
Dietary Quality Evidenced by the Healthy Eating Index and Cardiovascular Disease Risk Factors in Kuwaiti Schoolchildren

 ,
,
Abstract
:1. Introduction
2. Methods
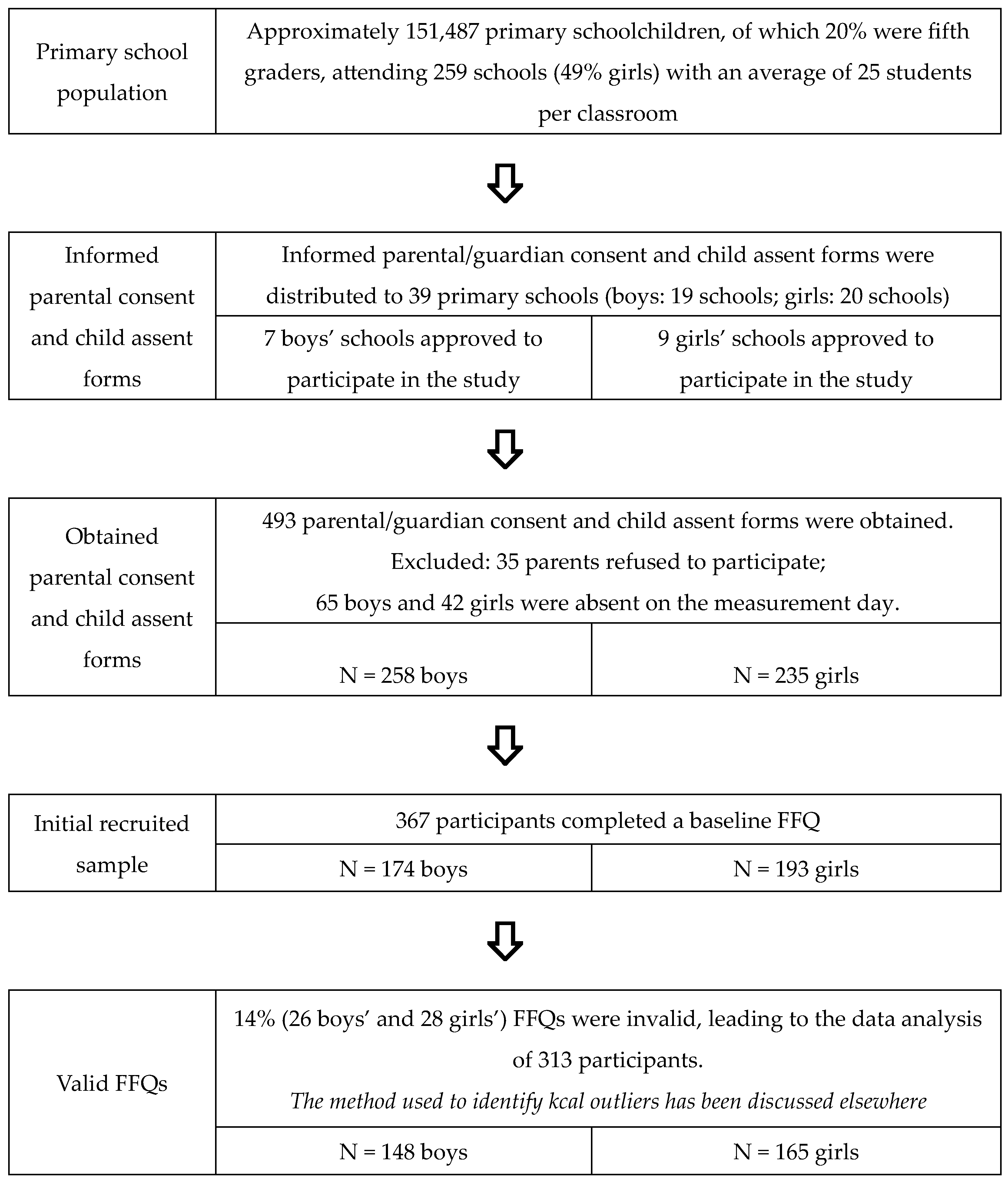
2.1. Study Design and Participants
2.2. Measurements
2.3. Dietary Indices
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malik, V.S.; Willett, W.C.; Hu, F.B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Montoye, A.H.; Pfeiffer, K.A.; Alaimo, K.; Betz, H.H.; Paek, H.J.; Carlson, J.J.; Eisenmann, J.C. Junk food consumption and screen time: Association with childhood adiposity. Am. J. Health Behav. 2013, 37, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Funtikova, A.N.; Navarro, E.; Bawaked, R.A.; Fíto, M.; Schröder, H. Impact of diet on cardiometabolic health in children and adolescents. Nutr. J. 2015, 14, 118. [Google Scholar] [CrossRef] [PubMed]
- Juhola, J.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A.; Srinivasan, S.R.; Daniels, S.R.; Davis, P.H.; Chen, W.; et al. Combined effects of child and adult elevated blood pressure on subclinical atherosclerosis: The International Childhood Cardiovascular Cohort Consortium. Circulation 2013, 128, 217–224. [Google Scholar] [CrossRef]
- Farrag, O.L. The status of child nutrition in the Gulf Arab States. J. Trop. Pediatr. 1983, 29, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Al-Farhan, A.k.; Weatherspoon, L.J.; Pfeiffer, K.A.; Li, W.; Carlson, J.J. Sex differences in the prevalence of multiple cardiovascular disease risk factors in schoolchildren: A cross-sectional study. Clin. Nutr. ESPEN 2022, 52, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Moussa MA, A.; Shaltout, A.A.; Nkansa-Dwamena, D.; Mourad, M.; Alsheikh, N.; Agha, N.; Galal, D.O. Factors associated with obesity in Kuwaiti children. Eur. J. Epidemiol. 1999, 15, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Al-Lahou, B.; Ausman, L.M.; Peñalvo, J.L.; Huggins, G.S.; Al-Hooti, S.; Al-Zenki, S.; Zhang, F.F. Dietary Patterns Associated with the Prevalence of Cardiovascular Disease Risk Factors in Kuwaiti Adults. J. Acad. Nutr. Diet. 2019, 120, 424–436. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef]
- The, N.S.; Couch, S.C.; Urbina, E.M.; Crandell, J.L.; Liese, A.D.; Dabelea, D.; Kim, G.J.; Tooze, J.A.; Lawrence, J.M.; Mayer-Davis, E.J. Body Mass Index Z-Score Modifies the Association between Added Sugar Intake and Arterial Stiffness in Youth with Type 1 Diabetes: The Search Nutrition Ancillary Study. Nutrients 2019, 11, 1752. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Diet quality as assessed by the Healthy Eating Index, the Alternate Healthy Eating Index, the Dietary Approaches to Stop Hypertension score, and health outcomes: A systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2015, 115, 780–800. [Google Scholar] [CrossRef]
