
Infant Red Blood Cell Arachidonic to Docosahexaenoic Acid Ratio Inversely Associates with Fat-Free Mass Independent of Breastfeeding Exclusivity
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Breastfed and FF Mother and Infant Dyads
3.2. Infant RBC and Breastmilk AA/DHA Ratios Are Related Only in Breastfeeding Dyads
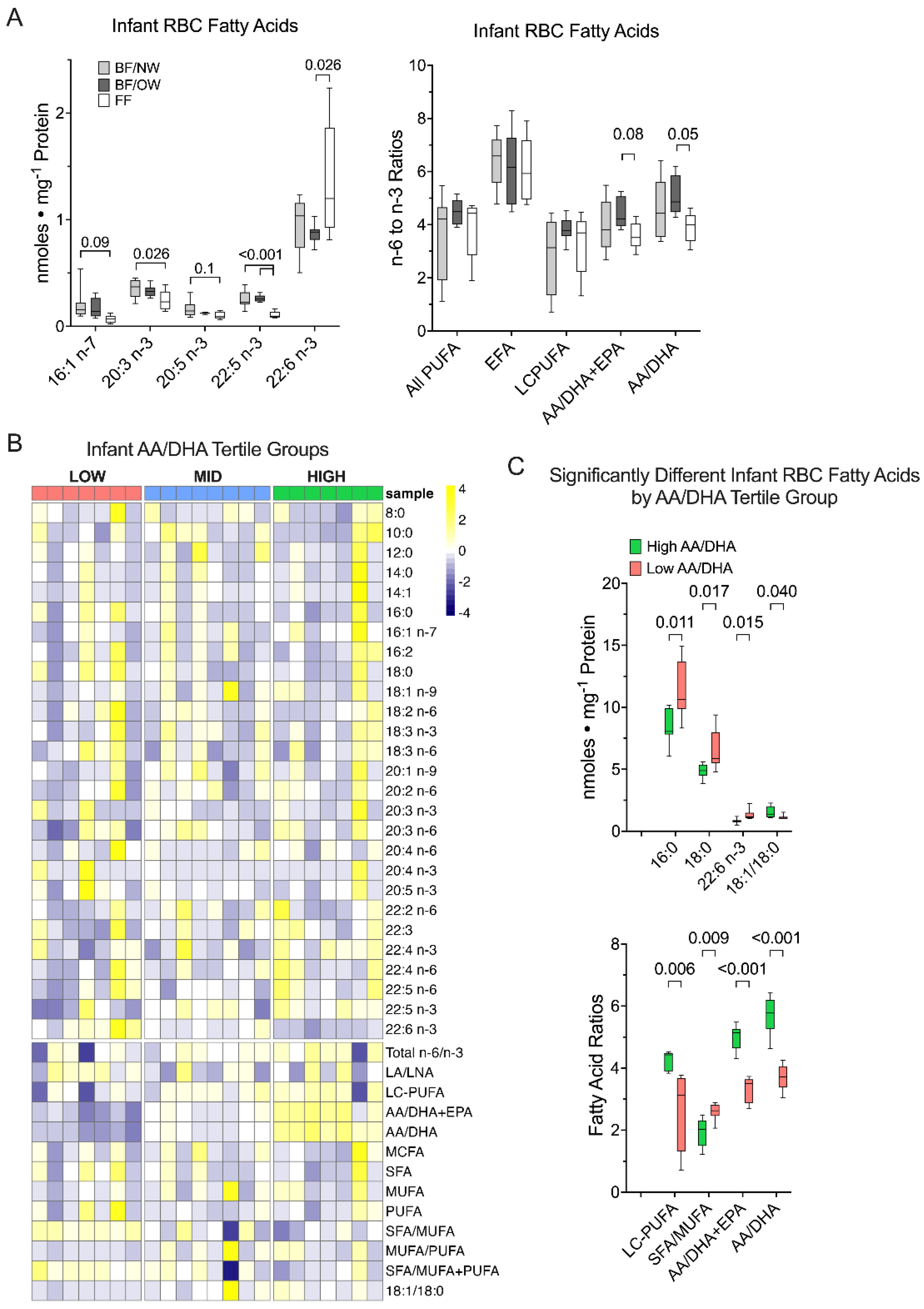
3.3. Docosahexaenoic Acid, but Not Other n-3 PUFA, Is Greater in Formula-Fed Infants
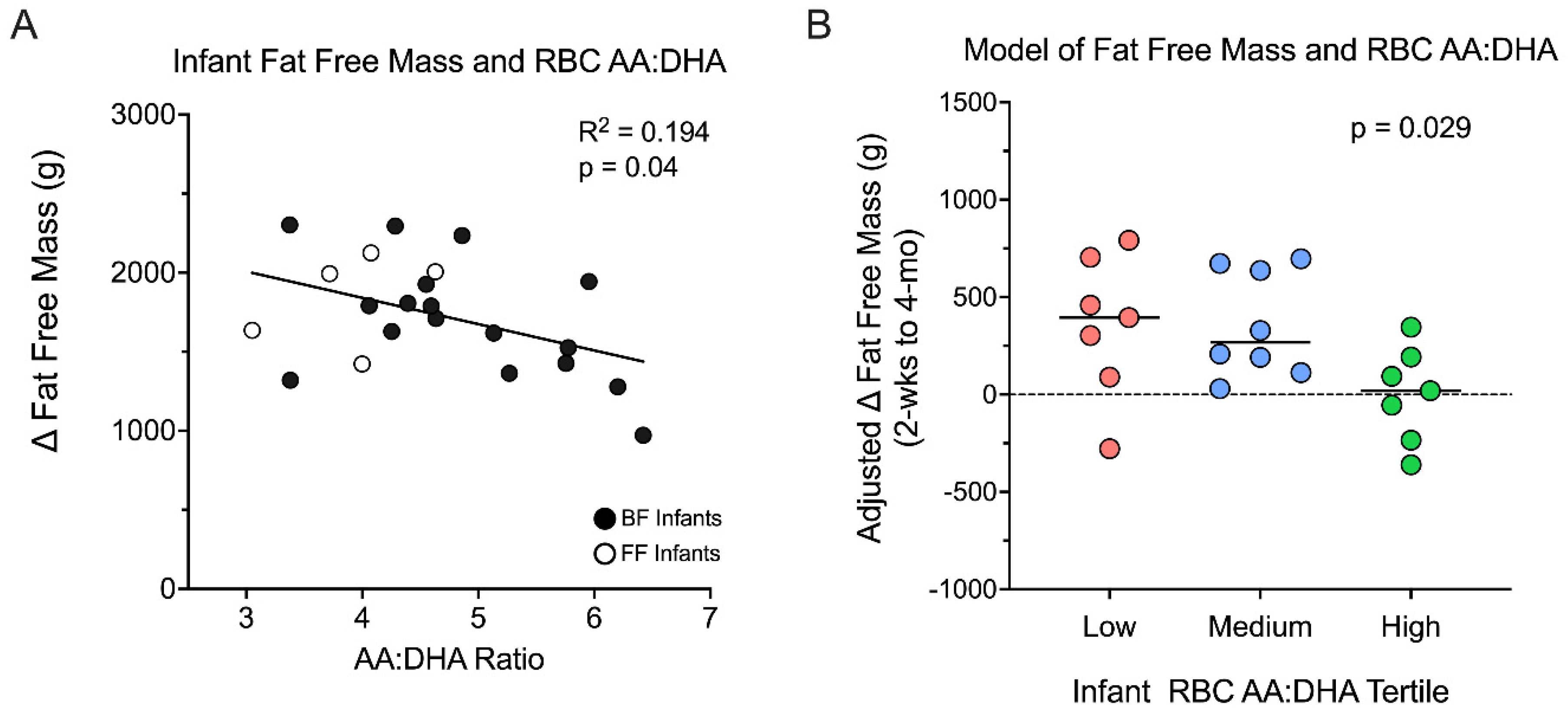
3.4. Infant RBC AA/DHA Ratio Relationships with Infant Body Composition
3.5. Infant Fat Free Mass Accumulation Is Greater in the Low AA/DHA Ratio Group
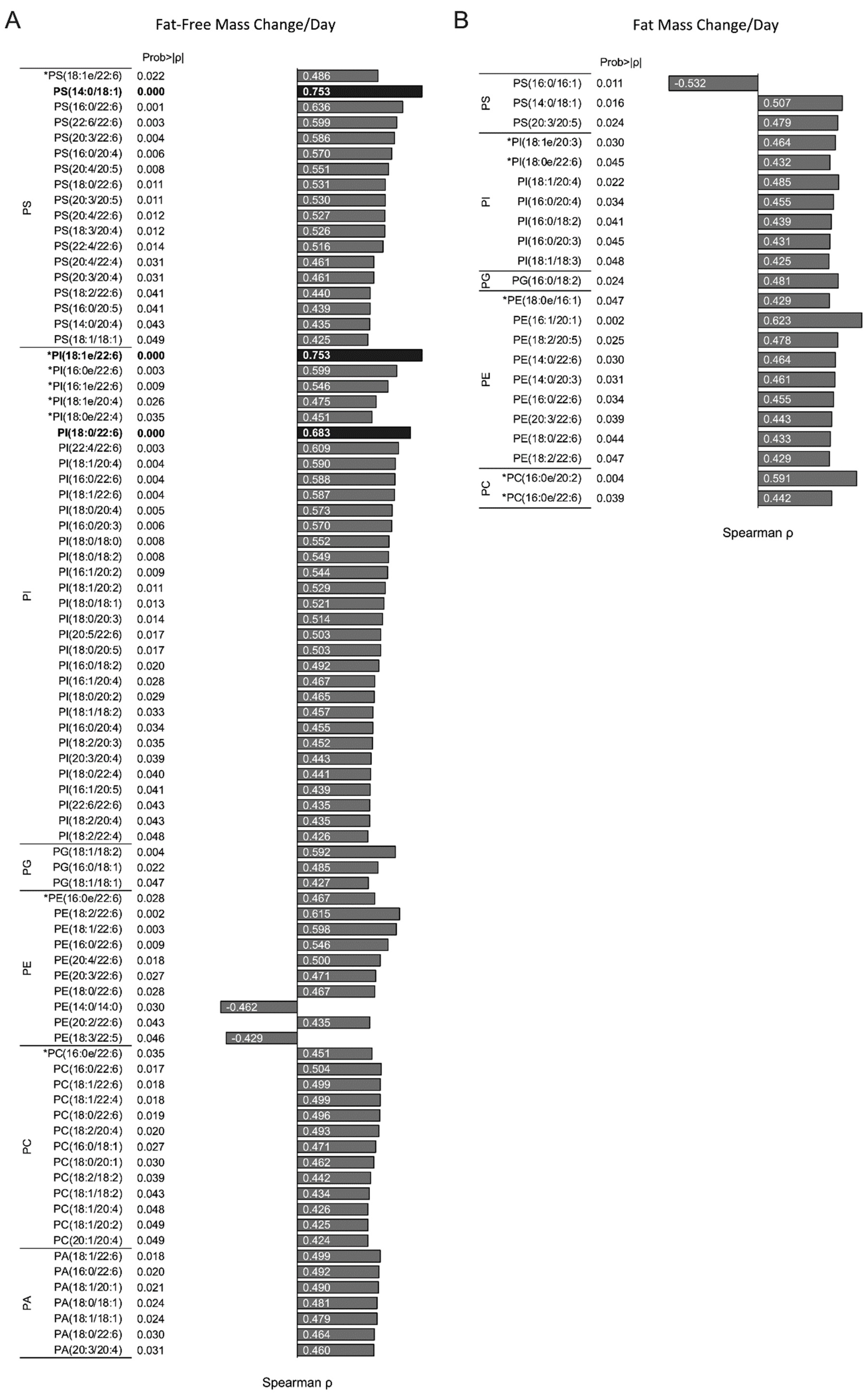
3.6. Infant RBC Phospholipid Species Containing AA and DHA Correlate with Changes Infant Fat-Free Mass Accumulation
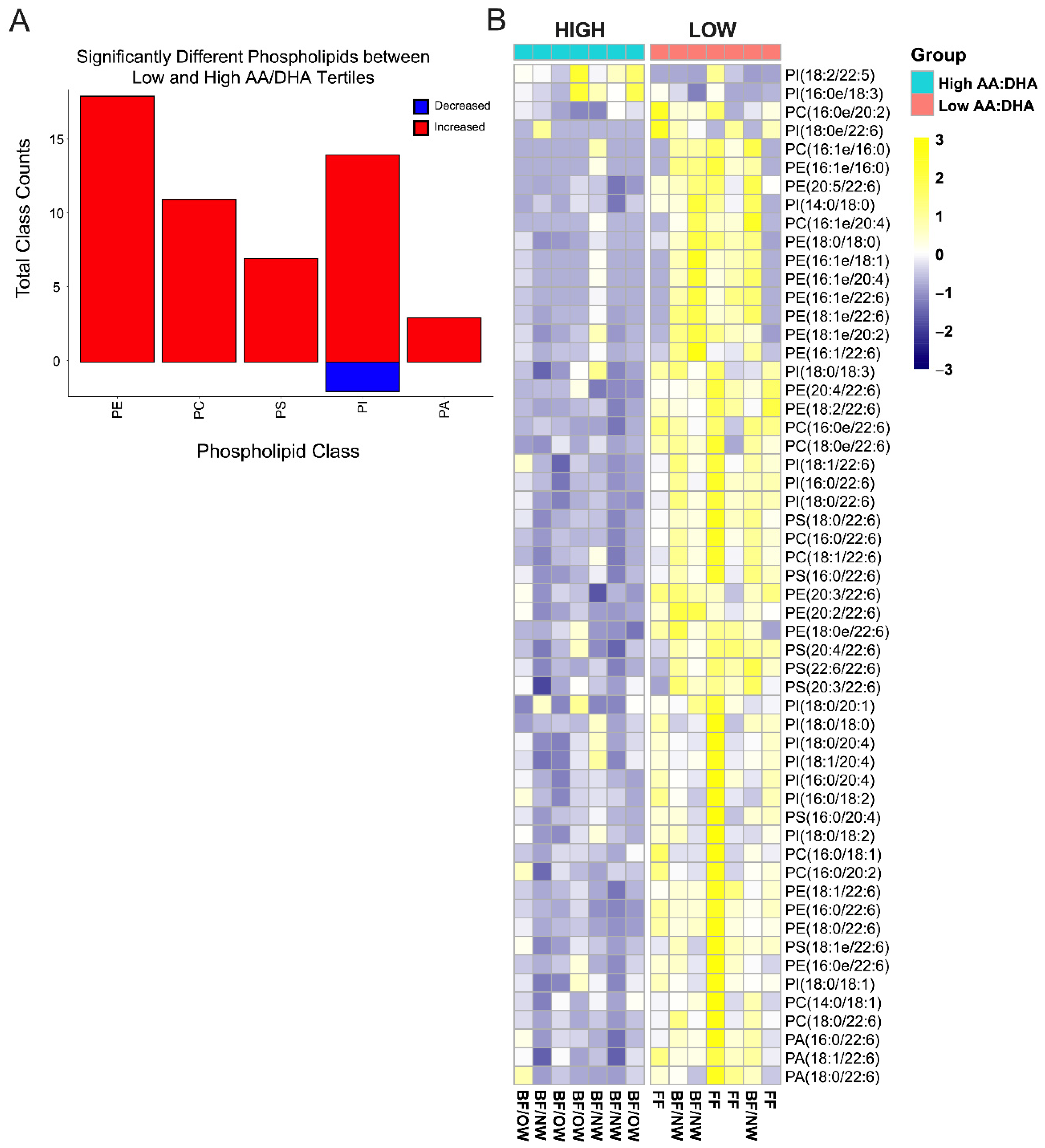
3.7. Plasmalogens Comprise Half of the Differential Infant RBC Phospholipids by Low AA/DHA Ratio
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Summermatter, S.; Marcelino, H.; Arsenijevic, D.; Buchala, A.; Aprikian, O.; Assimacopoulos-Jeannet, F.; Seydoux, J.; Montani, J.P.; Solinas, G.; Dulloo, A.G. Adipose tissue plasticity during catch-up fat driven by thrifty metabolism: Relevance for muscle-adipose glucose redistribution during catch-up growth. Diabetes 2009, 58, 2228–2237. [Google Scholar] [CrossRef] [Green Version]
- Ay, L.; Van Houten, V.A.; Steegers, E.A.; Hofman, A.; Witteman, J.C.; Jaddoe, V.W.; Hokken-Koelega, A.C. Fetal and postnatal growth and body composition at 6 months of age. J. Clin. Endocrinol. Metab. 2009, 94, 2023–2030. [Google Scholar] [CrossRef]
