
Beneficial Effect of Heat-Killed Lactic Acid Bacterium Lactobacillus johnsonii No. 1088 on Temporal Gastroesophageal Reflux-Related Symptoms in Healthy Volunteers: A Randomized, Placebo-Controlled, Double-Blind, Parallel-Group Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Test Foods
2.4. Measurements
2.4.1. Primary Endpoint
2.4.2. Secondary Endpoints
2.4.3. Blood Tests and Urinalysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
3.2. The Effect of Heat-Killed LJ88 on Gastroesophageal Reflux-Related Symptoms
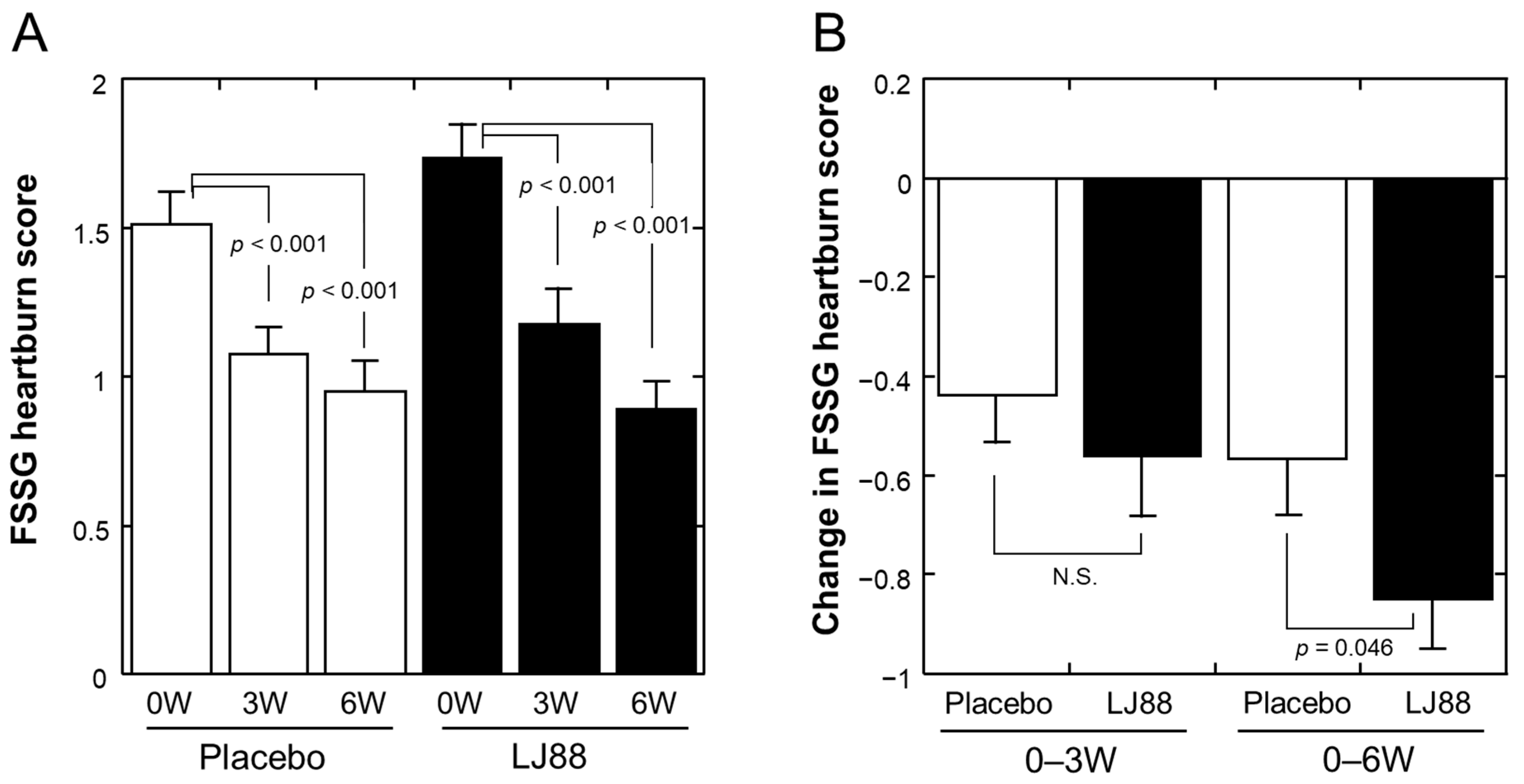
3.2.1. FSSG
3.2.2. GSRS
3.2.3. Stomach State Questionnaire
3.2.4. Serum Gastrin Concentration
3.3. Psychological Symptoms and Quality of Life
3.3.1. POMS2
3.3.2. SF36v2
3.4. Safety Aspects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naliboff, B.D.; Mayer, M.; Fass, R.; Fitzgerald, L.Z.; Chang, L.; Bolus, R.; Mayer, E.A. The effect of life stress on symptoms of heartburn. Psychosom. Med. 2004, 66, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Oliveria, S.A.; Christos, P.J.; Talley, N.J.; Dannenberg, A.J. Heartburn risk factors, knowledge, and prevention strategies: A population-based survey of individuals with heartburn. Arch. Intern. Med. 1999, 159, 1592–1598. [Google Scholar] [CrossRef] [PubMed]
- Wickramasinghe, N.; Thuraisingham, A.; Jayalath, A.; Wickramasinghe, D.; Samarasekara, N.; Yazaki, E.; Devanarayana, N.M. The association between symptoms of gastroesophageal reflux disease and perceived stress: A countrywide study of Sri Lanka. PLoS ONE 2023, 18, e0294135. [Google Scholar] [CrossRef] [PubMed]
- Yadlapati, R.; Gyawali, C.P.; Pandolfino, J.E.; Participants, C.G.C.C. AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review. Clin. Gastroenterol. Hepatol. 2022, 20, 984–994.e981. [Google Scholar] [CrossRef]
- Young, A.; Kumar, M.A.; Thota, P.N. GERD: A practical approach. Cleve Clin. J. Med. 2020, 87, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Iwakiri, K.; Fujiwara, Y.; Manabe, N.; Ihara, E.; Kuribayashi, S.; Akiyama, J.; Kondo, T.; Yamashita, H.; Ishimura, N.; Kitasako, Y.; et al. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2021. J. Gastroenterol. 2022, 57, 267–285. [Google Scholar] [CrossRef] [PubMed]
- Gomi, A.; Yamaji, K.; Watanabe, O.; Yoshioka, M.; Miyazaki, K.; Iwama, Y.; Urita, Y. Bifidobacterium bifidum YIT 10347 fermented milk exerts beneficial effects on gastrointestinal discomfort and symptoms in healthy adults: A double-blind, randomized, placebo-controlled study. J. Dairy Sci. 2018, 101, 4830–4841. [Google Scholar] [CrossRef] [PubMed]
- Takagi, A.; Yanagi, H.; Ozawa, H.; Uemura, N.; Nakajima, S.; Inoue, K.; Kawai, T.; Ohtsu, T.; Koga, Y. Effects of Lactobacillus gasseri OLL2716 on Helicobacter pylori-Associated Dyspepsia: A Multicenter Randomized Double-Blind Controlled Trial. Gastroenterol. Res. Pract. 2016, 2016, 7490452. [Google Scholar] [CrossRef]
- Ohtsu, T.; Takagi, A.; Uemura, N.; Inoue, K.; Sekino, H.; Kawashima, A.; Uchida, M.; Koga, Y. The Ameliorating Effect of Lactobacillus gasseri OLL2716 on Functional Dyspepsia in Helicobacter pylori-Uninfected Individuals: A Randomized Controlled Study. Digestion 2017, 96, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Ohtsu, T.; Haruma, K.; Ide, Y.; Takagi, A. The Effect of Continuous Intake of Lactobacillus gasseri OLL2716 on Mild to Moderate Delayed Gastric Emptying: A Randomized Controlled Study. Nutrients 2021, 13, 1852. [Google Scholar] [CrossRef] [PubMed]
- Otomi, K.; Ymaguchi, T.; Watanabe, S.; Kobayashi, A.; Kobayashi, K.; Hashiguchi, N. Effects of Yogurt Containing Lactobacillus gasseri OLL2716 on Autonomic Nerve Activities and Physiological Functions. Health 2015, 7, 397–405. [Google Scholar] [CrossRef]
