
Factors Associated with Dietary Restriction and Emotional and Uncontrolled Eating in Adults from Spanish-Speaking Countries during the COVID-19 Confinement: Results of the CoV-Eat Project
 , , ,
, , ,  ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
- (1)
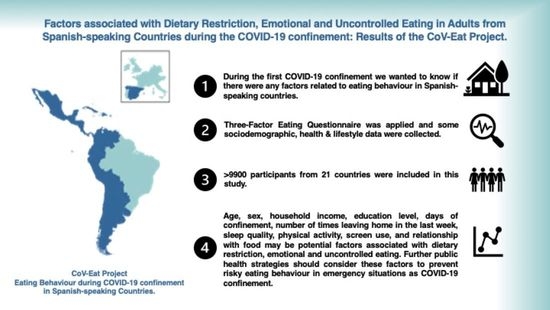
- To assess eating behaviour, we used the validated Spanish version of the Three-Factor Eating Questionnaire-R18 (TFEQ-R18-SP) [17]. This test measures three different types of eating behaviour: (a) cognitive restraint (CR), defined as the conscious restriction of the consumption of foods aimed at controlling the corporal weight and/or promoting the loss of weight; (b) emotional eating (EE), defined as eating as a way to suppress negative emotions; and (c) uncontrolled eating (UE), referred to the tendency to eat more than the usual because of a loss of control on the consumption with a subjective feeling of hunger. The questionnaire consists of 18 items divided into three subscales: CR (six items), EE (three items), and UE (nine items). The items can be scored on a four-point scale (definitively true: 1, mainly true: 2, mainly false: 3, definitively false: 4). The total score of each subscale can be obtained from the sum of the respective items. Higher scores in the subscales indicated greater CR, EE, and UE.
- (2)
- In the section on sociodemographic and health information, we collected the following data: (a) self-reported basic anthropometrics data: weight (kg), height (cm), abdominal circumference (cm); (b) health status information: previous diagnosis of chronic illnesses: diabetes, hypertension, cancer, obesity, and time passed from the diagnosis; and (c) sociodemographic data: country of residence, sex (woman/man), age, educational level (primary, secondary, university), employment situation prior to the pandemic and current (works, teleworking, retired, stopped/earning subsidy, stopped/without earning, student, unpaid domestic work, or other situations), marital status (single, coupled up), and number of people living at home.
- (3)
- The last section included information about lifestyles: (a) days of confinement, type of cohabitation (alone, in a family without children, in a family with children), frequency and reason for leaving the house; (b) data related with lifestyles before and during home confinement: sleep quality, physical activity, screen use, tobacco consumption, relationship with food; and (c) data related with the purchase of foods: frequency and monetary cost in the purchase of foods in the last week and frequency of food delivery to home.
2.2. Study Variables
2.2.1. Eating Behaviours
2.2.2. Covariates
2.3. Statistical Analyses
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ammar, A.; Mueller, P.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Brach, M.; Schmicker, M.; Bentlage, E.; et al. Psychological Consequences of COVID-19 Home Confinement: The ECLB-COVID19 Multicenter Study. PLoS ONE 2020, 15, e0240204. [Google Scholar] [CrossRef] [PubMed]
