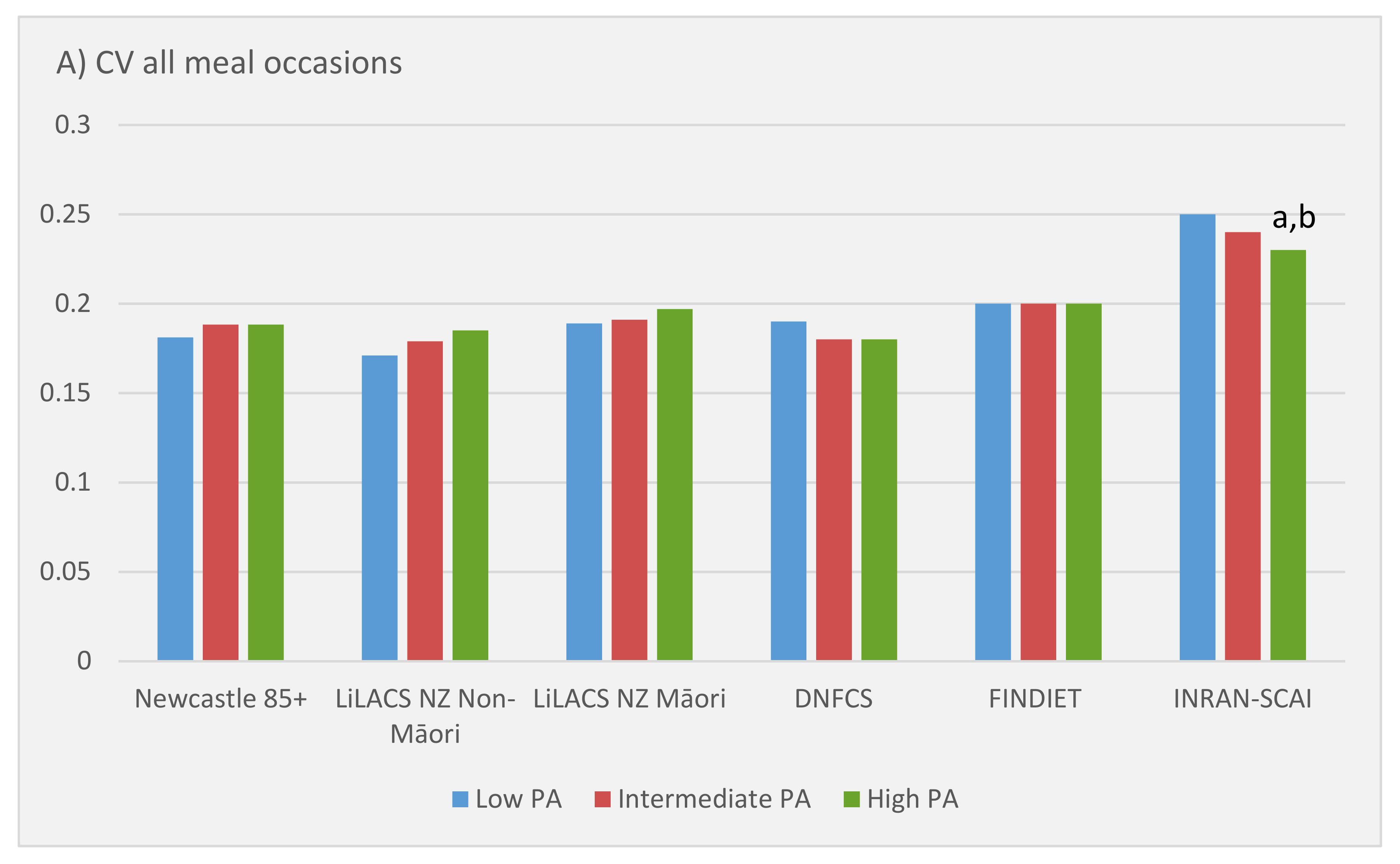
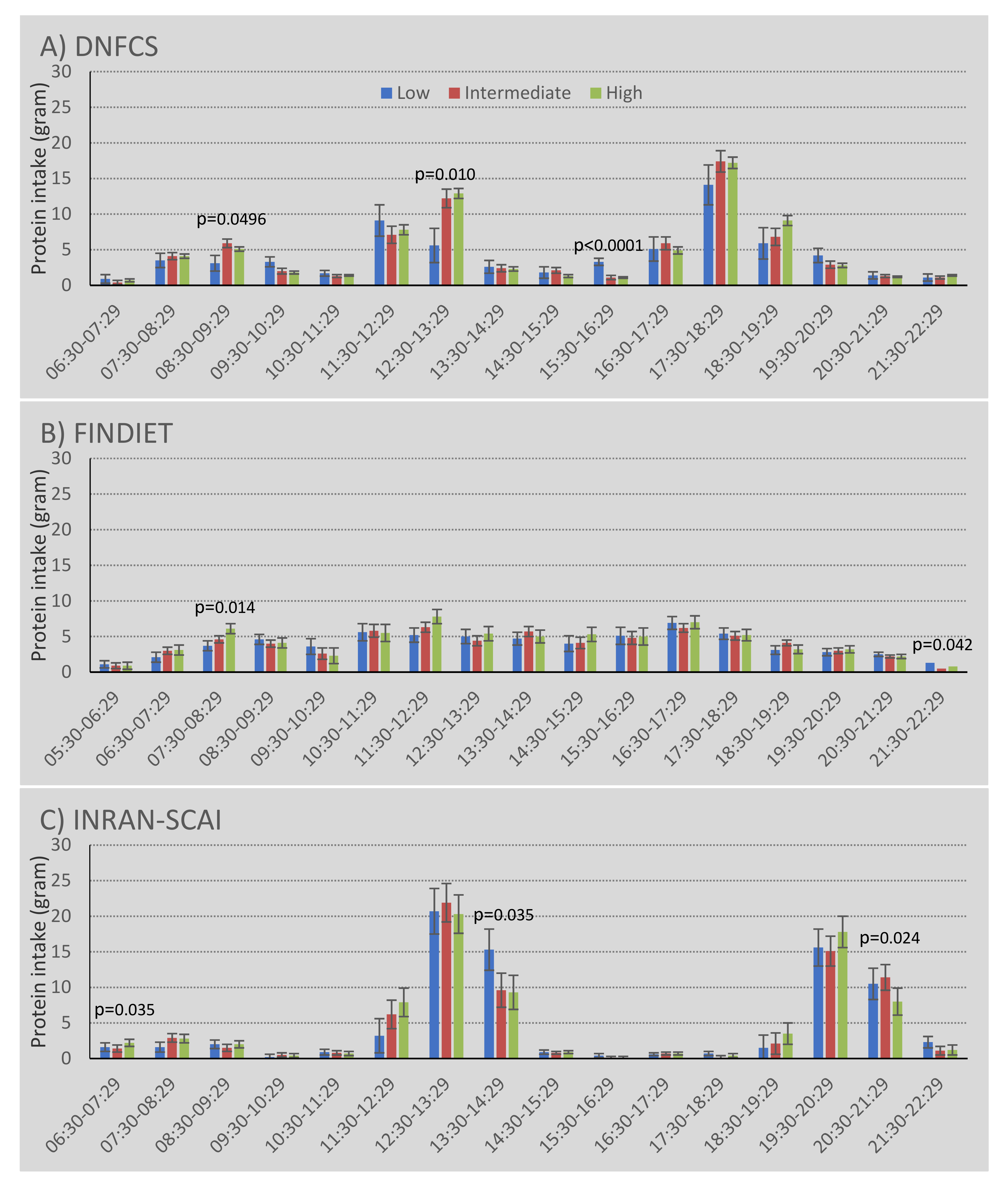
3.5. Physical Activity and Pattern of Protein Intake over the Day
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vandewoude, M.F.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-sarcopenia syndrome: Is this the future of nutrition screening and assessment for older adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef]
- Granic, A.; Mendonça, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Adamson, A.; Siervo, M.; Mathers, J.C.; Jagger, C. Low protein intake, muscle strength and physical performance in the very old: The Newcastle 85+ Study. Clin. Nutr. 2018, 37, 2260–2270. [Google Scholar] [CrossRef] [Green Version]
- Granic, A.; Mendonça, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Siervo, M.; Mathers, J.C.; Jagger, C. Effects of dietary patterns and low protein intake on sarcopenia risk in the very old: The Newcastle 85+ study. Clin. Nutr. 2020, 39, 166–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendonça, N.; Granic, A.; Hill, T.R.; Siervo, M.; Mathers, J.C.; Kingston, A.; Jagger, C. Protein intake and disability trajectories in very old adults: The Newcastle 85+ Study. J. Am. Geriatr. Soc. 2019, 67, 50–56. [Google Scholar] [CrossRef]
- Mendonça, N.; Kingston, A.; Granic, A.; Hill, T.R.; Mathers, J.C.; Jagger, C. Contribution of protein intake and its interaction with physical activity to transitions between disability states and to death in very old adults: The Newcastle 85+ Study. Eur. J. Nutr. 2019, 59, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendonça, N.; Kingston, A.; Granic, A.; Jagger, C. Protein intake and transitions between frailty states and to death in very old adults: The Newcastle 85+ study. Age Ageing 2020, 49, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Shakersain, B.; Santoni, G.; Faxen-Irving, G.; Rizzuto, D.; Fratiglioni, L.; Xu, W. Nutritional status and survival among old adults: An 11-year population-based longitudinal study. Eur. J. Clin. Nutr. 2016, 70, 320–325. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deer, R.R.; Volpi, E. Protein intake and muscle function in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 248. [Google Scholar] [CrossRef] [Green Version]
- Bouillanne, O.; Curis, E.; Hamon-Vilcot, B.; Nicolis, I.; Chrétien, P.; Schauer, N.; Vincent, J.P.; Cynober, L.; Aussel, C. Impact of protein pulse feeding on lean mass in malnourished and at-risk hospitalized elderly patients: A randomized controlled trial. Clin. Nutr. 2013, 32, 186–192. [Google Scholar] [CrossRef]
- Mamerow, M.M.; Mettler, J.A.; English, K.L.; Casperson, S.L.; Arentson-Lantz, E.; Sheffield-Moore, M.; Layman, D.K.; Paddon-Jones, D. Dietary protein distribution positively influences 24-h muscle protein synthesis in healthy adults. J. Nutr. 2014, 144, 876–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farsijani, S.; Morais, J.A.; Payette, H.; Gaudreau, P.; Shatenstein, B.; Gray-Donald, K.; Chevalier, S. Relation between mealtime distribution of protein intake and lean mass loss in free-living older adults of the NuAge study. Am. J. Clin. Nutr. 2016, 104, 694–703. [Google Scholar] [CrossRef]
- Chou, C.-H.; Hwang, C.-L.; Wu, Y.-T. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: A meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Broccatelli, M.; Savera, G.; D’Elia, M.; Pahor, M.; et al. Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 35–42. [Google Scholar] [CrossRef]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef]