- Konikowska, K.; Bombala, W.; Szuba, A.; Rozanska, D.; Regulska-Ilow, B. Metabolic Syndrome Is Associated with Low Diet Quality Assessed by the Healthy Eating Index-2015 (HEI-2015) and Low Concentrations of High-Density Lipoprotein Cholesterol. Biomedicines 2022, 10, 2487. [Google Scholar] [CrossRef]
- Hu, E.A.; Steffen, L.M.; Coresh, J.; Appel, L.J.; Rebholz, C.M. Adherence to the Healthy Eating Index-2015 and Other Dietary Patterns May Reduce Risk of Cardiovascular Disease, Cardiovascular Mortality, and All-Cause Mortality. J. Nutr. 2020, 150, 312–321. [Google Scholar] [CrossRef]
- Veugelers, P.J.; Fitzgerald, A.L.; Johnston, E. Dietary Intake and Risk Factors for Poor Diet Quality among Children in Nova Scotia. Can. J. Public Health 2005, 96, 212–216. [Google Scholar] [CrossRef]
- Camhi, S.M.; Whitney Evans, E.; Hayman, L.L.; Lichtenstein, A.H.; Must, A. Healthy eating index and metabolically healthy obesity in U.S. adolescents and adults. Prev. Med. 2015, 77, 23–27. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey. HEI-2010 Total and Component Scores for Children, Adults, and Older Adults during 2011–2012. Available online: https://fns-prod.azureedge.us/sites/default/files/media/file/HEI2010_Age_Groups_2011_2012.pdf (accessed on 7 August 2016).
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. 2020–2025 Dietary Guidelines for Americans Division of Health Promotion and Chronic Disease 2020, 9th ed.; pp. 1–149. Available online: https://www.dietaryguidelines.gov/resources/2020-2025-dietary-guidelines-online-materials (accessed on 12 September 2022).
- National Center for Health Statistics. Average Healthy Eating Index-2015 Scores for Children and Adolescents by Age Groups. National Health and Nutrition Examination Survey 2017–2018. Available online: https://www.fns.usda.gov/cnpp/hei-scores-americans (accessed on 10 December 2023).
- Zhang, Y.; Lu, C.; Li, X.; Fan, Y.; Li, J.; Liu, Y.; Yu, Y.; Zhou, L. Healthy Eating Index-2015 and Predicted 10-Year Cardiovascular Disease Risk, as Well as Heart Age. Front. Nutr. 2022, 9, 888966. [Google Scholar] [CrossRef]
- Pasdar, Y.; Hamzeh, B.; Moradi, S.; Mohammadi, E.; Cheshmeh, S.; Darbandi, M.; Faramani, R.S.; Najafi, F. Healthy eating index 2015 and major dietary patterns in relation to incident hypertension; a prospective cohort study. BMC Public Health 2022, 22, 734. [Google Scholar] [CrossRef]
- Al-Farhan, A.K.; Becker, T.B.; Petushek, E.; Weatherspoon, L.; Carlson, J.J. Reliability of the Block Kid’s Food Frequency Questionnaire translated to Arabic and adapted for Kuwaiti children. Nutrition 2021, 90, 111289. [Google Scholar] [CrossRef]
- Department of Educational Planning. Education Statistical Group 2015–2016. 2016. Available online: https://www.moe.edu.kw/pages/Statistics (accessed on 10 February 2016).