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from COVID-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef] [PubMed]
- Baenas, I.; Etxandi, M.; Munguía, L.; Granero, R.; Mestre-Bach, G.; Sánchez, I.; Ortega, E.; Andreu, A.; Moize, V.L.; Fernández-Real, J.-M.; et al. Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study. Nutrients 2021, 14, 100. [Google Scholar] [CrossRef]
- Molina-Montes, E.; Uzhova, I.; Verardo, V.; Artacho, R.; García-Villanova, B.; Jesús Guerra-Hernández, E.; Kapsokefalou, M.; Malisova, O.; Vlassopoulos, A.; Katidi, A.; et al. Impact of COVID-19 Confinement on Eating Behaviours across 16 European Countries: The COVIDiet Cross-National Study. Food Qual. Prefer. 2021, 93, 104231. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Globally Altered Sleep Patterns and Physical Activity Levels by Confinement in 5056 Individuals: ECLB COVID-19 International Online Survey. Biol. Sport 2021, 38, 495–506. [Google Scholar] [CrossRef]
- Mason, T.B.; Barrington-Trimis, J.; Leventhal, A.M. Eating to Cope With the COVID-19 Pandemic and Body Weight Change in Young Adults. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2021, 68, 277–283. [Google Scholar] [CrossRef]
- Lopez, K.V.; Garduño, A.M.J.; Regules, A.E.O.; Romero, L.M.I.; Martinez, O.A.G.; Pereira, T.S.S. Cambios en el estilo de vida y nutrición durante el confinamiento por SARS-CoV-2 (COVID-19) en México: Un estudio observacional. Rev. Esp. Nutr. Hum. Dietética 2021, 25, e1099. [Google Scholar] [CrossRef]
- Lamy, E.; Viegas, C.; Rocha, A.; Raquel Lucas, M.; Tavares, S.; Capela e Silva, F.; Guedes, D.; Laureati, M.; Zian, Z.; Salles Machado, A.; et al. Changes in Food Behavior during the First Lockdown of COVID-19 Pandemic: A Multi-Country Study about Changes in Eating Habits, Motivations, and Food-Related Behaviors. Food Qual. Prefer. 2022, 99, 104559. [Google Scholar] [CrossRef] [PubMed]
- Romeo-Arroyo, E.; Mora, M.; Vázquez-Araújo, L. Consumer Behavior in Confinement Times: Food Choice and Cooking Attitudes in Spain. Int. J. Gastron. Food Sci. 2020, 21, 100226. [Google Scholar] [CrossRef]
- Madalı, B.; Alkan, Ş.B.; Örs, E.D.; Ayrancı, M.; Taşkın, H.; Kara, H.H. Emotional Eating Behaviors during the COVID-19 Pandemic: A Cross-Sectional Study. Clin. Nutr. Espen 2021, 46, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased Emotional Eating during COVID-19 Associated with Lockdown, Psychological and Social Distress. Appetite 2021, 160, 105122. [Google Scholar] [CrossRef] [PubMed]
- Vacca, M.; De Maria, A.; Mallia, L.; Lombardo, C. Perfectionism and Eating Behavior in the COVID-19 Pandemic. Front. Psychol. 2021, 12, 580943. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Quaresma, M.V.; Marques, C.G.; Magalhães, A.C.O.; Dos Santos, R.V.T. Emotional Eating, Binge Eating, Physical Inactivity, and Vespertine Chronotype Are Negative Predictors of Dietary Practices during COVID-19 Social Isolation: A Cross-Sectional Study. Nutrition 2021, 90, 111223. [Google Scholar] [CrossRef] [PubMed]
