
Gastrointestinal Microbiota & Symptoms of Depression and Anxiety in Anorexia Nervosa—A Re-Analysis of the MICROBIAN Longitudinal Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Registrations of the Study
2.2. Design and Population
2.3. Microbiota and SCFA Analysis
2.4. Psychological Parameters
2.5. Dietary Intake
2.6. Statistics
3. Results
3.1. Characteristics
3.2. Alpha Diversity
3.3. Beta Diversity
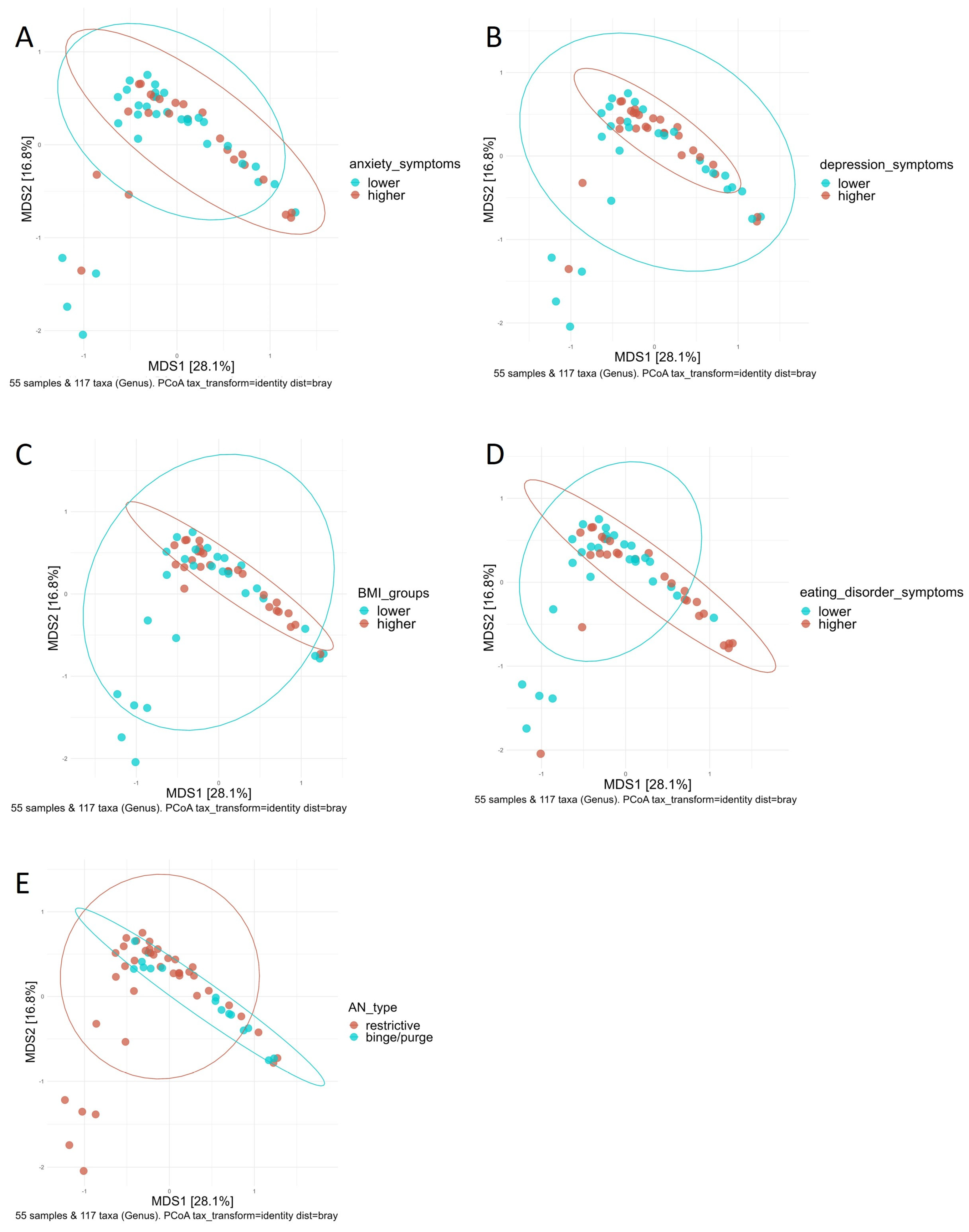
3.4. Principal Coordinate Analysis and Distance-Based Redundancy Analysis
3.5. Microbial Composition
3.5.1. Relationships between the Abundances of Taxa with Symptom Severity of Depression, Anxiety, and Eating Disorders before Adjusting for the BMI
3.5.2. Relationships between Abundances of Taxa with Symptom Severity of Depression, Anxiety and Eating Disorder Adjusted for the BMI
3.6. Relationship between SCFAs and Symptom Severity of Depression, Anxiety and Eating Disorder
3.6.1. Relationships between the SCFAs with Symptom Severity of Depression, Anxiety, and Eating Disorder before Adjusting for the BMI
3.6.2. Relationships between the SCFAs with Symptom Severity of Depression, Anxiety and Eating Disorder after Adjusting for the BMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ICD-11 for Mortality and Morbidity Statistics. Available online: https://icd.who.int/browse11/l-m/en (accessed on 19 November 2023).
