
Dietary Pattern Associated with the Risk of Hyperuricemia in Chinese Elderly: Result from China Nutrition and Health Surveillance 2015–2017

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Basic Information Interview
2.3. Dietary Assessment
2.4. Clinical Examination
2.5. Laboratory Test
2.6. Definition of HUA and Other NCDs
2.7. Covariates
2.8. Dietary Pattern
2.9. Nutrient Intake Assessment
2.10. Statistical Analysis
3. Results
3.1. Characteristics of Participants
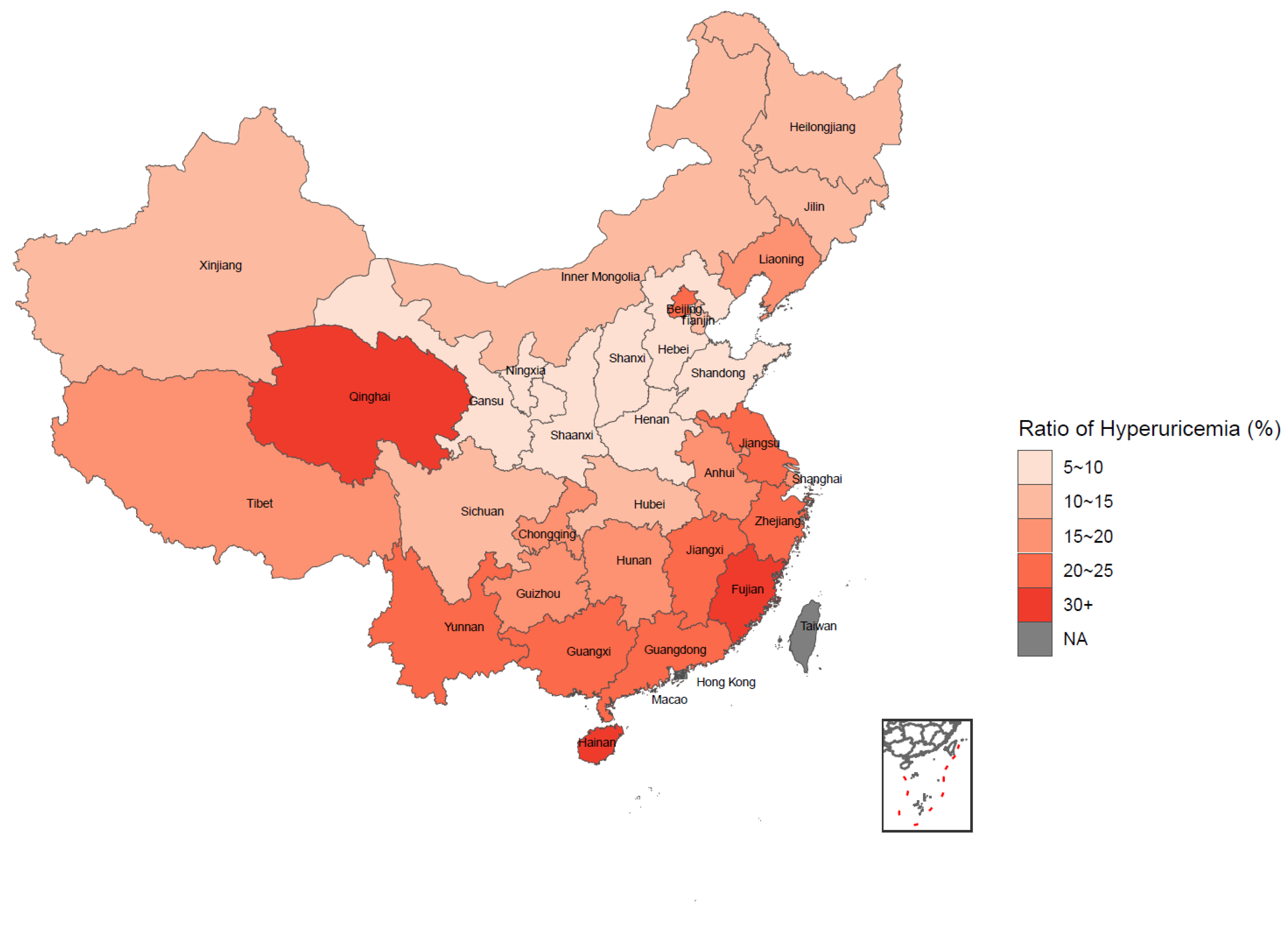
3.2. Weighted Prevalence of HUA and Its Distribution
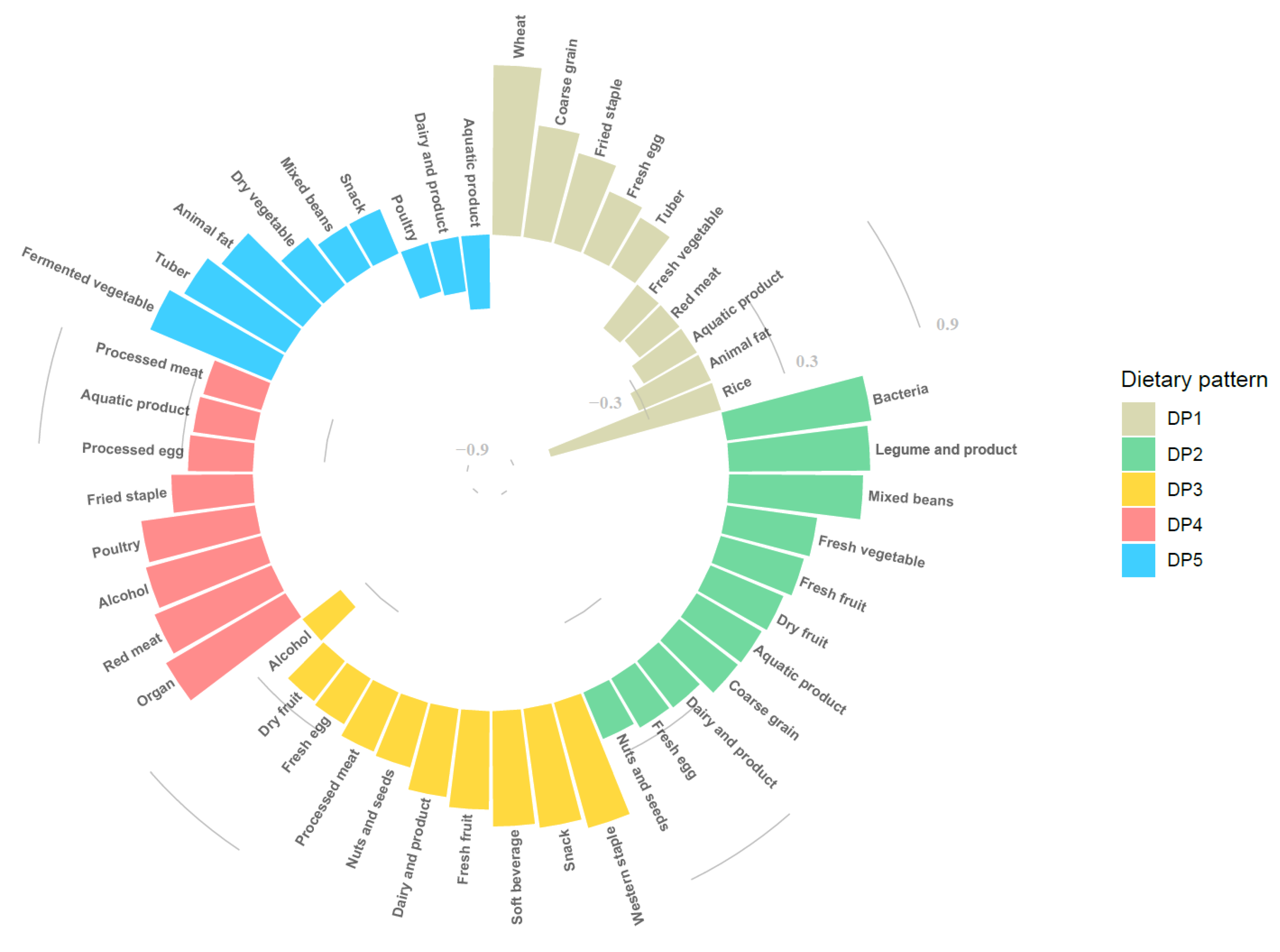
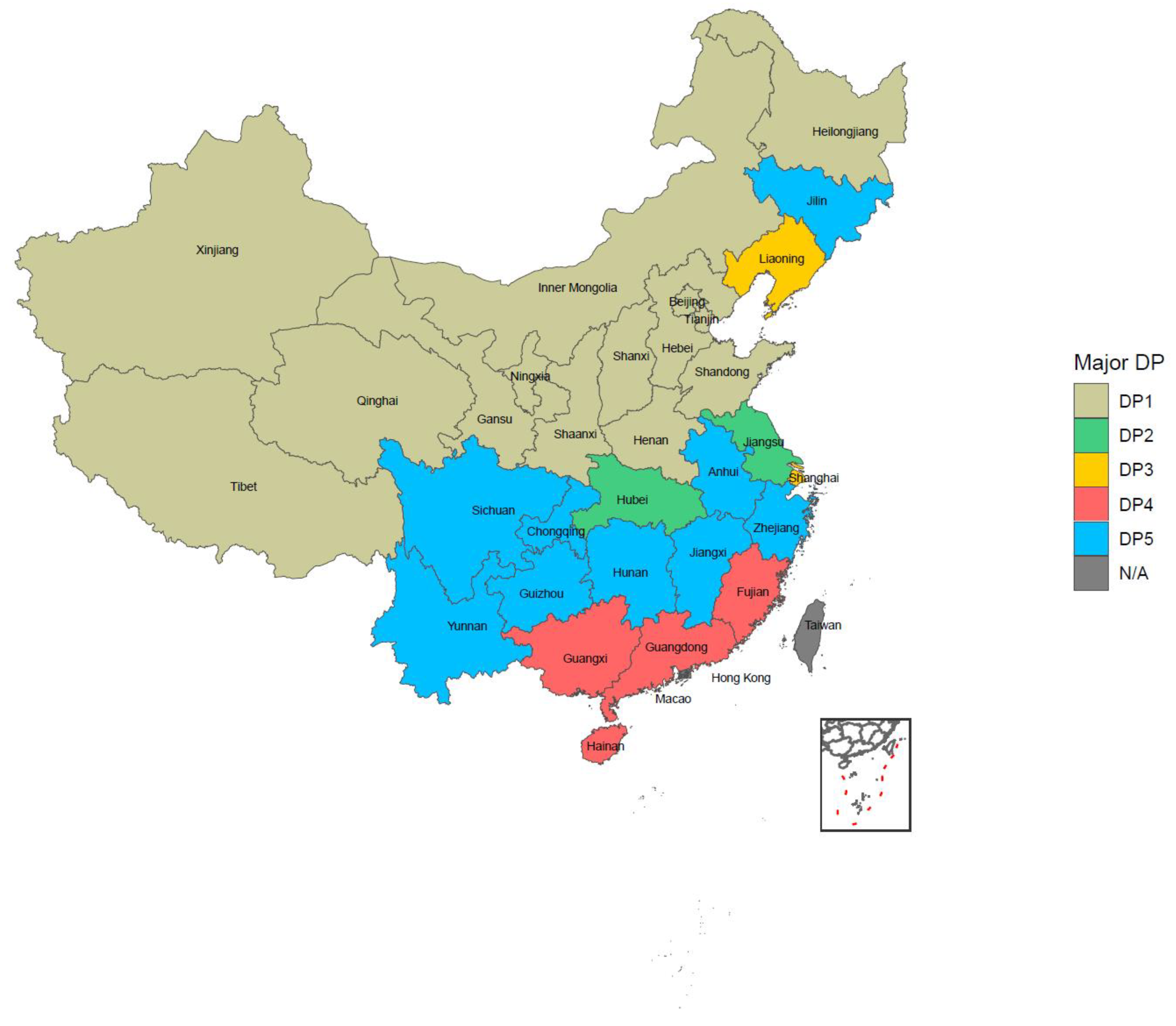
3.3. Dietary Patterns among Chinese Elderly
3.4. Association between Dietary Patterns and Hyperuricemia
3.5. Proportion of Participants Who Reached RNI/AI under Each Dietary Pattern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Escudero-Lopez, B.; Ortega, A.; Cerrillo, I.; Rodriguez-Grinolo, M.R.; Munoz-Hernandez, R.; Macher, H.C.; Martin, F.; Hornero-Mendez, D.; Mena, P.; Del Rio, D.; et al. Consumption of orange fermented beverage improves antioxidant status and reduces peroxidation lipid and inflammatory markers in healthy humans. J. Sci. Food Agric. 2018, 98, 2777–2786. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Sun, J.; Zhang, P.; Zhong, F.; Cai, J.; Ma, A. Association of dietary fiber intake with hyperuricemia in U.S. adults. Food Funct. 2019, 10, 4932–4940. [Google Scholar] [CrossRef] [PubMed]
- Bruins, M.J.; Van Dael, P.; Eggersdorfer, M. The Role of Nutrients in Reducing the Risk for Noncommunicable Diseases during Aging. Nutrients 2019, 11, 85. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Song, P.K.; Zhao, L.Y.; Sun, Y.; Yu, K.; Yin, J.; Pang, S.J.; Liu, Z.; Man, Q.Q.; He, L.; et al. Malnutrition in Relation with Dietary, Geographical, and Socioeconomic Factors among Older Chinese. Biomed. Environ. Sci. 2021, 34, 337–347. [Google Scholar] [CrossRef]
- Song, P.; Wang, H.; Xia, W.; Chang, X.; Wang, M.; An, L. Prevalence and correlates of hyperuricemia in the middle-aged and older adults in China. Sci. Rep. 2018, 8, 4314. [Google Scholar] [CrossRef]