- Almendra-Pegueros, R.; Baladia, E.; Contreras, C.R.; Cárdenas, P.R.; Martí, A.V.; Osorio, J.M.; Jiménez, E.A.; López, A.L.; Bonacich, K.B.; Nessier, M.C.; et al. Conducta alimentaria durante el confinamiento por COVID-19 (CoV-Eat Project): Protocolo de un estudio transversal en países de habla hispana. Rev. Nutr. Clínica Metab. 2021, 4, 267. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Jáuregui-Lobera, I.; García-Cruz, P.; Carbonero-Carreño, R.; Magallares, A.; Ruiz-Prieto, I. Psychometric Properties of Spanish Version of the Three-Factor Eating Questionnaire-R18 (Tfeq-Sp) and Its Relationship with Some Eating- and Body Image-Related Variables. Nutrients 2014, 6, 5619–5635. [Google Scholar] [CrossRef] [Green Version]
- Council for International Organizations of Medical Sciences (CIOMS). International Ethical Guidelines for Health-Related Research Involving Humans; Council for International Organizations of Medical Sciences (CIOMS): Geneva, Switzerland, 2016. [Google Scholar]
- Espelt, A.; Marí-Dell’Olmo, M.; Penelo, E.; Bosque-Prous, M. Applied Prevalence Ratio Estimation with Different Regression Models: An Example from a Cross-National Study on Substance Use Research. Adicciones 2016, 29, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Barros, A.J.D.; Hirakata, V.N. Alternatives for Logistic Regression in Cross-Sectional Studies: An Empirical Comparison of Models That Directly Estimate the Prevalence Ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Deddens, J.A.; Petersen, M.R. Approaches for Estimating Prevalence Ratios. Occup. Environ. Med. 2008, 65, 501–506. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Dosil-Santamaria, M.; Picaza-Gorrochategui, M.; Idoiaga-Mondragon, N. Stress, Anxiety, and Depression Levels in the Initial Stage of the COVID-19 Outbreak in a Population Sample in the Northern Spain. Cad. Saude Publica 2020, 36, e00054020. [Google Scholar] [CrossRef] [PubMed]
- Odriozola-González, P.; Planchuelo-Gómez, Á.; Irurtia, M.J.; de Luis-García, R. Psychological Effects of the COVID-19 Outbreak and Lockdown among Students and Workers of a Spanish University. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef] [PubMed]
- Caycho-Rodríguez, T.; Tomás, J.M.; Vilca, L.W.; Carbajal-León, C.; Cervigni, M.; Gallegos, M.; Martino, P.; Barés, I.; Calandra, M.; Anacona, C.A.R.; et al. Socio-Demographic Variables, Fear of COVID-19, Anxiety, and Depression: Prevalence, Relationships and Explanatory Model in the General Population of Seven Latin American Countries. Front. Psychol. 2021, 12, 695989. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, J.H.; Chung, J.H. The Association between Sleep Quality and Quality of Life: A Population-Based Study. Sleep Med. 2021, 84, 121–126. [Google Scholar] [CrossRef]
- Goldenberg, M.; Danovitch, I.; IsHak, W.W. Quality of Life and Smoking. Am. J. Addict. 2014, 23, 540–562. [Google Scholar] [CrossRef]
