
Effects of Mindful Eating in Patients with Obesity and Binge Eating Disorder
 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethical Aspects
2.2. Study Design
2.3. Participants
2.4. Study Protocol
2.5. Instruments
- Clinical and sociodemographic protocol: collects general clinical assessment information (signs, symptoms, disease, family history, dietary habits, and water intake), socioeconomic level, race, sex, age, occupation, educational degree, and other general information [24];
- “Quality of Life Scale WHOQOL-Bref”: evaluates the patient’s quality of life and consists of 26 questions on a Likert scale. This questionnaire is divided into 4 domains—physical, psychological, social, and environmental. According to the classification, a higher percentage indicates a better quality of life (range of scale values = minimum 0% and maximum 100%). The Cronbach’s alpha coefficient of the WHOQOL-BREF was 0.89. Internal reliability for all domains was above 0.70 [25]. This questionnaire was also translated into and validated in Brazilian Portuguese and its Cronbach’s alpha coefficient was 0.77 for the domains and 0.91 for the questions [26];
- “Body Shape Questionnaire (BSQ)”: measures satisfaction and concern with body shape, consisting of 34 items on a 6-point Likert scale. According to the classification, to be classified as “satisfied with your body shape”, a score <111 is necessary (range of scale values = minimum 34 points and maximum 204 points). Internal consistency, calculated in terms of Cronbach’s alpha, was 0.94 [27]. This questionnaire was also translated into and validated in Brazilian Portuguese and its Cronbach’s alpha coefficient was 0.97 [28];