- Choi, H.K.; Liu, S.; Curhan, G. Intake of purine-rich foods, protein, and dairy products and relationship to serum levels of uric acid: The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2005, 52, 283–289. [Google Scholar] [CrossRef]
- Rudnicka, E.; Napierala, P.; Podfigurna, A.; Meczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Juraschek, S.P.; Gelber, A.C.; Choi, H.K.; Appel, L.J.; Miller, E.R., 3rd. Effects of the Dietary Approaches to Stop Hypertension (DASH) Diet and Sodium Intake on Serum Uric Acid. Arthritis Rheumatol. 2016, 68, 3002–3009. [Google Scholar] [CrossRef] [Green Version]
- Kakutani-Hatayama, M.; Kadoya, M.; Okazaki, H.; Kurajoh, M.; Shoji, T.; Koyama, H.; Tsutsumi, Z.; Moriwaki, Y.; Namba, M.; Yamamoto, T. Nonpharmacological Management of Gout and Hyperuricemia: Hints for Better Lifestyle. Am. J. Lifestyle Med. 2017, 11, 321–329. [Google Scholar] [CrossRef]
- Zhang, T.; Rayamajhi, S.; Meng, G.; Zhang, Q.; Liu, L.; Wu, H.; Gu, Y.; Wang, Y.; Zhang, S.; Wang, X.; et al. Dietary patterns and risk for hyperuricemia in the general population: Results from the TCLSIH cohort study. Nutrition 2022, 93, 111501. [Google Scholar] [CrossRef]
- Kontogianni, M.D.; Chrysohoou, C.; Panagiotakos, D.B.; Tsetsekou, E.; Zeimbekis, A.; Pitsavos, C.; Stefanadis, C. Adherence to the Mediterranean diet and serum uric acid: The ATTICA study. Scand. J. Rheumatol. 2012, 41, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Fung, T.T.; Lu, N.; Keller, S.F.; Curhan, G.C.; Choi, H.K. The Dietary Approaches to Stop Hypertension (DASH) diet, Western diet, and risk of gout in men: Prospective cohort study. BMJ 2017, 357, j1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, O.; Miller, E.R., 3rd; Gelber, A.C.; Choi, H.K.; Appel, L.J.; Juraschek, S.P. DASH diet and change in serum uric acid over time. Clin. Rheumatol. 2017, 36, 1413–1417. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L.; et al. China Nutrition and Health Surveys (1982–2017). China CDC Wkly. 2021, 3, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.X. China Food Composition Tables, Standard Edition; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Yang, Y.X.; Wang, G.Y.; Pan, X.C. China Food Composition, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Chang, J.L.; Wang, Y.; Liang, X.F.; Wu, L.Y.; Ding, G.Q. Report of Chinese Residents’ Nutrition and Health Surveillance 2010–2013; Peking University Medical Press: Beijing, China, 2016. [Google Scholar]
- Pan, L.; Yang, Z.; Wu, Y.; Yin, R.X.; Liao, Y.; Wang, J.; Gao, B.; Zhang, L. China National Survey of Chronic Kidney Disease Working, G. The prevalence, awareness, treatment and control of dyslipidemia among adults in China. Atherosclerosis 2016, 248, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Lyu, J.; He, P. Chinese guidelines for data processing and analysis concerning the International Physical Activity Questionnaire. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 961–964. [Google Scholar] [PubMed]
- Li, C.; Kang, B.; Zhang, T.; Gu, H.; Song, P.; Chen, J.; Wang, X.; Xu, B.; Zhao, W.; Zhang, J. Dietary Pattern and Dietary Energy from Fat Associated with Sarcopenia in Community-Dwelling Older Chinese People: A Cross-Sectional Study in Three Regions of China. Nutrients 2020, 12, 3689. [Google Scholar] [CrossRef]
- Pearson, K.E.; Wadley, V.G.; McClure, L.A.; Shikany, J.M.; Unverzagt, F.W.; Judd, S.E. Dietary patterns are associated with cognitive function in the REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort. J. Nutr. Sci. 2016, 5, e38. [Google Scholar] [CrossRef] [Green Version]
- Marti del Moral, L.; Agil, A.; Navarro-Alarcon, M.; Lopez-Ga de la Serrana, H.; Palomares-Bayo, M.; Oliveras-Lopez, M.J. Altered serum selenium and uric acid levels and dyslipidemia in hemodialysis patients could be associated with enhanced cardiovascular risk. Biol. Trace Elem. Res. 2011, 144, 496–503. [Google Scholar] [CrossRef]
- Sun, Y.; Sun, J.; Wang, J.; Gao, T.; Zhang, H.; Ma, A. Association between vitamin C intake and risk of hyperuricemia in US adults. Asia Pac. J. Clin. Nutr. 2018, 27, 1271–1276. [Google Scholar] [CrossRef]