- Koopmann, A.; Georgiadou, E.; Reinhard, I.; Müller, A.; Lemenager, T.; Kiefer, F.; Hillemacher, T. The Effects of the Lockdown during the COVID-19 Pandemic on Alcohol and Tobacco Consumption Behavior in Germany. Eur. Addict. Res. 2021, 27, 242–256. [Google Scholar] [CrossRef]
- Martínez-Cao, C.; de la Fuente-Tomás, L.; Menéndez-Miranda, I.; Velasco, Á.; Zurrón-Madera, P.; García-Álvarez, L.; Sáiz, P.A.; Garcia-Portilla, M.P.; Bobes, J. Factors associated with alcohol and tobacco consumption as a coping strategy to deal with the coronavirus disease (COVID-19) pandemic and lockdown in Spain. Addict. Behav. 2021, 121, 107003. [Google Scholar] [CrossRef]
- Burr, D.A.; Castrellon, J.J.; Zald, D.H.; Samanez-Larkin, G.R. Emotion dynamics across adulthood in everyday life: Older adults are more emotionally stable and better at regulating desires. Emotion 2021, 21, 453–464. [Google Scholar] [CrossRef]
- Tibber, M.S.; Walji, F.; Kirkbride, J.B.; Huddy, V. The association between income inequality and adult mental health at the subnational level-a systematic review. Soc. Psychiatry Psychiatr Epidemiol. 2022, 57, 1–24. [Google Scholar] [CrossRef]
- Bilici, S.; Ayhan, B.; Karabudak, E.; Koksal, E. Factors affecting emotional eating and eating palatable food in adults. Nutr. Res. Pract. 2020, 14, 70–75. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, T.Y.; Bernal-Gómez, S.J.; Mora, A.; Hun, N.; Reyes-Castillo, Z.; Valdés-Miramontes, E.H.; Espinoza-Gallardo, A.C. Dysfunctional Patterns of Food Intake by Anxiety during Isolation by COVID-19 in Chile, Colombia and Mexico. Int. J. Psychol. Res. 2021, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Elmacıoğlu, F.; Emiroğlu, E.; Ülker, M.T.; Özyılmaz Kırcali, B.; Oruç, S. Evaluation of Nutritional Behaviour Related to COVID-19. Public Health Nutr. 2021, 24, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Ramalho, S.M.; Trovisqueira, A.; de Lourdes, M.; Gonçalves, S.; Ribeiro, I.; Vaz, A.R.; Machado, P.P.P.; Conceição, E. The Impact of COVID-19 Lockdown on Disordered Eating Behaviors: The Mediation Role of Psychological Distress. Eat. Weight Disord. EWD 2022, 27, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Burnatowska, E.; Surma, S.; Olszanecka-Glinianowicz, M. Relationship between Mental Health and Emotional Eating during the COVID-19 Pandemic: A Systematic Review. Nutrients 2022, 14, 3989. [Google Scholar] [CrossRef]
- Ghani, S.B.; Delgadillo, M.E.; Granados, K.; Okuagu, A.C.; Wills, C.C.A.; Alfonso-Miller, P.; Buxton, O.M.; Patel, S.R.; Ruiz, J.; Parthasarathy, S.; et al. Patterns of Eating Associated with Sleep Characteristics: A Pilot Study among Individuals of Mexican Descent at the US-Mexico Border. Behav. Sleep Med. 2022, 20, 212–223. [Google Scholar] [CrossRef]
- Zerón-Rugerio, M.F.; Hernáez, Á.; Cambras, T.; Izquierdo-Pulido, M. Emotional Eating and Cognitive Restraint Mediate the Association between Sleep Quality and BMI in Young Adults. Appetite 2022, 170, 105899. [Google Scholar] [CrossRef]