- Pantoflickova, D.; Corthesy-Theulaz, I.; Dorta, G.; Stolte, M.; Isler, P.; Rochat, F.; Enslen, M.; Blum, A.L. Favourable effect of regular intake of fermented milk containing Lactobacillus johnsonii on Helicobacter pylori associated gastritis. Aliment. Pharmacol. Ther. 2003, 18, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Guarner, F.; Schaafsma, G.J. Probiotics. Int. J. Food Microbiol. 1998, 39, 237–238. [Google Scholar] [CrossRef]
- Aiba, Y.; Nakano, Y.; Koga, Y.; Takahashi, K.; Komatsu, Y. A highly acid-resistant novel strain of Lactobacillus johnsonii No. 1088 has antibacterial activity, including that against Helicobacter pylori, and inhibits gastrin-mediated acid production in mice. Microbiologyopen 2015, 4, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S.; Collado, M.C.; Endo, A.; Hill, C.; Lebeer, S.; Quigley, E.M.M.; Sanders, M.E.; Shamir, R.; Swann, J.R.; Szajewska, H.; et al. The International Scientific Association of Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of postbiotics. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 649–667. [Google Scholar] [CrossRef] [PubMed]
- Aiba, Y.; Ishikawa, H.; Tokunaga, M.; Komatsu, Y. Anti-Helicobacter pylori activity of non-living, heat-killed form of lactobacilli including Lactobacillus johnsonii No.1088. FEMS Microbiol. Lett. 2017, 364, fnx102. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, Y.; Aiba, Y.; Nakano, Y.; Koga, Y. Probiotics, prebiotics, and biogenics for the stomach. In Prebiotics and Probiotics in Human Nutrition and Health; Rao, V., Rao, L.G., Eds.; InTech: Rijeka, Croatia, 2016; pp. 363–381. [Google Scholar]
- Komatsu, Y.; Sasaki, T.; Ohishi, M. Effect of heat-killed Lactobacillus johnsonii No.1088 on gastroesophageal reflux disease-related symptoms: A pilot clinical study. Am. J. Food Sci. Health 2016, 2, 176–185. [Google Scholar]
- Kusano, M.; Shimoyama, Y.; Sugimoto, S.; Kawamura, O.; Maeda, M.; Minashi, K.; Kuribayashi, S.; Higuchi, T.; Zai, H.; Ino, K.; et al. Development and evaluation of FSSG: Frequency scale for the symptoms of GERD. J. Gastroenterol. 2004, 39, 888–891. [Google Scholar] [CrossRef]
- Kusano, M.; Shimoyama, Y.; Kawamura, O.; Maeda, M.; Kuribayashi, S.; Nagoshi, A.; Zai, H.; Moki, F.; Horikoshi, T.; Toki, M.; et al. Proton pump inhibitors improve acid-related dyspepsia in gastroesophageal reflux disease patients. Dig. Dis. Sci. 2007, 52, 1673–1677. [Google Scholar] [CrossRef] [PubMed]
- Stanghellini, V.; Chan, F.K.; Hasler, W.L.; Malagelada, J.R.; Suzuki, H.; Tack, J.; Talley, N.J. Gastroduodenal Disorders. Gastroenterology 2016, 150, 1380–1392. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Svedlund, J.; Sjodin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Heuchert, J.P.; McNair, D.M. Profile of Mood States Second Edition: POMS2; Multi-Health Systems (MHS): North Tonawanda, NY, USA, 2012. [Google Scholar]
- Yokoyama, K.; Araki, S.; Kawakami, N.; Takeshita, T. Production of the Japanese edition of profile of mood states (POMS): Assessment of reliability and validity. Nihon Koshu Eisei Zasshi 1990, 37, 913–918. (In Japanese) [Google Scholar] [PubMed]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J. Clin. Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Ware, J.E., Jr.; Kosinski, M.; Wada, S.; Gandek, B. Psychometric and clinical tests of validity of the Japanese SF-36 Health Survey. J. Clin. Epidemiol. 1998, 51, 1045–1053. [Google Scholar] [CrossRef]
- Fatani, A.; Vaher, K.; Rivero-Mendoza, D.; Alabasi, K.; Dahl, W.J. Fermented soy supplementation improves indicators of quality of life: A randomized, placebo-controlled, double-blind trial in adults experiencing heartburn. BMC Res. Notes 2020, 13, 364. [Google Scholar] [CrossRef] [PubMed]
- Hanaishi, T.; Sakai, M.; Igarashi, T.; Tsukioka, T. Basic performance evaluation of a serum gastrin kit, gastrin RIA kit DP. Jpn. J. Med. Phrm. Sci. 2023, 80, 513–520. (In Japanese) [Google Scholar]
- Holtmann, G.; Talley, N.J. The stomach-brain axis. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 967–979. [Google Scholar] [CrossRef] [PubMed]