- Vatsalya, V.; Li, F.; Frimodig, J.; Shah, N.; Sutrawe, A.; Feng, W. Efficacy of Thiamine and Medical Management in Treating Hyperuricemia in AUD Patients with ALD: Role of Hyperuricemia in Liver Injury, Gut-Barrier Dysfunction, and Inflammation. Clin. Exp. Pharmacol. 2021, 11 (Suppl. S7), 001. [Google Scholar] [PubMed]
- Zhang, L.; Shi, X.; Yu, J.; Zhang, P.; Ma, P.; Sun, Y. Dietary Vitamin E Intake Was Inversely Associated with Hyperuricemia in US Adults: NHANES 2009–2014. Ann. Nutr. Metab. 2020, 76, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, Y.; Qiu, H. Association between Dietary Zinc Intake and Hyperuricemia among Adults in the United States. Nutrients 2018, 10, 568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Qiu, H. Dietary Magnesium Intake and Hyperuricemia among US Adults. Nutrients 2018, 10, 296. [Google Scholar] [CrossRef] [Green Version]
- Martinez de Victoria, E. Calcium, essential for health. Nutr. Hosp. 2016, 33, 341. [Google Scholar] [CrossRef] [Green Version]
- Chinese Nutrition Society. Chinese Dietary Guidelines Summary (2016); People’s Medical Publishing House: Beijing, China, 2016. [Google Scholar]
- Choi, H.K. A prescription for lifestyle change in patients with hyperuricemia and gout. Curr. Opin. Rheumatol. 2010, 22, 165–172. [Google Scholar] [CrossRef]
- Mena-Sanchez, G.; Babio, N.; Becerra-Tomas, N.; Martinez-Gonzalez, M.A.; Diaz-Lopez, A.; Corella, D.; Zomeno, M.D.; Romaguera, D.; Vioque, J.; Alonso-Gomez, A.M.; et al. Association between dairy product consumption and hyperuricemia in an elderly population with metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 214–222. [Google Scholar] [CrossRef]
- Singh, J.A.; Shah, N.; Edwards, N.L. A cross-sectional internet-based patient survey of the management strategies for gout. BMC Complement. Altern. Med. 2016, 16, 90. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Chang, H.; Gao, Y.; Wang, X.; Xu, W.; Liu, D.; Li, G.; Huang, G. Major dietary patterns and risk of asymptomatic hyperuricemia in Chinese adults. J. Nutr. Sci. Vitaminol. 2012, 58, 339–345. [Google Scholar] [CrossRef] [Green Version]
