

Association between Oral Health and Depressive Symptoms in Chinese Older Adults: The Mediating Role of Dietary Diversity
 ,
,
Abstract
:1. Introduction
2. Methods
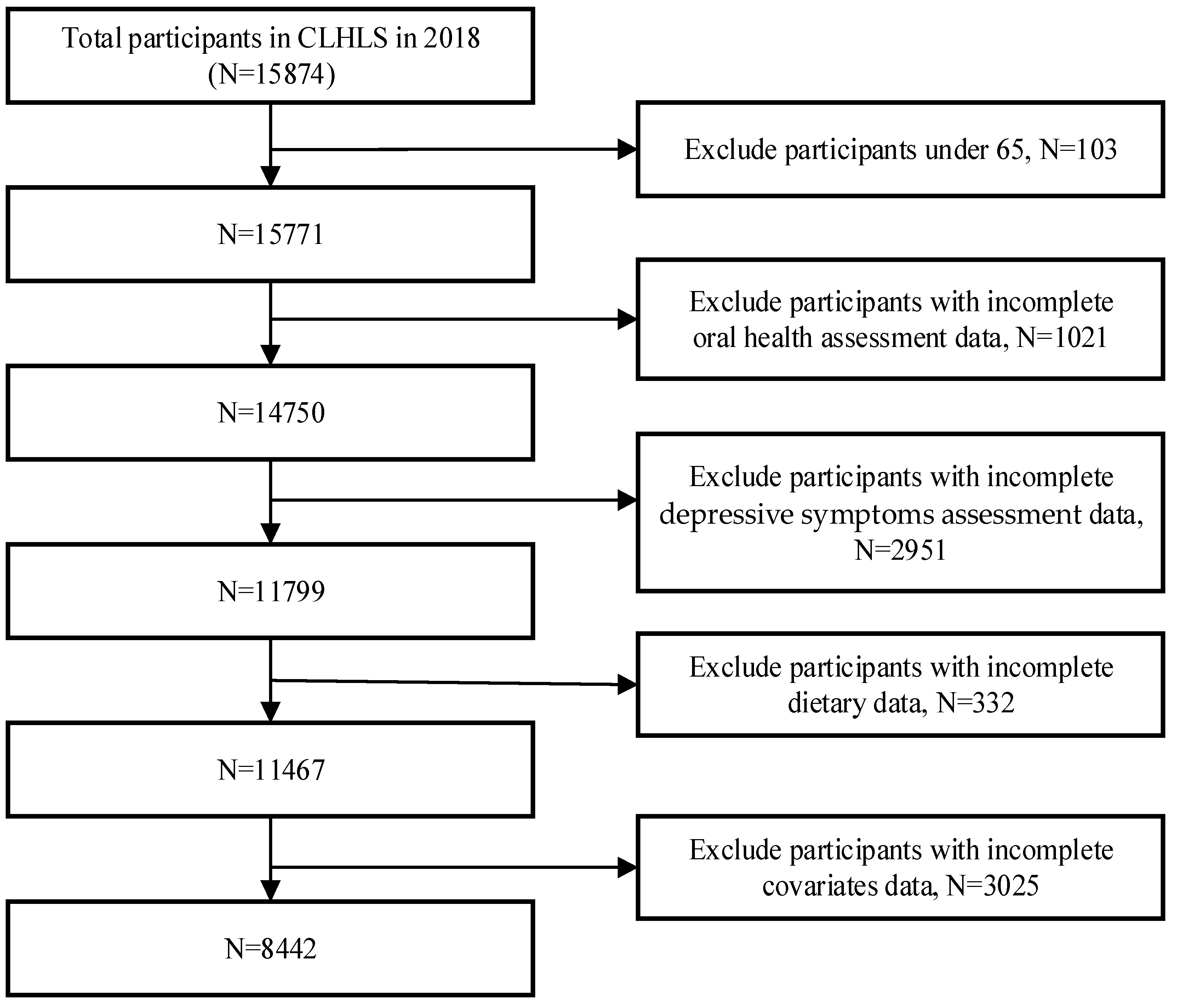
2.1. Data Sources and Sample
2.2. Measures
2.2.1. Assessment of Oral Health
2.2.2. Assessment of Dietary Diversity
2.2.3. Assessment of Depressive Symptoms
2.2.4. Assessment of Covariates Variables
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Correlation Analyses of Denture Use, Toothbrushing Frequency, DD, and Depressive Symptoms
3.3. Mediating Role of DD in the Association between Oral Health and Depressive Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Mental Disorders Collaborators. Global, Regional, and National Burden of 12 Mental Disorders in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Monahan, C.; Macdonald, J.; Lytle, A.; Apriceno, M.; Levy, S.R. COVID-19 and Ageism: How Positive and Negative Responses Impact Older Adults and Society. Am. Psychol. 2020, 75, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Erazo, M.; Fors, M.; Mullo, S.; González, P.; Viada, C. Internal Consistency of Yesavage Geriatric Depression Scale (GDS 15-Item Version) in Ecuadorian Older Adults. INQUIRY J. Health Care Organ. Provis. Financ. 2020, 57, 004695802097118. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.; Tein, J.-Y.; Zhang, M.; Yang, Y.; Wu, G. Changes in Depression among Older Adults in China: A Latent Transition Analysis. J. Affect. Disord. 2017, 209, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Shen, H.; Tan, L.; Huang, Q.; Chen, Q.; Liang, M.; He, L.; Zhou, Y. Prevalence and Factors Associated with Anxiety and Depression among Community-Dwelling Older Adults in Hunan, China: A Cross-Sectional Study. BMC Psychiatry 2023, 23, 107. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral Diseases: A Global Public Health Challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Pengpid, S. Anticipated Stigma in Chronic Illness Patients in Cambodia, Myanmar and Vietnam. Nagoya J. Med. Sci. 2016, 78, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Tannen, A.; Schütz, T.; Smoliner, C.; Dassen, T.; Lahmann, N. Care Problems and Nursing Interventions Related to Oral Intake in German Nursing Homes and Hospitals: A Descriptive Mulitcentre Study. Int. J. Nurs. Stud. 2012, 49, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Kunrath, I.; Silva, A.E.R. Oral Health and Depressive Symptoms among Older Adults: Longitudinal Study. Aging Ment. Health 2021, 25, 2265–2271. [Google Scholar] [CrossRef]
- Wright, F.A.C.; Takehara, S.; Stanaway, F.F.; Naganathan, V.; Blyth, F.M.; Hirani, V.; Le Couteur, D.G.; Handelsman, D.J.; Waite, L.M.; Seibel, M.J.; et al. Associations between Oral Health and Depressive Symptoms: Findings from the Concord Health and Ageing in Men Project. Australas. J. Ageing 2020, 39, e306–e314. [Google Scholar] [CrossRef]