- Aziz, Q.; Fass, R.; Gyawali, C.P.; Miwa, H.; Pandolfino, J.E.; Zerbib, F. Functional Esophageal Disorders. Gastroenterology 2016, 150, 1368–1379. [Google Scholar] [CrossRef]
- Liu, T.; Liu, J.; Wang, C.; Zou, D.; Wang, C.; Xu, T.; Ci, Y.; Guo, X.; Qi, X. Prevalence of gastrointestinal symptoms and their association with psychological problems in youths. Ann. Palliat. Med. 2023, 12, 311–323. [Google Scholar] [CrossRef]
- Kato-Kataoka, A.; Nishida, K.; Takada, M.; Kawai, M.; Kikuchi-Hayakawa, H.; Suda, K.; Ishikawa, H.; Gondo, Y.; Shimizu, K.; Matsuki, T.; et al. Fermented Milk Containing Lactobacillus casei Strain Shirota Preserves the Diversity of the Gut Microbiota and Relieves Abdominal Dysfunction in Healthy Medical Students Exposed to Academic Stress. Appl. Environ. Microbiol. 2016, 82, 3649–3658. [Google Scholar] [CrossRef]
- Takada, M.; Nishida, K.; Kataoka-Kato, A.; Gondo, Y.; Ishikawa, H.; Suda, K.; Kawai, M.; Hoshi, R.; Watanabe, O.; Igarashi, T.; et al. Probiotic Lactobacillus casei strain Shirota relieves stress-associated symptoms by modulating the gut-brain interaction in human and animal models. Neurogastroenterol. Motil. 2016, 28, 1027–1036. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | All Participants (n = 120) | Placebo Group (n = 60) | LJ88 Group (n = 60) | p-Value | (Method) (1) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | female | 67 | 33 | 34 | 1.000 | (Fisher’s exact test) | ||||||
| male | 53 | 27 | 26 | |||||||||
| Age (Years) | 46.7 | ± | 10.2 | 46.9 | ± | 9.7 | 46.5 | ± | 10.7 | 0.817 | (Student’s t-test) | |
| (21–63) (2) | (23–63) (2) | (21–63) (2) | ||||||||||
| Height (cm) | 164.6 | ± | 8.4 | 164.7 | ± | 8.7 | 164.6 | ± | 8.1 | 0.922 | ||
| Body weight (kg) | 60.4 | ± | 11.5 | 60.6 | ± | 11.5 | 60.3 | ± | 11.5 | 0.889 | ||
| BMI | 22.2 | ± | 3.2 | 22.2 | ± | 3.1 | 22.1 | ± | 3.3 | 0.887 | ||
| Systolic blood pressure (mmHg) | 116.9 | ± | 14.1 | 119.2 | ± | 15.2 | 114.7 | ± | 12.7 | 0.086 | ||
| Diastolic blood pressure (mmHg) | 72.5 | ± | 10.1 | 73.0 | ± | 10.9 | 72.1 | ± | 9.4 | 0.629 | ||
| Pulse rate (bpm) | 69.0 | ± | 8.8 | 68.4 | ± | 8.5 | 69.7 | ± | 9.2 | 0.434 | ||
| FSSG total score | 22.2 | ± | 5.8 | 22.0 | ± | 5.4 | 22.4 | ± | 6.2 | 0.805 | (Wilcoxon rank sum test) | |
| (14–47) (2) | (15–35) (2) | (14–47) (2) | ||||||||||
| Items | Group | n | FSSG Scores | Change in FSSG Scores | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 W | 3 W | 6 W | 0–3 W | 0–6 W | |||||||||||||||||
| Mean | ± | SD | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (2) | Mean | ± | SD | p Value (2) | |||
| 1. Do you get heartburn? | >Placebo | >55 | 1.51 | ± | 0.79 | 1.07 | ± | 0.63 | 0.000 | 0.95 | ± | 0.73 | 0.000 | −0.44 | ± | 0.71 | 0.334 | −0.56 | ± | 0.86 | 0.046 |
| LJ88 | 52 | 1.73 | ± | 0.82 | 1.17 | ± | 0.86 | 0.000 | 0.88 | ± | 0.65 | 0.000 | −0.56 | ± | 0.89 | −0.85 | ± | 0.72 | |||
| 2. Does your stomach get bloated? | Placebo | 55 | 1.62 | ± | 0.89 | 1.31 | ± | 0.90 | 0.002 | 1.20 | ± | 0.97 | 0.003 | −0.31 | ± | 0.66 | 0.305 | −0.42 | ± | 0.94 | 0.209 |
| LJ88 | 52 | 1.92 | ± | 0.99 | 1.48 | ± | 0.96 | 0.002 | 1.23 | ± | 0.90 | 0.000 | −0.44 | ± | 0.92 | −0.69 | ± | 0.96 | |||
| 3. Does your stomach ever feel heavy after meals? | Placebo | 55 | 1.78 | ± | 0.74 | 1.27 | ± | 0.73 | 0.000 | 1.07 | ± | 0.81 | 0.000 | −0.51 | ± | 0.84 | 0.075 | −0.71 | ± | 0.63 | 0.199 |
| LJ88 | 52 | 1.69 | ± | 0.81 | 1.40 | ± | 0.85 | 0.016 | 1.23 | ± | 0.67 | 0.002 | −0.29 | ± | 0.82 | −0.46 | ± | 0.94 | |||
| 4. Do you sometimes subconsciously rub your chest with your hand? | Placebo | 55 | 0.82 | ± | 0.84 | 0.53 | ± | 0.69 | 0.001 | 0.40 | ± | 0.60 | 0.000 | −0.29 | ± | 0.60 | 0.896 | −0.42 | ± | 0.79 | 0.209 |
| LJ88 | 52 | 0.94 | ± | 0.87 | 0.69 | ± | 0.85 | 0.029 | 0.37 | ± | 0.63 | 0.000 | −0.25 | ± | 0.79 | −0.58 | ± | 0.78 | |||
| 5. Do you ever feel sick after meals? | Placebo | 55 | 1.15 | ± | 0.99 | 0.73 | ± | 0.62 | 0.002 | 0.64 | ± | 0.75 | 0.001 | −0.42 | ± | 0.92 | 0.107 | −0.51 | ± | 1.00 | 0.614 |