- St-Onge, M.-P.; McReynolds, A.; Trivedi, Z.B.; Roberts, A.L.; Sy, M.; Hirsch, J. Sleep Restriction Leads to Increased Activation of Brain Regions Sensitive to Food Stimuli. Am. J. Clin. Nutr. 2012, 95, 818–824. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | n = 9849 |
|---|---|
| Age in years, median (IR 1) | 31 (27; 43) |
| Sex (women), % | 80.1 |
| Marital status (with partner), % | 93.4 |
| Educational level (≤primary), % | 18.6 |
| Household income, % | |
| Lower | 17.1 |
| Medium | 75.6 |
| Higher | 7.3 |
| Number of people in home (>2), % | 66.5 |
| Days of confinement, median (IR) | 23 (17; 36) |
| Numbers time left their home in the last week, % | |
| 0 | 15.2 |
| 1 | 33.4 |
| >1 | 51.3 |
| Sleep quality, % | |
| As before | 46.4 |
| Higher | 11.7 |
| Lower | 41.9 |
| Physical activity, % | |
| As before | 21.5 |
| Higher | 16.2 |
| Lower | 62.3 |
| Screen use, % | |
| As before | 24.5 |
| Higher | 72.4 |
| Lower | 3.1 |
| Tobacco consumption, % | |
| Non-smoker | 64.9 |
| As before | 4.4 |
| Higher | 4.8 |
| Lower | 6.0 |
| Ex-smoker | 20.0 |
| Relationship with food, % | |
| As before | 47.6 |
| Different | 52.4 |
| <15 Points (n = 3593) | 15–16 Points (n = 3420) | >16 Points (n = 2836) | ||||||
|---|---|---|---|---|---|---|---|---|
| % | % | PR (95% CI) | p-Value | % | PR (95% CI) | p-Value | ||
| Age in years | 18–30 | 33.6 | 37.7 | 1.00 | 39.9 | 1.00 | ||
| 31–40 | 32.2 | 30.7 | 0.92 (0.86; 0.97) | 0.003 | 30.5 | 0.91 (0.85; 0.97) | 0.006 | |
| 41–65 | 34.3 | 31.6 | 0.90 (0.84; 0.95) | 0.001 | 29.6 | 0.83 (0.78; 0.89) | <0.001 | |
| Sex | Woman | 83.8 | 79.9 | 1.00 | 75.5 | 1.00 | ||
| Man | 16.2 | 20.1 | 1.14 (1.07; 1.21) | <0.001 | 24.5 | 1.30 (1.22; 1.38) | <0.001 | |
| Marital status | Coupled up | 92.7 | 93.9 | 1.00 | 93.8 | 1.00 | ||
| Single | 7.3 | 6.1 | 0.95 (0.85; 1.06) | 0.357 | 6.2 | 1.01 (0.90; 1.14) | 0.881 | |
| Education level | ≤primary | 18.5 | 17.3 | 1.00 | 20.1 | 1.00 | ||
| >primary | 81.5 | 82.7 | 1.05 (0.98; 1.12) | 0.191 | 79.9 | 0.97 (0.91; 1.04) | 0.371 | |
| Household income | Lower | 16.5 | 16.0 | 1.00 | 19.0 | 1.00 | ||
| Medium | 75.5 | 76.5 | 1.00 (0.94; 1.08) | 0.894 | 74.7 | 0.90 (0.84; 0.96) | 0.002 | |
| Higher | 8.0 | 7.5 | 0.96 (0.86; 1.07) | 0.458 | 6.3 | 0.80 (0.70; 0.91) | 0.001 | |
| People living at home | 0–2 | 33.1 | 34.5 | 1.00 | 32.8 | 1.00 | ||
| >2 | 66.9 | 65.5 | 0.96 (0.91; 1.01) | 0.128 | 67.2 | 0.98 (0.92; 1.04) | 0.493 | |
| Days of confinement | 7–21 days | 33.2 | 34.8 | 1.00 | 37.1 | 1.00 | ||
| 22–31 days | 31.8 | 33.1 | 0.98 (0.93; 1.04) | 0.587 | 33.0 | 0.92 (0.86; 0.98) | 0.010 | |
| >31 days | 35.0 | 32.1 | 0.96 (0.90; 1.02) | 0.166 | 29.9 | 0.90 (0.84; 0.97) | 0.003 | |
| Number of times leaving home during the last week | 0 | 13.9 | 15.3 | 1.00 | 16.9 | 1.00 | ||
| 1 | 33.6 | 33.6 | 0.95 (0.88; 1.02) | 0.177 | 33.0 | 0.91 (0.84; 0.98) | 0.014 | |