- Standard WHOCG. Length-for-Age Z-Score. WHO Library Cataloguing-in-Publication Data 2024. Available online: https://www.who.int/tools/child-growth-standards/standards/length-height-for-age (accessed on 3 June 2018).
- de Onis, M. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Alaqil, A.I.; Petushek, E.J.; Gautam, Y.R.; Pfeiffer, K.A.; Carlson, J.J. Determining independence and associations among various cardiovascular disease risk factors in 9–12 years old school-children: A cross sectional study. BMC Public Health 2022, 22, 1639. [Google Scholar] [CrossRef]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; de Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef]
- Services USDA. 2015–2020 Dietary Guidelines for Americans Division of Health Promotion and Chronic Disease 2015, 8th ed.; Government Printing Office: Washington, DC, USA, 2015.
- Kann, L.; Kinchen, S.; Shanklin, S.L.; Flint, K.H.; Hawkins, J.; Harris, W.A.; Lowry, R.; Olsen, E.O.M.; McManus, T.; Chyen, D.; et al. Youth Risk Behavior Surveillance—United States, 2013. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2014, 63, 1–68. [Google Scholar]
- Carlson, J.J.; Eisenmann, J.C.; Pfeiffer, K.A.; Jager, K.B.; Sehnert, S.T.; Yee, K.E.; Klavinski, R.A.; Feltz, D.L. (S)Partners for Heart Health: A school-based program for enhancing physical activity and nutrition to promote cardiovascular health in 5th grade students. BMC Public Health 2008, 8, 420. [Google Scholar] [CrossRef]
- Drenowatz, C.; Carlson, J.J.; Pfeiffer, K.A.; Eisenmann, J.C. Joint association of physical activity/screen time and diet on CVD risk factors in 10-year-old children. Front. Med. 2012, 6, 428–435. [Google Scholar] [CrossRef]
- Feskanich, D.; Rockett, H.R.; Colditz, G.A. Modifying the Healthy Eating Index to assess diet quality in children and adolescents. J. Am. Diet. Assoc. 2004, 104, 1375–1383. [Google Scholar] [CrossRef]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Guo, X.; Warden, B.A.; Paeratakul, S.; Bray, G.A. Healthy Eating Index and obesity. Eur. J. Clin. Nutr. 2004, 58, 1580–1586. [Google Scholar] [CrossRef]
- National Cancer Institute. The Healthy Eating Index. Division of Cancer Control & Population Sciences. 2018. Available online: https://epi.grants.cancer.gov/hei/uses.html (accessed on 5 June 2018).
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Schroeder, N.; Shimizu, M.; LaComb, R.P.; Moshfegh, A.J. Food Patterns Equivalents Intakes by Americans: What We Eat in America, NHANES 2003–2004 and 2015–2016. Food Surv. Res. Group. Diet. Data Brief 2018, 20. Available online: https://www.ncbi.nlm.nih.gov/books/NBK589289/pdf/Bookshelf_NBK589289.pdf (accessed on 3 October 2019).
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. HEI-J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Salas-Gonzalez, M.D.; Aparicio, A.; Loria-Kohen, V.; Ortega, R.M.; Lopez-Sobaler, A.M. Association of Healthy Eating Index-2015 and Dietary Approaches to Stop Hypertension Patterns with Insulin Resistance in Schoolchildren. Nutrients 2022, 14, 4232. [Google Scholar] [CrossRef]
- Thomson, J.L.; Tussing-Humphreys, L.M.; Goodman, M.H.; Landry, A.S. Diet quality in a nationally representative sample of American children by sociodemographic characteristics. Am. J. Clin. Nutr. 2019, 109, 127–138. [Google Scholar] [CrossRef]
- Thomson, J.L.; Landry, A.S.; Tussing-Humphreys, L.M.; Goodman, M.H. Diet quality of children in the United States by body mass index and sociodemographic characteristics. Obes. Sci. Pract. 2020, 6, 84–98. [Google Scholar] [CrossRef]
- Stavnsbo, M.; Resaland, G.K.; Anderssen, S.A.; Steene-Johannessen, J.; Domazet, S.L.; Skrede, T.; Sardinha, L.B.; Kriemler, S.; Ekelund, U.; Andersen, L.B.; et al. Reference values for cardiometabolic risk scores in children and adolescents: Suggesting a common standard. Atherosclerosis 2018, 278, 299–306. [Google Scholar] [CrossRef]
- Hooshmand, F.; Asghari, G.; Yuzbashian, E.; Mahdavi, M.; Mirmiran, P.; Azizi, F. Modified Healthy Eating Index and Incidence of Metabolic Syndrome in Children and Adolescents: Tehran Lipid and Glucose Study. J. Pediatr. 2018, 197, 134–139. [Google Scholar] [CrossRef]
- Ekelund, U.; Brage, S.; Froberg, K.; Harro, M.; Anderssen, S.A.; Sardinha, L.B.; Riddoch, C.; Andersen, L.B. TV viewing and physical activity are independently associated with metabolic risk in children: The European Youth Heart Study. PLoS Med. 2006, 3, e448. [Google Scholar] [CrossRef]
- World Health Organization Technical Report Series. Diet, Nutrition and the Prevention of Chronic Diseases. Report of a Joint WHO/FAO Expert Consultation. 2003. Available online: https://www.who.int/publications/i/item/924120916X (accessed on 8 April 2024).