| LJ88 | 52 | 1.12 | ± | 0.92 | 1.00 | ± | 0.74 | 0.419 | 0.71 | ± | 0.72 | 0.003 | −0.12 | ± | 0.92 | −0.40 | ± | 0.89 | |||
| 6. Do you get heartburn after meals? | Placebo | 55 | 1.49 | ± | 0.90 | 1.02 | ± | 0.73 | 0.001 | 0.82 | ± | 0.72 | 0.000 | −0.47 | ± | 0.92 | 0.509 | −0.67 | ± | 0.86 | 0.812 |
| LJ88 | 52 | 1.50 | ± | 0.87 | 1.13 | ± | 0.74 | 0.001 | 0.83 | ± | 0.76 | 0.000 | −0.37 | ± | 0.69 | −0.67 | ± | 0.76 | |||
| 7. Do you have an unusual (e.g., burning) sensation in your throat? | Placebo | 55 | 0.65 | ± | 0.87 | 0.47 | ± | 0.77 | 0.116 | 0.25 | ± | 0.62 | 0.001 | −0.18 | ± | 0.82 | 0.335 | −0.40 | ± | 0.78 | 0.051 |
| LJ88 | 52 | 0.42 | ± | 0.85 | 0.33 | ± | 0.71 | 0.519 | 0.25 | ± | 0.71 | 0.132 | −0.10 | ± | 0.87 | −0.17 | ± | 0.90 | |||
| 8. Do you feel full while eating meals? | Placebo | 55 | 1.20 | ± | 1.03 | 0.96 | ± | 0.96 | 0.051 | 0.96 | ± | 1.04 | 0.104 | −0.24 | ± | 0.86 | 0.760 | −0.24 | ± | 1.00 | 0.482 |
| LJ88 | 52 | 1.23 | ± | 1.02 | 0.94 | ± | 0.92 | 0.024 | 0.90 | ± | 1.01 | 0.018 | −0.29 | ± | 0.87 | −0.33 | ± | 0.98 | |||
| 9. Do some things get stuck when you swallow? | Placebo | 55 | 0.80 | ± | 0.93 | 0.55 | ± | 0.72 | 0.037 | 0.44 | ± | 0.66 | 0.008 | −0.25 | ± | 0.87 | 0.783 | −0.36 | ± | 0.97 | 0.590 |
| LJ88 | 52 | 0.69 | ± | 0.81 | 0.40 | ± | 0.66 | 0.008 | 0.33 | ± | 0.73 | 0.003 | −0.29 | ± | 0.75 | −0.37 | ± | 0.91 | |||
| 10. Do you get bitter liquid (acid) coming up into your throat? | Placebo | 55 | 1.09 | ± | 0.91 | 0.78 | ± | 0.71 | 0.006 | 0.60 | ± | 0.71 | 0.000 | −0.31 | ± | 0.79 | 0.891 | −0.49 | ± | 0.81 | 0.774 |
| LJ88 | 52 | 1.00 | ± | 0.79 | 0.73 | ± | 0.72 | 0.008 | 0.60 | ± | 0.77 | 0.000 | −0.27 | ± | 0.69 | −0.40 | ± | 0.66 | |||
| 11. Do you burp a lot? | Placebo | 55 | 1.45 | ± | 1.07 | 1.11 | ± | 0.96 | 0.002 | 1.11 | ± | 0.98 | 0.003 | −0.35 | ± | 0.78 | 0.735 | −0.35 | ± | 0.80 | 0.265 |
| LJ88 | 52 | 1.60 | ± | 0.93 | 1.17 | ± | 0.86 | 0.001 | 1.10 | ± | 0.91 | 0.000 | −0.42 | ± | 0.78 | −0.50 | ± | 0.75 | |||
| 12. Do you get heartburn if you bend over? | Placebo | 55 | 0.85 | ± | 1.01 | 0.73 | ± | 0.91 | 0.231 | 0.55 | ± | 0.86 | 0.009 | −0.13 | ± | 0.86 | 0.124 | −0.31 | ± | 0.81 | 0.377 |
| LJ88 | 52 | 0.81 | ± | 0.74 | 0.50 | ± | 0.70 | 0.005 | 0.44 | ± | 0.73 | 0.002 | −0.31 | ± | 0.73 | −0.37 | ± | 0.84 | |||
| Total score | Placebo | 55 | 14.42 | ± | 6.24 | 10.53 | ± | 4.89 | 0.000 | 8.98 | ± | 5.77 | 0.000 | −3.89 | ± | 5.32 | 0.710 | −5.44 | ± | 5.71 | 0.376 |
| LJ88 | 52 | 14.65 | ± | 5.75 | 10.96 | ± | 5.63 | 0.000 | 8.87 | ± | 6.10 | 0.000 | −3.69 | ± | 4.74 | −5.79 | ± | 5.78 | |||
| Sub-score: Acid reflux related symptom (1, 4, 6, 7, 9, 10, 12) | Placebo | 55 | 7.22 | ± | 4.22 | 5.15 | ± | 2.85 | 0.000 | 4.00 | ± | 3.18 | 0.000 | −2.07 | ± | 3.34 | 0.466 | −3.22 | ± | 3.73 | 0.248 |
| LJ88 | 52 | 7.10 | ± | 3.60 | 4.96 | ± | 3.27 | 0.000 | 3.69 | ± | 3.67 | 0.000 | −2.13 | ± | 2.70 | −3.40 | ± | 3.34 | |||
| Sub-score: Dyspeptic (Dysmotility) symptom (2, 3, 5, 8, 11) | Placebo | 55 | 7.20 | ± | 2.83 | 5.38 | ± | 2.74 | 0.000 | 4.98 | ± | 3.27 | 0.000 | −1.82 | ± | 2.53 | 0.639 | −2.22 | ± | 2.61 | 0.706 |
| LJ88 | 52 | 7.56 | ± | 2.75 | 6.00 | ± | 2.89 | 0.000 | 5.17 | ± | 2.98 | 0.000 | −1.56 | ± | 2.55 | −2.38 | ± | 2.96 | |||
| Items | Group | n | Relief Rate (1) | |||||
|---|---|---|---|---|---|---|---|---|
| 0 W to 3 W | 0 W to 6 W | |||||||
| Not Alleviated | Alleviated | p Value (2) | Not Alleviated | Alleviated | p Value (2) | |||
| 1. Do you get heartburn? | Placebo | 55 | 32 | 23 | 0.178 | 28 | 27 | 0.049 |
| LJ88 | 52 | 23 | 29 | 16 | 36 | |||
| 2. Does your stomach get bloated? | Placebo | 55 | 36 | 19 | 0.173 | 31 | 24 | 0.248 |
| LJ88 | 52 | 27 | 25 | 23 | 29 | |||
| 3. Does your stomach ever feel heavy after meals? | Placebo | 55 | 28 | 27 | 0.076 | 19 | 36 | 0.242 |
| LJ88 | 52 | 36 | 16 | 24 | 28 | |||
