
The Possible Synergistic Pharmacological Effect of an Oral Berberine (BBR) and Curcumin (CUR) Complementary Therapy Alleviates Symptoms of Irritable Bowel Syndrome (IBS): Results from a Real-Life, Routine Clinical Practice Settings-Based Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Patients’ Inclusion Criteria
2.3. Variables
2.4. Study Outcome Measures
2.5. Berberine–Curcumin (BBR–CUR) Supplementation
2.6. Statistical Analysis
3. Results
3.1. Primary Outcome Measure
3.2. Secondary Outcome Measures
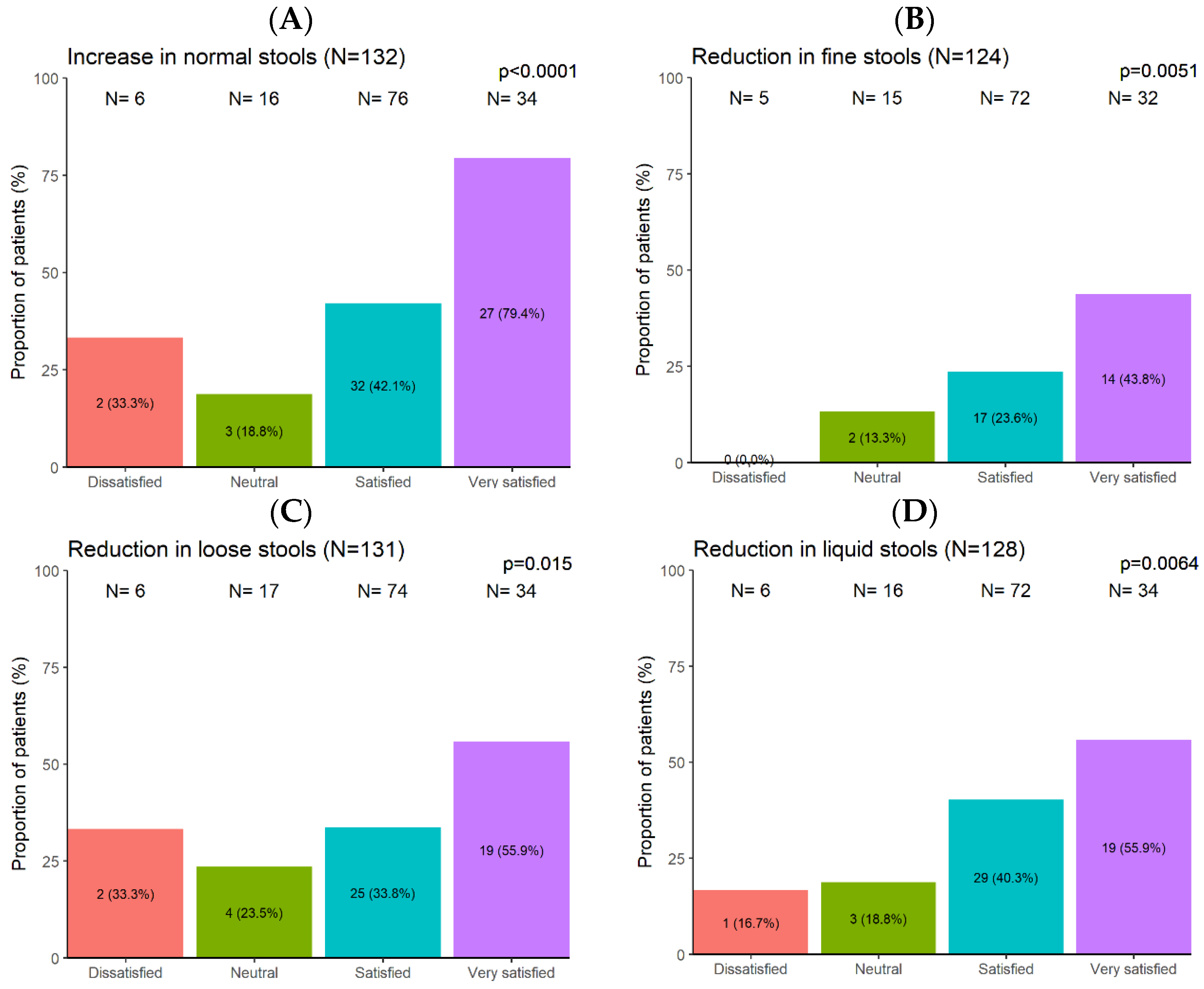
3.2.1. Supplementation Effect on Patients’ Stool Type (Status)
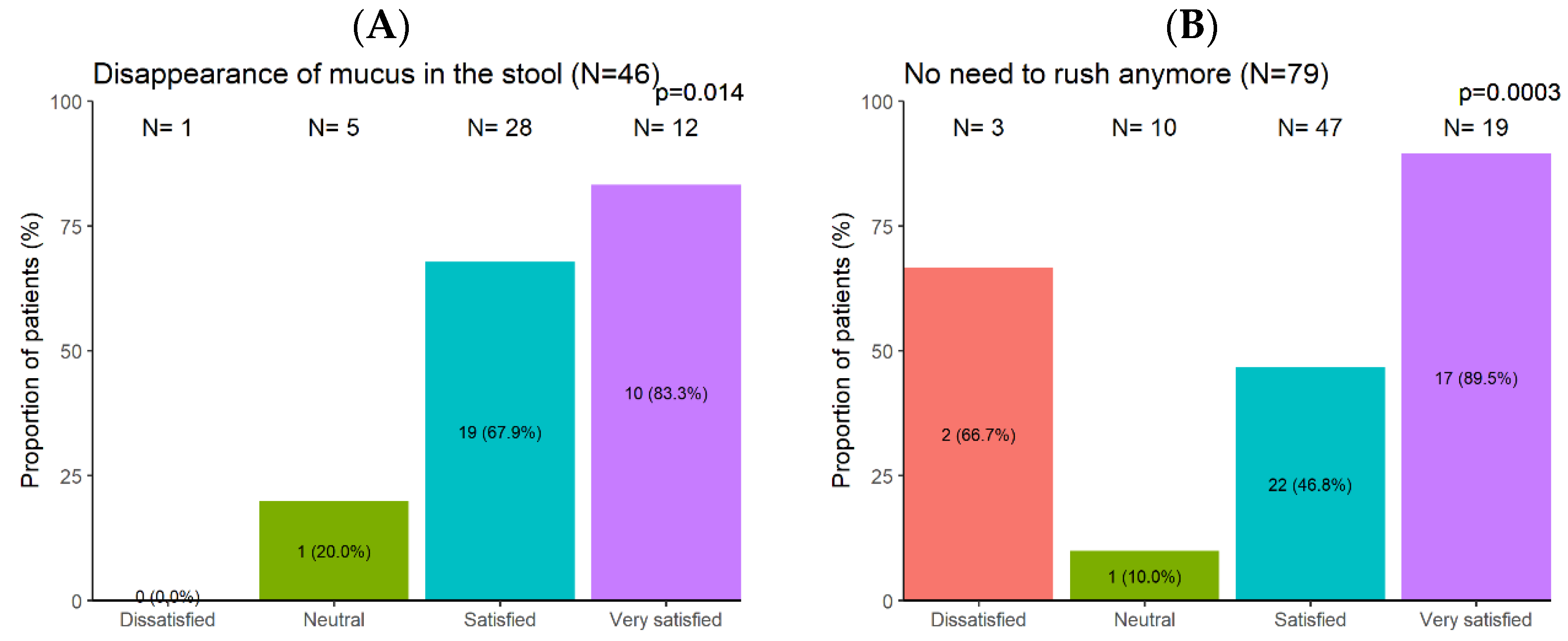
3.2.2. Supplementation Effect on Patients’ Stool Situation
3.2.3. Supplementation Effect on IBS Sub-Types
3.2.4. Supplementation Effect on Concomitant Conventional IBS Treatment
3.2.5. Supplementation Safety and Tolerability
3.2.6. Patients’ Satisfaction with Supplement Complementary Therapy
4. Discussion
- Berberine
- Anti-diarrhoeal effects: BBR has been shown to possess anti-diarrhoeal properties, which may be beneficial for IBS patients experiencing diarrhoea-dominated symptoms.
- Antimicrobial and antispasmodic effects: BBR exhibits broad-spectrum antimicrobial activity, including against pathogenic bacteria and parasites, which may help rebalance gut microbiota in IBS patients. It also exhibits antispasmodic effects, potentially reducing IBS-related abdominal pain.
- Regulation of gut motility: BBR has been reported to modulate gut motility, potentially alleviating symptoms of abdominal pain and discomfort associated with IBS.