- He, F.; Wang, L.L.; Yu, X.L. Dietary patterns associated hyperuricemia among Chinese aged 45 to 59 years: An observational study. Medicine (Baltimore) 2017, 96, e9248. [Google Scholar] [CrossRef]
- Zgaga, L.; Theodoratou, E.; Kyle, J.; Farrington, S.M.; Agakov, F.; Tenesa, A.; Walker, M.; McNeill, G.; Wright, A.F.; Rudan, I.; et al. The association of dietary intake of purine-rich vegetables, sugar-sweetened beverages and dairy with plasma urate, in a cross-sectional study. PLoS ONE 2012, 7, e38123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayachandran, M.; Xiao, J.; Xu, B. A Critical Review on Health Promoting Benefits of Edible Mushrooms through Gut Microbiota. Int. J. Mol. Sci. 2017, 18, 1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.Y.; Jeong, J.K.; Lee, Y.E.; Daily, J.W., 3rd. Health benefits of kimchi (Korean fermented vegetables) as a probiotic food. J. Med. Food 2014, 17, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Zhang, C.; Zeng, X.; Yuan, Z. Microecological treatment of hyperuricemia using Lactobacillus from pickles. BMC Microbiol. 2020, 20, 195. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | Total | |
|---|---|---|---|
| N (%) | 9332 (49.93) | 9359 (50.07) | 18,691 |
| Age (years) * | 66.89 (63.19, 72.10) | 66.11 (62.77, 71.18) | 66.51 (62.97, 71.69) |
| BMI (kg/m2) * | 23.68 (21.36, 26.11) | 24.25 (21.91, 26.81) | 23.96 (21.62, 26.46) |
| Urban or rural * | |||
| Urban | 4148 (44.45) | 4365 (46.64) | 8513 (45.55) |
| Rural | 5184 (55.55) | 4994 (53.36) | 10,178 (54.45) |
| Education* | |||
| Primary school or below | 5462 (58.53) | 7171 (76.62) | 12,633 (67.59) |
| Middle school | 2436 (26.1) | 1417 (15.14) | 3853 (20.61) |
| High school or higher | 1434 (15.37) | 771 (8.24) | 2205 (11.8) |
| Income (CNY) | |||
| Low | 3819 (40.92) | 3710 (39.64) | 7529 (40.28) |
| Medium | 3384 (36.26) | 3465 (37.02) | 6849 (36.64) |