- “Binge Eating Scale (BES)”: quantifies the severity of binge eating, cognitions, feelings, and behaviors, consisting of 16 items in a 4-point Likert format and 62 statements that best represent the individual’s response. Each statement corresponds to a number of points from 0 to 3, ranging from the absence (“0”) to the maximum severity (“3”) of binge eating. The final score is the result of the sum of the points for each item. According to the classification, individuals with a score less than or equal to 17 are classified as “Without Binge Eating”. Individuals with a score between 18 and 26 are considered to have “Moderate Binge Eating”, and those with a score greater than or equal to 27 are classified as “Severe Binge Eating” (range of scale values = minimum 0 points and maximum 48 points). The internal consistency, calculated in terms of Cronbach’s alpha, was 0.89 [29]. This questionnaire was also translated into and validated in Brazilian Portuguese and its Cronbach’s alpha coefficient was 0.85 [30].Authorization and consent were obtained from all authors of the questionnaires and protocols that were applied in this study.
2.6. Data Collection, Considerations, and Additional Information
2.7. Data Analysis
3. Results
3.1. Sociodemographic Data
3.2. Weight
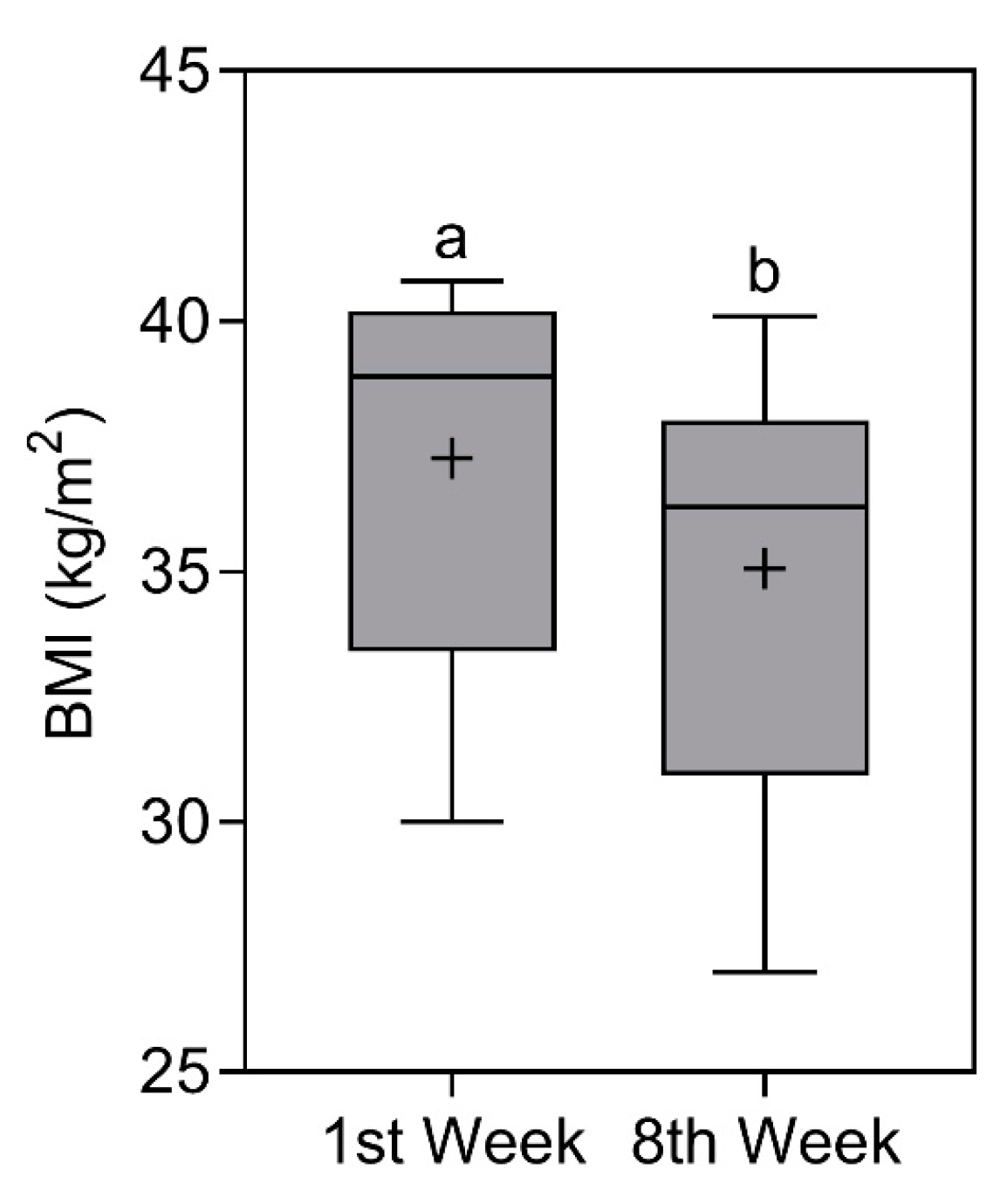
3.3. Body Mass Index (BMI)
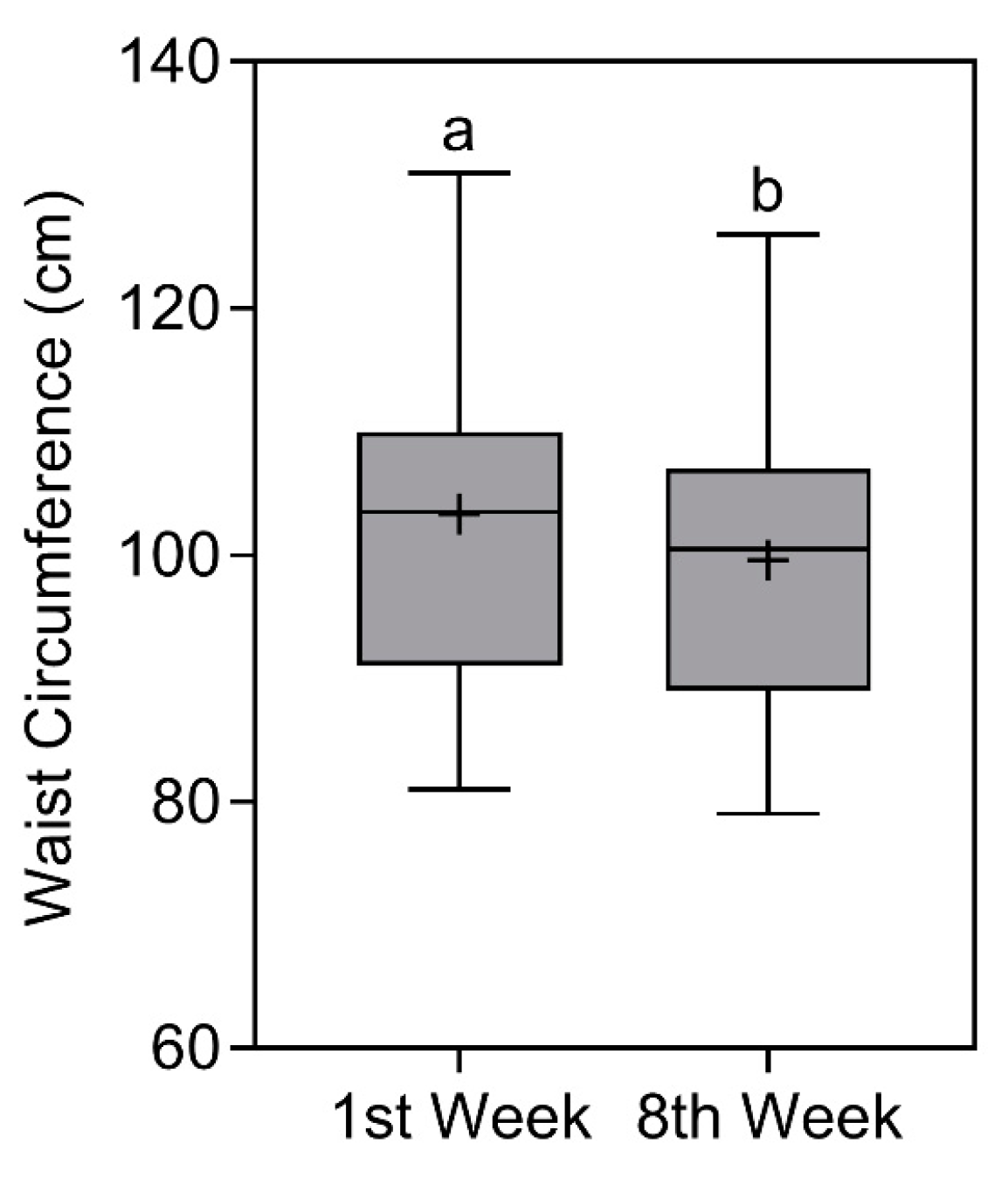
3.4. Waist Circumference
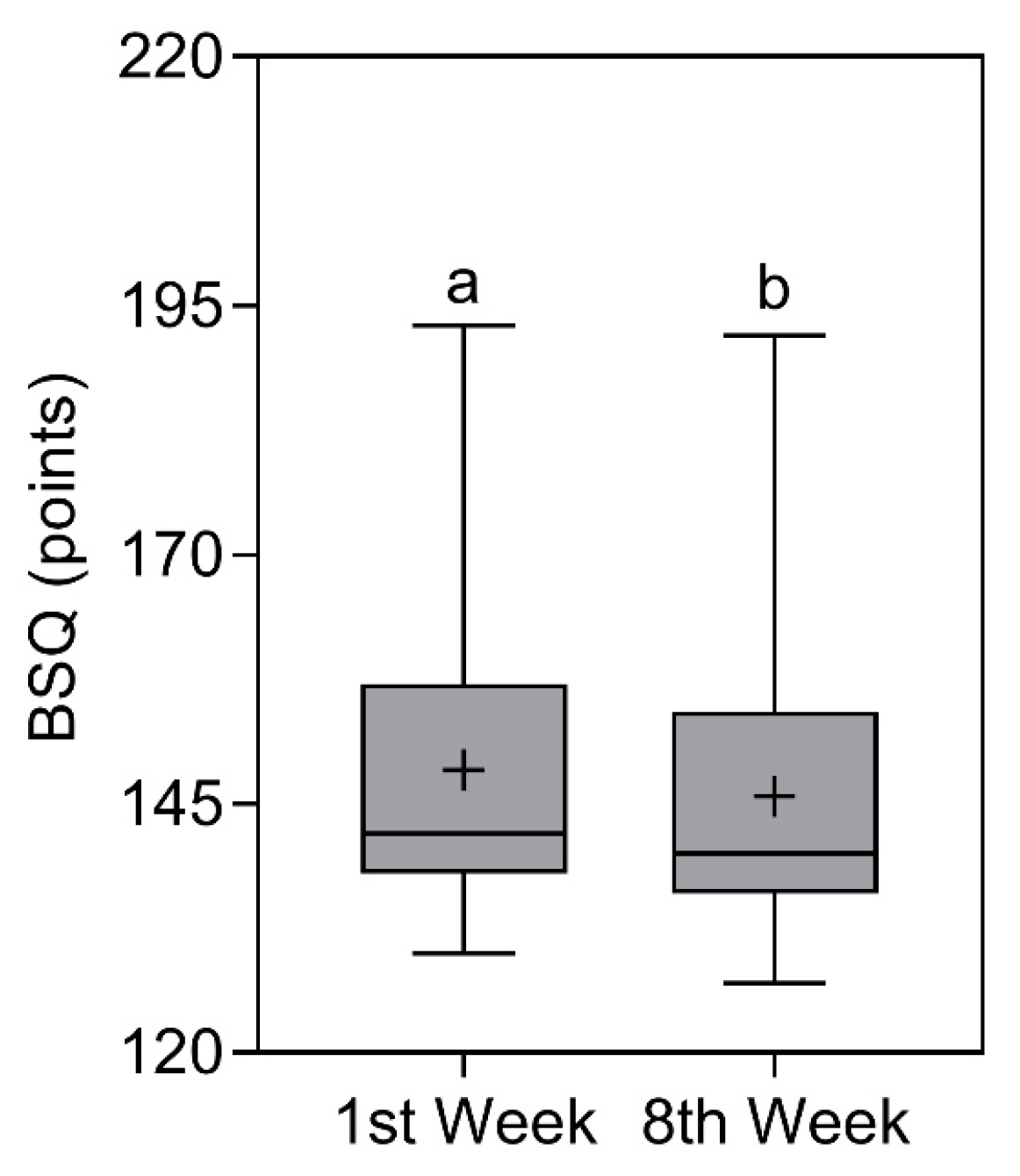
3.5. Body Shape Questionnaire (BSQ)
3.6. Binge Eating Scale (BES)
3.7. Binge Eating Episodes
3.8. Quality of Life Scale—WHOQOL-BREF
3.9. Additional Results for Qualitative and Quantitative Dietary Habits
3.10. Follow-Up (By Telephone)
4. Discussion
4.1. Follow-Up
4.2. Advantages, Strengths, and Perspectives
4.3. Limitations
5. Conclusions
6. Highlights—Take-Home Message
- There is still little evidence of the practice of mindful eating (ME) for the improvement of anthropometric data (weight, BMI, and waist circumference) in patients with obesity and binge eating disorder (BED);