- Summermatter, S.; Mainieri, D.; Russell, A.P.; Seydoux, J.; Montani, J.P.; Buchala, A.; Solinas, G.; Dulloo, A.G. Thrifty metabolism that favors fat storage after caloric restriction: A role for skeletal muscle phosphatidylinositol-3-kinase activity and AMP-activated protein kinase. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2008, 22, 774–785. [Google Scholar] [CrossRef] [Green Version]
- Dulloo, A.G. Thrifty energy metabolism in catch-up growth trajectories to insulin and leptin resistance. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 155–171. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Nissensohn, M.; Overby, N.C.; Fekete, K. Dietary methods and biomarkers of omega 3 fatty acids: A systematic review. Br. J. Nutr. 2012, 107 (Suppl. S2), S64–S76. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.M.; Franco, R.S.; Khera, P.K.; Smith, E.P.; Lindsell, C.J.; Ciraolo, P.J.; Palascak, M.B.; Joiner, C.H. Red cell life span heterogeneity in hematologically normal people is sufficient to alter HbA1c. Blood 2008, 112, 4284–4291. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, M.C.; Young, B.E.; Lemas, D.J.; Palmer, C.E.; Hernandez, T.L.; Barbour, L.A.; Friedman, J.E.; Krebs, N.F.; MacLean, P.S. Early infant adipose deposition is positively associated with the n-6 to n-3 fatty acid ratio in human milk independent of maternal BMI. Int. J. Obes. (Lond.) 2017, 41, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Young, B.E.; Levek, C.; Reynolds, R.M.; Rudolph, M.C.; MacLean, P.; Hernandez, T.L.; Friedman, J.E.; Krebs, N.F. Bioactive components in human milk are differentially associated with rates of lean and fat mass deposition in infants of mothers with normal vs. elevated BMI. Pediatr. Obes. 2018, 13, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, M.C.; Jackman, M.R.; Presby, D.M.; Houck, J.A.; Webb, P.G.; Johnson, G.C.; Soderborg, T.K.; de la Houssaye, B.A.; Yang, I.V.; Friedman, J.E.; et al. Low Neonatal Plasma n-6/n-3 PUFA Ratios Regulate Offspring Adipogenic Potential and Condition Adult Obesity Resistance. Diabetes 2018, 67, 651–661. [Google Scholar] [CrossRef] [Green Version]
- Young, B.E.; Johnson, S.L.; Krebs, N.F. Biological determinants linking infant weight gain and child obesity: Current knowledge and future directions. Adv. Nutr. 2012, 3, 675–686. [Google Scholar] [CrossRef] [Green Version]
- Young, B.E.; Patinkin, Z.; Palmer, C.; de la Houssaye, B.; Barbour, L.; Hernandez, T.; Friedman, J.; Krebs, N. Human Milk Insulin is Related to Maternal Plasma Insulin and BMI—But other Components of Human Milk do not Differ by BMI. Eur. J. Clin. Nutr. 2017, 71, 1094–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, H.G.; Oklander, M. Improved Procedure for the Extraction of Lipids from Human Erythrocytes. J. Lipid Res. 1965, 6, 428–431. [Google Scholar] [CrossRef]
- Okuno, T.; Gijon, M.A.; Zarini, S.; Martin, S.A.; Barkley, R.M.; Johnson, C.A.; Ohba, M.; Yokomizo, T.; Murphy, R.C. Altered eicosanoid production and phospholipid remodeling during cell culture. J. Lipid Res. 2018, 59, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Vinding, R.K.; Stokholm, J.; Sevelsted, A.; Sejersen, T.; Chawes, B.L.; Bonnelykke, K.; Thorsen, J.; Howe, L.D.; Krakauer, M.; Bisgaard, H. Effect of fish oil supplementation in pregnancy on bone, lean, and fat mass at six years: Randomised clinical trial. BMJ 2018, 362, k3312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossato, L.T.; Schoenfeld, B.J.; de