- Moreira, R.d.S.; Nico, L.S.; Tomita, N.E. Spatial risk and factors associated with edentulism among elderly persons in Southeast Brazil. Cad. Saude Publica 2011, 27, 2041–2054. [Google Scholar] [CrossRef] [PubMed]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the Neglect of Global Oral Health: Time for Radical Action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Montagnese, C.; Santarpia, L.; Buonifacio, M.; Nardelli, A.; Caldara, R.A.; Silvestri, E.; Contaldo, F.; Pasanisi, F. European Food-Based Dietary Guidelines: A Comparison and Update. Nutrition 2015, 31, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Rouen, P.A.; Wallace, B.R. The 2015-2020 Dietary Guidelines: Overview and Implications for Nursing Practice. Home Healthc. Now 2017, 35, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-S.; Lay, S.; Yu, H.-N.; Shen, S.-R. Dietary Guidelines for Chinese Residents (2016): Comments and Comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef]
- Hoddinott, J.; Yohannes, Y. Dietary Diversity as a Food Security Indicator; FCND discussion papers; International Food Policy Research Institute: Washington, DC, USA, 2002. [Google Scholar]
- Leles, C.R.; Oliveira, T.M.C.; de Araújo, S.C.; Nogueira, T.E.; Schimmel, M. Individual Factors Associated with Masticatory Performance of Complete Denture Wearers: A Cross-Sectional Study. J. Oral Rehabil. 2019, 46, 903–911. [Google Scholar] [CrossRef]
- Marito, P.; Hasegawa, Y.; Tamaki, K.; Sta. Maria, M.T.; Yoshimoto, T.; Kusunoki, H.; Tsuji, S.; Wada, Y.; Ono, T.; Sawada, T.; et al. The Association of Dietary Intake, Oral Health, and Blood Pressure in Older Adults: A Cross-Sectional Observational Study. Nutrients 2022, 14, 1279. [Google Scholar] [CrossRef]
- Iwasaki, M.; Hirano, H.; Ohara, Y.; Motokawa, K. The Association of Oral Function with Dietary Intake and Nutritional Status among Older Adults: Latest Evidence from Epidemiological Studies. Jpn. Dent. Sci. Rev. 2021, 57, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Poorrezaeian, M.; Siassi, F.; Milajerdi, A.; Qorbani, M.; Karimi, J.; Sohrabi-Kabi, R.; Pak, N.; Sotoudeh, G. Depression Is Related to Dietary Diversity Score in Women: A Cross-Sectional Study from a Developing Country. Ann. Gen. Psychiatry 2017, 16, 39. [Google Scholar] [CrossRef]
- Cano-Ibáñez, N.; Serra-Majem, L.; Martín-Peláez, S.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Lassale, C.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Dietary Diversity and Depression: Cross-Sectional and Longitudinal Analyses in Spanish Adult Population with Metabolic Syndrome. Findings from PREDIMED-Plus Trial. Public Health Nutr. 2022, 26, 598–610. [Google Scholar] [CrossRef]