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef]
- Jj, C.; Ka, P. (S)Partners for Heart Health: A School- and Web-Based Intervention Pilot: Effects on Nutrition, Physical Activity, Screen Time and Cardiovascular Risk Factors in 5th Grade Children. J. Community Med. Health Educ. 2015, 5, 1000376. [Google Scholar] [CrossRef]
- Eck, L.H.; Klesges, L.M.; Klesges, R.C. Precision and estimated accuracy of two short-term food frequency questionnaires compared with recalls and records. J. Clin. Epidemiol. 1995, 49, 1195–1200. [Google Scholar] [CrossRef]
- Kourlaba, G.; Panagiotakos, D.B. Dietary quality indices and human health: A review. Maturitas 2009, 62, 1–8. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Overall (n = 313) | Boys (n = 148) | Girls (n = 165) | p-Value |
|---|---|---|---|---|
| City | ||||
| Capital | 11.8% | 9.5% | 13.9% | 0.22 |
| Hawalli | 38.7% | 37.8% | 39.4% | 0.77 |
| Farwaniya | 5.8% | 6.8% | 4.8% | 0.47 |
| Mubarak Al-Kabir | 22.7% | 25.7% | 20.0% | 0.23 |
| Ahmadi | 10.5% | 3.4% | 17.0% | 0.001 |
| Jahra | 10.5% | 16.9% | 4.8% | 0.001 |
| Age (years) | 10.45 ± 0.38 | 10.44 ± 0.35 | 10.46 ± 0.40 | 0.572 |
| Height (cm) | 142.06 ± 6.62 | 141.3± 7.07 | 142.4 ± 6.12 | 0.104 |
| Weight (kg) | 44.48 ± 13.11 | 43.93 ± 14.22 | 44.98 ± 12.05 | 0.479 |
| BMI (kg/m2) | 21.74 ± 4.99 | 21.59 ± 5.32 | 21.87 ± 4.68 | 0.631 * |
| BMI Z-score | 1.42 ± 0.07 | 1.47 ± 0.11 | 1.39 ± 0.10 | 0.103 * |
| +1 Z-score | 22.8% | 18.2% | 26.8% | 0.071 |
| +2 Z-score | 42% | 43.9% | 40.2% | 0.511 |
| WC (cm) | 69.9 ± 0.78 | 69.5 ± 1.21 | 70.3 ± 1.0 | 0.466 * |
| BF% | 28.5 ± 0.57 | 27.4 ± 0.95 | 29.5 ± 0.67 | 0.468 * |
| SBP mmHg | 106.3 ± 0.69 | 103.9 ± 0.99 | 108.3 ± 0.94 | 0.058 * |
| DBP mmHg | 68.01 ± 0.55 | 65.1 ± 0.73 | 70.5 ± 0.76 | 0.001 * |
| Elevated BP | ||||
| ≥90th to <95th percentiles or 120/<80 to 129/<80 mm Hg | 16% (n = 49) | 5.2% (n = 16) | 10.7% (n = 33) | 0.029 |
| Stage 1 HTN | ||||
| 95th percentiles or 130/80 to 139/89 mmHg Stage 2 HTN | 2.9% (n = 9) | 1.3% (n = 4) | 1.6% (n = 5) | 0.881 |
| 95th + 12 mmHg or ≥140/90 mm Hg | 0.7% (n = 2) | 0.3% (n = 1) | 0.3% (n = 1) | 0.930 |
| TC (mg/dL) | 152.9 ± 2.2 | 149.5 ± 2.7 | 156 ± 3.4 | 0.837 * |
| LDL (mg/dL) | 82.6 ± 1.81 | 82.9 ± 2.66 | 82.4 ± 2.47 | 0.505 * |
| HDL (mg/dL) | 51.5 ± 0.94 | 51.6 ± 1.18 | 51.4 ± 1.45 | 0.383 * |
| None-HDL (mg/dL) | 100.7 ± 1.7 | 99.2 ± 2.4 | 102.1 ± 2.5 | 0.936 * |
| TC:HDL | 3.0 ± 0.05 | 2.9 ± 0.07 | 3.1 ± 0.08 | 0.399 * |
| Triglycerides (mg/dL) | 98.4 ± 3.2 | 90.1 ± 4.1 | 105.7 ± 4.9 | 0.029 * |
| Covariate | ||||
| MVPA (d/wk) | 2.89 ± 2.34 | 3.37 ± 2.36 | 2.47 ± 2.24 | 0.001 |
| % met MVPA | 19.3% | 24% | 15.2% | 0.054 |
| ST (h/day) | 4.72 ± 2.68 | 4.97 ± 2.56 | 4.50 ± 2.77 | 0.119 |
| % met ST ≤ 2 h/d | 17.4% | 9.6% | 24.2% | 0.001 |
| Nutrition Variable | Overall (n = 313) | Boys (n = 148) | Girls (n = 165) | p-Value | p-Value * |