| >1 | 52.5 | 51.1 | 0.93 (0.86; 0.99) | 0.032 | 50.1 | 0.87 (0.81; 0.94) | <0.001 | |
| Sleep quality | As before | 41.7 | 46.1 | 1.00 | 52.7 | 1.00 | ||
| Higher | 12.4 | 11.4 | 0.92 (0.85; 1.00) | 0.047 | 11.1 | 0.88 (0.80; 0.96) | 0.004 | |
| Lower | 45.9 | 42.5 | 0.94 (0.90; 1.00) | 0.035 | 36.2 | 0.87 (0.82; 0.92) | <0.001 | |
| Physical activity | As before | 19.8 | 21.4 | 1.00 | 23.8 | 1.00 | ||
| Higher | 15.8 | 15.9 | 0.98 (0.90; 1.06) | 0.534 | 16.9 | 1.01 (0.93; 1.09) | 0.874 | |
| Lower | 64.3 | 62.7 | 0.99 (0.93; 1.05) | 0.668 | 59.2 | 0.97 (0.90; 1.03) | 0.283 | |
| Screen use | As before | 22.4 | 23.2 | 1.00 | 28.6 | 1.00 | ||
| Higher | 74.8 | 73.6 | 1.00 (0.94; 1.06) | 0.894 | 67.9 | 0.91 (0.85; 0.96) | 0.001 | |
| Lower | 2.8 | 3.2 | 1.11 (0.97; 1.28) | 0.125 | 3.5 | 1.08 (0.94; 1.24) | 0.288 | |
| Tobacco consumption | No smoker | 61.6 | 64.1 | 1.00 | 69.9 | 1.00 | ||
| As before | 4.5 | 4.5 | 0.99 (0.88; 1.11) | 0.813 | 4.1 | 0.88 (0.77; 1.01) | 0.075 | |
| Higher | 5.7 | 4.6 | 0.91 (0.80; 1.02) | 0.114 | 3.8 | 0.81 (0.69; 0.94) | 0.006 | |
| Lower | 6.3 | 6.0 | 0.97 (0.87; 1.07) | 0.538 | 5.5 | 0.87 (0.77; 0.98) | 0.020 | |
| Ex-smoker | 21.9 | 20.8 | 0.98 (0.92; 1.04) | 0.560 | 16.6 | 0.83 (0.77; 0.89) | <0.001 | |
| Relationship with food | As before | 39.9 | 46.1 | 1.00 | 59.1 | 1.00 | ||
| Different | 60.1 | 53.9 | 0.89 (0.85; 0.94) | <0.001 | 40.9 | 0.69 (0.65; 0.73) | <0.001 | |
| <9 Points (n = 4395) | 9–10 Points (n = 2874) | >10 Points (n = 2580) | ||||||
|---|---|---|---|---|---|---|---|---|
| % | % | PR (95% CI) | p-Value | % | PR (95% CI) | p-Value | ||
| Age in years | 18–30 | 38.9 | 37.9 | 1.00 | 32.0 | 1.00 | ||
| 31–40 | 32.7 | 29.2 | 0.95 (0.89; 1.02) | 0.172 | 30.9 | 0.95 (0.90; 1.00) | 0.032 | |
| 41–65 | 28.4 | 32.9 | 1.08 (1.01; 1.16) | 0.024 | 37.1 | 0.92 (0.87; 0.97) | 0.002 | |
| Sex | Women | 85.0 | 79.1 | 1.00 | 72.8 | 1.00 | ||
| Men | 15.0 | 20.9 | 1.22 (1.14; 1.3) | <0.001 | 27.2 | 1.11 (1.06; 1.17) | <0.001 | |
| Marital status | Coupled up | 93.7 | 93.6 | 1.00 | 92.6 | 1.00 | ||
| Single | 6.3 | 6.4 | 1.03 (0.92; 1.16) | 0.613 | 7.4 | 0.97 (0.89; 1.07) | 0.581 | |
| Education level | ≤primary | 19.3 | 16.9 | 1.00 | 19.2 | 1.00 | ||
| >primary | 80.7 | 83.1 | 1.09 (1.01; 1.18) | 0.024 | 80.8 | 1.02 (0.96; 1.08) | 0.508 | |
| Household income | Lower | 18.8 | 15.3 | 1.00 | 16.1 | 1.00 | ||
| Medium | 73.9 | 76.9 | 1.09 (1.00; 1.18) | 0.052 | 77.1 | 0.98 (0.92; 1.03) | 0.428 | |
| Higher | 7.4 | 7.8 | 1.07 (0.95; 1.22) | 0.268 | 6.8 | 0.94 (0.85; 1.04) | 0.223 | |
| People living at home | 0–2 | 33.1 | 33.9 | 1.00 | 33.9 | 1.00 | ||
| >2 | 66.9 | 66.1 | 0.98 (0.92; 1.04) | 0.518 | 66.1 | 0.99 (0.94; 1.03) | 0.594 | |
| Days of confinement | 7–21 days | 33.2 | 35.5 | 1.00 | 37.1 | 1.00 | ||
| 22–31 days | 30.9 | 33.2 | 0.97 (0.91; 1.04) | 0.361 | 34.7 | 0.98 (0.93; 1.03) | 0.391 | |
| >31 days | 35.9 | 31.3 | 0.93 (0.87; 1.00) | 0.047 | 28.2 | 0.97 (0.92; 1.02) | 0.202 | |
