
Impact of a Prenatal Vitamin D Supplementation Program on Vitamin D Deficiency, Rickets and Early Childhood Caries in an Alaska Native Population

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Design
2.3. Data Analysis
3. Results
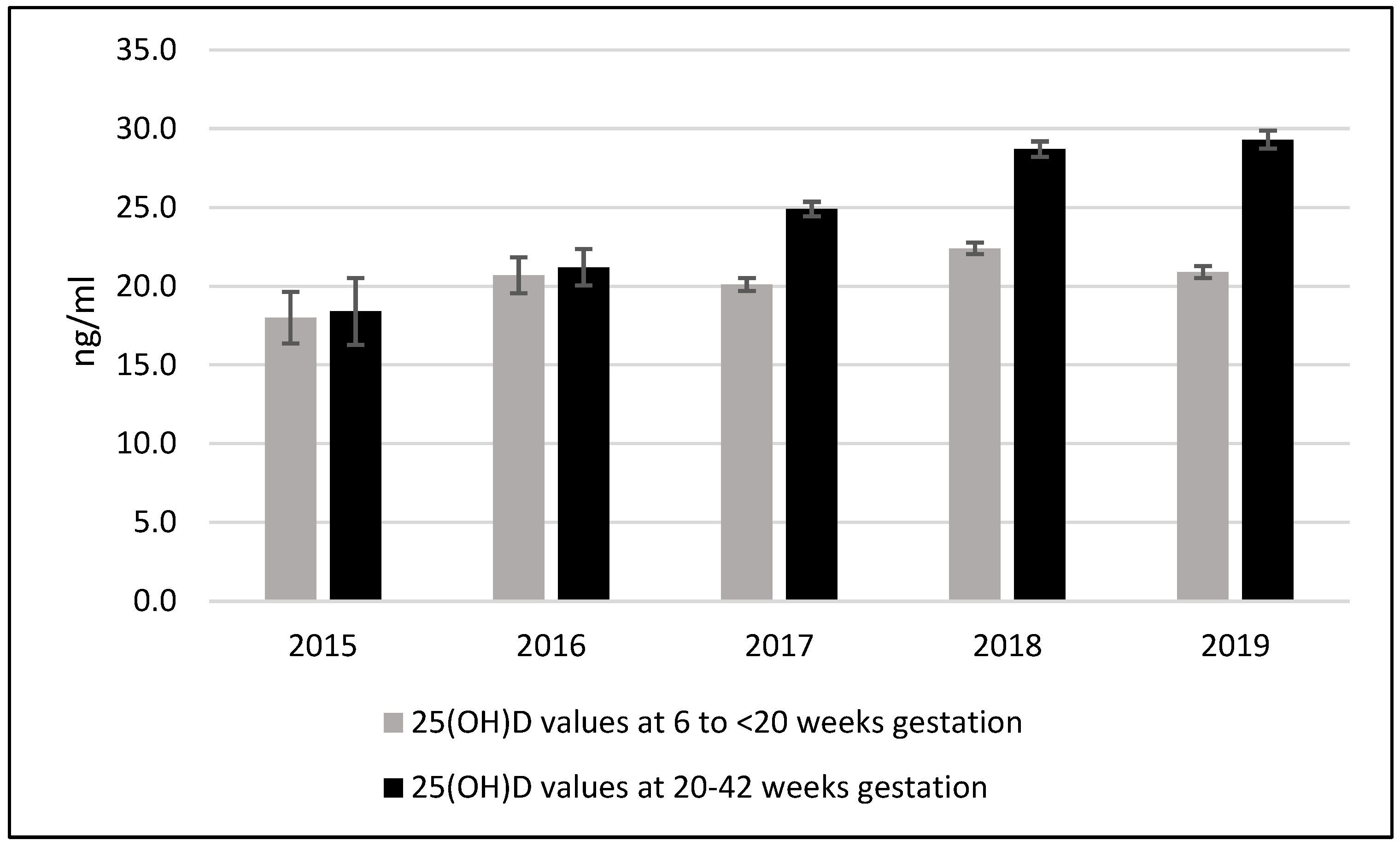
3.1. Prenatal 25(OH)D Concentrations
3.2. Birthweight and Prematurity
3.3. Early Childhood Caries
3.4. Rickets
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ward, L.M.; Gaboury, I.; Ladhani, M.; Zlotkin, S. Vitamin D-deficiency rickets among children in Canada. Can. Med. Assoc. J. 2007, 177, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Gessner, B.D.; Deschweinitz, E.; Petersen, K.M.; Lewandowski, C. Nutritional rickets among breast-fed black and Alaska Native children. Alsk. Med. 1997, 39, 72–74. [Google Scholar]
- Singleton, R.; Lescher, R.; Gessner, B.D.; Benson, M.; Bulkow, L.; Rosenfeld, J.; Thomas, T.; Holman, R.C.; Haberling, D.; Bruce, M.; et al. Rickets and vitamin D deficiency in Alaska native children. J. Pediatr. Endocrinol. Metab. 2015, 28, 815–823. [Google Scholar] [CrossRef]
- Gross, M.L.; Tenenbein, M.; Sellers, E.A.C. Severe vitamin D deficiency in 6 Canadian First Nation formula-fed infants. Int. J. Circumpolar Health 2013, 72, 20244. [Google Scholar] [CrossRef] [PubMed]
- Fohner, A.E.; Wang, Z.; Yracheta, J.; O’Brien, D.M.; Hopkins, S.E.; Black, J.; Philip, J.; Wiener, H.W.; Tiwari, H.K.; Stapleton, P.L.; et al. Genetics, Diet, and Season Are Associated with Serum 25-Hydroxycholecalciferol Concentration in a Yup’ik Study Population from Southwestern Alaska. J. Nutr. 2016, 146, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Bersamin, A.; Zidenberg-Cherr, S.; Stern, J.S.; Luick, B.R. Nutrient intakes are associated with adherence to a traditional diet among Yup’ik Eskimos living in remote Alaska Native communities: The CANHR Study. Int. J. Circumpolar Health 2007, 66, 62–70. [Google Scholar] [CrossRef]
- Kuhnlein, H.V.; Receveur, O.; Soueida, R.; Egeland, G.M. Arctic Indigenous Peoples Experience the Nutrition Transition with Changing Dietary Patterns and Obesity. J. Nutr. 2004, 134, 1447–1453. [Google Scholar] [CrossRef]
- Sharma, S.; Barr, A.B.; Macdonald, H.M.; Sheehy, T.; Novotny, R.; Corriveau, A. Vitamin D deficiency and disease risk among aboriginal Arctic populations. Nutr. Rev. 2011, 69, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Egeland, G.M.; Johnson-Down, L.; Cao, Z.R.; Sheikh, N.; Weiler, H. Food Insecurity and Nutrition Transition Combine to Affect Nutrient Intakes in Canadian Arctic Communities. J. Nutr. 2011, 141, 1746–1753. [Google Scholar] [CrossRef]