- Dejong, H.; Broadbent, H.; Schmidt, U. A Systematic Review of Dropout from Treatment in Outpatients with Anorexia Nervosa. Int. J. Eat. Disord. 2012, 45, 635–647. [Google Scholar] [CrossRef] [PubMed]
- Mehler, P.S.; Brown, C. Anorexia Nervosa—Medical Complications. J. Eat. Disord. 2015, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, S.; Löwe, B.; Reas, D.L.; Deter, H.C.; Herzog, W. Long-Term Prognosis in Anorexia Nervosa: Lessons from a 21-Year Follow-up Study. Lancet 2000, 355, 721–722. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia Nervosa: Aetiology, Assessment, and Treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Fudge, J.L.; Paulus, M. New Insights into Symptoms and Neurocircuit Function of Anorexia Nervosa. Nat. Rev. Neurosci. 2009, 10, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Quaglio, A.E.V.; Grillo, T.G.; De Oliveira, E.C.S.; Di Stasi, L.C.; Sassaki, L.Y. Gut Microbiota, Inflammatory Bowel Disease and Colorectal Cancer. World J. Gastroenterol. 2022, 28, 4053–4060. [Google Scholar] [CrossRef] [PubMed]
- Moniaga, C.S.; Tominaga, M.; Takamori, K. An Altered Skin and Gut Microbiota Are Involved in the Modulation of Itch in Atopic Dermatitis. Cells 2022, 11, 3930. [Google Scholar] [CrossRef]
- Scheithauer, T.P.M.; Rampanelli, E.; Nieuwdorp, M.; Vallance, B.A.; Verchere, C.B.; van Raalte, D.H.; Herrema, H. Gut Microbiota as a Trigger for Metabolic Inflammation in Obesity and Type 2 Diabetes. Front. Immunol. 2020, 11, 571731. [Google Scholar] [CrossRef]
- Festi, D.; Schiumerini, R.; Eusebi, L.H.; Marasco, G.; Taddia, M.; Colecchia, A. Gut Microbiota and Metabolic Syndrome. World J. Gastroenterol. 2014, 20, 16079–16094. [Google Scholar] [CrossRef]
- Di Lodovico, L.; Mondot, S.; Doré, J.; Mack, I.; Hanachi, M.; Gorwood, P. Anorexia Nervosa and Gut Microbiota: A Systematic Review and Quantitative Synthesis of Pooled Microbiological Data. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 106, 110114. [Google Scholar] [CrossRef]
- Garcia, N.; Gutierrez, E. Anorexia Nervosa and Microbiota: Systematic Review and Critical Appraisal. Eat. Weight Disord. 2023, 28, 1. [Google Scholar] [CrossRef] [PubMed]
- Carbone, E.A.; D’Amato, P.; Vicchio, G.; De Fazio, P.; Segura-Garcia, C. A Systematic Review on the Role of Microbiota in the Pathogenesis and Treatment of Eating Disorders. Eur. Psychiatry 2020, 64, e2. [Google Scholar] [CrossRef] [PubMed]
- Mack, I.; Penders, J.; Cook, J.; Dugmore, J.; Mazurak, N.; Enck, P. Is the Impact of Starvation on the Gut Microbiota Specific or Unspecific to Anorexia Nervosa? A Narrative Review Based on a Systematic Literature Search. Curr. Neuropharmacol. 2018, 16, 1131–1149. [Google Scholar] [CrossRef]