Oliveira, E.P. Is there sufficient evidence to supplement omega-3 fatty acids to increase muscle mass and strength in young and older adults? Clin. Nutr. 2020, 39, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Leyton, J.; Drury, P.J.; Crawford, M.A. Differential oxidation of saturated and unsaturated fatty acids in vivo in the rat. Br. J. Nutr. 1987, 57, 383–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innis, S.M. Dietary omega 3 fatty acids and the developing brain. Brain Res. 2008, 1237, 35–43. [Google Scholar] [CrossRef]
- Devarshi, P.P.; Grant, R.W.; Ikonte, C.J.; Hazels Mitmesser, S. Maternal Omega-3 Nutrition, Placental Transfer and Fetal Brain Development in Gestational Diabetes and Preeclampsia. Nutrients 2019, 11, 1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharami, K.; Das, M.; Das, S. Essential role of docosahexaenoic acid towards development of a smarter brain. Neurochem. Int. 2015, 89, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Docosahexaenoic Acid. Ann. Nutr. Metab. 2016, 69 (Suppl. S1), 7–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innis, S.M. Metabolic programming of long-term outcomes due to fatty acid nutrition in early life. Matern. Child Nutr. 2011, 7 (Suppl. S2), 112–123. [Google Scholar] [CrossRef]
- Donahue, S.M.; Rifas-Shiman, S.L.; Gold, D.R.; Jouni, Z.E.; Gillman, M.W.; Oken, E. Prenatal fatty acid status and child adiposity at age 3 y: Results from a US pregnancy cohort. Am. J. Clin. Nutr. 2011, 93, 780–788. [Google Scholar] [CrossRef] [Green Version]