- Areta, J.L.; Burke, L.M.; Ross, M.L.; Camera, D.M.; West, D.W.; Broad, E.M.; Jeacocke, N.A.; Moore, D.R.; Stellingwerff, T.; Phillips, S.M.; et al. Timing and distribution of protein ingestion during prolonged recovery from resistance exercise alters myofibrillar protein synthesis. J. Physiol. 2013, 591, 2319–2331. [Google Scholar] [CrossRef]
- Moore, D.R.; Robinson, M.J.; Fry, J.L.; Tang, J.E.; Glover, E.I.; Wilkinson, S.B.; Prior, T.; Tarnopolsky, M.A.; Phillips, S.M. Ingested protein dose response of muscle and albumin protein synthesis after resistance exercise in young men. Am. J. Clin. Nutr. 2009, 89, 161–168. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Aragon, A.A.; Krieger, J.W. The effect of protein timing on muscle strength and hypertrophy: A meta-analysis. J. Int. Soc. Sports Nutr. 2013, 10, 53. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.E.; Snijders, T.; Zulyniak, M.; Kumbhare, D.; Parise, G.; Chabowski, A.; Phillips, S.M. A whey protein-based multi-ingredient nutritional supplement stimulates gains in lean body mass and strength in healthy older men: A randomized controlled trial. PLoS ONE 2017, 12, e0181387. [Google Scholar] [CrossRef] [Green Version]
- Björkman, M.P.; Suominen, M.H.; Kautiainen, H.; Jyväkorpi, S.K.; Finne-Soveri, H.U.; Strandberg, T.E.; Pitkälä, K.H.; Tilvis, R.S. Effect of Protein Supplementation on Physical Performance in Older People With Sarcopenia–A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 21, 226–232. [Google Scholar] [CrossRef]
- Markofski, M.M.; Jennings, K.; Timmerman, K.L.; Dickinson, J.M.; Fry, C.S.; Borack, M.S.; Reidy, P.T.; Deer, R.R.; Randolph, A.; Rasmussen, B.B.; et al. Effect of Aerobic Exercise Training and Essential Amino Acid Supplementation for 24 Weeks on Physical Function, Body Composition, and Muscle Metabolism in Healthy, Independent Older Adults: A Randomized Clinical Trial. J. Gerontol. Ser. A 2019, 74, 1598–1604. [Google Scholar] [CrossRef]