- This study provides an update on the development of nutritional interventions that incorporate the practice of ME to optimize the complex treatment of this public health concern;
- This research study combined nutrition with psychology to understand what happens on the physiological and emotional planes in patients who have obesity and BED;
- It is possible to promote nutritional interventions that include qualitative subjective nutritional management without necessarily being a standard dietary prescription and that also present good results;
- ME should not be seen as a miracle treatment, but rather a strategy to complement nutritional management;
- Obesity and BED are a complex interaction of different factors for different people in different countries and cultures. They do not have a specific color, address, or socioeconomic status. They can affect anyone and deserve the attention of all health systems in the world. One universal strategy for every person is never going to be the solution.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arlington, V.A. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Giel, K.E.; Bulik, C.M.; Fernandez-Aranda, F.; Hay, P.; Keski-Rahkonen, A.; Schag, K.; Schmidt, U.; Zipfel, S. Binge eating disorder. Nat. Rev. Dis. Prim. 2022, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Pacanowski, C.R.; Mason, T.B.; Crosby, R.D.; Mitchell, J.E.; Crow, S.J.; Wonderlich, S.A.; Peterson, C.B. Weight Change over the Course of Binge Eating Disorder Treatment: Relationship to Binge Episodes and Psychological Factors. Obesity 2018, 26, 838–844. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 2024, 403, 1027–1050. [Google Scholar] [CrossRef] [PubMed]