- Li, R.; Zong, Z.-Y.; Gu, X.-X.; Wang, D.-N.; Dong, C.; Sun, C.; Zhao, R.; Gu, Z.-F.; Gao, J.-L. Higher Dietary Diversity as a Protective Factor against Depression among Older Adults in China: A Cross-Sectional Study. Ann. Palliat. Med. 2022, 11, 1278289. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Dupre, M.E.; Sautter, J.; Zhu, H.; Liu, Y.; Yi, Z. Frailty and Mortality among Chinese at Advanced Ages. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64, 279–289. [Google Scholar] [CrossRef]
- Aihemaitijiang, S.; Zhang, L.; Ye, C.; Halimulati, M.; Huang, X.; Wang, R.; Zhang, Z. Long-Term High Dietary Diversity Maintains Good Physical Function in Chinese Elderly: A Cohort Study Based on CLHLS from 2011 to 2018. Nutrients 2022, 14, 1730. [Google Scholar] [CrossRef] [PubMed]
- Walls, A.W.G.; Steele, J.G. The Relationship between Oral Health and Nutrition in Older People. Mech. Ageing Dev. 2004, 125, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Mui, A.C. Factorial Validity of the Center for Epidemiologic Studies Depression Scale Short Form in Older Population in China. Int. Psychogeriatr. 2013, 26, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for Depression in Well Older Adults: Evaluation of a Short Form of the CES-D. Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Sun, H. Association of Unmet Long-Term Care Needs with Depression and Anxiety among Older Adults in Urban and Rural China. Geriatr. Nurs. 2023, 49, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Opio, J.; Wynne, K.; Attia, J.; Oldmeadow, C.; Hancock, S.; Kelly, B.; Inder, K.; McEvoy, M. Metabolic Health, Overweight or Obesity, and Depressive Symptoms among Older Australian Adults. Nutrients 2024, 16, 928. [Google Scholar] [CrossRef] [PubMed]
- Qi, R.; Sheng, B.; Zhou, L.; Chen, Y.; Sun, L.; Zhang, X. Association of Plant-Based Diet Indices and Abdominal Obesity with Mental Disorders among Older Chinese Adults. Nutrients 2023, 15, 2721. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S. No Mental Health without Oral Health. Can. J. Psychiatry 2016, 61, 277–282. [Google Scholar] [CrossRef]
- Kotronia, E.; Wannamethee, S.G.; Papacosta, A.O.; Whincup, P.H.; Lennon, L.T.; Visser, M.; Kapila, Y.L.; Weyant, R.J.; Ramsay, S.E. Poor Oral Health and Inflammatory, Hemostatic, and Cardiac Biomarkers in Older Age: Results From Two Studies in the UK and USA. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; de Mello, A.L.F.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral Health in the Elderly Patient and Its Impact on General Well-Being: A Nonsystematic Review. Clin. Interv. Aging 2015, 10, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Bk, S. Oral Health Problems among Geriatric Population and Its Implication on General Health: A Cross-sectional Survey. J. Dent. Res. Rev. 2017, 4, 13–16. [Google Scholar] [CrossRef]