- Glenny, E.M.; Fouladi, F.; Thomas, S.A.; Bulik-Sullivan, E.C.; Tang, Q.; Djukic, Z.; Trillo-Ordonez, Y.S.; A Fodor, A.; Tarantino, L.M.; M Bulik, C.; et al. Gut Microbial Communities from Patients with Anorexia Nervosa Do Not Influence Body Weight in Recipient Germ-Free Mice. Gut Microbes 2021, 13, 1897216. [Google Scholar] [CrossRef]
- Fan, Y.; Støving, R.K.; Berreira Ibraim, S.; Hyötyläinen, T.; Thirion, F.; Arora, T.; Lyu, L.; Stankevic, E.; Hansen, T.H.; Déchelotte, P.; et al. The Gut Microbiota Contributes to the Pathogenesis of Anorexia Nervosa in Humans and Mice. Nat. Microbiol. 2023, 8, 787–802. [Google Scholar] [CrossRef] [PubMed]
- Margolis, K.G.; Cryan, J.F.; Mayer, E.A. The Microbiota-Gut-Brain Axis: From Motility to Mood. Gastroenterology 2021, 160, 1486–1501. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Bouzari, B.; Hosseini-Fard, S.R.; Mazaheri, M.; Ahmadyousefi, Y.; Abdi, M.; Jalalifar, S.; Karimitabar, Z.; Teimoori, A.; Keyvani, H.; et al. Role of Microbiota-Derived Short-Chain Fatty Acids in Nervous System Disorders. Biomed. Pharmacother. 2021, 139, 111661. [Google Scholar] [CrossRef]
- Simpson, C.A.; Diaz-Arteche, C.; Eliby, D.; Schwartz, O.S.; Simmons, J.G.; Cowan, C.S.M. The Gut Microbiota in Anxiety and Depression—A Systematic Review. Clin. Psychol. Rev. 2021, 83, 101943. [Google Scholar] [CrossRef]
- Zhu, S.; Jiang, Y.; Xu, K.; Cui, M.; Ye, W.; Zhao, G.; Jin, L.; Chen, X. The Progress of Gut Microbiome Research Related to Brain Disorders. J. Neuroinflam. 2020, 17, 25. [Google Scholar] [CrossRef]
- Kleiman, S.C.; Watson, H.J.; Bulik-Sullivan, E.C.; Huh, E.Y.; Tarantino, L.M.; Bulik, C.M.; Carroll, I.M. The Intestinal Microbiota in Acute Anorexia Nervosa and during Renourishment: Relationship to Depression, Anxiety, and Eating Disorder Psychopathology. Psychosom. Med. 2015, 77, 969–981. [Google Scholar] [CrossRef]
- Schulz, N.; Belheouane, M.; Dahmen, B.; Ruan, V.A.; Specht, H.E.; Dempfle, A.; Herpertz-Dahlmann, B.; Baines, J.F.; Seitz, J. Gut Microbiota Alteration in Adolescent Anorexia Nervosa Does Not Normalize with Short-Term Weight Restoration. Int. J. Eat. Disord. 2021, 54, 969–980. [Google Scholar] [CrossRef] [PubMed]
- Borgo, F.; Riva, A.; Benetti, A.; Casiraghi, M.C.; Bertelli, S.; Garbossa, S.; Anselmetti, S.; Scarone, S.; Pontiroli, A.E.; Morace, G.; et al. Microbiota in Anorexia Nervosa: The Triangle between Bacterial Species, Metabolites and Psychological Tests. PLoS ONE 2017, 12, e0179739. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Cassioli, E.; Vitali, F.; Rossi, E.; Dani, C.; Melani, G.; Flaccomio, D.; D’Andria, M.; Mejia Monroy, M.; Galli, A.; et al. Gut Microbiota Metabolites Mediate the Interplay between Childhood Maltreatment and Psychopathology in Patients with Eating Disorders. Sci. Rep. 2023, 13, 11753. [Google Scholar] [CrossRef] [PubMed]