- Seino, S.; Sumi, K.; Narita, M.; Yokoyama, Y.; Ashida, K.; Kitamura, A.; Shinkai, S. Effects of low-dose dairy protein plus micronutrient supplementation during resistance exercise on muscle mass and physical performance in older adults: A randomized, controlled trial. J. Nutr. Health Aging 2018, 22, 59–67. [Google Scholar] [CrossRef]
- Collerton, J.; Davies, K.; Jagger, C.; Kingston, A.; Bond, J.; Eccles, M.P.; Robinson, L.A.; Martin-Ruiz, C.; von Zglinicki, T.; James, O.F.; et al. Health and disease in 85 year olds: Baseline findings from the Newcastle 85+ cohort study. BMJ 2009, 339, b4904. [Google Scholar] [CrossRef] [Green Version]
- Davies, K.; Kingston, A.; Robinson, L.; Hughes, J.; Hunt, J.M.; Barker, S.A.; Edwards, J.; Collerton, J.; Jagger, C.; Kirkwood, T.B. Improving retention of very old participants in longitudinal research: Experiences from the Newcastle 85+ study. PLoS ONE 2014, 9, e108370. [Google Scholar] [CrossRef] [Green Version]
- Dyall, L.; Kepa, M.; Hayman, K.; Teh, R.; Moyes, S.; Broad, J.B.; Kerse, N. Engagement and recruitment of Māori and non-Māori people of advanced age to LiLACS NZ. Aust. N. Z. J. Public Health 2013, 37, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Kerse, N.; Teh, R.; Moyes, S.A.; Broad, J.; Rolleston, A.; Gott, M.; Kepa, M.; Wham, C.; Hayman, K.; Jatrana, S.; et al. Cohort Profile: Te Puawaitanga o Nga Tapuwae Kia Ora Tonu, Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ). Int. J. Epidemiol. 2015, 44, 1823–1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocke, M.C. Diet of Community-Dwelling Older Adults: Dutch National Food Consumption Survey Older Adults 2010–2012; National Institute for Public Health and the Environment: Utrecht, The Netherlands, 2013.