| High | 2129 (22.81) | 2184 (23.34) | 4313 (23.08) |
| Marital status * | |||
| Living with spouse | 8712 (93.36) | 8004 (85.52) | 16,716 (89.43) |
| Other status | 620 (6.64) | 1355 (14.48) | 1975 (10.57) |
| Current smoker * | |||
| No | 5071 (54.34) | 8959 (95.73) | 14,030 (75.06) |
| Yes | 4261 (45.66) | 400 (4.27) | 4661 (24.94) |
| Alcohol drinking * | |||
| No | 4684 (50.19) | 8126 (86.83) | 12,810 (68.54) |
| Yes | 4648 (49.81) | 1233 (13.17) | 5881 (31.46) |
| Physical activity * | |||
| Low | 2358 (25.27) | 2092 (22.35) | 4450 (23.81) |
| Moderate | 2502 (26.81) | 2489 (26.59) | 4991 (26.7) |
| High | 4472 (47.92) | 4778 (51.05) | 9250 (49.49) |
| Sedentary behavior (h) * | |||
| 0~<2 | 1066 (11.42) | 1340 (14.32) | 2406 (12.87) |
| 2~3 | 3399 (36.42) | 3483 (37.22) | 6882 (36.82) |
| ≥4 | 4867 (52.15) | 4536 (48.47) | 9403 (50.31) |
| Sleeping time (h) * | |||
| 0~<6 | 912 (9.77) | 1368 (14.62) | 2280 (12.2) |
| 6~9 | 7131 (76.41) | 6904 (73.77) | 14,035 (75.09) |
| ≥10 | 1289 (13.81) | 1087 (11.61) | 2376 (12.71) |
| NCDs * | |||
| Less than one disease | 5629 (60.32) | 5224 (55.82) | 10,853 (58.07) |
| Over two diseases | 3703 (39.68) | 4135 (44.18) | 7838 (41.93) |
| Glu (mmol/L) * | 5.35 (4.92, 5.91) | 5.39 (4.99, 5.98) | 5.37 (4.96, 5.94) |
| Tc (mmol/L) * | 4.69 (4.12, 5.31) | 5.07 (4.47, 5.72) | 4.87 (4.27, 5.53) |
| Tg (mmol/L) * | 1.14 (0.8, 1.67) | 1.37 (0.98, 1.97) | 1.25 (0.88, 1.83) |
| LDL (mmol/L) * | 2.89 (2.37, 3.44) | 3.19 (2.64, 3.78) | 3.03 (2.49, 3.61) |
| HDL (mmol/L) * | 1.24 (1.03, 1.49) | 1.29 (1.09, 1.52) | 1.27 (1.06, 1.51) |
| HbA1c (%) * | 5.1 (4.6, 5.5) | 5.2 (4.7, 5.6) | 5.1 (4.7, 5.5) |
| SBP (mmHg) * | 142 (129.67, 157) | 144.33 (130.67, 160.33) | 143 (130, 158.67) |
| DBP (mmHg) * | 80.67 (73.67, 88) | 78 (71, 85.67) | 79.33 (72, 87) |
| SUA (μmmol/L) * | 333 (281, 392.6) | 275.9 (233, 328.3) | 303.4 (252.3, 364.3) |
| Prevalence %, (95% CI) | p-Value | |
|---|---|---|
| Total | 15.73 (14.47, 16.99) | |
| Gender | 0.3294 | |
| Male | 16.19 (14.62, 17.76) | |
| Female | 15.26 (13.69, 16.83) | |