- de Wit, L.M.; van Straten, A.; van Herten, M.; Penninx, B.W.; Cuijpers, P. Depression and Body Mass Index, a u-Shaped Association. BMC Public Health 2009, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Li, X.; Li, Y.; Niu, X. The Nonlinear Relationship Between Body Mass Index (BMI) and Perceived Depression in the Chinese Population. Psychol. Res. Behav. Manag. 2023, 16, 2103–2124. [Google Scholar] [CrossRef] [PubMed]
- Mack, I.; Cuntz, U.; Grämer, C.; Niedermaier, S.; Pohl, C.; Schwiertz, A.; Zimmermann, K.; Zipfel, S.; Enck, P.; Penders, J. Weight Gain in Anorexia Nervosa Does Not Ameliorate the Faecal Microbiota, Branched Chain Fatty Acid Profiles and Gastrointestinal Complaints. Sci. Rep. 2016, 6, 26752. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Psychosomatische Medizin und Psychotherapie (DGPM): 13. Kongress der Deutschen Gesellschaft für Psychosomatische Medizin und Psychotherapie Somatoforme Störungen—Multimethodale Behandlung. Z. Psychosom. Med. Psychother. 2005, 51, 325. [Google Scholar] [CrossRef]
- Segal, D.L. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2010; pp. 1–3. ISBN 978-0-470-47921-6. [Google Scholar]
- DIMDI—ICD-10-GM Version 2011. Available online: https://www.dimdi.de/static/de/klassifikationen/icd/icd-10-gm/kode-suche/htmlgm2011/block-f50-f59.htm (accessed on 22 August 2023).
- Caporaso, J.G.; Lauber, C.L.; Walters, W.A.; Berg-Lyons, D.; Huntley, J.; Fierer, N.; Owens, S.M.; Betley, J.; Fraser, L.; Bauer, M.; et al. Ultra-High-Throughput Microbial Community Analysis on the Illumina HiSeq and MiSeq Platforms. ISME J. 2012, 6, 1621–1624. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-Resolution Sample Inference from Illumina Amplicon Data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing, Version 4.1.0; R Core Team: Vienna, Austria, 2020.
- Allaire, J.; Yihui, X.; McPherson, J.; Luraschi, J.; Ushey, K.; Atkins, A.; Wickham, H.; Cheng, J.; Chang, W.; Iannone, R. Rmarkdown: Dynamic Documents for R; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar]
- Xie, Y.; Allaire, J.J.; Grolemund, G. R Markdown: The Definitive Guide; Routledge: Boca Raton, FL, USA, 2018; ISBN 978-1-138-35933-8. [Google Scholar]
- Xie, Y.; Dervieux, C.; Riederer, E. R Markdown Cookbook; Chapman & Hall/CRC: Boca Raton, FL, USA, 2020. [Google Scholar]
- Callahan, B.J.; Sankaran, K.; Fukuyama, J.A.; McMurdie, P.J.; Holmes, S.P. Bioconductor Workflow for Microbiome Data Analysis: From Raw Reads to Community Analyses. F1000 Res. 2016, 5, 1492. [Google Scholar] [CrossRef]
- Pau, G.; Barr, C.; Reeder, J.; Lawrence, M.; Degenhardt, J.; Wu, T.; Huntley, M.; Brauer, M. HTSeqGenie: A Software Package to Analyse High-Throughput Sequencing Experiments. Available online: https://rdrr.io/bioc/HTSeqGenie/ (accessed on 9 September 2021).
- Pagès, H.; Aboyoun, P.; Gentleman, R.; DebRoy, S. Biostrings: Efficient Manipulation of Biological Strings; R Package, Version 2.46.0. Available online: https://bioconductor.org/packages/Biostrings(accessed on 9 September 2021).