- Morillo-Sarto, H.; López-Del-Hoyo, Y.; Pérez-Aranda, A.; Modrego-Alarcón, M.; Barceló-Soler, A.; Borao, L.; Puebla-Guedea, M.; Demarzo, M.; García-Campayo, J.; Montero-Marin, J. ‘Mindful eating’ for reducing emotional eating in patients with overweight or obesity in primary care settings: A randomized controlled trial. Eur. Eat. Disord. Rev. 2022, 31, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.D.; Ivezaj, V.; Pittman, B.P.; Grilo, C.M. Early weight loss predicts weight loss treatment response regardless of binge-eating disorder status and pretreatment weight change. Int. J. Eat. Disord. 2018, 51, 558–564. [Google Scholar] [CrossRef]
- Smith, J.; Ang, X.Q.; Giles, E.L.; Traviss-Turner, G. Emotional Eating Interventions for Adults Living with Overweight or Obesity: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 2722. [Google Scholar] [CrossRef]
- Smith, K.E.; Goldschmidt, A.B. Treatment of Binge-Eating Disorder Across the Lifespan: An Updated Review of the Literature and Considerations for Future Research. Curr. Obes. Rep. 2024. [Google Scholar] [CrossRef]
- Blanchet, C.; Mathieu, M.; St-Laurent, A.; Fecteau, S.; St-Amour, N.; Drapeau, V. A Systematic Review of Physical Activity Interventions in Individuals with Binge Eating Disorders. Curr. Obes. Rep. 2018, 7, 76–88. [Google Scholar] [CrossRef]
- Palavras, M.A.; Hay, P.; Filho, C.A.d.S.; Claudino, A. The Efficacy of Psychological Therapies in Reducing Weight and Binge Eating in People with Bulimia Nervosa and Binge Eating Disorder Who Are Overweight or Obese—A Critical Synthesis and Meta-Analyses. Nutrients 2017, 9, 299. [Google Scholar] [CrossRef]
- Tronieri, J.S.; Wadden, T.A.; Pearl, R.L.; Berkowitz, R.I.; Alamuddin, N.; Chao, A.M. Mindful Eating, General Mindful Awareness, and Acceptance as Predictors of Weight Loss. Mindfulness 2020, 11, 2818–2827. [Google Scholar] [CrossRef]