- Bersamin, A.; Luick, B.R.; Ruppert, E.; Stern, J.S.; Zidenberg-Cherr, S. Diet Quality among Yup’ik Eskimos Living in Rural Communities Is Low: The Center for Alaska Native Health Research Pilot Study. J. Am. Diet. Assoc. 2006, 106, 1055–1063. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Golden, N.H.; Abrams, S.A. Optimizing Bone Health in Children and Adolescents. Pediatrics 2014, 134, e1229–e1243. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, R.L.; Sternberg, M.R.; Lacher, D.A.; Sempos, C.T.; Looker, A.C.; Durazo-Arvizu, R.A.; Yetley, E.A.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am. J. Clin. Nutr. 2016, 104, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Pacaud, D.; Petryk, A.; Collett-Solberg, P.F.; Kappy, M.; On Behalf of the Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D Deficiency in Children and Its Management: Review of Current Knowledge and Recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, D.M.; E Thummel, K.; Bulkow, L.R.; Wang, Z.; Corbin, B.; Klejka, J.; E Hopkins, S.; Boyer, B.B.; Hennessy, T.W.; Singleton, R. Declines in traditional marine food intake and vitamin D levels from the 1960s to present in young Alaska Native women. Public Health Nutr. 2016, 20, 1738–1745. [Google Scholar] [CrossRef]
- Berdal, A.; Balmain, N.; Cuisinier-Gleizes, P.; Mathieu, H. Histology and microradiography of earlypost-natal molar tooth development in vitamin-D deficient rats. Arch. Oral Biol. 1987, 32, 493–498. [Google Scholar] [CrossRef]
- Caufield, P.; Li, Y.; Bromage, T. Hypoplasia-associated Severe Early Childhood Caries—A Proposed Definition. J. Dent. Res. 2012, 91, 544–550. [Google Scholar] [CrossRef]
- Nikiforuk, G.; Fraser, D. The etiology of enamel hypoplasia: A unifying concept. J. Pediatr. 1981, 98, 888–893. [Google Scholar] [CrossRef]
- Schroth, R.J.; Lavelle, C.; Tate, R.; Bruce, S.; Billings, R.J.; Moffatt, M.E. Prenatal Vitamin D and Dental Caries in Infants. Pediatrics 2014, 133, e1277–e1284. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Dental caries in rural Alaska Native children—Alaska, 2008. MMWR. Morb. Mortal. Wkly. Rep. 2011, 60, 1275–1278. [Google Scholar]
- Mosites, E.; Rodriguez, E.; Caudill, S.P.; Hennessy, T.W.; Berner, J. A comparison of individual-level vs. hypothetically pooled mercury biomonitoring data from the Maternal Organics Monitoring Study (MOMS), Alaska, 1999–2012. Int. J. Circumpolar Health 2020, 79, 1726256. [Google Scholar] [CrossRef] [PubMed]
- Singleton, R.; Day, G.; Thomas, T.; Schroth, R.; Klejka, J.; Lenaker, D.; Berner, J. Association of Maternal Vitamin D Deficiency with Early Childhood Caries. J. Dent. Res. 2019, 98, 549–555. [Google Scholar] [CrossRef]
- Vitamin D Deficiency in Prenatal Alaska Native Women. In State of Alaska Epidemiology Bulletin; No 27; State of Alaska: Anchorage, AK, USA, 2016.