| 4. Do you sometimes subconsciously rub your chest with your hand? | Placebo | 55 | 41 | 14 | 0.667 | 33 | 22 | 0.177 |
| LJ88 | 52 | 36 | 16 | 24 | 28 | |||
| 5. Do you ever feel sick after meals? | Placebo | 55 | 33 | 22 | 0.690 | 29 | 26 | 0.698 |
| LJ88 | 52 | 34 | 18 | 30 | 22 | |||
| 6. Do you get heartburn after meals? | Placebo | 55 | 27 | 28 | 0.563 | 25 | 30 | 0.557 |
| LJ88 | 52 | 29 | 23 | 20 | 32 | |||
| 7. Do you have an unusual (e.g., burning) sensation in your throat? | Placebo | 55 | 39 | 16 | 0.061 | 35 | 20 | 0.056 |
| LJ88 | 52 | 45 | 7 | 42 | 10 | |||
| 8. Do you feel full while eating meals? | Placebo | 55 | 34 | 21 | 1.000 | 36 | 19 | 0.843 |
| LJ88 | 52 | 33 | 19 | 33 | 19 | |||
| 9. Do some things get stuck when you swallow? | Placebo | 55 | 38 | 17 | 1.000 | 36 | 19 | 0.693 |
| LJ88 | 52 | 35 | 17 | 32 | 20 | |||
| 10. Do you get bitter liquid (acid) coming up into your throat? | Placebo | 55 | 40 | 15 | 0.673 | 30 | 25 | 1.000 |
| LJ88 | 52 | 35 | 17 | 28 | 24 | |||
| 11. Do you burp a lot? | Placebo | 55 | 32 | 23 | 1.000 | 32 | 23 | 0.336 |
| LJ88 | 52 | 31 | 21 | 25 | 27 | |||
| 12. Do you get heartburn if you bend over? | Placebo | 55 | 43 | 12 | 0.059 | 38 | 17 | 0.235 |
| LJ88 | 52 | 31 | 21 | 30 | 22 | |||
| Total score | Placebo | 55 | 14 | 41 | 1.000 | 7 | 48 | 1.000 |
| LJ88 | 52 | 13 | 39 | 7 | 45 | |||
| Sub-score: Acid reflux related symptom (1, 4, 6, 7, 9, 10, 12) | Placebo | 55 | 20 | 35 | 0.217 | 11 | 44 | 0.617 |
| LJ88 | 52 | 13 | 39 | 8 | 43 | |||
| Sub-score: Dyspeptic (Dysmotility) symptom (2, 3, 5, 8, 11) | Placebo | 55 | 20 | 35 | 0.844 | 14 | 41 | 0.824 |
| LJ88 | 52 | 20 | 32 | 12 | 40 | |||
| Items | Group | n | GSRS Scores | Change in GSRS Scores | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 W | 3 W | 6 W | 0–3 W | 0–6 W | |||||||||||||||||
| Mean | ± | SD | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (2) | Mean | ± | SD | p Value (2) | |||
| 1. Abdominal pain | Placebo | 55 | 1.98 | ± | 0.93 | 1.89 | ± | 0.79 | 0.382 | 1.84 | ± | 0.92 | 0.254 | −0.09 | ± | 0.80 | 0.728 | −0.15 | ± | 0.91 | 0.260 |
| LJ88 | 52 | 2.12 | ± | 0.92 | 1.96 | ± | 0.86 | 0.166 | 1.81 | ± | 0.77 | 0.029 | −0.15 | ± | 0.83 | −0.31 | ± | 0.94 | |||
| 2. Heartburn | Placebo | 55 | 2.24 | ± | 1.12 | 1.96 | ± | 0.82 | 0.024 | 1.58 | ± | 0.83 | 0.000 | −0.27 | ± | 0.87 | 0.777 | −0.65 | ± | 1.06 | 0.778 |
| LJ88 | 52 | 2.37 | ± | 0.89 | 2.06 | ± | 0.96 | 0.010 | 1.73 | ± | 0.74 | 0.000 | −0.31 | ± | 0.81 | −0.63 | ± | 0.82 | |||
| 3. Acid regurgitation | Placebo | 55 | 2.11 | ± | 1.05 | 1.87 | ± | 0.86 | 0.045 | 1.67 | ± | 0.86 | 0.003 | −0.24 | ± | 0.86 | 0.723 | −0.44 | ± | 1.03 | 0.857 |
| LJ88 | 52 | 2.00 | ± | 0.84 | 1.77 | ± | 0.81 | 0.037 | 1.63 | ± | 0.71 | 0.001 | −0.23 | ± | 0.76 | −0.37 | ± | 0.71 | |||
| 4. Sucking sensations in the epigastrium | Placebo | 55 | 2.13 | ± | 1.06 | 1.96 | ± | 1.00 | 0.112 | 1.82 | ± | 1.00 | 0.012 | −0.16 | ± | 0.76 | 0.784 | −0.31 | ± | 0.86 | 0.554 |
| LJ88 | 52 | 2.15 | ± | 1.06 | 1.98 | ± | 0.98 | 0.130 | 1.71 | ± | 0.78 | 0.002 | −0.17 | ± | 0.81 | −0.44 | ± | 0.94 | |||
| 5. Nausea and vomiting | Placebo | 55 | 1.58 | ± | 0.69 | 1.42 | ± | 0.79 | 0.044 | 1.31 | ± | 0.50 | 0.005 | −0.16 | ± | 0.83 | 0.029 | −0.27 | ± | 0.68 | 0.081 |
| LJ88 | 52 | 1.42 | ± | 0.80 | 1.50 | ± | 0.75 | 0.475 | 1.37 | ± | 0.60 | 0.826 | 0.08 | ± | 0.88 | −0.06 | ± | 0.85 | |||
| 6. Borborygmus | Placebo | 55 | 2.40 | ± | 1.18 | 2.40 | ± | 1.23 | 0.973 | 2.33 | ± | 1.28 | 0.442 | 0.00 | ± | 1.11 | 0.801 | −0.07 | ± | 0.90 | 0.493 |
| LJ88 | 52 | 2.42 | ± | 1.07 | 2.44 | ± | 1.23 | 0.769 | 2.15 | ± | 1.18 | 0.059 | 0.02 | ± | 0.90 | −0.27 | ± | 0.95 | |||
| 7. Abdominal distension | Placebo | 55 | 2.42 | ± | 1.08 | 2.16 | ± | 1.12 | 0.105 | 2.07 | ± | 1.02 | 0.021 | −0.25 | ± | 1.13 | 0.896 | −0.35 | ± | 1.04 | 0.256 |
| LJ88 | 52 | 2.65 | ± | 1.08 | 2.42 | ± | 1.11 | 0.128 | 2.10 | ± | 1.01 | 0.000 | −0.23 | ± | 1.06 | −0.56 | ± | 0.98 | |||