- Choleretic effect: BBR may increase bile production and secretion, which may aid in the digestion of fats, and thus could alleviate some digestive symptoms commonly associated with IBS, such as bloating, gas, and discomfort. Bile acids have been shown to influence gut motility, and abnormalities in bile acid metabolism have been implicated in IBS. By promoting bile secretion, BBR may help regulate gut motility, potentially reducing symptoms like diarrhoea or constipation in individuals with IBS.
- Metabolic benefits: BBR has shown benefits in managing blood sugar levels and lipid profiles, which may indirectly impact IBS symptoms [86].
- While some clinical studies have investigated the efficacy of BBR in IBS, the overall evidence base is still limited compared to conventional treatments. BBR may cause GI side effects, such as nausea, vomiting, and abdominal discomfort, in some individuals. BBR may interact with certain medications, including those metabolised by the liver or affecting heart rhythm.
- Curcumin
- Anti-inflammatory properties: CUR has potent anti-inflammatory effects, which may help alleviate gut inflammation associated with IBS symptoms.
- Antioxidant properties: CUR exhibits antioxidant properties, which can help neutralise free radicals and reduce oxidative stress, potentially contributing to the improvement of IBS symptoms.
- Gut health support: CUR may promote gut health by modulating gut microbiota and improving intestinal barrier function.
- Cellular communication: CUR influences cellular communication pathways, potentially mitigating intestinal bleeding, ulcers, and irritation within the digestive tract.
- Psychological benefits: Some studies suggest CUR may reduce anxiety associated with IBS [46].
- Choleretic effect: CUR exhibits choleretic properties, stimulating bile production and secretion. This can aid in the digestion of fats, potentially alleviating symptoms such as bloating and discomfort in individuals with IBS.
- Low toxicity: CUR is generally considered safe and well-tolerated, even at high doses.