|---|---|---|---|---|---|
| Food Group | |||||
| Fruits (cup) | 2.36 ± 0.080 | 2.56 ± 0.12 | 2.19 ± 0.10 | 0.020 | 0.487 |
| Vegetables (cup) | 1.81 ± 0.05 | 1.81 ± 0.08 | 1.80 ± 0.07 | 0.963 | 0.011 |
| Dairy (cup) | 1.67 ± 0.04 | 1.70 ± 0.06 | 1.65 ± 0.06 | 0.311 | 0.027 |
| Whole Grains (ounces) | 0.63 ± 0.02 | 0.68 ± 0.03 | 0.59 ± 0.02 | 0.047 | 0.785 |
| Macronutrient (g) | |||||
| Total Calories | 2460.29 ± 52.2 | 2652.59 ± 76.9 | 2287.38 ± 68.5 | 0.001 | |
| Total Fat | 92.08 ± 2.25 | 99.82 ± 3.34 | 85.14 ± 2.96 | 0.001 | 0.892 |
| Saturated Fat | 29.21 ± 0.66 | 31.3 ± 0.95 | 27.3 ± 0.91 | 0.002 | 0.306 |
| Trans-fat | 8.15 ± 0.23 | 8.82 ± 0.33 | 7.55 ± 0.33 | 0.008 | 0.653 |
| n-6 FAs | 19.12 ± 0.62 | 21 ± 0.97 | 17.4 ± 0.76 | 0.004 | 0.829 |
| n-3 FAs | 1.67 ± 0.041 | 1.82 ± 0.062 | 1.53 ± 0.053 | 0.001 | 0.377 |
| Cholesterol (mg) | 305.1 ± 8.22 | 338.3 ± 12.07 | 275.3 ± 10.73 | 0.001 | 0.029 |
| Carbohydrates | 335.7 ± 7.10 | 359.1 ± 10.64 | 314.6 ± 9.25 | 0.002 | 0.414 |
| Total Sugar | 162.6 ± 4.04 | 175.6 ± 6.38 | 150.9 ± 4.94 | 0.002 | 0.790 |
| Added Sugar (tsp) “ | 22.1 ± 0.68 | 24 ± 1.09 | 20.5 ± 0.84 | 0.012 | 0.373 |
| Total Fiber | 22.08 ± 0.55 | 23.6 ± 0.82 | 20.7 ± 0.72 | 0.010 | 0.449 |
| Fiber per 1000 kcals | 8.9 ± 0.11 | 8.8 ± 2.00 | 8.9 ± 2.00 | 0.655 | 0.418 |
| Protein | 83.2 ± 1.85 | 91.2 ± 2.74 | 76.2 ± 2.38 | 0.001 | 0.028 |
| Micronutrient | |||||
| Calcium (mg) | 964.04 ± 22.08 | 1008.8 ± 30.34 | 923.8 ± 31.58 | 0.054 | 0.031 |
| Magnesium (mg) | 332.8 ± 8,02 | 357.9 ± 11.97 | 310.1 ± 10.51 | 0.003 | 0.527 |
| Potassium (mg) | 3010.8 ± 66.7 | 3201.3 ± 108.41 | 2840.0 ± 97.15 | 0.007 | 0.369 |
| Sodium (mg) | 3664.2 ± 79.5 | 3920.3 ± 113.6 | 3434.5 ± 108.4 | 0.002 | 0.695 |
| Vitamin D (IU) ^ | 140.7 ± 4.29 | 145.8 ± 6.28 | 136.2 ± 5.87 | 0.267 | 0.556 |
| Component | Maximum Points | Standard for Maximum Score | Standard for Minimum Score of Zero | Participants’ Standard Scores per 1000 kcal | Participants’ Maximum Points | ||||
|---|---|---|---|---|---|---|---|---|---|
| Adequacy: | Boys | Girls | p-Value | Boys | Girls | p-Value | |||
| Total Fruit 2 | 5 | ≥0.8 cup equivalent per 1000 kcal | No fruit | 0.99 ± 0.045 | 0.98 ± 0.043 | 0.911 | 3.33 ± 0.07 | 3.29 ± 0.07 | 0.655 |
| Whole Fruit 3 | 5 | ≥0.4 cup equivalent per 1000 kcal | No whole fruit | 0.54 ± 0.036 | 0.53 ± 0.031 | 0.921 | 3.09 ± 0.096 | 3.12 ± 0.090 | 0.841 |
| Total Vegetables 4 | 5 | ≥1.1 cup equivalent per 1000 kcal | No vegetables | 0.69 ± 0.028 | 0.78 ± 0.026 | 0.016 | 2.30 ± 0.069 | 2.61 ± 0.061 | 0.001 |
| Greens and Beans 4 | 5 | ≥0.2 cup equivalent per 1000 kcal | No dark leafy vegetables or greens and beans | 0.20 ± 0.016 | 0.23 ± 0.016 | 0.161 | 2.56 ± 0.161 | 2.64 ± 0.153 | 0.717 |
| Whole Grains | 10 | ≥1.5 oz equivalent per 1000 kcal | No whole grains | 0.26 ± 0.011 | 0.26 ± 0.011 | 0.823 | 4.09 ± 0.170 | 3.63 ± 0.151 | 0.042 |