| 8. Eructation | Placebo | 55 | 2.36 | ± | 1.25 | 2.13 | ± | 1.06 | 0.057 | 2.00 | ± | 1.12 | 0.009 | −0.24 | ± | 0.90 | 0.891 | −0.36 | ± | 0.97 | 0.736 |
| LJ88 | 52 | 2.33 | ± | 1.06 | 2.17 | ± | 0.98 | 0.208 | 1.98 | ± | 0.92 | 0.005 | −0.15 | ± | 0.85 | −0.35 | ± | 0.84 | |||
| 9. Increased flatus | Placebo | 55 | 2.76 | ± | 1.14 | 2.75 | ± | 1.28 | 0.990 | 2.53 | ± | 1.23 | 0.082 | −0.02 | ± | 0.97 | 0.957 | −0.24 | ± | 1.05 | 0.745 |
| LJ88 | 52 | 3.02 | ± | 1.09 | 2.94 | ± | 1.21 | 0.720 | 2.69 | ± | 1.29 | 0.064 | −0.08 | ± | 1.01 | −0.33 | ± | 1.15 | |||
| 10 Decreased passage of stools | Placebo | 55 | 2.00 | ± | 1.07 | 2.04 | ± | 1.14 | 0.637 | 1.85 | ± | 1.01 | 0.226 | 0.04 | ± | 1.12 | 0.934 | −0.15 | ± | 0.87 | 0.459 |
| LJ88 | 52 | 2.13 | ± | 1.12 | 2.13 | ± | 1.09 | 0.906 | 1.90 | ± | 1.09 | 0.070 | 0.00 | ± | 0.97 | −0.23 | ± | 0.83 | |||
| 11. Increased passage of stools | Placebo | 55 | 1.67 | ± | 0.88 | 1.49 | ± | 0.77 | 0.080 | 1.62 | ± | 0.91 | 0.590 | −0.18 | ± | 0.75 | 0.436 | −0.05 | ± | 0.91 | 0.339 |
| LJ88 | 52 | 1.58 | ± | 0.89 | 1.46 | ± | 0.78 | 0.351 | 1.38 | ± | 0.87 | 0.151 | −0.12 | ± | 0.83 | −0.19 | ± | 0.91 | |||
| 12. Loose stools | Placebo | 55 | 1.73 | ± | 0.93 | 1.67 | ± | 0.88 | 0.665 | 1.73 | ± | 0.95 | 0.944 | −0.05 | ± | 0.80 | 0.663 | 0.00 | ± | 1.00 | 0.099 |
| LJ88 | 52 | 1.71 | ± | 0.91 | 1.69 | ± | 1.02 | 0.983 | 1.38 | ± | 0.84 | 0.006 | −0.02 | ± | 0.80 | −0.33 | ± | 0.81 | |||
| 13. Hard stools | Placebo | 55 | 1.96 | ± | 1.22 | 1.87 | ± | 1.02 | 0.649 | 1.75 | ± | 0.99 | 0.162 | −0.09 | ± | 1.09 | 0.883 | −0.22 | ± | 1.05 | 0.970 |
| LJ88 | 52 | 1.87 | ± | 0.84 | 1.87 | ± | 1.16 | 0.927 | 1.79 | ± | 1.16 | 0.321 | 0.00 | ± | 0.93 | −0.08 | ± | 0.90 | |||
| 14. Urgent need for defecation | Placebo | 55 | 2.00 | ± | 1.00 | 1.82 | ± | 1.06 | 0.154 | 1.78 | ± | 1.10 | 0.067 | −0.18 | ± | 1.00 | 0.604 | −0.22 | ± | 0.96 | 0.488 |
| LJ88 | 52 | 1.92 | ± | 1.13 | 1.79 | ± | 1.09 | 0.234 | 1.77 | ± | 1.04 | 0.198 | −0.13 | ± | 0.91 | −0.15 | ± | 0.83 | |||
| 15. Feeling of incomplete evacuation | Placebo | 55 | 2.60 | ± | 1.37 | 2.44 | ± | 1.33 | 0.404 | 2.45 | ± | 1.21 | 0.277 | −0.16 | ± | 1.13 | 0.720 | −0.15 | ± | 0.95 | 0.603 |
| LJ88 | 52 | 2.48 | ± | 1.26 | 2.44 | ± | 1.19 | 0.719 | 2.17 | ± | 1.12 | 0.043 | −0.04 | ± | 1.14 | −0.31 | ± | 1.06 | |||
| Total score | Placebo | 55 | 31.95 | ± | 9.18 | 29.87 | ± | 8.41 | 0.029 | 28.33 | ± | 9.33 | 0.001 | −2.07 | ± | 6.68 | 0.699 | −3.62 | ± | 7.52 | 0.422 |
| LJ88 | 52 | 32.17 | ± | 8.60 | 30.63 | ± | 9.62 | 0.149 | 27.58 | ± | 8.31 | 0.000 | −1.54 | ± | 6.64 | −4.60 | ± | 6.93 | |||
| Items | Group | n | Relief Rate (1) | |||||
|---|---|---|---|---|---|---|---|---|
| 0 W to 3 W | 0 W to 6 W | |||||||
| Not Alleviated | Alleviated | p Value (2) | Not Alleviated | Alleviated | p Value (2) | |||
| 1. Abdominal pain | Placebo | 55 | 41 | 14 | 1.000 | 40 | 15 | 0.530 |
| LJ88 | 52 | 38 | 14 | 34 | 18 | |||
| 2. Heartburn | Placebo | 55 | 33 | 22 | 1.000 | 28 | 27 | 0.563 |
| LJ88 | 52 | 32 | 20 | 23 | 29 | |||
| 3. Acid regurgitation | Placebo | 55 | 40 | 15 | 1.000 | 32 | 23 | 0.844 |
| LJ88 | 52 | 37 | 15 | 32 | 20 | |||
| 4. Sucking sensations in the epigastrium | Placebo | 55 | 40 | 15 | 0.673 | 35 | 20 | 0.558 |
| LJ88 | 52 | 35 | 17 | 30 | 22 | |||
| 5. Nausea and vomiting | Placebo | 55 | 40 | 15 | 0.162 | 39 | 16 | 0.266 |
| LJ88 | 52 | 44 | 8 | 42 | 10 | |||
| 6. Borborygmus | Placebo | 55 | 40 | 15 | 0.367 | 37 | 18 | 0.839 |
| LJ88 | 52 | 42 | 10 | 36 | 16 | |||
| 7. Abdominal distension | Placebo | 55 | 33 | 22 | 1.000 | 32 | 23 | 0.336 |
| LJ88 | 52 | 31 | 21 | 25 | 27 | |||
| 8. Eructation | Placebo | 55 | 38 | 17 | 0.836 | 35 | 20 | 0.436 |
| LJ88 | 52 | 37 | 15 | 29 | 23 | |||
| 9. Increased flatus | Placebo | 55 | 40 | 15 | 1.000 | 34 | 21 | 0.697 |
| LJ88 | 52 | 38 | 14 | 30 | 22 | |||
| 10 Decreased passage of stools | Placebo | 55 | 43 | 12 | 1.000 | 38 | 17 | 0.837 |