| Number of times leaving home during the last week | 0 | 14.9 | 14.7 | 1.00 | 16.4 | 1.00 | ||
| 1 | 34.2 | 33.1 | 0.98 (0.90; 1.07) | 0.651 | 32.6 | 0.95 (0.89; 1.01) | 0.087 | |
| >1 | 50.9 | 52.2 | 0.97 (0.89; 1.05) | 0.472 | 51.0 | 0.92 (0.87; 0.97) | 0.004 | |
| Sleep quality | As before | 39.7 | 49.5 | 1.00 | 54.5 | 1.00 | ||
| Higher | 11.2 | 11.6 | 0.96 (0.88; 1.05) | 0.38 | 12.6 | 0.92 (0.86; 0.99) | 0.023 | |
| Lower | 49.2 | 38.9 | 0.88 (0.82; 0.93) | <0.001 | 32.9 | 0.95 (0.91; 1.00) | 0.031 | |
| Physical activity | As before | 17.3 | 23.6 | 1.00 | 26.4 | 1.00 | ||
| Higher | 13.8 | 17.2 | 1.02 (0.94; 1.11) | 0.603 | 19.1 | 0.99 (0.92; 1.06) | 0.743 | |
| Lower | 68.9 | 59.2 | 0.86 (0.8; 0.92) | <0.001 | 54.5 | 0.99 (0.94; 1.04) | 0.747 | |
| Screen use | As before | 19.0 | 27.0 | 1.00 | 31.0 | 1.00 | ||
| Higher | 78.5 | 70.3 | 0.85 (0.80; 0.91) | <0.001 | 64.4 | 0.97 (0.92; 1.02) | 0.203 | |
| Lower | 2.5 | 2.7 | 0.99 (0.83; 1.17) | 0.867 | 4.6 | 1.05 (0.94; 1.18) | 0.375 | |
| Tobacco consumption | No smoker | 62.3 | 66.1 | 1.00 | 67.8 | 1.00 | ||
| As before | 4.2 | 4.5 | 1.00 (0.87; 1.14) | 0.969 | 4.7 | 0.97 (0.87; 1.08) | 0.596 | |
| Higher | 5.3 | 5.0 | 1.00 (0.88; 1.14) | 0.974 | 3.6 | 0.87 (0.78; 0.98) | 0.026 | |
| Lower | 6.6 | 5.6 | 0.92 (0.81; 1.05) | 0.222 | 5.4 | 0.94 (0.86; 1.03) | 0.184 | |
| Ex-smoker | 21.7 | 18.8 | 0.88 (0.82; 0.95) | 0.001 | 18.5 | 0.98 (0.93; 1.04) | 0.587 | |
| Relationship with food | As before | 32.9 | 53.1 | 1.00 | 66.5 | 1.00 | ||
| Different | 67.1 | 46.9 | 0.67 (0.63; 0.71) | <0.001 | 33.5 | 0.91 (0.87; 0.95) | <0.001 | |
| <24 Points (n = 4086) | 24–26 Points (n = 2508) | >26 Points (n = 3255) | ||||||
|---|---|---|---|---|---|---|---|---|
| % | % | PR (95% CI) | p-Value | % | PR (95% CI) | p-Value | ||
| Age in years | 18–30 | 40.8 | 36.4 | 32.1 | ||||
| 31–40 | 31.6 | 31.6 | 1.08 (1.00; 1.17) | 0.040 | 30.3 | 0.96 (0.91; 1.01) | 0.083 | |
| 41–65 | 27.6 | 31.9 | 1.18 (1.09; 1.28) | <0.001 | 37.5 | 0.93 (0.89; 0.98) | 0.007 | |
| Sex | Women | 80.3 | 79.6 | 80.2 | ||||
| Men | 19.7 | 20.4 | 0.98 (0.91; 1.06) | 0.573 | 19.8 | 1.11 (1.06; 1.16) | <0.001 | |
| Marital status | Coupled up | 94.1 | 93.6 | 92.4 | ||||
| Single | 5.9 | 6.4 | 1.03 (0.91; 1.17) | 0.634 | 7.6 | 0.97 (0.89; 1.06) | 0.565 | |
| Education level | ≤primary | 20.8 | 16.7 | 17.2 | ||||
| >primary | 79.2 | 83.3 | 1.16 (1.06; 1.26) | 0.001 | 82.8 | 1.01 (0.96; 1.06) | 0.757 | |
| Household income | Lower | 19.0 | 15.5 | 15.8 | ||||
| Medium | 74.3 | 76.6 | 1.06 (0.97; 1.16) | 0.195 | 76.4 | 1.00 (0.95; 1.06) | 0.897 | |
| Higher | 6.7 | 7.9 | 1.14 (1.00; 1.31) | 0.051 | 7.7 | 0.98 (0.89; 1.07) | 0.658 | |
| People living at home | 0–2 | 32.3 | 33.7 | 34.9 | ||||
| >2 | 67.7 | 66.3 | 0.97 (0.91; 1.03) | 0.329 | 65.1 | 0.98 (0.94; 1.02) | 0.299 | |
| Days of confinement | 7–21 days | 31.6 | 35.2 | 38.7 | ||||
| 22–31 days | 32.1 | 34.3 | 0.95 (0.88; 1.02) | 0.149 | 32.0 | 0.97 (0.93; 1.02) | 0.269 | |