- Davis, D.M.; Fiske, J.; Scott, B.; Radford, D.R. The Emotional Effects of Tooth Loss in a Group of Partially Dentate People: A Quantitative Study. Eur. J. Prosthodont. Restor. Dent. 2001, 9, 53–57. [Google Scholar] [PubMed]
- Skośkiewicz-Malinowska, K.; Malicka, B.; Ziętek, M.; Kaczmarek, U. Oral Health Condition and Occurrence of Depression in the Elderly. Medicine 2018, 97, e12490. [Google Scholar] [CrossRef] [PubMed]
- Manzon, L.; Vozza, I.; Poli, O. Bite Force in Elderly with Full Natural Dentition and Different Rehabilitation Prosthesis. Int. J. Environ. Res. Public Health 2021, 18, 1424. [Google Scholar] [CrossRef]
- Sharma, P.; Gupta, N.; Sharma, C.; Jaswal, R. A Review on Geriatric Oral Health: Nutritional Pattern and Dynamics. Int. J. Community Dent. 2021, 9, 29. [Google Scholar] [CrossRef]
- Emami, E.; De Souza, R.F.; Kabawat, M.; Feine, J.S. The Impact of Edentulism on Oral and General Health. Int. J. Dent. 2013, 2013, 498305. [Google Scholar] [CrossRef]
- Zelig, R.; Jones, V.M.; Touger-Decker, R.; Hoskin, E.R.; Singer, S.R.; Byham-Gray, L.; Radler, D.R.; Rothpletz-Puglia, P. The Eating Experience: Adaptive and Maladaptive Strategies of Older Adults with Tooth Loss. JDR Clin. Trans. Res. 2019, 4, 217–228. [Google Scholar] [CrossRef]
- Kotronia, E.; Brown, H.; Papacosta, A.O.; Lennon, L.T.; Weyant, R.J.; Whincup, P.H.; Wannamethee, S.G.; Ramsay, S.E. Poor Oral Health and the Association with Diet Quality and Intake in Older People in Two Studies in the UK and USA. Br. J. Nutr. 2021, 126, 118–130. [Google Scholar] [CrossRef]
- Saletti, A.; Lindgren, E.Y.; Johansson, L.; Cederholm, T. Nutritional Status According to Mini Nutritional Assessment in an Institutionalized Elderly Population in Sweden. Gerontology 2000, 46, 139–145. [Google Scholar] [CrossRef]
- Cichero, J.A.Y. Age-Related Changes to Eating and Swallowing Impact Frailty: Aspiration, Choking Risk, Modified Food Texture and Autonomy of Choice. Geriatrics 2018, 3, 69. [Google Scholar] [CrossRef]
- Beezhold, B.L.; Johnston, C.S.; Daigle, D.R. Vegetarian Diets Are Associated with Healthy Mood States: A Cross-Sectional Study in Seventh Day Adventist Adults. Nutr. J. 2010, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Skarupski, K.A.; Tangney, C.; Li, H.; Ouyang, B.; Evans, D.A.; Morris, M.C. Longitudinal Association of Vitamin B-6, Folate, and Vitamin B-12 with Depressive Symptoms among Older Adults over Time. Am. J. Clin. Nutr. 2010, 92, 330–335. [Google Scholar] [CrossRef]
- Gilbody, S.; Lightfoot, T.; Sheldon, T. Is Low Folate a Risk Factor for Depression? A Meta-Analysis and Exploration of Heterogeneity. J. Epidemiol. Community Health 2007, 61, 631–637. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet Quality and Major Chronic Disease Risk in Men and Women: Moving toward Improved Dietary Guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Karimbeiki, R.; Pourmasoumi, M.; Feizi, A.; Abbasi, B.; Hadi, A.; Rafie, N.; Safavi, S.M. Higher Dietary Diversity Score Is Associated with Obesity: A Case-Control Study. Public Health 2018, 157, 127–134. [Google Scholar] [CrossRef]