- Limitations associated with CUR include its poor bioavailability, and limited clinical evidence. While promising, clinical evidence supporting CUR’s efficacy in IBS remains limited. More robust clinical trials are needed.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Definition |
| AD | Alzheimer’s disease |
| BBR | Berberine |
| BSC | Bristol Stool Chart |
| BDNF | Brain-derived Neurotrophic Factor |
| CUR | Curcumin |
| CRF | Case Report Form |
| CI | Confidence Interval |
| COX-2 | Cyclooxygenase-2 |
| cAMP | Cyclic Adenosine Monophosphate |
| FODMAP | Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols |
| FDA | Food and Drug Administration |
| GI | Gastrointestinal |
| GP | General Practitioner |
| GCP | Good Clinical Practice |
| GRAS | Generally Recognized As Safe |
| 5-HT | 5-Hydroxytryptamine |
| IBS | Irritable Bowel Syndrome |
| IBSSI | Irritable Bowel Syndrome Severity Index |
| IRB | Institutional Review Board |
| INF-γ | Interferon-gamma |
| IL-7 | Interleukin-7 |
| iNOS | Inducible Nitric Oxide Synthase |
| IQR | Interquartile Range |
| 5-LOX | 5-Lipoxygenase |
| N | Numbers |
| NF-kB | Nuclear Factor-kappa B |
| NAFLD | Non-alcoholic Fatty Liver Disease |
| OR | Odd Ratio |
| pCREB | Phosphorylated cAMP Response Element-binding |
| QoL | Quality of life |
| RCT | Randomized Clinical Trial |
| SAS | Statistical Analysis System |
| SD | Standard Deviation |
| TrkB | Tropomyosin Receptor Kinase B |
| VAS | Visual Analogue Scale |
| ZO-1 | Zonula Occludens-1 |
References
- Enck, P.; Aziz, Q.; Barbara, G.; Farmer, A.D.; Fukudo, S.; Mayer, E.A.; Niesler, B.; Quigley, E.M.M.; Rajilić-Stojanović, M.; Schemann, M.; et al. Irritable bowel syndrome. Nat. Rev. Dis. Primers 2016, 2, 16014. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel disorders. Gastroenterology 2016, 150, 1393–1407.e5. [Google Scholar] [CrossRef] [PubMed]
- Weaver, K.R.; Melkus, G.D.; Henderson, W.A. Irritable Bowel Syndrome. Am. J. Nurs. 2017, 117, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Peery, A.F.; Dellon, E.S.; Lund, J.; Crockett, S.D.; McGowan, C.E.; Bulsiewicz, W.J.; Gangarosa, L.M.; Thiny, M.T.; Stizenberg, K.; Morgan, D.R.; et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 2012, 143, 1179–1187.e3. [Google Scholar] [CrossRef] [PubMed]
- Lovell, R.M.; Ford, A.C. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721.e4. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; De Giorgio, R.; Stanghellini, V.; Cremon, C.; Corinaldesi, R. A role for inflammation in irritable bowel syndrome? Gut 2002, 51 (Suppl. 1), i41–i44. [Google Scholar] [CrossRef]
- Barbara, G.; Zecchi, L.; Barbaro, R.; Cremon, C.; Bellacosa, L.; Marcellini, M.; De Giorgio, R.; Corinaldesi, R.; Stanghellini, V. Mucosal permeability and immune activation as potential therapeutic targets of probiotics in irritable bowel syndrome. J. Clin. Gastroenterol. 2012, 46, S52–S55. [Google Scholar] [CrossRef]
- Camilleri, M.; Gorman, H. Intestinal permeability and irritable bowel syndrome. Neurogastroenterol. Motil. 2007, 19, 545–552. [Google Scholar] [CrossRef]
- Tillisch, K.; Labus, J.S. Advances in imaging the brain-gut axis: Functional gastrointestinal disorders. Gastroenterology 2011, 140, 407–411.e1. [Google Scholar] [CrossRef]
- Tillisch, K.; Mayer, E.A.; Labus, J.S. Quantitative meta-analysis identifies brain regions activated during rectal distension in irritable bowel syndrome. Gastroenterology 2011, 140, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Cann, P.A.; Read, N.W.; Brown, C.; Hobson, N.; Holdsworth, C.D. Irritable bowel syndrome: Relationship of disorders in the transit of a single solid meal to symptom patterns. Gut 1983, 24, 405–411. [Google Scholar] [CrossRef]
- Stanghellini, V.; Tosetti, C.; Barbara, G.; De Giorgio, R.; Cogliandro, L.; Cogliandro, R.; Corinaldesi, R. Dyspeptic symptoms and gastric emptying in the irritable bowel syndrome. Am. J. Gastroenterol. 2002, 97, 2738–2743. [Google Scholar] [CrossRef]
- Chadwick, V.S.; Chen, W.; Shu, D.; Paulus, B.; Bethwaite, P.; Tie, A.; Wilson, I. Activation of the mucosal immune system in irritable bowel syndrome. Gastroenterology 2002, 122, 1778–1783. [Google Scholar] [CrossRef]
- Cremon, C.; Gargano, L.; Morselli-Labate, A.M.; Santini, D.; Cogliandro, R.F.; De Giorgio, R.; Stanghellini, V.; Corinaldesi, R.; Barbara, G. Mucosal immune activation in irritable bowel syndrome: Gender-dependence and association with digestive symptoms. Am. J. Gastroenterol. 2009, 104, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Mearin, F.; Perelló, A.; Balboa, A. Irritable bowel syndrome and inflammatory bowel disease: Is there a connection? Gastroenterol. Hepatol. 2009, 32, 364–372. [Google Scholar] [CrossRef]