- Pietinen, P.; Paturi, M.; Reinivuo, H.; Tapanainen, H.; Valsta, L.M. FINDIET 2007 Survey: Energy and nutrient intakes. Public Health Nutr. 2010, 13, 920–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinivuo, H.; Hirvonen, T.; Ovaskainen, M.L.; Korhonen, T.; Valsta, L.M. Dietary survey methodology of FINDIET 2007 with a risk assessment perspective. Public Health Nutr. 2010, 13, 915–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclercq, C.; Arcella, D.; Piccinelli, R.; Sette, S.; Le Donne, C. The Italian National Food Consumption Survey INRAN-SCAI 2005–06: Main results in terms of food consumption. Public Health Nutr. 2009, 12, 2504–2532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendonça, N.; Hill, T.R.; Granic, A.; Davies, K.; Collerton, J.; Mathers, J.C.; Siervo, M.; Wrieden, W.L.; Seal, C.J.; Kirkwood, T.B.; et al. Macronutrient intake and food sources in the very old: Analysis of the Newcastle 85+ Study. Br. J. Nutr. 2016, 115, 2170–2180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wham, C.; Teh, R.; Moyes, S.A.; Rolleston, A.; Muru-Lanning, M.; Hayman, K.; Adamson, A.; Kerse, N. Macronutrient intake in advanced age: Te Puawaitanga o Nga Tapuwae Kia ora Tonu, Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ). Br. J. Nutr. 2016, 116, 1103–1115. [Google Scholar] [CrossRef] [Green Version]
- Sette, S.; Le Donne, C.; Piccinelli, R.; Arcella, D.; Turrini, A.; Leclercq, C. The third Italian national food consumption survey, INRAN-SCAI 2005–06–part 1: Nutrient intakes in Italy. Nutrition. Metab. Cardiovasc. Dis. 2011, 21, 922–932. [Google Scholar] [CrossRef]
- Sette, S.; Le Donne, C.; Piccinelli, R.; Arcella, D.; Turrini, A.; Leclercq, C.; INRAN-SCAI 2005–06 Study Group. The third National Food Consumption Survey, INRAN-SCAI 2005–06: Major dietary sources of nutrients in Italy. Int. J. Food Sci. Nutr. 2013, 64, 1014–1021. [Google Scholar] [CrossRef]
- European Food Safety Authority. Dietary Reference Values for Nutrients Summary Report; EFSA Supporting Publications: Parma, Italy, 2017; Volume 14, p. e15121. 98p. [Google Scholar] [CrossRef] [Green Version]
- Berner, L.A.; Becker, G.; Wise, M.; Doi, J. Characterization of dietary protein among older adults in the United States: Amount, animal sources, and meal patterns. J. Acad. Nutr. Diet. 2013, 113, 809–815. [Google Scholar] [CrossRef]
- Innerd, P.; Catt, M.; Collerton, J.; Davies, K.; Trenell, M.; Kirkwood, T.B.; Jagger, C. A comparison of subjective and objective measures of physical activity from the Newcastle 85+ study. Age Ageing 2015, 44, 691–694. [Google Scholar] [CrossRef] [Green Version]
- Washburn, R.A.; McAuley, E.; Katula, J.; Mihalko, S.L.; Boileau, R.A. The Physical Activity Scale for the Elderly (PASE): Evidence for Validity. J. Clin. Epidemiol. 1999, 52, 643–651. [Google Scholar] [CrossRef]
- Loland, N. Reliability of the physical activity scale for the elderly (PASE). Eur. J. Sport Sci. 2002, 2, 1–12. [Google Scholar] [CrossRef]