- Liu, C.-K.; Huang, Y.-C.; Lo, Y.-T.C.; Wahlqvist, M.L.; Lee, M.-S. Dietary Diversity Offsets the Adverse Mortality Risk among Older Indigenous Taiwanese. Asia Pac. J. Clin. Nutr. 2019, 28, 593–600. [Google Scholar] [CrossRef]
- Folayan, M.O.; Ibigbami, O.I.; Oloniniyi, I.O.; Oginni, O.; Aloba, O. Associations between Psychological Wellbeing, Depression, General Anxiety, Perceived Social Support, Tooth Brushing Frequency and Oral Ulcers among Adults Resident in Nigeria during the First Wave of the COVID-19 Pandemic. BMC Oral Health 2021, 21, 520. [Google Scholar] [CrossRef]
- Okoro, C.A.; Strine, T.W.; Eke, P.I.; Dhingra, S.S.; Balluz, L.S. The Association between Depression and Anxiety and Use of Oral Health Services and Tooth Loss. Community Dent. Oral Epidemiol. 2012, 40, 134–144. [Google Scholar] [CrossRef]
- Cademartori, M.G.; Gastal, M.T.; Nascimento, G.G.; Demarco, F.F.; Corrêa, M.B. Is Depression Associated with Oral Health Outcomes in Adults and Elders? A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2018, 22, 2685–2702. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, J.S.; Jun, M.S.; Yun, H.K. The Relationship between Objective Oral Health Conditions and Subjective Oral Health Perception of the Elderly in Gimcheon. J. Korean Soc. Dent. Hyg. 2015, 15, 417–424. [Google Scholar] [CrossRef]
- Ramon, T.; Grinshpoon, A.; Zusman, S.P.; Weizman, A. Oral Health and Treatment Needs of Institutionalized Chronic Psychiatric Patients in Israel. Eur. Psychiatry 2003, 18, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Chauncey, H.H.; Muench, M.E.; Kapur, K.K.; Wayler, A.H. The Effect of the Loss of Teeth on Diet and Nutrition. Int. Dent. J. 1984, 34, 98–104. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Variables | All (N = 8442) | Depressive Symptoms (N = 3729) | t/F/H Value | p-Value |
|---|---|---|---|---|
| Sex | −9.546 | <0.001 | ||
| Male | 3878 (45.9%) | 1532 (39.5%) | ||
| Female | 4564 (54.1%) | 2197 (48.1%) | ||
| Age | 30.488 | <0.001 | ||
| 65–74 | 2298 (27.2%) | 853 (37.1%) | ||
| 75–84 | 2476 (29.3%) | 1095 (44.2%) | ||
| 85–94 | 2082 (24.7%) | 977 (46.9%) | ||
| ≥95 | 1586 (18.8%) | 804 (50.6%) | ||
| Residence | −5.724 | <0.001 | ||
| Urban areas | 2194 (26.0%) | 832 (37.9%) | ||
| Rural areas | 6248 (74.0%) | 2897 (46.3%) | ||
| Marital Status | −11.341 | <0.001 | ||
| With spouse | 4015 (47.6%) | 1535 (38.25%) | ||
| No spouse | 4427 (52.4%) | 2194 (49.5%) | ||
| Living arrangement | 42.277 | <0.001 | ||
| Living with family | 6761 (80.1%) | 2583 (42.1%) | ||
| Living alone | 1396 (16.5%) | 721 (51.6%) | ||
| Nursing home | 285 (3.4%) | 155 (54.3%) | ||