| LJ88 | 52 | 41 | 11 | 34 | 18 | |||
| 11. Increased passage of stools | Placebo | 55 | 41 | 14 | 0.824 | 43 | 12 | 0.653 |
| LJ88 | 52 | 40 | 12 | 38 | 14 | |||
| 12. Loose stools | Placebo | 55 | 43 | 12 | 0.813 | 42 | 13 | 0.390 |
| LJ88 | 52 | 42 | 10 | 35 | 17 | |||
| 13. Hard stools | Placebo | 55 | 43 | 12 | 0.820 | 38 | 17 | 1.000 |
| LJ88 | 52 | 39 | 13 | 36 | 16 | |||
| 14. Urgent need for defecation | Placebo | 55 | 35 | 20 | 0.217 | 33 | 22 | 0.219 |
| LJ88 | 52 | 39 | 13 | 38 | 14 | |||
| 15. Feeling of incomplete evacuation | Placebo | 55 | 37 | 18 | 0.839 | 37 | 18 | 0.690 |
| LJ88 | 52 | 36 | 16 | 33 | 19 | |||
| Total score | Placebo | 55 | 24 | 31 | 0.700 | 19 | 36 | 0.300 |
| LJ88 | 52 | 25 | 27 | 13 | 39 | |||
| Group | n | Stomach State Questionnaire (1) (Score) | Stomach State Questionnaire (1) (Relief Rate) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3 W | 6 W | 3 W | 6 W | ||||||||||||
| Mean | ± | SD | p Value (2) | Mean | ± | SD | p Value (2) | Not Alleviated | Alleviated | p Value (3) | Not Alleviated | Alleviated | p Value (3) | ||
| Placebo | 55 | 2.44 | ± | 0.54 | 0.816 | 2.38 | ± | 0.68 | 0.939 | 25 | 30 | 0.846 | 25 | 30 | 1.000 |
| LJ88 | 52 | 2.42 | ± | 0.57 | 2.40 | ± | 0.63 | 22 | 30 | 23 | 29 | ||||
| Group | Gastrin Concentration (pmoles/L) | Change in Gastrin Concentration n | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 0 W | n | 6 W | n | 0–6 W | |||||||||
| Mean | ± | SD | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (2) | ||||
| Placebo | 55 | 20.3 | ± | 4.9 | 55 | 21.4 | ± | 4.3 | 0.099 | 55 | 1.2 | ± | 5.2 | 0.311 |
| LJ88 | 52 | 27.7 | ± | 34.3 | 52 | 26.4 | ± | 27.1 | 0.824 | 52 | −1.2 | ± | 9.3 | |
| Items | Group | n | POMS-2 Scores | Change in POMS-2 Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 W | 6 W | 0–6 W | |||||||||||
| Mean | ± | SD | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (2) | |||
| Anger-hostility | Placebo | 55 | 47.64 | ± | 9.08 | 47.13 | ± | 8.10 | 0.492 | −0.51 | ± | 5.45 | 0.906 |
| LJ88 | 52 | 46.35 | ± | 8.07 | 45.96 | ± | 8.83 | 0.614 | −0.38 | ± | 5.47 | ||
| Confusion-bewilderment | Placebo | 55 | 49.36 | ± | 9.33 | 49.38 | ± | 9.80 | 0.983 | 0.02 | ± | 6.14 | 0.349 |
| LJ88 | 52 | 47.77 | ± | 8.51 | 46.71 | ± | 7.35 | 0.184 | −1.06 | ± | 5.67 | ||
| Depression-dejection | Placebo | 55 | 48.67 | ± | 8.49 | 49.20 | ± | 9.40 | 0.583 | 0.53 | ± | 7.07 | 0.260 |
| LJ88 | 52 | 46.04 | ± | 6.53 | 45.29 | ± | 4.79 | 0.218 | −0.75 | ± | 4.34 | ||
| Fatigue-inertia | Placebo | 55 | 47.69 | ± | 8.99 | 47.84 | ± | 10.26 | 0.870 | 0.15 | ± | 6.54 | 0.663 |
| LJ88 | 52 | 46.42 | ± | 8.41 | 46.06 | ± | 8.17 | 0.633 | −0.37 | ± | 5.48 | ||
| Tension-anxiety | Placebo | 55 | 49.27 | ± | 8.75 | 49.11 | ± | 10.14 | 0.861 | −0.16 | ± | 6.87 | 0.577 |
| LJ88 | 52 | 46.56 | ± | 8.82 | 47.04 | ± | 8.94 | 0.484 | 0.48 | ± | 4.91 | ||
| Vigor-activity | Placebo | 55 | 53.04 | ± | 10.25 | 51.95 | ± | 10.08 | 0.166 | −1.09 | ± | 5.77 | 0.097 |
| LJ88 | 52 | 53.48 | ± | 9.83 | 54.56 | ± | 11.55 | 0.309 | 1.08 | ± | 7.56 | ||
| Friendliness | Placebo | 55 | 55.53 | ± | 10.01 | 53.33 | ± | 10.19 | 0.007 | −2.20 | ± | 5.86 | 0.116 |
| LJ88 | 52 | 53.75 | ± | 9.13 | 53.56 | ± | 10.70 | 0.848 | −0.19 | ± | 7.21 | ||
| Total mood disturbance | Placebo | 55 | 47.80 | ± | 8.29 | 48.02 | ± | 9.64 | 0.760 | 0.22 | ± | 5.27 | 0.370 |
| LJ88 | 52 | 45.71 | ± | 7.60 | 45.08 | ± | 6.36 | 0.311 | −0.63 | ± | 4.48 | ||
| Items | Group | n | SF-36v2 Scores | Change in SF-36v2 Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 W | 6 W | 0–6 W | |||||||||||
| Mean | ± | SD | Mean | ± | SD | p Value (1) | Mean | ± | SD | p Value (2) | |||
| Physical functioning | Placebo | 55 | 54.44 | ± | 4.01 | 54.38 | ± | 4.06 | 0.909 | −0.05 | ± | 3.42 | 0.225 |
| LJ88 | 52 | 53.76 | ± | 4.63 | 54.49 | ± | 3.93 | 0.106 | 0.73 | ± | 3.21 | ||