- Massiera, F.; Saint-Marc, P.; Seydoux, J.; Murata, T.; Kobayashi, T.; Narumiya, S.; Guesnet, P.; Amri, E.Z.; Negrel, R.; Ailhaud, G. Arachidonic acid and prostacyclin signaling promote adipose tissue development: A human health concern? J. Lipid Res. 2003, 44, 271–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Tierney-Ginn, P.F.; Davina, D.; Gillingham, M.; Barker, D.J.P.; Morris, C.; Thornburg, K.L. Neonatal fatty acid profiles are correlated with infant growth measures at 6 months. J. Dev. Orig. Health Dis. 2017, 8, 474–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, L.; Lauritzen, L.; Brasholt, M.; Buhl, T.; Bisgaard, H. Polyunsaturated fatty acid content of mother’s milk is associated with childhood body composition. Pediatr. Res. 2012, 72, 631–636. [Google Scholar] [CrossRef] [Green Version]
- Farahnak, Z.; Yuan, Y.; Vanstone, C.A.; Weiler, H.A. Maternal and neonatal red blood cell n-3 polyunsaturated fatty acids inversely associate with infant whole-body fat mass assessed by dual-energy X-ray absorptiometry. Appl. Physiol. Nutr. Metab. 2020, 45, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; Nordgren, M.; Wang, B.; Apanasets, O. Role of peroxisomes in ROS/RNS-metabolism: Implications for human disease. Biochim. Biophys. Acta 2012, 1822, 1363–1373. [Google Scholar] [CrossRef] [Green Version]
- Metherel, A.H.; Bazinet, R.P. Updates to the n-3 polyunsaturated fatty acid biosynthesis pathway: DHA synthesis rates, tetracosahexaenoic acid and (minimal) retroconversion. Prog. Lipid Res. 2019, 76, 101008. [Google Scholar] [CrossRef] [PubMed]
- Park, H.G.; Park, W.J.; Kothapalli, K.S.; Brenna, J.T. The fatty acid desaturase 2 (FADS2) gene product catalyzes Delta4 desaturation to yield n-3 docosahexaenoic acid and n-6 docosapentaenoic acid in human cells. FASEB J. 2015, 29, 3911–3919. [Google Scholar] [CrossRef] [Green Version]