- Wendel-Vos, G.W.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Lincoln, N.B.; Gladman, J.R. The Extended Activities of Daily Living scale: A further validation. Disabil. Rehabil. 1992, 14, 41–43. [Google Scholar] [CrossRef]
- StataCorp, L. Stata Statistical Software: Release 15; StataCorp LP: College Station, TX, USA, 2017. [Google Scholar]
- Campbell, W.W.; Crim, M.C.; Young, V.R.; Evans, W.J. Increased energy requirements and changes in body composition with resistance training in older adults. Am. J. Clin. Nutr. 1994, 60, 167–175. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia: Protein, amino acid metabolism and therapy. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86. [Google Scholar] [CrossRef] [Green Version]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Distribution but not amount of protein intake is associated with frailty: A cross-sectional investigation in the region of Nürnberg. Nutr. J. 2013, 12, 109. [Google Scholar] [CrossRef] [Green Version]
- Kang, L.; Gao, Y.; Liu, X.; Liang, Y.; Chen, Y.; Liang, Y.; Zhang, L.; Chen, W.; Pang, H.; Peng, L.N. Effects of whey protein nutritional supplement on muscle function among community-dwelling frail older people: A multicenter study in China. Arch. Gerontol. Geriatr. 2019, 83, 7–12. [Google Scholar] [CrossRef]
- Chalé, A.; Cloutier, G.J.; Hau, C.; Phillips, E.M.; Dallal, G.E.; Fielding, R.A. Efficacy of whey protein supplementation on resistance exercise–induced changes in lean mass, muscle strength, and physical function in mobility-limited older adults. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2013, 68, 682–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Suzuki, T.; Saito, K.; Kojima, N.; Hosoi, E.; Yoshida, H. Long-term effects of exercise and amino acid supplementation on muscle mass, physical function and falls in community-dwelling elderly J apanese sarcopenic women: A 4-year follow-up study. Geriatr. Gerontol. Int. 2016, 16, 175–181. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Physical Activity Level | ||||
|---|---|---|---|---|
| Low | Intermediate | High | p-Value | |
| Newcastle 85+ Study * (n = 721) | n = 184 | n = 335 | n = 202 | |
| Protein intake—grams/day | 59.4 ± 1.6 | 63.8 ± 1.1 | 68.7 ± 1.4 | 0.0001 |
| Protein intake—g/kg/aBW/day | 0.94 ± 0.03 | 0.99 ± 0.02 | 1.07 ± 0.02 | 0.0003 |
| LiLACS NZ Non-Māori * (n = 353) | n = 123 | n = 120 | n = 110 | |
| Protein intake—grams/day | 56.6 ± 2.1 | 56.4 ± 2.0 | 60.8 ± 2.0 | 0.212 |
| Protein intake—g/kg/aBW/day | 1.1 ± 0.03 | 1.0 ± 0.03 | 1.1 ± 0.03 | 0.181 |
| LiLACS NZ Māori * (n = 183) | n = 58 | n = 57 | n = 68 | |
| Protein intake—grams/day | 52.4 ± 4.8 | 51.1 ± 4.6 | 66.0 ± 4.1 | 0.031 |
| Protein intake—g/kg/aBW/day | 1.1 ± 0.10 | 1.1 ± 0.09 | 1.3 ± 0.08 | 0.334 |
| DNFCS † (n = 1476) | n = 64 | n = 252 | n = 1160 | |