- McLaren, M.R. Silva SSU Taxonomic Training Data Formatted for DADA2, Silva; Version 138; Zenodo: Raleigh, NC, USA, 2020. [Google Scholar] [CrossRef]
- Davis, N.M.; Proctor, D.M.; Holmes, S.P.; Relman, D.A.; Callahan, B.J. Simple Statistical Identification and Removal of Contaminant Sequences in Marker-Gene and Metagenomics Data. Microbiome 2018, 6, 226. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Schliep, K.P. Phangorn: Phylogenetic Analysis in R. Bioinformatics 2011, 27, 592–593. [Google Scholar] [CrossRef] [PubMed]
- McMurdie, P.J.; Holmes, S. Phyloseq: An R Package for Reproducible Interactive Analysis and Graphics of Microbiome Census Data. PLoS ONE 2013, 8, e61217. [Google Scholar] [CrossRef] [PubMed]
- Phyloseq Taxa Filter. Available online: https://giangle.shinyapps.io/phyloFilter/ (accessed on 4 August 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; Version 4.2.3; R Core Team: Vienna, Austria, 2023. [Google Scholar]
- Lahti, L.; Shetty, S. Tools for Microbiome Analysis in R. Available online: http://microbiome.github.com/microbiome (accessed on 4 August 2023).
- Oksanen, J.; Simpson, G.L.; Blanchet, F.G.; Kindt, R.; Legendre, P.; Minchin, P.R.; O’Hara, R.B.; Solymos, P.; Stevens, M.H.H.; Szoecs, E.; et al. Vegan: Community Ecology Package. Available online: https://cran.r-project.org/web/packages/vegan/index.html (accessed on 4 August 2023).
- Barnett, D.; Arts, I.; Penders, J. microViz: An R Package for Microbiome Data Visualization and Statistics. JOSS 2021, 6, 3201. [Google Scholar] [CrossRef]
- GraphPad Software Inc. GraphPad Software, Version 9.4.1; GraphPad Software Inc.: Boston, MA, USA, 2022.
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Thiel, A.; Jacobi, C.; Horstmann, S.; Paul, T.; Nutzinger, D.; Schüßler, G. A German Version of the Eating Disorder Inventory EDI-2. Psychother. Psychosom. Med. Psychol. 1970, 47, 365–376. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories -IA and -II in Psychiatric Outpatients. J. Pers Assess 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Franke, G.H. BSI—Brief Symptom Inventory: Deutsche Version, Manual; Beltz: Göttingen, Germany, 2000. [Google Scholar]
- Fichter, M.; Quadflieg, N. Das Strukturierte Interview für Anorektische und Bulimische Ess-Störungen nach DSM-IV und ICD-10 zur Expertenbeurteilung (SIAB-EX) und dazugehöriger Fragebogen zur Selbsteinschätzung (SIAB-S). Verhaltenstherapie 2001, 11, 314–325. [Google Scholar] [CrossRef]
- Toussaint, A.; Hüsing, P.; Gumz, A.; Wingenfeld, K.; Härter, M.; Schramm, E.; Löwe, B. Sensitivity to Change and Minimal Clinically Important Difference of the 7-Item Generalized Anxiety Disorder Questionnaire (GAD-7). J. Affect. Disord. 2020, 265, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Anderson, M.J. A New Method for Non-Parametric Multivariate Analysis of Variance. Austral Ecol. 2001, 26, 32–46. [Google Scholar] [CrossRef]
- Jackson, M.A.; Verdi, S.; Maxan, M.-E.; Shin, C.M.; Zierer, J.; Bowyer, R.C.E.; Martin, T.; Williams, F.M.K.; Menni, C.; Bell, J.T.; et al. Gut Microbiota Associations with Common Diseases and Prescription Medications in a Population-Based Cohort. Nat. Commun. 2018, 9, 2655. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Vasupanrajit, A.; Jirakran, K.; Klomkliew, P.; Chanchaem, P.; Tunvirachaisakul, C.; Payungporn, S. Exploration of the Gut Microbiome in Thai Patients with Major Depressive Disorder Shows a Specific Bacterial Profile with Depletion of the Ruminococcus Genus as a Putative Biomarker. Cells 2023, 12, 1240. [Google Scholar] [CrossRef] [PubMed]