- Dean, J.M.; Lodhi, I.J. Structural and functional roles of ether lipids. Protein Cell 2018, 9, 196–206. [Google Scholar] [CrossRef]
- Calder, P.C. Functional Roles of Fatty Acids and Their Effects on Human Health. JPEN J. Parenter Enter. Nutr. 2015, 39, 18S–32S. [Google Scholar] [CrossRef]
- Tulodziecka, K.; Diaz-Rohrer, B.B.; Farley, M.M.; Chan, R.B.; Di Paolo, G.; Levental, K.R.; Waxham, M.N.; Levental, I. Remodeling of the postsynaptic plasma membrane during neural development. Mol. Biol. Cell 2016, 27, 3480–3489. [Google Scholar] [CrossRef]
- Wolfs, D.; Lynes, M.D.; Tseng, Y.H.; Pierce, S.; Bussberg, V.; Darkwah, A.; Tolstikov, V.; Narain, N.R.; Rudolph, M.C.; Kiebish, M.A.; et al. Brown Fat-Activating Lipokine 12,13-diHOME in Human Milk Is Associated With Infant Adiposity. J. Clin. Endocrinol. Metab. 2021, 106, e943–e956. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | BF/NW (n = 8) | BF/OW (n = 9) | FF (n = 5) | p-Value |
|---|---|---|---|---|
| Maternal age (yrs) | 29.9 ± 2.7 | 31.4 ± 4.4 | 27.4 ± 4.1 | 0.1976 |
| Pre-Pregnancy BMI (kg/m2) | 20.9 ± 2.2 | 30.5 ± 3.9 | 33.2 ± 7.1 | <0.0001 |
| Gestational age (wks) | 39.6 ± 0.8 | 39.4 ± 0.9 | 39.6 ± 0.9 | 0.938 |
| Race | Asian: 12.5% White 87.5% | Asian 1: 22.2% African American: 11.1% White: 66.7% | Hawaiian/Pacific Islander: 20.0% White: 80.0% | 0.342 |
| Ethnicity | Hispanic: 12.5% Non-Hispanic: 87.5% | Hispanic: 25.0% Non-Hispanic: 75.0% | Hispanic: 60.0% Non-Hispanic: 40.0% | 0.185 |
| Infant sex (% male) | 62.5% | 77.8% | 20% | 0.098 |
| Birth weight (g) | 3130 ± 357 | 3473 ± 544 | 3781 ± 366 | 0.056 |