| Protein intake—grams/day | 68.7 ± 3.3 | 75.1 ± 1.8 | 76.5 ± 1.0 | 0.055 |
| Protein intake—g/kg/aBW/day | 0.94 ± 0.05 | 1.05 ± 0.03 | 1.07 ± 0.01 | 0.044 |
| FINDIET † (n = 1734) | n = 286 | n = 1088 | n = 360 | |
| Protein intake—grams/day | 67.5 ± 2.4 | 68.2± 1.7 | 72.5 ± 2.3 | 0.085 |
| Protein intake—g/kg/aBW/day | 0.97 ± 0.03 | 0.99 ± 0.02 | 1.06 ± 0.03 | 0.039 |
| INRAN-SCAI † (n = 1530) | n = 201 | n = 642 | n = 687 | |
| Protein intake—grams/day | 79.1 ± 3.3 | 77.8 ± 2.7 | 79.3 ± 2.8 | 0.73 |
| Protein intake—g/kg/aBW/day | 1.16 ± 0.05 | 1.15 ± 0.04 | 1.18 ± 0.04 | 0.70 |
| Physical Activity Level | |||
|---|---|---|---|
| Low | Intermediate | High | |
| Newcastle 85+ Study | |||
| OR (95% CI) | |||
| Model 1 | 0.86 (0.62–1.20) | 1.0 (Ref) | 1.53 (1.10–2.13) |
| Model 2 | 0.88 (0.61–1.25) | 1.0 (Ref) | 1.54 (1.10–2.14) |
| Model 3 | 0.91 (0.64–1.31) | 1.0 (Ref) | 1.45 (1.03–2.03) |
| Model 4 | 0.93 (0.62–1.39) | 1.0 (Ref) | 1.33 (0.93–1.90) |
| LiLACS NZ Non-Māori | |||
| OR (95% CI) | |||
| Model 1 | 1.03 (0.64–1.67) | 1.0 (Ref) | 1.68 (1.01–2.79) |
| Model 2 | 1.41 (0.83–2.41) | 1.0 (Ref) | 1.95 (1.15–3.33) |
| Model 3 | 1.42 (0.83–2.43) | 1.0 (Ref) | 1.89 (1.11–3.23) |
| Model 4 | 1.45 (0.82–2.57) | 1.0 (Ref) | 1.88 (1.06–3.32) |
| LiLACS NZ Māori | |||
| OR (95% CI) | |||
| Model 1 | 0.86 (0.44–1.70) | 1.0 (Ref) | 0.76 (0.39–1.49) |
| Model 2 | 0.86 (0.39–1.89) | 1.0 (Ref) | 0.83 (0.39–1.76) |
| Model 3 | 0.83 (0.37–1.85) | 1.0 (Ref) | 0.74 (0.34–1.61) |
| Model 4 | 0.77 (0.32–1.87) | 1.0 (Ref) | 0.81 (0.36–1.82) |
| Physical Activity Level | ||||
|---|---|---|---|---|
| Low | Intermediate | High | p-Value | |
| DNFCS * (n = 1476 days) | ||||
| Number of eating occasions | ||||
| Model 1 | 5.4 (0.10) | 5.6 (0.05) | 5.6 (0.02) | 0.057 |
| Model 2 | 5.4 (0.10) | 5.5 (0.06) | 5.6 (0.03) | 0.070 |
| Model 3 | 5.4 (0.10) | 5.6 (0.06) | 5.6 (0.03) | 0.16 |
| Exclusion special days | 5.4 (0.11) | 5.6 (0.05) | 5.6 (0.03) | 0.22 |
| Exclusion special diets | 5.4 (0.12 | 5.6 (0.06) | 5.6 (0.03) | 0.25 |
| FINDIET * (n = 1734 days) | ||||
| Number of eating occasions | ||||
| Model 1 | 4.4 (0.06) | 4.5 (0.03) | 4.6 (0.05) | 0.0081 |
| Model 2 | 4.3 (0.07) | 4.4 (0.05) | 4.5 (0.07) | 0.032 |
| Model 3 | 4.3 (0.07) | 4.4 (0.05) | 4.5 (0.07) | 0.046 |
| Exclusion special days | 4.3 (0.07) | 4.5 (0.05) | 4.5 (0.07) | 0.031 |
| Exclusion special diets | N/A | N/A | N/A | N/A |
| INRAN-SCAI * (n = 1530 days) | ||||
| Number of eating occasions | ||||
| Model 1 | 3.8 (0.11) | 3.8 (0.06) | 4.1 (0.06) | 0.0078 |
| Model 2 | 3.8 (0.15) | 3.9 (0.12) | 4.1 (0.12) | 0.012 |
| Model 3 | 3.8 (0.14) | 3.9 (0.12) | 4.1 (0.12) | 0.021 |
| Exclusion special days | 3.8 (0.15) | 3.8 (0.12) | 4.0 (0.13) | 0.062 |
| Exclusion special diets | 3.9 (0.15) | 3.9 (0.12) | 4.1 (0.12) | 0.047 |
| Physical Activity Level | ||||
|---|---|---|---|---|
| Low | Intermediate | High | p-Value | |