- Kristeller, J.L.; Jordan, K.D. Mindful Eating: Connecting with the Wise Self, the Spiritual Self. Front. Psychol. 2018, 9, 1271. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C.; Pinto-Gouveia, J.; Stubbs, R.J. Compassionate Attention and Regulation of Eating Behaviour: A pilot study of a brief low-intensity intervention for binge eating. Clin. Psychol. Psychother. 2017, 24, O1437–O1447. [Google Scholar] [CrossRef] [PubMed]
- Minari, T.P.; Tácito, L.H.B.; Yugar, L.B.T.; Ferreira-Melo, S.E.; Manzano, C.F.; Pires, A.C.; Moreno, H.; Vilela-Martin, J.F.; Cosenso-Martin, L.N.; Yugar-Toledo, J.C. Nutritional Strategies for the Management of Type 2 Diabetes Mellitus: A Narrative Review. Nutrients 2023, 15, 5096. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, G.A.; da Fonseca, P.N. Binge Eating at the Reception of Health Professionals; São Paulo Psychiatric Hospital: São Paulo, Brazil, 2006; Volume 4, pp. 1–18. [Google Scholar]
- Alvarenga, M.S.; Dunker, K.L.L.; Roman, E.C.B.; Philippi, S.T. Nutritional therapy for eating disorders. In Eating Disorders: A Nutritional View; Philippi, S.T., Alvarenga, M., Eds.; Manole: Barueri, Brazil, 2004; pp. 26–229. [Google Scholar]
- Costa, M.B.; Melnik, T. Effectiveness of psychosocial interventions in eating disorders: An overview of Cochrane systematic reviews. Einstein 2016, 14, 235–277. [Google Scholar] [CrossRef]
- Philippi, S.T.; Alvarenga, M.S.; Scagliusi, F.B. Nutrition and Eating Disorders: Evaluation and Treatment; Manole: Barueri, Brazil, 2010; p. 521. [Google Scholar]
- Black, M. Mindful Eating for Weight Loss: Try Before You Buy. J. Clin. Endocrinol. Metab. 2018, 104, 864–866. [Google Scholar] [CrossRef]
- Tapper, K. Mindful eating: What we know so far. Nutr. Bull. 2022, 47, 168–185. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Monteiro, C.A. Food Guide for the Brazilian Population [Internet]. 2014. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_para_a_pop_brasiliera_miolo_internet.pdf (accessed on 20 October 2023).