- Rong, H.; Xie, X.; Zhao, J.; Lai, W.; Wang, M.; Xu, D.; Liu, Y.; Guo, Y.; Xu, S.; Deng, W.; et al. Similarly in Depression, Nuances of Gut Microbiota: Evidences from a Shotgun Metagenomics Sequencing Study on Major Depressive Disorder versus Bipolar Disorder with Current Major Depressive Episode Patients. J. Psychiatr. Res. 2019, 113, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.G.; Goldenthal, A.R.; Uhlemann, A.-C.; Mann, J.J.; Miller, J.M.; Sublette, M.E. Systematic Review of Gut Microbiota and Major Depression. Front. Psychiatry 2019, 10, 34. [Google Scholar] [CrossRef]
- Jiang, H.; Ling, Z.; Zhang, Y.; Mao, H.; Ma, Z.; Yin, Y.; Wang, W.; Tang, W.; Tan, Z.; Shi, J.; et al. Altered Fecal Microbiota Composition in Patients with Major Depressive Disorder. Brain Behav. Immun. 2015, 48, 186–194. [Google Scholar] [CrossRef]
- Zhu, J.; Li, M.; Shao, D.; Ma, S.; Wei, W. Altered Fecal Microbiota Signatures in Patients with Anxiety and Depression in the Gastrointestinal Cancer Screening: A Case-Control Study. Front. Psychiatry 2021, 12, 757139. [Google Scholar] [CrossRef]
- Zheng, P.; Zeng, B.; Zhou, C.; Liu, M.; Fang, Z.; Xu, X.; Zeng, L.; Chen, J.; Fan, S.; Du, X.; et al. Gut Microbiome Remodeling Induces Depressive-like Behaviors through a Pathway Mediated by the Host’s Metabolism. Mol. Psychiatry 2016, 21, 786–796. [Google Scholar] [CrossRef]
- Zhao, H.; Jin, K.; Jiang, C.; Pan, F.; Wu, J.; Luan, H.; Zhao, Z.; Chen, J.; Mou, T.; Wang, Z.; et al. A Pilot Exploration of Multi-Omics Research of Gut Microbiome in Major Depressive Disorders. Transl. Psychiatry 2022, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- La Reau, A.J.; Suen, G. The Ruminococci: Key Symbionts of the Gut Ecosystem. J. Microbiol. 2018, 56, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zheng, P.; Liu, Y.; Zhong, X.; Wang, H.; Guo, Y.; Xie, P. Sex Differences in Gut Microbiota in Patients with Major Depressive Disorder. Neuropsychiatr. Dis. Treat. 2018, 14, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.-C.E.; Chen, H.-C.; Chou, H.-C.L.; Chen, I.-M.; Lee, M.-S.; Chuang, L.-C.; Liu, Y.-W.; Lu, M.-L.; Chen, C.-H.; Wu, C.-S.; et al. Exploration of Microbiota Targets for Major Depressive Disorder and Mood Related Traits. J. Psychiatr. Res. 2019, 111, 74–82. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, L.; Wang, X.; Wang, Z.; Zhang, J.; Jiang, R.; Wang, X.; Wang, K.; Liu, Z.; Xia, Z.; et al. Similar Fecal Microbiota Signatures in Patients with Diarrhea-Predominant Irritable Bowel Syndrome and Patients with Depression. Clin. Gastroenterol. Hepatol. 2016, 14, 1602–1611.e5. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Shi, X.; Li, Z.; Shen, Y.; Shi, X.; Wang, L.; Li, G.; Yuan, Y.; Wang, J.; Zhang, Y.; et al. Possible Association of Firmicutes in the Gut Microbiota of Patients with Major Depressive Disorder. Neuropsychiatr. Dis. Treat. 2018, 14, 3329–3337. [Google Scholar] [CrossRef] [PubMed]
- Yuan, R.; Yang, L.; Yao, G.; Geng, S.; Ge, Q.; Bo, S.; Li, X. Features of Gut Microbiota in Patients with Anorexia Nervosa. Chin. Med. J. 2022, 135, 1993–2002. [Google Scholar] [CrossRef]
- Hao, C.; Gao, Z.; Liu, X.; Rong, Z.; Jia, J.; Kang, K.; Guo, W.; Li, J. Intravenous Administration of Sodium Propionate Induces Antidepressant or Prodepressant Effect in a Dose Dependent Manner. Sci. Rep. 2020, 10, 19917. [Google Scholar] [CrossRef]