| Education | 103.360 | <0.001 | ||
| No education experience | 3654 (43.3%) | 1882 (51.5%) | ||
| Primary school | 2931 (34.7%) | 1191 (40.6%) | ||
| Junior high school and above | 1857 (22.0%) | 656 (35.3%) | ||
| Self-assessment of economic status | 207.325 | <0.001 | ||
| Poorer | 811 (9.6%) | 537 (66.2%) | ||
| General | 5918 (70.1%) | 2662 (44.9%) | ||
| wealthier | 1713 (20.3%) | 530 (30.9%) | ||
| Smoking | 31.697 | <0.001 | ||
| No smoking | 5775 (68.4%) | 2713 (46.9%) | ||
| Past smoking | 1316 (15.6%) | 480 (36.4%) | ||
| Now smoking | 1351 (16.0%) | 536 (39.6%) | ||
| Drinking | 86.592 | <0.001 | ||
| No drinking | 6129 (72.6%) | 2858 (46.6%) | ||
| Past drinking | 1020 (12.1%) | 417 (40.8%) | ||
| Drinking now | 1293 (15.3%) | 454 (39.1%) | ||
| Exercise | −16.117 | <0.001 | ||
| No | 5432 (64.3%) | 2699 (49.6%) | ||
| Yes | 3010 (35.7%) | 1030 (34.2%) | ||
| Serious illness | −7.160 | <0.001 | ||
| No | 6353 (75.3%) | 2707 (42.6%) | ||
| Yes | 2089 (24.7%) | 1022 (48.9%) | ||
| ADL | −11.114 | <0.001 | ||
| No difficulty | 6916 (81.9%) | 2911 (42.0%) | ||
| Difficulty | 1526 (18.1%) | 818 (53.6%) | ||
| Denture use | −6.893 | <0.001 | ||
| Yes | 3443 (40.8%) | 1376 (39.9%) | ||
| No | 4999 (59.2%) | 2353 (47.0%) | ||
| Toothbrushing frequency | 127.890 | <0.001 | ||
| Hardly | 1364 (16.2%) | 712 (52.1%) | ||
| Occasional | 991 (11.7%) | 523 (52.7%) | ||
| Once a day | 3537 (41.9%) | 1493 (42.2%) | ||
| Twice a day | 2033 (24.1%) | 831 (40.8%) | ||
| Three or more times a day | 517 (6.1%) | 170 (32.8%) |
| Variables | Denture Use | Toothbrushing Frequency | DD | Depressive Symptoms |
|---|---|---|---|---|
| Denture use | 1.000 | |||
| Toothbrushing frequency | 0.251 ** | 1.000 | ||
| DD | 0.113 ** | 0.268 ** | 1.000 | |
| Depressive symptoms | −0.077 ** | −0.115 ** | −0.186 ** | 1.000 |
| Pathway 1 | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Dependent Variable | Depressive Symptoms | DD | Depressive Symptoms | |||
| Indicators | β | t | β | t | β | t |
| Denture use | −0.341 | −4.094 *** | 0.307 | 5.785 *** | −0.294 | −3.540 *** |
| DD | −0.153 | −8.989 *** | ||||
| Sex | 0.085 | 0.818 | 0.037 | 0.562 | 0.091 | 0.877 |
| Age | 0.027 | 0.534 | −0.001 | −0.034 | 0.027 | 0.533 |
| Residence | 0.081 | 0.780 | −1.613 | −24.384 *** | −0.166 | −1.550 |
| Marital status | 0.206 | 1.937 * | −0.112 | −1.657 * | 0.189 | 1.783 * |
| Living arrangement | 0.593 | 6.752 *** | −0.169 | −3.022 *** | 0.567 | 6.485 *** |
| Education | −0.202 | −3.049 *** | 0.518 | 12.256 *** | −0.123 | −1.846 * |
| Economic status | 1.486 | 19.040 *** | −0.735 | −14.786 *** | 1.373 | 17.457 *** |
| Smoking | −0.170 | −2.622 *** | 0.052 | 1.252 | −0.162 | −2.512 ** |
| Drinking | −0.257 | −4.195 *** | 0.225 | 5.768 *** | −0.223 | −3.643 *** |
| Exercise | −0.905 | −10.064 *** | 0.430 | 7.499 *** | −0.840 | −9.347 *** |