| Age (years) | <0.0001 | |
| 60~79 | 14.96 (13.72, 16.20) | |
| ≥80 | 23.4 (19.40, 27.40) | |
| BMI | <0.0001 | |
| Underweight | 6.81 (4.46, 9.16) | |
| Normal | 11.04 (9.72, 12.36) | |
| Overweight | 19.39 (17.67, 21.11) | |
| Obese | 24.78 (21.61, 27.95) | |
| Education | 0.0033 | |
| Primary school or below | 14.8 (13.37, 16.24) | |
| Middle school | 17.11 (14.87, 19.35) | |
| High school or higher | 18.93 (16.42, 21.43) | |
| Income (CNY) | <0.0001 | |
| Low | 12.12 (10.66, 13.59) | |
| Medium | 16.07 (14.41, 17.72) | |
| High | 21.02 (18.67, 23.37) | |
| Marital status | 0.6513 | |
| Living with spouse | 15.65 (14.38, 16.91) | |
| Other status | 16.29 (13.38, 19.20) | |
| Current smoker | 0.27 | |
| No | 16.02 (14.69, 17.36) | |
| Yes | 14.84 (12.81, 16.87) | |
| Alcohol drinking | 0.0019 | |
| No | 14.79 (13.37, 16.13) | |
| Yes | 17.85 (15.93, 19.78) | |
| Physical activity | 0.0743 | |
| Low | 16.12 (14.09, 18.16) | |
| Moderate | 17.02 (15.04, 19.01) | |
| High | 14.72 (13.35, 16.09) | |
| Sedentary behavior (h) | 0.0004 | |
| <2 | 11.34 (9.32, 13.36) | |
| 2~3 | 15.55 (13.81, 17.29) | |
| ≥4 | 17 (15.25, 18.76) | |
| Sleeping time (h) | 0.3426 | |
| <6 | 15.33 (12.73, 17.93) | |
| 6~9 | 15.42 (14.08, 16.77) | |
| ≥10 | 17.59 (14.19, 20.99) | |
| NCDs | <0.0001 | |
| Less than one disease | 11.24 (10.12, 12.37) | |
| Over two diseases | 21.52 (19.58, 23.45) |
| Dietary Pattern | Group of Quartile | No. of Cases | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |||
| Typical Chinese | Q1 | 899 | reference | reference | reference |
| Q2 | 982 | 1.13 (1.02, 1.25) | 1.06 (0.96, 1.18) | 1.00 (0.90, 1.12) | |
| Q3 | 742 | 0.8 (0.72, 0.89) | 0.66 (0.59, 0.74) | 0.60 (0.53, 0.68) | |
| Q4 | 415 | 0.41 (0.37, 0.47) | 0.34 (0.30, 0.38) | 0.32 (0.28, 0.37) | |
| p for trend | - | <0.0001 | <0.0001 | <0.0001 | |
| Modern Chinese | Q1 | 706 | reference | reference | reference |
| Q2 | 784 | 1.14 (1.02, 1.28) | 1.13 (1.01, 1.27) | 1.10 (0.98, 1.23) | |
| Q3 | 798 | 1.17 (1.05, 1.31) | 1.13 (1.01, 1.26) | 1.04 (0.92, 1.17) | |