| >31 days | 36.3 | 30.5 | 0.87 (0.81; 0.94) | <0.001 | 29.3 | 0.95 (0.91; 1.00) | 0.064 | |
| Number of times leaving home during the last week | 0 | 14.8 | 15.7 | 1.00 | 15.4 | 1.00 | ||
| 1 | 33.9 | 32.5 | 0.94 (0.85; 1.03) | 0.159 | 33.6 | 0.96 (0.91; 1.02) | 0.222 | |
| >1 | 51.2 | 51.8 | 0.93 (0.85; 1.02) | 0.131 | 51.0 | 0.94 (0.89; 1.00) | 0.033 | |
| Sleep quality | As before | 40.5 | 47.2 | 1.00 | 53.2 | 1.00 | ||
| Higher | 10.8 | 13.0 | 1.07 (0.97; 1.17) | 0.157 | 11.8 | 0.96 (0.90; 1.02) | 0.206 | |
| Lower | 48.7 | 39.7 | 0.90 (0.84; 0.96) | 0.002 | 35.1 | 0.95 (0.91; 0.99) | 0.029 | |
| Physical activity | As before | 17.9 | 23.2 | 1.00 | 24.9 | 1.00 | ||
| Higher | 13.3 | 17.4 | 1.06 (0.96; 1.16) | 0.249 | 18.8 | 1.01 (0.94; 1.07) | 0.844 | |
| Lower | 68.8 | 59.4 | 0.86 (0.80; 0.93) | <0.001 | 56.3 | 1.00 (0.95; 1.05) | 0.911 | |
| Screen use | As before | 19.0 | 25.3 | 1.00 | 30.7 | 1.00 | ||
| Higher | 78.7 | 71.5 | 0.86 (0.81; 0.92) | <0.001 | 65.1 | 0.99 (0.94; 1.04) | 0.634 | |
| Lower | 2.3 | 3.2 | 1.11 (0.93; 1.32) | 0.237 | 4.1 | 1.09 (0.98; 1.21) | 0.124 | |
| Tobacco consumption | No smoker | 62.2 | 64.7 | 1.00 | 68.4 | 1.00 | ||
| As before | 4.3 | 4.3 | 0.97 (0.84; 1.12) | 0.682 | 4.5 | 0.98 (0.89; 1.08) | 0.723 | |
| Higher | 5.7 | 4.5 | 0.90 (0.77; 1.05) | 0.186 | 3.7 | 0.93 (0.84; 1.03) | 0.169 | |
| Lower | 6.9 | 5.8 | 0.93 (0.81; 1.07) | 0.306 | 5.0 | 0.95 (0.86; 1.04) | 0.226 | |
| Ex-smoker | 20.9 | 20.7 | 0.95 (0.88; 1.03) | 0.198 | 18.4 | 0.98 (0.93; 1.03) | 0.396 | |
| Relationship with food | As before | 34.1 | 49.3 | 1.00 | 63.2 | 1.00 | ||
| Different | 65.9 | 50.7 | 0.73 (0.69; 0.78) | <0.001 | 36.8 | 0.90 (0.86; 0.94) | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vila-Marti, A.; Ramírez-Contreras, C.; Apolinar-Jiménez, E.; Rojas-Cárdenas, P.; Valera-Gran, D.; Almendra-Pegueros, R.; Navarrete-Muñoz, E.M. Factors Associated with Dietary Restriction and Emotional and Uncontrolled Eating in Adults from Spanish-Speaking Countries during the COVID-19 Confinement: Results of the CoV-Eat Project. Nutrients 2022, 14, 4866. https://doi.org/10.3390/nu14224866
Vila-Marti A, Ramírez-Contreras C, Apolinar-Jiménez E, Rojas-Cárdenas P, Valera-Gran D, Almendra-Pegueros R, Navarrete-Muñoz EM. Factors Associated with Dietary Restriction and Emotional and Uncontrolled Eating in Adults from Spanish-Speaking Countries during the COVID-19 Confinement: Results of the CoV-Eat Project. Nutrients. 2022; 14(22):4866. https://doi.org/10.3390/nu14224866
Chicago/Turabian StyleVila-Marti, Anna, Catalina Ramírez-Contreras, Evelia Apolinar-Jiménez, Pía Rojas-Cárdenas, Desirée Valera-Gran, Rafael Almendra-Pegueros, and Eva María Navarrete-Muñoz. 2022. "Factors Associated with Dietary Restriction and Emotional and Uncontrolled Eating in Adults from Spanish-Speaking Countries during the COVID-19 Confinement: Results of the CoV-Eat Project" Nutrients 14, no. 22: 4866. https://doi.org/10.3390/nu14224866