| DNFCS (n = 1476 days) | n = 64 | n = 252 | n = 1160 | |
| ≥2 eating occasions >20 g protein (%) | 28.0 (13.7–42.2) | 43.3 (35.7–50.9) | 49.9 (45.7–54.2) | 0.0043 |
| ≥2 eating occasions >30 g protein (%) | 1.9 (−6.1–9.9) | 7.7 (3.5–12.0) | 9.8 (7.4–12.2) | 0.12 |
| ≥2 main meals >20 g protein (%) | 20.5 (6.2–34.8) | 41.5 (33.9–49.1) | 46.0 (41.7–50.3) | 0.0018 |
| ≥2 main meals >30 g protein (%) | 1.6 (−6.2–9.4) | 6.0 (1.9–10.2) | 9.0 (6.7–11.3) | 0.089 |
| FINDIET (n = 1734 days) | n = 286 | n = 1088 | n = 360 | |
| ≥2 eating occasions >20 g protein (%) | 37.3 (29.4–45.1) | 39.0 (33.4–44.6) | 38.0 (30.3–45.7) | 0.88 |
| ≥2 eating occasions >30 g protein (%) | 13.6 (8.4–18.9) | 11.9 (8.2–15.7) | 14.6 (9.5–19.7) | 0.47 |
| ≥2 main meals >20 g protein (%) | 27.2 (19.8–34.6) | 28.3 (23.1–33.6) | 27.6 (20.4–34.8) | 0.94 |
| ≥2 main meals >30 g protein (%) | 9.2 (4.60–13.8) | 8.4 (5.2–11.7) | 8.5 (4.1–13.0) | 0.95 |
| INRAN-SCAI (n = 1530 days) | n = 201 | n = 642 | n = 687 | |
| ≥2 eating occasions >20 g protein (%) | 58.2 (47.3–69.1) | 56.7 (47.7–65.7) | 62.0 (52.8–71.2) | 0.24 |
| ≥2 eating occasions >30 g protein (%) | 28.5 (18.1–38.9) | 30.1 (21.5–38.7) | 31.8 (21.5–38.7) | 0.73 |
| ≥2 main meals >20 g protein (%) | 57.3 (46.3–68.3) | 56.6 (47.5–65.7) | 61.9 (52.6–71.2) | 0.23 |
| ≥2 main meals >30 g protein | 28.5 (18.0–38.9) | 29.9 (21.3–38.6) | 31.6 (22.8–40.4) | 0.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lourida, I.; Boer, J.M.A.; Teh, R.; Kerse, N.; Mendonça, N.; Rolleston, A.; Sette, S.; Tapanainen, H.; Turrini, A.; Virtanen, S.M.; et al. Association of Daily Physical Activity and Sedentary Behaviour with Protein Intake Patterns in Older Adults: A Multi-Study Analysis across Five Countries. Nutrients 2021, 13, 2574. https://doi.org/10.3390/nu13082574
Lourida I, Boer JMA, Teh R, Kerse N, Mendonça N, Rolleston A, Sette S, Tapanainen H, Turrini A, Virtanen SM, et al. Association of Daily Physical Activity and Sedentary Behaviour with Protein Intake Patterns in Older Adults: A Multi-Study Analysis across Five Countries. Nutrients. 2021; 13(8):2574. https://doi.org/10.3390/nu13082574
Chicago/Turabian StyleLourida, Ilianna, Jolanda M. A. Boer, Ruth Teh, Ngaire Kerse, Nuno Mendonça, Anna Rolleston, Stefania Sette, Heli Tapanainen, Aida Turrini, Suvi M. Virtanen, and et al. 2021. "Association of Daily Physical Activity and Sedentary Behaviour with Protein Intake Patterns in Older Adults: A Multi-Study Analysis across Five Countries" Nutrients 13, no. 8: 2574. https://doi.org/10.3390/nu13082574
APA StyleLourida, I., Boer, J. M. A., Teh, R., Kerse, N., Mendonça, N., Rolleston, A., Sette, S., Tapanainen, H., Turrini, A., Virtanen, S. M., Visser, M., & Jagger, C. (2021). Association of Daily Physical Activity and Sedentary Behaviour with Protein Intake Patterns in Older Adults: A Multi-Study Analysis across Five Countries. Nutrients, 13(8), 2574. https://doi.org/10.3390/nu13082574