| Dairy 5 | 10 | ≥1.3 cup equivalent per 1000 kcal | No dairy | 0.66 ± 0.020 | 0.72 ± 0.024 | 0.036 | 4.56 ± 0.123 | 4.96 ± 0.136 | 0.034 |
| Total Protein Foods 6 | 5 | ≥2.5 oz equivalent per 1000 kcal | No protein foods | 2.44 ± 0.070 | 2.19 ± 0.067 | 0.011 | 3.23 ± 0.058 | 2.99 ± 0.065 | 0.006 |
| Seafood and Plant Proteins 7 | 5 | ≥0.8 oz equivalent per 1000 kcal | No seafood or plant proteins | 1.49 ± 0.083 | 1.33 ± 0.070 | 0.131 | 3.58 ± 0.059 | 3.49 ± 0.061 | 0.291 |
| Fatty Acids 8 | 10 | (PUFAs + MUFAs)/SFAs > 2.5 | (PUFAs + MUFAs)/SFAs ≤ 1.2 | 0.81 ± 0.029 | 0.96 ± 0.037 | 0.001 | 1.26 ± 0.099 | 1.73 ± 0.149 | 0.010 |
| Moderation: | |||||||||
| Refined Grains | 10 | ≤1.8 oz equivalent per 1000 kcal | ≥4.3 oz equivalents per 1000 kcal | 2.80 ± 0.050 | 2.83 ± 0.050 | 0.620 | 7.27 ± 0.15 | 7.15 ± 0.16 | 0.578 |
| Sodium | 10 | ≤1.1 g per 1000 kcal | ≥2.0 g per 1000 kcal | 1.49 ± 0.018 | 1.50 ± 0.018 | 0.683 | 9.27 ± 0.202 | 8.36 ± 0.271 | 0.009 |
| Empty Calories 9 | 20 | ≤19% of energy | ≥50% of energy | 28.56 ± 0.46 | 28.69 ± 0.44 | 0.845 | 13.98 ± 0.723 | 13.86 ± 0.254 | 0.734 |
| Total HEI Score | 58.54 ± 7.02 | 57.86 ± 7.81 | 0.429 | ||||||
| Good Score ≥ 80 | 0% | 0% | |||||||
| Poor Score ≤ 50 | 12.2% | 15.8% | 0.374 | ||||||
| Component | Maximum Points | Standard for Maximum Score | Standard for Minimum Score of Zero | Participants’ Standard Scores per 1000 kcal | Participants’ Maximum Points | ||||
|---|---|---|---|---|---|---|---|---|---|
| Adequacy: | Boys | Girls | p-Value | Boys | Girls | p-Value | |||
| Total Fruit 2 | 5 | ≥0.8 cup equivalent per 1000 kcal | No fruit | 0.99 ± 0.045 | 0.98 ± 0.043 | 0.911 | 3.33 ± 0.07 | 3.29 ± 0.07 | 0.655 |
| Whole Fruit 3 | 5 | ≥0.4 cup equivalent per 1000 kcal | No whole fruit | 0.54 ± 0.036 | 0.53 ± 0.031 | 0.921 | 3.09 ± 0.096 | 3.12 ± 0.090 | 0.841 |
| Total Vegetables 4 | 5 | ≥1.1 cup equivalent per 1000 kcal | No vegetables | 0.69 ± 0.028 | 0.78 ± 0.026 | 0.016 | 2.30 ± 0.069 | 2.61 ± 0.061 | 0.001 |
| Greens and Beans 4 | 5 | ≥0.2 cup equivalent per 1000 kcal | No dark leafy vegetables or greens and beans | 0.20 ± 0.016 | 0.23 ± 0.016 | 0.161 | 2.56 ± 0.161 | 2.64 ± 0.153 | 0.717 |
| Whole Grains | 10 | ≥1.5 oz equivalent per 1000 kcal | No whole grains | 0.26 ± 0.011 | 0.26 ± 0.011 | 0.823 | 4.09 ± 0.170 | 3.63 ± 0.151 | 0.042 |
| Dairy 5 | 10 | ≥1.3 cup equivalent per 1000 kcal | No dairy | 0.66 ± 0.020 | 0.72 ± 0.024 | 0.036 | 4.56 ± 0.123 | 4.96 ± 0.136 | 0.034 |
| Total Protein Foods 6 | 5 | ≥2.5 oz equivalent per 1000 kcal | No protein foods | 2.44 ± 0.070 | 2.19 ± 0.067 | 0.011 | 3.23 ± 0.058 | 2.99 ± 0.065 | 0.006 |
| Seafood and Plant Proteins 7 | 5 | ≥0.8 oz equivalent per 1000 kcal | No seafood or plant proteins | 1.49 ± 0.083 | 1.33 ± 0.070 | 0.131 | 3.58 ± 0.059 | 3.49 ± 0.061 | 0.291 |