- Junqueira, S.A.E. Socio-Demographic and Clinical Profile of Psychiatric Patients Treated at Hospital Dia. Master’s Thesis, University of São Paulo), São Paulo, SP, Brazil, 2009. [Google Scholar]
- Development of the World Health Organization. WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. 1998, 28, 551–558. Available online: http://www.who.int/mental_health/media/en/76.pdf (accessed on 20 October 2023). [CrossRef] [PubMed]
- Fleck, M.P.; Louzada, S.; Xavier, M.; Chachamovich, E.; Vieira, G.; Santos, L.; Pinzon, V. Application of the Portuguese version of the abbreviated quality of life assessment instrument “WHOQOL-bref” [Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref]. Rev. Saude Publica 2000, 34, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Taylor, M.J.; Cooper, Z.; Fairbum, C.G. The development and validation of the body shape questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Di Pietro, M.C. Internal Validity, Dimensionality and Performance of the BSQ Scale—Body Shape Questionnaire—in a Population of University Students. Master’s Thesis, Federal University of São Paulo, São Paulo, Brazil, 2001. [Google Scholar] [CrossRef]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Freitas, S.; Lopes, C.S.; Coutinho, W.; Appolinario, J.C. Translation and adaptation of the Binge Eating Scale into Portuguese. Rev. Bras. Psiquiatr. 2001, 23, 215–220. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; Ridder, H. International Standards for Anthropometric Assessment; ISAK: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Word Health Organization. Obesity: Preventing and Managing the Global Epidemic; Reporf of WHO Consultation on Obesity; WHO Technical Report Series; Word Health Organization: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar]
- Brazilian Institute of Geography and Statistics. Family Budget Survey 2022–2023: Expenses, Income and Living Conditions; IBGE: Rio de Janeiro, Brazil, 2023. Available online: https://www.ibge.gov.br/pt/inicio.html (accessed on 4 January 2024).