| Q4 | 750 | 1.08 (0.97, 1.21) | 0.96 (0.86, 1.08) | 0.81 (0.71, 0.93) | |
| p for trend | - | 0.1462 | 0.4453 | 0.0021 | |
| Western | Q1 | 726 | reference | reference | reference |
| Q2 | 733 | 1.02 (0.91, 1.14) | 1.03 (0.92, 1.16) | 1.05 (0.93, 1.18) | |
| Q3 | 734 | 1.02 (0.92, 1.14) | 0.99 (0.88, 1.10) | 0.97 (0.86, 1.09) | |
| Q4 | 845 | 1.21 (1.09, 1.35) | 1.11 (1.00, 1.24) | 1.04 (0.93, 1.17) | |
| p for trend | - | 0.0009 | 0.1207 | 0.8218 | |
| Animal products and alcohol | Q1 | 651 | reference | reference | reference |
| Q2 | 733 | 1.16 (1.04, 1.30) | 1.19 (1.06, 1.33) | 1.18 (1.05, 1.32) | |
| Q3 | 773 | 1.24 (1.10, 1.38) | 1.27 (1.13, 1.42) | 1.25 (1.11, 1.41) | |
| Q4 | 881 | 1.45 (1.30, 1.62) | 1.49 (1.33, 1.68) | 1.49 (1.31, 1.70) | |
| p for trend | - | <0.0001 | <0.0001 | <0.0001 | |
| Tuber and fermented vegetables | Q1 | 899 | reference | reference | reference |
| Q2 | 769 | 0.84 (0.75, 0.93) | 0.87 (0.78, 0.97) | 0.91 (0.82, 1.02) | |
| Q3 | 735 | 0.79 (0.71, 0.88) | 0.85 (0.76, 0.95) | 0.89 (0.80, 1.00) | |
| Q4 | 635 | 0.67 (0.60, 0.75) | 0.73 (0.65, 0.82) | 0.78 (0.69, 0.88) | |
| p for trend | - | <0.0001 | <0.0001 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Piao, W.; Huang, K.; Fang, H.; Ju, L.; Zhao, L.; Yu, D.; Ma, Y. Dietary Pattern Associated with the Risk of Hyperuricemia in Chinese Elderly: Result from China Nutrition and Health Surveillance 2015–2017. Nutrients 2022, 14, 844. https://doi.org/10.3390/nu14040844
Yang Y, Piao W, Huang K, Fang H, Ju L, Zhao L, Yu D, Ma Y. Dietary Pattern Associated with the Risk of Hyperuricemia in Chinese Elderly: Result from China Nutrition and Health Surveillance 2015–2017. Nutrients. 2022; 14(4):844. https://doi.org/10.3390/nu14040844
Chicago/Turabian StyleYang, Yuxiang, Wei Piao, Kun Huang, Hongyun Fang, Lahong Ju, Liyun Zhao, Dongmei Yu, and Yanan Ma. 2022. "Dietary Pattern Associated with the Risk of Hyperuricemia in Chinese Elderly: Result from China Nutrition and Health Surveillance 2015–2017" Nutrients 14, no. 4: 844. https://doi.org/10.3390/nu14040844