| Breastfeeding Exposure (months) | 3.9 ± 0.42 | 4.0 ± 0.06 | 0.8 ± 0.41 | <0.0001 |
| Milk | Infant RBCs | p-Value | R2 |
|---|---|---|---|
| 16:0 | 16:0 | 0.715 | |
| 18:2 n6 | 18:2 n6 | 0.397 | |
| 18:3 n3 | 18:3 n3 | 0.999 | |
| 20:4 n6 | 20:4 n6 | 0.128 | |
| 20:5 n3 | 20:5 n3 | 0.997 | |
| 22:6 n3 | 22:6 n3 | 0.0038 | 0.44 |
| Total n6/n3 | Total n6/n3 | 0.95 | |
| AA to DHA | AA to DHA | 0.0005 | 0.56 |
| AA to DHA + EPA | AA to DHA + EPA | 0.0007 | 0.55 |
| Outcome | p-Value | Relationship (Tukey) |
|---|---|---|
| ∆ FFM/day | 0.029 | high < mid, p = 0.032 high < low, p = 0.075 |
| ∆ Fat Mass/day | 0.144 | |
| ∆ % Fat/day | 0.479 | |
| ∆ WLZ/day | 0.190 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Young, B.E.; Kyere-Davies, G.; Farriester, J.W.; Varshney, R.; MacLean, P.S.; Krebs, N.F.; Rudolph, M.C. Infant Red Blood Cell Arachidonic to Docosahexaenoic Acid Ratio Inversely Associates with Fat-Free Mass Independent of Breastfeeding Exclusivity. Nutrients 2022, 14, 4238. https://doi.org/10.3390/nu14204238
Young BE, Kyere-Davies G, Farriester JW, Varshney R, MacLean PS, Krebs NF, Rudolph MC. Infant Red Blood Cell Arachidonic to Docosahexaenoic Acid Ratio Inversely Associates with Fat-Free Mass Independent of Breastfeeding Exclusivity. Nutrients. 2022; 14(20):4238. https://doi.org/10.3390/nu14204238
Chicago/Turabian StyleYoung, Bridget E., Gertrude Kyere-Davies, Jacob W. Farriester, Rohan Varshney, Paul S. MacLean, Nancy F. Krebs, and Michael C. Rudolph. 2022. "Infant Red Blood Cell Arachidonic to Docosahexaenoic Acid Ratio Inversely Associates with Fat-Free Mass Independent of Breastfeeding Exclusivity" Nutrients 14, no. 20: 4238. https://doi.org/10.3390/nu14204238