| Serious illness | 0.636 | 6.728 *** | −0.130 | −2.156 ** | 0.616 | 6.547 *** |
| ADL | 0.745 | 6.314 *** | 0.181 | 2.409 ** | 0.773 | 6.577 *** |
| R-side | 0.111 | 0.209 | 0.119 | |||
| F | 80.865 *** | 171.187 *** | 81.571 *** | |||
| Pathway 2 | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Dependent Variable | Depressive Symptoms | DD | Depressive Symptoms | |||
| Indicators | β | t | β | t | β | t |
| Toothbrushing frequency | −0.124 | −3.041 ** | 0.270 | 10.474 *** | −0.082 | −2.022 * |
| DD | −0.153 | −8.937 *** | ||||
| Sex | 0.105 | 0.999 | −0.014 | −0.217 | 0.103 | 0.983 |
| Age | 0.010 | 0.197 | 0.036 | 1.115 | 0.015 | 0.307 |
| Residence | 0.029 | 0.275 | −1.474 | −21.844 *** | −0.196 | −1.800 * |
| Marital status | 0.208 | 1.954 * | −0.099 | −1.470 | 0.193 | 1.820 * |
| Living arrangement | 0.594 | 6.767 *** | −0.184 | −3.302 *** | 0.566 | 6.473 *** |
| Education | −0.178 | −2.649 *** | 0.458 | 10.764 *** | −0.108 | −1.603 |
| Economic status | 1.492 | 19.115 *** | −0.717 | −14.490 *** | 1.383 | 17.576 *** |
| Smoking | −0.178 | −2.741 *** | 0.064 | 1.556 | −0.168 | −2.602 *** |
| Drinking | −0.253 | −4.128 *** | 0.220 | 5.647 *** | −0.220 | −3.591 *** |
| Exercise | 0.903 | 10.012 *** | −0.395 | −6.895 *** | 0.843 | 9.361 *** |
| Serious illness | 0.627 | 6.635 *** | −0.133 | −2.210 ** | 0.607 | 6.449 *** |
| ADL | 0.713 | 6.024 *** | 0.244 | 3.250 *** | 0.751 | 6.364 *** |
| R-side | 0.110 | 0.216 | 0.119 | |||
| F | 80.865 *** | 178.571 *** | 80.888 *** | |||
| Category | Effect Value | Bootstrap SE | LLCI | ULCI | Effect Ratio |
|---|---|---|---|---|---|
| Denture use → total effect of depressive symptoms | −0.341 | 0.083 | −0.505 | −0.178 | |
| Denture use → DD → depressive symptoms | −0.047 | 0.010 | −0.068 | −0.028 | 13.77% |
| Toothbrushing frequency → total effect of depressive symptoms | −0.124 | 0.041 | −0.203 | −0.044 | |
| Toothbrushing frequency → DD → Depressive symptoms | −0.041 | 0.006 | −0.054 | −0.030 | 33.39% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lou, J.; Wang, J.; Fu, Y.; Huang, D.; Liu, M.; Zhao, R.; Deng, J. Association between Oral Health and Depressive Symptoms in Chinese Older Adults: The Mediating Role of Dietary Diversity. Nutrients 2024, 16, 1231. https://doi.org/10.3390/nu16081231
Lou J, Wang J, Fu Y, Huang D, Liu M, Zhao R, Deng J. Association between Oral Health and Depressive Symptoms in Chinese Older Adults: The Mediating Role of Dietary Diversity. Nutrients. 2024; 16(8):1231. https://doi.org/10.3390/nu16081231
Chicago/Turabian StyleLou, Jiaxu, Jian Wang, Yingjie Fu, Derong Huang, Mei Liu, Ruonan Zhao, and Jiahui Deng. 2024. "Association between Oral Health and Depressive Symptoms in Chinese Older Adults: The Mediating Role of Dietary Diversity" Nutrients 16, no. 8: 1231. https://doi.org/10.3390/nu16081231