| Fatty Acids 8 | 10 | (PUFAs + MUFAs)/SFAs > 2.5 | (PUFAs + MUFAs)/SFAs ≤ 1.2 | 0.81 ± 0.029 | 0.96 ± 0.037 | 0.001 | 1.26 ± 0.099 | 1.73 ± 0.149 | 0.010 |
| Moderation: | |||||||||
| Refined Grains | 10 | ≤1.8 oz equivalent per 1000 kcal | ≥4.3 oz equivalent per 1000 kcal | 2.80 ± 0.050 | 2.83 ± 0.050 | 0.620 | 7.27 ± 0.15 | 7.15 ± 0.16 | 0.578 |
| Sodium | 10 | ≤1.1 g per 1000 kcal | ≥2.0 g per 1000 kcal | 1.49 ± 0.018 | 1.50 ± 0.018 | 0.683 | 9.27 ± 0.202 | 8.36 ± 0.271 | 0.009 |
| Added Sugars | 10 | ≤6.5% of energy | ≥26% of energy | 14.98 ± 0.47 | 15.17 ± 0.43 | 0.768 | 4.43 ± 0.197 | 4.46 ± 0.189 | 0.901 |
| Saturated Fats 9 | 10 | ≤8% of energy | ≥16% of energy | 10.63 ± 0.104 | 10.62 ± 0.113 | 0.954 | 3.47 ± 0.111 | 3.44 ± 0.120 | 0.850 |
| Total HEI Score | 52.50 ± 5.68 | 51.92 ± 6.17 | 0.385 | ||||||
| Good Score ≥ 80 | 0% | 0% | |||||||
| Poor Score ≤ 50 | 31.1% | 41.2% | 0.063 | ||||||
| BMI | BMI-Z | WC | BF% | SBP | DBP | TC | HDL | LDL | TC:HDL | Non-HDL | TG | MVPA | ST | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adequacy Components | ||||||||||||||
| Total Fruit | −0.054 | −0.064 | −0.042 | −0.079 | −0.063 | −0.039 | −0.004 | 0.038 | −0.004 | −0.021 | −0.005 | −0.074 | 0.229 ** | −0.030 |
| Whole Fruit | −0.109 | −0.101 | −0.094 | −0.105 | −0.079 | −0.076 | −0.013 | 0.065 | −0.031 | −0.045 | −0.028 | −0.052 | 0.109 | −0.030 |
| Total Vegetables | −0.024 | 0.025 | 0.032 | 0.024 | 0.089 | 0.074 | 0.020 | −0.025 | 0.013 | 0.047 | 0.034 | 0.119 | −0.007 | −0.030 |
| Greens and Beans | 0.057 | 0.097 | 0.070 | 0.089 | 0.103 | 0.050 | −0.003 | −0.049 | 0.040 | 0.107 | 0.065 | 0.134 | 0.057 | 0.059 |
| Whole Grains | 0.038 | 0.040 | 0.044 | 0.027 | −0.067 | −0.001 | −0.026 | −0.046 | 0.001 | 0.066 | 0.047 | 0.008 | 0.141 * | −0.045 |
| Dairy | 0.014 | 0.014 | 0.013 | 0.016 | 0.023 | 0.055 | 0.008 | 0.110 | 0.004 | −0.066 | 0.011 | −0.065 | 0.068 | −0.020 |
| Total Protein Foods | 0.000 | 0.019 | −0.023 | 0.005 | −0.012 | −0.010 | −0.054 | −0.025 | 0.014 | −0.052 | −0.062 | −0.133 | −0.029 | 0.049 |
| Seafood and Plant Proteins | 0.028 | 0.006 | 0.033 | 0.032 | −0.012 | −0.056 | −0.014 | 0.027 | −0.015 | −0.007 | −0.021 | 0.028 | 0.013 | 0.027 |
| Fatty Acids | 0.075 | 0.067 | 0.057 | 0.074 | 0.140 * | 0.053 | −0.043 | 0.024 | −0.073 | −0.068 | −0.065 | −0.002 | −0.069 | −0.089 |
| Moderation Components | ||||||||||||||
| Refined Grains | −0.050 | −0.041 | 0.026 | −0.040 | −0.020 | −0.033 | −0.038 | −0.013 | −0.054 | −0.010 | −0.010 | 0.123 | 0.018 | 0.048 |
| Sodium | −0.026 | −0.022 | 0.009 | −0.012 | −0.112 * | −0.051 | 0.078 | −0.038 | 0.099 | 0.090 | 0.120 | 0.062 | 0.085 | 0.082 |
| Empty Calories (HEI-2010) | −0.035 | −0.017 | −0.035 | −0.006 | −0.025 | −0.052 | 0.035 | 0.005 | 0.059 | 0.013 | 0.026 | −0.094 | 0.093 | −0.119 * |