- Ng, Q.X.; Yau, C.E.; Yaow, C.Y.L.; Chong, R.I.H.; Chong, N.Z.; Teoh, S.E.; Lim, Y.L.; Soh, A.Y.S.; Ng, W.K.; Thumboo, J. What Has Longitudinal ‘Omics’ Studies Taught Us about Irritable Bowel Syndrome? A Systematic Review. Metabolites 2023, 13, 484. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Lasch, K.; Zhou, W. Irritable bowel syndrome: Methods, mechanisms, and pathophysiology. The confluence of increased permeability, inflammation, and pain in irritable bowel syndrome. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G775–G785. [Google Scholar] [CrossRef]
- Ford, A.C.; Lacy, B.E.; Talley, N.J. Irritable Bowel Syndrome. N. Engl. J. Med. 2017, 376, 2566–2578. [Google Scholar] [CrossRef]
- Holtmann, G.J.; Ford, A.C.; Talley, N.J. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol. Hepatol. 2016, 1, 133–146. [Google Scholar] [CrossRef]
- Drossmann, D.A.; Chey, W.D.; Johanson, J.F.; Fass, R.; Scott, C.; Panas, R.; Ueno, R. Clinical trial: Lubiprostone in patients with constipation-associated irritable bowel syndrome—Results of two randomized, placebo-controlled studies. Aliment. Pharmacol. Ther. 2009, 29, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Moayyedi, P.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.R.; Quigley, E.M.M.; FACG for the Task Force on the Management of Functional Bowel Disorders. American College of Gastroenterology Monograph on the Management of Irritable Bowel Syndrome and Chronic Idiopathic Constipation. Off. J. Am. Coll. Gastroenterol. ACG 2014, 109, S2–S26. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Chang, L. Diagnosis and management of IBS. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Lembo, A.J.; Lacy, B.E.; Zuckerman, M.J.; Schey, R.; Dove, L.S.; Andrae, D.A.; Davenport, J.M.; McIntyre, G.; Lopez, R.; Turner, L.; et al. Eluxadoline for Irritable Bowel Syndrome with Diarrhea. N. Engl. J. Med. 2016, 374, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M.; Lembo, A.; Chey, W.D.; Zakko, S.; Ringel, Y.; Yu, J.; Mareya, S.M.; Shaw, A.L.; Bortey, E.; Forbes, W.P. Rifaximin Therapy for Patients with Irritable Bowel Syndrome without Constipation. N. Engl. J. Med. 2011, 364, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Regimbeau, C.; Benhamou, Y. Meta-analysis of smooth muscle relaxants in the treatment of irritable bowel syndrome. Aliment. Pharmacol. Ther. 2001, 15, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Halland, M.; Saito, Y.A. Irritable bowel syndrome: New and emerging treatments. BMJ Br. Med. J. 2015, 350, h1622. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, R.; Abdollahi, M. Herbal medicines for the management of irritable bowel syndrome: A comprehensive review. World J. Gastroenterol. 2012, 18, 589–600. [Google Scholar] [CrossRef]
- Bahrami, H.R.; Hamedi, S.; Salari, R.; Noras, M. Herbal Medicines for the Management of Irritable Bowel Syndrome: A Systematic Review. Electron. Physician 2016, 8, 2719–2725. [Google Scholar] [CrossRef]
- Hawrelak, J.A.; Wohlmuth, H.; Pattinson, M.; Myers, S.P.; Goldenberg, J.Z.; Harnett, J.; Cooley, K.; Van De Venter, C.; Reid, R.; Whitten, D.L. Western herbal medicines in the treatment of irritable bowel syndrome: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 48, 102233. [Google Scholar] [CrossRef]
- Bashan, I. Effect of berberine on irritable bowel syndrome: A symptom-based review. Int. J. Plant Based Pharm. 2022, 2, 190–195. [Google Scholar]
- Chen, C.; Lu, M.; Pan, Q.; Fichna, J.; Zheng, L.; Wang, K.; Yu, Z.; Li, Y.; Li, K.; Song, A.; et al. Berberine Improves Intestinal Motility and Visceral Pain in the Mouse Models Mimicking Diarrhea-Predominant Irritable Bowel Syndrome (IBS-D) Symptoms in an Opioid-Receptor Dependent Manner. PLoS ONE 2015, 10, e0145556. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Tao, C.; Liu, Z.; Lu, M.; Pan, Q.; Zheng, L.; Li, Q.; Song, Z.; Fichna, J. A Randomized Clinical Trial of Berberine Hydrochloride in Patients with Diarrhea-Predominant Irritable Bowel Syndrome. Phytother. Res. 2015, 29, 1822–1827. [Google Scholar] [CrossRef] [PubMed]