- State of Alaska. Vitamin D Supplementation and Screening for the Prevention of Rickets and Osteomalacia in Alaska. Epi-Demiology Bull. Recomm. Rep. 2018, 20. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Alaska Department of Labor and Workforce Development, R.a.A.S. Alaska Population by Age, Sex, Bridged Race and Hispanic Origin, 2000 to 2010. Available online: https://live.laborstats.alaska.gov/pop/index.cfm (accessed on 24 August 2021).
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Sao Paulo Med. J. 2016, 134, 274–275. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; De-Regil, L.M.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation during pregnancy: Updated meta-analysis on maternal outcomes. J. Steroid Biochem. Mol. Biol. 2016, 164, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.C.; Stewart, A.W.; Scragg, R.; Milne, T.; Rowden, J.; Ekeroma, A.; Wall, C.; Mitchell, E.A.; Crengle, S.; Trenholme, A.; et al. Vitamin D During Pregnancy and Infancy and Infant Serum 25-Hydroxyvitamin D Concentration. Pediatrics 2014, 133, e143–e153. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Ye, C.; Swaminathan, B.; Hanley, A.J.; Connelly, P.; Sermer, M.; Zinman, B.; Retnakaran, R. The persistence of maternal vitamin D deficiency and insufficiency during pregnancy and lactation irrespective of season and supplementation. Clin. Endocrinol. 2016, 84, 680–686. [Google Scholar] [CrossRef]
- Irvine, J.W.; Ward, L.M. Canadian Paediatric Society; First Nations, Inuit, and Metis Health Committee. Preventing symptomatic vitamin D deficiency and rickets among Indigenous infants and children in Canada. Paediatr. Child Health 2022, 27, 127. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists (ACOG). Vitamin D: Screening and Sup-plementation During Pregnancy. Obstet. Gynecol. 2011, 118, 197–198. [Google Scholar] [CrossRef]
- Nutrition Working Group; O’Connor, D.L.; Blake, J.; Bell, R.; Bowen, A.; Callum, J.; Fenton, S.; Gray-Donald, K.; Rossiter, M.; Adamo, K.; et al. Canadian consensus on female nutrition: Adolescence, reproduction, menopause, and beyond. J. Obstet. Gynaecol. Can. 2016, 38, 508–554. [Google Scholar] [CrossRef]
- Schroth, R.J.; A Levi, J.; A Sellers, E.; Friel, J.; Kliewer, E.; Moffatt, M.E. Vitamin D status of children with severe early childhood caries: A case–control study. BMC Pediatr. 2013, 13, 174. [Google Scholar] [CrossRef]
- Theodoratou, E.; Tzoulaki, I.; Zgaga, L.; Ioannidis, J.P.A. Vitamin D and multiple health outcomes: Umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 2014, 348, g2035. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; Dhalla, S.; Tate, R.; Moffatt ME, K. Prenatal and early childhood determinants of enamel hypoplasia in infants. J. Pediatrics Perinatol. Child Health 2021, 5, 5–17. [Google Scholar]
- Schroth, R.J.; Christensen, J.; Morris, M.; Gregory, P.; Mittermuller, B.-A.; Rockman-Greenberg, C. The Influence of Prenatal Vitamin D Supplementation on Dental Caries in Infants. J. Can. Dent. Assoc. 2020, 86, k13. [Google Scholar] [PubMed]


{kind=link}
| Maternal Characteristics, Mean (SD) | |