- Li, J.; Hou, L.; Wang, C.; Jia, X.; Qin, X.; Wu, C. Short Term Intrarectal Administration of Sodium Propionate Induces Antidepressant-like Effects in Rats Exposed to Chronic Unpredictable Mild Stress. Front. Psychiatry 2018, 9, 454. [Google Scholar] [CrossRef]
- Burokas, A.; Arboleya, S.; Moloney, R.D.; Peterson, V.L.; Murphy, K.; Clarke, G.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Targeting the Microbiota-Gut-Brain Axis: Prebiotics Have Anxiolytic and Antidepressant-like Effects and Reverse the Impact of Chronic Stress in Mice. Biol. Psychiatry 2017, 82, 472–487. [Google Scholar] [CrossRef]
- Navarro-Tapia, E.; Almeida-Toledano, L.; Sebastiani, G.; Serra-Delgado, M.; García-Algar, Ó.; Andreu-Fernández, V. Effects of Microbiota Imbalance in Anxiety and Eating Disorders: Probiotics as Novel Therapeutic Approaches. Int. J. Mol. Sci. 2021, 22, 2351. [Google Scholar] [CrossRef]
- Le Morvan de Sequeira, C.; Hengstberger, C.; Enck, P.; Mack, I. Effect of Probiotics on Psychiatric Symptoms and Central Nervous System Functions in Human Health and Disease: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 621. [Google Scholar] [CrossRef]
- Ansari, F.; Neshat, M.; Pourjafar, H.; Jafari, S.M.; Samakkhah, S.A.; Mirzakhani, E. The Role of Probiotics and Prebiotics in Modulating of the Gut-Brain Axis. Front. Nutr. 2023, 10, 1173660. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T1 | T2 | |||
|---|---|---|---|---|
| Symptom Severity | Higher | Lower | Higher | Lower |
| Anxiety (GAD-7) | >11 | ≤11 | >5 | ≤5 |
| Depression (PHQ-9) | >14 | ≤14 | >5 | ≤5 |
| Eating disorder (EDI-II) | >82 | ≤82 | >31 | ≤31 |
| Improvement of Symptom Severity (∆T2 − T1) | Higher | Lower |
|---|---|---|
| Anxiety (GAD-7) | ≤−5 | >−5 |
| Depression (PHQ-9) | ≤−8 | >−8 |
| Eating disorder (EDI-II) | ≤−44 | >−44 |
| T1(n = 55) Mean (SD) (Min–Max) | T2 (n = 44) Mean (SD) (Min–Max) | p-Value | |
|---|---|---|---|
| Age | 23.8 (6.8) years (min–max: 14–39) | 23.1 (6.7) years (min–max: 14–39) | 0.944 |
| BMI | 15.4 (1.4) (min–max: 11.6–17.7) kg/m2 | 17.7 (1.4) (min–max: 13.9–21.8) kg/m2 | <0.001 |
| Anxiety symptoms (GAD-7) | 10.6 (4.7) (min–max: 2–21) | 5.4 (4.0) (min–max: 0–17) | <0.001 |
| Depression symptoms (PHQ-9) | 14.1 (5.5) (min–max: 0–25) | 5.6 (4.4) (min–max: 0–21) | <0.001 |
| Eating disorder symptoms (EDI-II) | 87.1 (38.6) (min–max: 20–194) | 42.0 (33.4) (min–max: 6–167) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ketel, J.; Bosch-Bruguera, M.; Auchter, G.; Cuntz, U.; Zipfel, S.; Enck, P.; Mack, I. Gastrointestinal Microbiota & Symptoms of Depression and Anxiety in Anorexia Nervosa—A Re-Analysis of the MICROBIAN Longitudinal Study. Nutrients 2024, 16, 891. https://doi.org/10.3390/nu16060891
Ketel J, Bosch-Bruguera M, Auchter G, Cuntz U, Zipfel S, Enck P, Mack I. Gastrointestinal Microbiota & Symptoms of Depression and Anxiety in Anorexia Nervosa—A Re-Analysis of the MICROBIAN Longitudinal Study. Nutrients. 2024; 16(6):891. https://doi.org/10.3390/nu16060891
Chicago/Turabian StyleKetel, Jasmin, Miquel Bosch-Bruguera, Greta Auchter, Ulrich Cuntz, Stephan Zipfel, Paul Enck, and Isabelle Mack. 2024. "Gastrointestinal Microbiota & Symptoms of Depression and Anxiety in Anorexia Nervosa—A Re-Analysis of the MICROBIAN Longitudinal Study" Nutrients 16, no. 6: 891. https://doi.org/10.3390/nu16060891