- Hou, Q.; Zhu, S.; Zhang, C.; Huang, Y.; Guo, Y.; Li, P.; Chen, X.; Wen, Y.; Han, Q.; Liu, F. Berberine improves intestinal epithelial tight junctions by upregulating A20 expression in IBS-D mice. Biomed. Pharmacother. 2019, 118, 109206. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-q.; Liu, J.-l.; Chen, G.-x.; Shen, D.-t.; Zhu, W.; Chen, X.-l.; Liu, F.-b.; Hou, Q.-k. Berberine Enhances Intestinal Mucosal Barrier Function by Promoting Vitamin D Receptor Activity. Chin. J. Integr. Med. 2023, 30, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Cui, H.; Li, T.; Qi, J.; Chen, H.; Gao, F.; Tian, X.; Mu, Y.; He, R.; Lv, S.; et al. Synergistic Effect of Berberine-Based Chinese Medicine Assembled Nanostructures on Diarrhea-Predominant Irritable Bowel Syndrome In Vivo. Front. Pharmacol. 2020, 11, 1210. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Huang, J.; Zhang, Y.; Huang, Z.; Yan, W.; Zhou, T.; Wang, Z.; Liao, L.; Cao, H.; Tan, B. Therapeutic Effects of Berberine Hydrochloride on Stress-Induced Diarrhea-Predominant Irritable Bowel Syndrome Rats by Inhibiting Neurotransmission in Colonic Smooth Muscle. Front. Pharmacol. 2021, 12, 596686. [Google Scholar] [CrossRef]
- Tang, Q.L.; Lai, M.L.; Zhong, Y.F.; Wang, A.M.; Su, J.K.; Zhang, M.Q. Antinociceptive effect of berberine on visceral hypersensitivity in rats. World J. Gastroenterol. 2013, 19, 4582–4589. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Feng, X.; Chang, Y.; Luo, J. Therapeutic Effect of Berberine (BBR) Combined with Probiotics on Irritable Bowel Syndrome through Regulation of Inflammatory Response. Lat. Am. J. Pharm. 2022, 41, 923–930. [Google Scholar]
- Yu, Z.C.; Cen, Y.X.; Wu, B.H.; Wei, C.; Xiong, F.; Li, D.F.; Liu, T.T.; Luo, M.H.; Guo, L.L.; Li, Y.X.; et al. Berberine prevents stress-induced gut inflammation and visceral hypersensitivity and reduces intestinal motility in rats. World J. Gastroenterol. 2019, 25, 3956–3971. [Google Scholar] [CrossRef]
- Zhang, J.D.; Liu, J.; Zhu, S.W.; Fang, Y.; Wang, B.; Jia, Q.; Hao, H.F.; Kao, J.Y.; He, Q.H.; Song, L.J.; et al. Berberine alleviates visceral hypersensitivity in rats by altering gut microbiome and suppressing spinal microglial activation. Acta Pharmacol. Sin. 2021, 42, 1821–1833. [Google Scholar] [CrossRef]
- Brinkhaus, B.; Hentschel, C.; Von Keudell, C.; Schindler, G.; Lindner, M.; Stützer, H.; Kohnen, R.; Willich, S.N.; Lehmacher, W.; Hahn, E.G. Herbal medicine with curcuma and fumitory in the treatment of irritable bowel syndrome: A randomized, placebo-controlled, double-blind clinical trial. Scand. J. Gastroenterol. 2005, 40, 936–943. [Google Scholar] [CrossRef]
- Bundy, R.; Walker, A.F.; Middleton, R.W.; Booth, J. Turmeric extract may improve irritable bowel syndrome symptomology in otherwise healthy adults: A pilot study. J. Altern. Complement. Med. 2004, 10, 1015–1018. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Portincasa, P.; Maes, N.; Albert, A. Efficacy of bio-optimized extracts of turmeric and essential fennel oil on the quality of life in patients with irritable bowel syndrome. Ann. Gastroenterol. 2018, 31, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Lior, O.; Sklerovsy-Benjaminov, F.; Lish, I.; Konokoff, F.; Naftali, T. Treatment of Irritable Bowel Syndrome with a Combination of Curcumin, Green Tea and Selenomethionine Has a Positive Effect on Satisfaction with Bowel Habits. J. Biosci. Med. 2019, 7, 170–179. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Smith, S.J.; Rea, A.; Michel, S. Efficacy of a curcumin extract (CurcugenTM) on gastrointestinal symptoms and intestinal microbiota in adults with self-reported digestive complaints: A randomised, double-blind, placebo-controlled study. BMC Complement. Med. Ther. 2021, 21, 40. [Google Scholar] [CrossRef]
- Portincasa, P.; Bonfrate, L.; Scribano, M.L.; Kohn, A.; Caporaso, N.; Festi, D.; Campanale, M.C.; Di Rienzo, T.; Guarino, M.; Taddia, M.; et al. Curcumin and Fennel Essential Oil Improve Symptoms and Quality of Life in Patients with Irritable Bowel Syndrome. J. Gastrointestin. Liver Dis. 2016, 25, 151–157. [Google Scholar] [CrossRef]
- Woźniak, M.; Fabisiak, A.; Talar-Wojnarowska, R.; Małecka-Wojciesko, E. The effect of curcumin on symptoms and quality of life in patients with irritable bowel syndrome. Postepy Hig. Med. Dosw. 2022, 76, 345–350. [Google Scholar] [CrossRef]
- Neag, M.A.; Mocan, A.; Echeverría, J.; Pop, R.M.; Bocsan, C.I.; Crişan, G.; Buzoianu, A.D. Berberine: Botanical Occurrence, Traditional Uses, Extraction Methods, and Relevance in Cardiovascular, Metabolic, Hepatic, and Renal Disorders. Front. Pharmacol. 2018, 9, 557. [Google Scholar] [CrossRef] [PubMed]
- Ts, G.; Kaginelli, S.; Basalingappa, K. Berberine and its pharmacological potential: A Review. Eur. J. Biomed 2020, 7, 115–123. [Google Scholar]