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality. Biometrika 1965, 52, 591–599. [Google Scholar] [CrossRef]
- GraphPad. Prism Version 9.0 for Windows; GraphPad Software: La Jolla, CA, USA, 2019. [Google Scholar]
- Artiles, R.F.; Staub, K.; Aldakak, L.; Eppenberger, P.; Rühli, F.; Bender, N. Mindful eating and common diet programs lower body weight similarly: Systematic review and meta-analysis. Obes. Rev. 2019, 20, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Bennett, B.L.; Latner, J.D. Mindful eating, intuitive eating, and the loss of control over eating. Eat. Behav. 2022, 47, 101680. [Google Scholar] [CrossRef] [PubMed]
- Pepe, R.B.; Coelho, G.S.d.M.A.; Miguel, F.d.S.; Gualassi, A.C.; Sarvas, M.M.; Cercato, C.; Mancini, M.C.; de Melo, M.E. Mindful eating for weight loss in women with obesity: A randomised controlled trial. Br. J. Nutr. 2023, 130, 911–920. [Google Scholar] [CrossRef]
- Assari, S. Perceived Discrimination and Binge Eating Disorder; Gender Difference in African Americans. J. Clin. Med. 2018, 7, 89. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, F.; Rosa, B.; Faria, M. Frontal Lobe Functions and Quality of Life in Individuals with Obesity with and without Binge Eating Disorder. Endocrines 2023, 4, 696–708. [Google Scholar] [CrossRef]
- Ágh, T.; Kovács, G.; Supina, D.; Pawaskar, M.; Herman, B.K.; Vokó, Z.; Sheehan, D.V. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat. Weight Disord. 2016, 21, 353–364. [Google Scholar] [CrossRef]
- de Moraes, C.E.F.; Hay, P.; Sichieri, R.; Fazzino, T.L.; Mourilhe, C.; Appolinario, J.C. Hyperpalatable Foods Consumption in a Representative Sample of the General Population in Brazil: Differences of Binge and Non-Binge Eating Meals. Behav. Sci. 2023, 13, 149. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Individual Weekly Meetings | Goals | Procedures |
|---|---|---|
| 1st meeting: interview, evaluation, and data collection | (1) Get to know and approach the patients. (2) Evaluate clinical and sociodemographic data, level of quality of life, risk of BED, and dissatisfaction with body image at the 1st meeting. (3) Teach and apply ME techniques using favorite food dynamics. | (1) Informal introductory chat to get to know the patients and learn about all the points and dynamics that will be developed in the intervention. (2) Application of protocols: “Clinical and Sociodemographic Protocol” [24]; “Quality of Life Scale WHOQOL-BREF” [25,26]; “Body Shape Questionnaire (BSQ)” [27,28]; “Binge Eating Scale (BES)” [29,30]. (3) Learn and develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 2nd meeting: nutritional intervention | (1) Provide feedback on questionnaire results to participants. (2) Develop a “food diary” to increase food awareness and encourage autonomy in food intake. (3) Make a qualitative individual healthy eating plan, without prescribing calories, carbohydrates, proteins, fiber, and fats. (4) Apply ME techniques using favorite food dynamics. | (1) Discussion of the questionnaires, aiming to clarify the diagnosis, results, scores obtained, and possible treatments for obesity and BED. (2) Patients were encouraged to write down all the foods they ate, quantities, times, and other information. (3) Encouragement to eat more natural, minimally processed food; eat fewer ultra-processed foods; drink more water. (4) Develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 3rd meeting: nutritional intervention | (1) Explanation of the history, theory, practice, and studies involving ME. (2) Apply ME techniques using favorite food dynamics. | (1) Informative chat with patients, seeking to teach and understand what patients knew about the technique. (2) Develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 4th meeting: nutritional intervention | (1) Clarify the myths and truths on healthy eating. (2) Apply ME techniques using favorite food dynamics. | (1) Clarification of food myths and truths published in the media: carbohydrates are not the villain; gluten and lactose do not need to be excluded from your diet; you do not need to starve to lose weight; intermittent fasting is not the best nutritional strategy; eating carbohydrates at night does not make you gain weight; and others. (2) Develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 5th meeting: nutritional intervention | (1) Encourage