| Role physical | Placebo | 55 | 54.08 | ± | 5.24 | 53.03 | ± | 6.19 | 0.098 | −1.05 | ± | 4.62 | 0.057 |
| LJ88 | 52 | 53.98 | ± | 5.92 | 54.59 | ± | 4.38 | 0.309 | 0.61 | ± | 4.29 | ||
| Bodily Pain | Placebo | 55 | 53.39 | ± | 8.16 | 53.27 | ± | 7.61 | 0.888 | −0.12 | ± | 6.38 | 0.163 |
| LJ88 | 52 | 51.77 | ± | 8.91 | 53.67 | ± | 8.01 | 0.109 | 1.89 | ± | 8.38 | ||
| General health | Placebo | 55 | 53.85 | ± | 8.01 | 54.93 | ± | 8.47 | 0.249 | 1.07 | ± | 6.83 | 0.628 |
| LJ88 | 52 | 55.68 | ± | 8.26 | 57.36 | ± | 7.81 | 0.050 | 1.68 | ± | 6.02 | ||
| Vitality | Placebo | 55 | 50.61 | ± | 8.37 | 51.33 | ± | 8.75 | 0.389 | 0.72 | ± | 6.17 | 0.784 |
| LJ88 | 52 | 49.84 | ± | 9.17 | 50.90 | ± | 8.19 | 0.239 | 1.06 | ± | 6.39 | ||
| Social functioning | Placebo | 55 | 53.40 | ± | 6.77 | 54.22 | ± | 6.46 | 0.433 | 0.82 | ± | 7.69 | 0.350 |
| LJ88 | 52 | 53.58 | ± | 6.80 | 52.72 | ± | 10.12 | 0.563 | −0.86 | ± | 10.64 | ||
| Role emotional | Placebo | 55 | 52.41 | ± | 6.98 | 51.93 | ± | 7.90 | 0.547 | −0.47 | ± | 5.77 | 0.799 |
| LJ88 | 52 | 53.58 | ± | 7.02 | 53.44 | ± | 4.74 | 0.889 | −0.14 | ± | 7.40 | ||
| Mental health | Placebo | 55 | 53.02 | ± | 6.80 | 52.88 | ± | 8.05 | 0.859 | −0.14 | ± | 5.69 | 0.424 |
| LJ88 | 52 | 54.24 | ± | 7.26 | 55.02 | ± | 6.43 | 0.363 | 0.78 | ± | 6.13 | ||
| Physical Component Summary (three components) | Placebo | 55 | 54.17 | ± | 5.65 | 54.05 | ± | 5.49 | 0.850 | −0.11 | ± | 4.32 | 0.050 |
| LJ88 | 52 | 53.19 | ± | 6.32 | 55.10 | ± | 6.88 | 0.029 | 1.92 | ± | 6.15 | ||
| Mental Component Summary (three components) | Placebo | 55 | 51.25 | ± | 7.11 | 52.31 | ± | 7.93 | 0.169 | 1.06 | ± | 5.62 | 0.808 |
| LJ88 | 52 | 51.82 | ± | 8.26 | 53.15 | ± | 7.35 | 0.115 | 1.33 | ± | 5.98 | ||
| Role-social Component Summary (three components) | Placebo | 55 | 52.09 | ± | 5.97 | 51.26 | ± | 7.58 | 0.318 | −0.84 | ± | 6.17 | 0.622 |
| LJ88 | 52 | 52.77 | ± | 7.45 | 51.24 | ± | 7.04 | 0.184 | −1.53 | ± | 8.19 | ||
| Physical Component Summary Universal (two components) | Placebo | 55 | 54.22 | ± | 5.07 | 54.19 | ± | 4.90 | 0.958 | −0.03 | ± | 3.56 | 0.049 |
| LJ88 | 52 | 53.32 | ± | 5.65 | 54.76 | ± | 5.34 | 0.014 | 1.44 | ± | 4.07 | ||
| Mental Component Summary Universal (two components) | Placebo | 55 | 51.65 | ± | 6.93 | 51.90 | ± | 7.85 | 0.733 | 0.25 | ± | 5.40 | 0.763 |
| LJ88 | 52 | 52.91 | ± | 7.50 | 52.78 | ± | 6.21 | 0.900 | −0.13 | ± | 7.48 | ||
| Physical Component Summary Japanese (two components) | Placebo | 55 | 54.53 | ± | 5.74 | 53.75 | ± | 5.94 | 0.147 | −0.77 | ± | 3.90 | 0.182 |
| LJ88 | 52 | 54.18 | ± | 5.62 | 54.56 | ± | 4.60 | 0.586 | 0.37 | ± | 4.88 | ||
| Mental Component Summary Japanese (two components) | Placebo | 55 | 51.64 | ± | 7.00 | 52.53 | ± | 7.71 | 0.230 | 0.90 | ± | 5.47 | 0.925 |
| LJ88 | 52 | 52.23 | ± | 7.94 | 53.23 | ± | 7.14 | 0.259 | 1.00 | ± | 6.34 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komatsu, Y.; Miura, H.; Iwama, Y.; Urita, Y. Beneficial Effect of Heat-Killed Lactic Acid Bacterium Lactobacillus johnsonii No. 1088 on Temporal Gastroesophageal Reflux-Related Symptoms in Healthy Volunteers: A Randomized, Placebo-Controlled, Double-Blind, Parallel-Group Study. Nutrients 2024, 16, 1230. https://doi.org/10.3390/nu16081230
Komatsu Y, Miura H, Iwama Y, Urita Y. Beneficial Effect of Heat-Killed Lactic Acid Bacterium Lactobacillus johnsonii No. 1088 on Temporal Gastroesophageal Reflux-Related Symptoms in Healthy Volunteers: A Randomized, Placebo-Controlled, Double-Blind, Parallel-Group Study. Nutrients. 2024; 16(8):1230. https://doi.org/10.3390/nu16081230
Chicago/Turabian StyleKomatsu, Yasuhiko, Hiroyasu Miura, Yoshitaka Iwama, and Yoshihisa Urita. 2024. "Beneficial Effect of Heat-Killed Lactic Acid Bacterium Lactobacillus johnsonii No. 1088 on Temporal Gastroesophageal Reflux-Related Symptoms in Healthy Volunteers: A Randomized, Placebo-Controlled, Double-Blind, Parallel-Group Study" Nutrients 16, no. 8: 1230. https://doi.org/10.3390/nu16081230