- Fuloria, S.; Mehta, J.; Chandel, A.; Sekar, M.; Rani, N.; Begum, M.Y.; Subramaniyan, V.; Chidambaram, K.; Thangavelu, L.; Nordin, R.; et al. A Comprehensive Review on the Therapeutic Potential of Curcuma longa Linn. in Relation to its Major Active Constituent Curcumin. Front. Pharmacol. 2022, 13, 820806. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B.; Harikumar, K.B. Potential therapeutic effects of curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. Int. J. Biochem. Cell Biol. 2009, 41, 40–59. [Google Scholar] [CrossRef]
- Dong, S.; Zeng, Q.; Mitchell, E.S.; Xiu, J.; Duan, Y.; Li, C.; Tiwari, J.K.; Hu, Y.; Cao, X.; Zhao, Z. Curcumin enhances neurogenesis and cognition in aged rats: Implications for transcriptional interactions related to growth and synaptic plasticity. PLoS ONE 2012, 7, e31211. [Google Scholar] [CrossRef] [PubMed]
- Ak, T.; Gülçin, I. Antioxidant and radical scavenging properties of curcumin. Chem. Biol. Interact. 2008, 174, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Dulbecco, P.; Savarino, V. Therapeutic potential of curcumin in digestive diseases. World J. Gastroenterol. 2013, 19, 9256–9270. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Gkiouras, K.; Theodoridis, X.; Asteriou, E.; Forbes, A.; Bogdanos, D.P. Oral Adjuvant Curcumin Therapy for Attaining Clinical Remission in Ulcerative Colitis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 1737. [Google Scholar] [CrossRef]
- Yu, J.; Xu, W.H.; Sun, W.; Sun, Y.; Guo, Z.L.; Yu, X.L. Curcumin Alleviates the Functional Gastrointestinal Disorders of Mice In Vivo. J. Med. Food 2017, 20, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L. The Problem of Curcumin and Its Bioavailability: Could Its Gastrointestinal Influence Contribute to Its Overall Health-Enhancing Effects? Adv. Nutr. 2018, 9, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, E.; Sharma, S.; Jadhav, K.; Banerjee, R. Combinatorial liposomes of berberine and curcumin inhibit biofilm formation and intracellular methicillin resistant Staphylococcus aureus infections and associated inflammation. J. Mater. Chem. B 2021, 9, 864–875. [Google Scholar] [CrossRef]
- Deutch, C.E. Synergistic inhibition of the urinary tract pathogen Staphylococcus saprophyticus by curcumin and berberine. Int. J. Herb. Med. 2022, 10, 1–8. [Google Scholar] [CrossRef]
- Neyrinck, A.M.; Sánchez, C.R.; Rodriguez, J.; Cani, P.D.; Bindels, L.B.; Delzenne, N.M. Prebiotic Effect of Berberine and Curcumin Is Associated with the Improvement of Obesity in Mice. Nutrients 2021, 13, 1436. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, A.; Umar, S.M.; Dev, J.R.A.; Mendiratta, M.; Prasad, C.P. In vitro anticancer efficacy of a polyphenolic combination of Quercetin, Curcumin, and Berberine in triple negative breast cancer (TNBC) cells. Phytomedicine Plus 2022, 2, 100265. [Google Scholar] [CrossRef]
- Maiti, P.; Plemmons, A.; Dunbar, G.L. Combination treatment of berberine and solid lipid curcumin particles increased cell death and inhibited PI3K/Akt/mTOR pathway of human cultured glioblastoma cells more effectively than did individual treatments. PLoS ONE 2019, 14, e0225660. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhang, C.; Bao, J.; Jia, X.; Liang, Y.; Wang, X.; Chen, M.; Su, H.; Li, P.; Wan, J.B.; et al. Synergistic chemopreventive effects of curcumin and berberine on human breast cancer cells through induction of apoptosis and autophagic cell death. Sci. Rep. 2016, 6, 26064. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Jiang, Z.; Xu, J.; Zhang, J.; Sun, R.; Zhou, J.; Lu, Y.; Gong, Z.; Huang, J.; Shen, X.; et al. Improving the ameliorative effects of berberine and curcumin combination via dextran-coated bilosomes on non-alcohol fatty liver disease in mice. J. Nanobiotechnology 2021, 19, 230. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.W.; Kuang, S.Y.; Tu, C.; Ma, Z.J.; Pang, J.Y.; Wang, Y.H.; Zang, Q.C.; Liu, T.S.; Zhao, Y.L.; Xiao, X.H.; et al. Natural products berberine and curcumin exhibited better ameliorative effects on rats with non-alcohol fatty liver disease than lovastatin. Biomed. Pharmacother. 2018, 99, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Li, C.; Zhang, D.; Yuan, M.; Chen, C.H.; Li, M. Synergic Effects of Berberine and Curcumin on Improving Cognitive Function in an Alzheimer’s Disease Mouse Model. Neurochem. Res. 2020, 45, 1130–1141. [Google Scholar] [CrossRef]
- Belgian Statute Gazette: 7 MAI 2004.—Loi Relative Aux Expérimentations sur la Personne Humaine. Available online: https://www.ejustice.just.fgov.be/cgi_loi/change_lg.pl?language=fr&la=F&cn=2004050732&table_name=loi (accessed on 11 March 2024).