participants’ culinary habits through culinary workshops and food tasting. The recipes were developed in the clinic’s kitchen. (2) Apply ME techniques using favorite food dynamics. | (1) Activity in the kitchen and active participation in cooking traditional Brazilian recipes: salads; basic dishes (rice, beans, protein sources, and whole grains); typical dishes (“feijoada”, fish “moqueca”, shrimp “bobo”, and “galinhada”); refreshing juices; fruit-flavored water. (2) Develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 6th meeting: nutritional intervention | (1) Evaluate the relationship of patients with food through blindfolded sensory analysis. (2) Apply ME techniques using favorite food dynamics. | (1) The participants’ eyes were blindfolded and they were presented with some foods (fruits, vegetables, spices, and herbs). Patients could only use touch, smell, and taste to elucidate them. (2) Develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 7th meeting: nutritional intervention | (1) Talk about eating disorders and eating behavior. Apply measures to channel some symptoms caused by BED. (2) Apply ME techniques using favorite food dynamics. | (1) Discover patients’ opinions about the symptoms of eating disorders in social situations. (2) Develop the habit of enjoying food; identify signs of hunger and satiety; develop the act of paying attention to food; eat calmly and without rushing; control breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| 8th meeting: final evaluation and data collection | (1) Discuss and complete interventions through mindfulness and ME videos. (2) Evaluate clinical and sociodemographic data, quality of life, risk of BED, and dissatisfaction with body image at the 8th meeting. (3) Apply ME techniques using favorite food dynamics. | (1) Patient feedback on nutritional interventions and completion of activities with audiovisual dynamics. (2) Reapplication of protocols: “Clinical and Sociodemographic Protocol” [24]; “Quality of Life Scale WHOQOL-BREF” [25,26]; “Body Shape Questionnaire (BSQ)” [27,28]; “Binge Eating Scale (BES)” [29,30]. (3) Develop the habit of enjoying food; Identify signs of hunger and satiety; Develop the act of paying attention to your food; Eat calmly and without rushing; Control your breathing to reduce anxiety before eating. All techniques were applied while patients ate their favorite foods that they brought to the meeting. |
| Variables | Total Sample Size (n = 82) | Total of the Individuals (%) |
|---|---|---|
| Sex | ||
| Female | n = 47 | 57.3% |
| Male | n = 35 | 42.7% |
| Economic Class | ||
| A | n = 9 | 11.0% |
| B | n = 23 | 28.0% |
| C | n = 33 | 40.2% |
| D | n = 8 | 9.8% |
| E | n = 9 | 11.0% |
| Race | ||
| White | n = 16 | 19.5% |
| Black | n = 18 | 22.0% |
| Brown | n = 14 | 17.1% |
| Indigenous | n = 12 | 14.6% |
| Yellow | n = 22 | 26.8% |
| Age | ||
| From 37 years to 56 years | n = 82 | N/A |
| Md ± IQR = 48.5 (51–43) | ||
| ± SD = 47.5 ± 4.8 |
| Variables | 1st Week | 8th Week | p |
|---|---|---|---|
| TEV (Kcal) (median ± IQR) | 2552 (2555–2550) * [ ± SD = 2552 ± 2.5] | 2202 (2204–2201) * [ ± SD = 2203 ± 2.4] | <0.0001 |
| Water Intake (L) (median ± IQR) | 1.5 (1.6–1.5) * [ ± SD = 1.5 ± 0.2] | 3.1 (3.5–3.1) * [ ± SD = 3.2± 0.2] | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minari, T.P.; Araújo-Filho, G.M.d.; Tácito, L.H.B.; Yugar, L.B.T.; Rubio, T.d.A.; Pires, A.C.; Vilela-Martin, J.F.; Cosenso-Martin, L.N.; Fattori, A.; Yugar-Toledo, J.C.; et al. Effects of Mindful Eating in Patients with Obesity and Binge Eating Disorder. Nutrients 2024, 16, 884. https://doi.org/10.3390/nu16060884
Minari TP, Araújo-Filho GMd, Tácito LHB, Yugar LBT, Rubio TdA, Pires AC, Vilela-Martin JF, Cosenso-Martin LN, Fattori A, Yugar-Toledo JC, et al. Effects of Mindful Eating in Patients with Obesity and Binge Eating Disorder. Nutrients. 2024; 16(6):884. https://doi.org/10.3390/nu16060884
Chicago/Turabian StyleMinari, Tatiana Palotta, Gerardo Maria de Araújo-Filho, Lúcia Helena Bonalume Tácito, Louise Buonalumi Tácito Yugar, Tatiane de Azevedo Rubio, Antônio Carlos Pires, José Fernando Vilela-Martin, Luciana Neves Cosenso-Martin, André Fattori, Juan Carlos Yugar-Toledo, and et al. 2024. "Effects of Mindful Eating in Patients with Obesity and Binge Eating Disorder" Nutrients 16, no. 6: 884. https://doi.org/10.3390/nu16060884