| Maternal age, years | 25.9 (5.6) |
| Gestational age at 20+ weeks, weeks | 33.1 (5.9) |
| Prenatal plasma 25(OH) vitamin D, ng/mL | 26.5(5.6) |
| Season at prenatal visit, n (%) | |
| Nov-Apr | 771 (50.7) |
| May-Oct | 751 (49.3) |
| Sub-region, n (%) | |
| Coastal | 682 (44.8) |
| River | 840 (55.2) |
| Dental Health Aide Therapist/Dentist in Community, n (%) | |
| Yes | 627 (41.2) |
| No | 895 (58.8) |
| Serum 25-hydroxy vitamin D concentration, n (%) | |
| Deficient | 94 (6.2) |
| Insufficient | 344 (22.6) |
| Sufficient | 1084 (71.2) |
| Mean (SD) 25(OH)D (ng/mL) N = 1522 | p-Value 1 | |
|---|---|---|
| Maternal Age, years | ||
| <33 | 26.3 (10.6) | 0.06 |
| ≥33 | 27.8 (10.6) | |
| Gestational Age, weeks | ||
| <36 | 26.9 (10.4) | 0.14 |
| ≥36 | 26.1 (10.8) | |
| Season at prenatal visit | ||
| Nov-Apr | 25.9 (11.4) | 0.03 |
| May-Oct | 27.1 (9.7) | |
| Sub-region | ||
| Coastal | 25.5 (11.2) | 0.0008 |
| River | 27.3 (10.0) |
| 25(OH) Vitamin D Concentration | 2015–2016 | 2017–2019 | p-Value |
|---|---|---|---|
| n = 175 | n = 1347 | ||
| Mean | 20 | 27.3 | <0.0001 1 |
| SD | 7.9 | 10.6 | |
| Min | 5.8 | 5 | |
| Max | 41.7 | 100 | |
| 25 (OH) Vitamin D concentration | n (%) | n (%) | p-value |
| Deficient <12 ng/mL | 26 (14.9) | 68 (5.0) | <0.0001 2 |
| Insufficient ≥12 ng/mL and <20 ng/mL | 76 (43.4) | 268 (19.9) | |
| Sufficient ≥20 ng/mL | 73 (41.7) | 1011 (75.1) | |
| Mean (SD) | Mean (SD) | p-value | |
| Maternal Age, years (n = 1522) | n = 175 | n = 1347 | |
| <33 (n = 1315) | 19.8 (7.7) | 27.2 (10.6) | <0.0001 1 |
| ≥33 (n = 207) | 21.4 (9.2) | 28.6 (10.6) | 0.003 |
| Season at prenatal visit (n = 1522) | |||
| Nov-Apr (n = 771) | 19.8 (8.0) | 26.9 (11.6) | <0.0001 1 |
| May-Oct (n = 840 | 20.4 (7.8) | 27.7 (9.6) | <0.0001 1 |
| Sub-region (n = 1522) | |||
| Coastal | 18.0 (7.1) | 26.5 (11.3) | <0.0001 1 |
| River | 21.8 (8.2) | 28.0 (9.9) | <0.0001 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singleton, R.J.; Day, G.M.; Thomas, T.K.; Klejka, J.A.; Desnoyers, C.A.; McIntyre, M.N.P.; Compton, D.M.; Thummel, K.E.; Schroth, R.J.; Ward, L.M.; et al. Impact of a Prenatal Vitamin D Supplementation Program on Vitamin D Deficiency, Rickets and Early Childhood Caries in an Alaska Native Population. Nutrients 2022, 14, 3935. https://doi.org/10.3390/nu14193935
Singleton RJ, Day GM, Thomas TK, Klejka JA, Desnoyers CA, McIntyre MNP, Compton DM, Thummel KE, Schroth RJ, Ward LM, et al. Impact of a Prenatal Vitamin D Supplementation Program on Vitamin D Deficiency, Rickets and Early Childhood Caries in an Alaska Native Population. Nutrients. 2022; 14(19):3935. https://doi.org/10.3390/nu14193935
Chicago/Turabian StyleSingleton, Rosalyn J., Gretchen M. Day, Timothy K. Thomas, Joseph A. Klejka, Christine A. Desnoyers, Melanie N. P. McIntyre, David M. Compton, Kenneth E. Thummel, Robert J. Schroth, Leanne M. Ward, and et al. 2022. "Impact of a Prenatal Vitamin D Supplementation Program on Vitamin D Deficiency, Rickets and Early Childhood Caries in an Alaska Native Population" Nutrients 14, no. 19: 3935. https://doi.org/10.3390/nu14193935