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef]
- Yan, F.; Wang, L.; Shi, Y.; Cao, H.; Liu, L.; Washington, M.K.; Chaturvedi, R.; Israel, D.A.; Cao, H.; Wang, B. Berberine promotes recovery of colitis and inhibits inflammatory responses in colonic macrophages and epithelial cells in DSS-treated mice. Am. J. Physiol.-Gastrointest. Liver Physiol. 2012, 302, G504–G514. [Google Scholar] [CrossRef]
- Farzaei, M.H.; Bahramsoltani, R.; Abdollahi, M.; Rahimi, R. The Role of Visceral Hypersensitivity in Irritable Bowel Syndrome: Pharmacological Targets and Novel Treatments. J. Neurogastroenterol. Motil. 2016, 22, 558–574. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Guo, Q.; Lu, N. Role of Gut Microbiota in the Pharmacological Effects of Natural Products. Evid. Based Complement. Alternat. Med. 2019, 2019, 2682748. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Xu, J.H.; Yu, T.; Chen, Q.K. Effects of berberine and metformin on intestinal inflammation and gut microbiome composition in db/db mice. Biomed. Pharmacother. 2019, 118, 109131. [Google Scholar] [CrossRef] [PubMed]
- Jia, Q.; Zhang, L.; Zhang, J.; Pei, F.; Zhu, S.; Sun, Q.; Duan, L. Fecal Microbiota of Diarrhea-Predominant Irritable Bowel Syndrome Patients Causes Hepatic Inflammation of Germ-Free Rats and Berberine Reverses It Partially. Biomed Res. Int. 2019, 2019, 4530203. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chang, L.; Zhang, X.; Ning, Z.; Mayne, J.; Ye, Y.; Stintzi, A.; Liu, J.; Figeys, D. Berberine and its structural analogs have differing effects on functional profiles of individual gut microbiomes. Gut Microbes 2020, 11, 1348–1361. [Google Scholar] [CrossRef]
- Jafarzadeh, E.; Shoeibi, S.; Bahramvand, Y.; Nasrollahi, E.; Maghsoudi, A.S.; Yazdi, F.; KarkonShayan, S.; Hassani, S. Turmeric for Treatment of Irritable Bowel Syndrome: A Systematic Review of Population-Based Evidence. Iran J. Public Health 2022, 51, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Koh, S.S.H.; Chan, H.W.; Ho, C.Y.X. Clinical Use of Curcumin in Depression: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; Maffioli, P.; Simental-Mendía, L.E.; Bo, S.; Sahebkar, A. Effect of curcumin on circulating interleukin-6 concentrations: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2016, 111, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Lim, D.Y.; Yeo, W.-S. The role of inflammation in irritable bowel syndrome (IBS). J. Inflamm. Res. 2018, 11, 345–349. [Google Scholar] [CrossRef]
- Hewlings, S.J.; Kalman, D.S. Curcumin: A Review of Its Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef]
- Jurenka, J.S. Anti-inflammatory properties of curcumin, a major constituent of Curcuma longa: A review of preclinical and clinical research. Altern. Med. Rev. 2009, 14, 141–153. [Google Scholar] [PubMed]
- Grover, M.; Camilleri, M. Effects on gastrointestinal functions and symptoms of serotonergic psychoactive agents used in functional gastrointestinal diseases. J. Gastroenterol. 2013, 48, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wu, S.; Li, J.; Wang, R.; Xie, X.; Yu, X.; Pan, J.; Xu, Y.; Zheng, L. The effect of curcumin on the brain-gut axis in rat model of irritable bowel syndrome: Involvement of 5-HT-dependent signaling. Metab. Brain Dis. 2015, 30, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Wang, H.; Zhang, P.; Gao, C.; Tao, J.; Ge, Z.; Zhu, D.; Bi, Y. Modulation of gut microbiota contributes to curcumin-mediated attenuation of hepatic steatosis in rats. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 1801–1812. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Liu, X.; Wu, N.; Han, Y.; Wang, J.; Yu, Y.; Chen, Q. Efficacy and Safety of Berberine Alone for Several Metabolic Disorders: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Front. Pharmacol. 2021, 12, 653887. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, X.; Zou, D.; Liu, W.; Yang, J.; Zhu, N.; Huo, L.; Wang, M.; Hong, J.; Wu, P.; et al. Treatment of type 2 diabetes and dyslipidemia with the natural plant alkaloid berberine. J. Clin. Endocrinol. Metab. 2008, 93, 2559–2565. [Google Scholar] [CrossRef]
- Liang, Y.; Xu, X.; Yin, M.; Zhang, Y.; Huang, L.; Chen, R.; Ni, J. Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: A systematic literature review and a meta-analysis. Endocr. J. 2019, 66, 51–63. [Google Scholar] [CrossRef]
- Lan, J.; Zhao, Y.; Dong, F.; Yan, Z.; Zheng, W.; Fan, J.; Sun, G. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension. J. Ethnopharmacol. 2015, 161, 69–81. [Google Scholar] [CrossRef]
- Yang, L.; Zhu, W.; Zhang, X.; Zhou, X.; Wu, W.; Shen, T. Efficacy and safety of berberine for several cardiovascular diseases: A systematic review and meta-analysis of randomized controlled trials. Phytomedicine 2023, 112, 154716. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration GRAS Notices. Available online: https://www.cfsanappsexternal.fda.gov/scripts/fdcc/index.cfm?set=GRASNotices&sort=GRN_No&order=DESC&startrow=1&type=basic&search=turmeric (accessed on 11 March 2024).
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar]
- Sharma, R.A.; Euden, S.A.; Platton, S.L.; Cooke, D.N.; Shafayat, A.; Hewitt, H.R.; Marczylo, T.H.; Morgan, B.; Hemingway, D.; Plummer, S.M.; et al. Phase I clinical trial of oral curcumin: Biomarkers of systemic activity and compliance. Clin. Cancer Res. 2004, 10, 6847–6854. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IBS Symptoms | n | Score at T0 | Score at T1 | Difference T1−T0 (95% CI) | p-Value | Change (%) |
|---|---|---|---|---|---|---|
| Abdominal pain | 146 | 60.2 ± 19.8 | 31.8 ± 19.6 | 28.4 (25.1–31.7) | <0.0001 | 47.2 |
| Abdominal distension | 146 | 64.0 ± 20.1 | 33.3 ± 20.8 | 30.7 (26.9–34.4) | <0.0001 | 48.0 |
| Intestinal transit | 146 | 66.0 ± 19.1 | 35.1 ± 20.8 | 30.9 (27.1–34.8) | <0.0001 | 46.8 |
| Influence on quality of life | 146 | 65.1 ± 17.2 | 33.8 ± 20.2 | 31.3 (27.8–34.8) | <0.0001 | 48.1 |
| IBSSI | 146 | 255 ± 55 | 134 ± 71.1 | 121 (109–133) | <0.0001 | 47.5 |
| Weekly stool passage frequency | ||||||
| Minimum | 128 | 7.3 ± 6.6 | 6.7 ± 4.3 | 0.58 (−0.43–1.58) | 0.26 | 8.2 |
| Maximum | 129 | 16.5 ± 11.9 | 12.0 ± 7.5 | 4.57 (2.94–6.21) | <0.0001 | 27.3 |
| Concomitant IBS Treatment | Number of Medications or Use | T0 | T1 | Percent Decrease in Patients on Concomitant Treatment |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Antispasmodic medication | 64.0 | |||
| 0 | 96 (65.8) | 128 (87.7) | ||
| 1 | 43 (29.4) | 14 (9.6) | ||
| 2 | 7 (4.8) | 3 (2.0) | ||
| 3 | 1 (0.7) | |||
| Antidiarrhoeic medication | 64.6 | |||
| 0 | 132 (90.4) | 141 (96.6) | ||
| 1 | 13 (8.9) | 3 (2.0) | ||
| 2 | 1 (0.7) | 2 (1.4) | ||
| Laxative medication | 13.3 | |||
| 0 | 123 (84.2) | 126 (86.3) | ||
| 1 | 19 (13.1) | 19 (13.0) | ||
| 2 | 4 (2.7) | 1 (0.7) | ||
| Antidepressants benzodiazepines | 8.9 | |||
| No | 97 (66.4) | 100 (69.4) | ||
| Yes | 49 (33.6) | 44 (30.6) | ||
| Probiotics | 38.0 | |||
| No | 101 (69.7) | 117 (81.2) | ||
| Yes | 44 (30.3) | 27 (18.8) | ||
| Food restriction | 28.5 | |||
| No | 88 (61.1) | 104 (72.2) | ||
| Yes | 56 (38.9) | 40 (27.8) |
| Concomitant Treatment | Without Treatment | With Treatment | |||
|---|---|---|---|---|---|
| n | IBSSI Score | n | IBSSI Score | p-Value | |
| Antispasmodic | 96 | 119.5 ± 73.5 | 50 | 124.6 ± 74.1 | 0.70 |
| Antidiarrhoeic medication | 132 | 119.1 ± 75.6 | 14 | 141.7 ± 46.9 | 0.27 |
| Laxative medication | 123 | 125.0 ± 74.8 | 23 | 101.3 ± 64.2 | 0.16 |
| Antidepressants/benzodiazepines | 97 | 124.3 ± 71.3 | 49 | 115.2 ± 78.0 | 0.48 |
| Probiotics | 101 | 118.8 ± 75.9 | 44 | 126.0 ± 69.0 | 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wade, U.; Pascual-Figal, D.A.; Rabbani, F.; Ernst, M.; Albert, A.; Janssens, I.; Dierckxsens, Y.; Iqtadar, S.; Khokhar, N.A.; Kanwal, A.; et al. The Possible Synergistic Pharmacological Effect of an Oral Berberine (BBR) and Curcumin (CUR) Complementary Therapy Alleviates Symptoms of Irritable Bowel Syndrome (IBS): Results from a Real-Life, Routine Clinical Practice Settings-Based Study. Nutrients 2024, 16, 1204. https://doi.org/10.3390/nu16081204
Wade U, Pascual-Figal DA, Rabbani F, Ernst M, Albert A, Janssens I, Dierckxsens Y, Iqtadar S, Khokhar NA, Kanwal A, et al. The Possible Synergistic Pharmacological Effect of an Oral Berberine (BBR) and Curcumin (CUR) Complementary Therapy Alleviates Symptoms of Irritable Bowel Syndrome (IBS): Results from a Real-Life, Routine Clinical Practice Settings-Based Study. Nutrients. 2024; 16(8):1204. https://doi.org/10.3390/nu16081204
Chicago/Turabian StyleWade, Ursula, Domingo A. Pascual-Figal, Fazale Rabbani, Marie Ernst, Adelin Albert, Isabelle Janssens, Yvan Dierckxsens, Somia Iqtadar, Nisar A. Khokhar, Ayesha Kanwal, and et al. 2024. "The Possible Synergistic Pharmacological Effect of an Oral Berberine (BBR) and Curcumin (CUR) Complementary Therapy Alleviates Symptoms of Irritable Bowel Syndrome (IBS): Results from a Real-Life, Routine Clinical Practice Settings-Based Study" Nutrients 16, no. 8: 1204. https://doi.org/10.3390/nu16081204