| Added Sugars (HEI-2015) | 0.032 | 0.015 | 0.040 | 0.002 | 0.030 | 0.055 | −0.043 | 0.022 | −0.068 | −0.038 | −0.054 | 0.077 | −0.069 | 0.101 |
| Saturated Fats (HEI-2015) | −0.053 | −0.061 | −0.103 | −0.027 | −0.009 | −0.025 | 0.028 | −0.048 | 0.060 | 0.098 | 0.097 | 0.051 | −0.123 * | 0.070 |
| Total HEI Score | ||||||||||||||
| HEI-2010 | −0.027 | 0.001 | 0.025 | 0.007 | −0.031 | −0.034 | 0.026 | 0.000 | 0.048 | 0.060 | 0.085 | 0.052 | 0.179 ** | −0.040 |
| HEI-2015 | −0.015 | 0.002 | 0.034 | 0.005 | −0.022 | −0.006 | −0.016 | −0.002 | 0.010 | 0.053 | 0.065 | 0.127 | 0.106 | 0.088 |
| HEI-2010 Poor Total Score ≤ 50 Points | ||||||||||||
| Adjustment for Sex, MVPA, and ST | ||||||||||||
| Risk Factor | B | SE | Sig. | Exp(B) | 95% CI for Exp(B) | B | SE | Sig. | Exp(B) | 95% CI for Exp(B) | ||
| Lower | Upper | Lower | Upper | |||||||||
| Obesity +2 SD | −1.057 | 0.202 | 0.000 | 0.347 | 0.234 | 0.516 | −0.310 | 0.258 | 0.229 | 0.733 | 0.442 | 1.216 |
| Elevated BP | −0.595 | 0.311 | 0.056 | 0.552 | 0.300 | 1.016 | −0.174 | 0.327 | 0.594 | 0.840 | 0.443 | 1.594 |
| Stage 1 HTN | 0.511 | 0.730 | 0.484 | 1.667 | 0.398 | 6.974 | 1.001 | 0.756 | 0.185 | 2.722 | 0.619 | 11.976 |
| Stage 2 HTN | −21.203 | 28,420.722 | 0.999 | 0.000 | 0.000 | 0.000 | −0.174 | 0.327 | 0.594 | 0.840 | 0.443 | 1.594 |
| HEI-2015 Poor Total Score ≤ 50 Points | ||||||||||||
| Adjustment for Sex, MVPA, and ST | ||||||||||||
| Risk Factor | B | SE | Sig. | Exp(B) | 95% CI for Exp(B) | B | SE | Sig. | Exp(B) | 95% CI for Exp(B) | ||
| Lower | Upper | Lower | Upper | |||||||||
| Obesity +2 SD | −0.578 | 0.184 | 0.002 | 0.561 | 0.391 | 0.805 | −0.105 | 0.241 | 0.665 | 0.901 | 0.561 | 1.446 |
| Elevated BP | 0.442 | 0.427 | 0.301 | 1.556 | 0.673 | 3.594 | 0.804 | 0.446 | 0.071 | 2.235 | 0.932 | 5.365 |
| Confounder | ||||||||||||
| Sex | −0.744 | 0.200 | 0.000 | 0.475 | 0.321 | 0.703 | ||||||
| Stage 1 HTN | 0.000 | 0.707 | 1.000 | 1.000 | 0.250 | 3.998 | 0.300 | 0.722 | 0.677 | 1.350 | 0.328 | 5.556 |
| Stage 2 HTN | 0.000 | 1.414 | 1.000 | 1.000 | 0.063 | 15.988 | 0.358 | 1.440 | 0.804 | 1.430 | 0.085 | 24.069 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Farhan, A.K.; Weatherspoon, L.J.; Pfeiffer, K.A.; Li, W.; Carlson, J.J. Dietary Quality Evidenced by the Healthy Eating Index and Cardiovascular Disease Risk Factors in Kuwaiti Schoolchildren. Nutrients 2024, 16, 1243. https://doi.org/10.3390/nu16081243
Al-Farhan AK, Weatherspoon LJ, Pfeiffer KA, Li W, Carlson JJ. Dietary Quality Evidenced by the Healthy Eating Index and Cardiovascular Disease Risk Factors in Kuwaiti Schoolchildren. Nutrients. 2024; 16(8):1243. https://doi.org/10.3390/nu16081243
Chicago/Turabian StyleAl-Farhan, Abdulaziz Kh., Lorraine J. Weatherspoon, Karin A. Pfeiffer, Wei Li, and Joseph J. Carlson. 2024. "Dietary Quality Evidenced by the Healthy Eating Index and Cardiovascular Disease Risk Factors in Kuwaiti Schoolchildren" Nutrients 16, no. 8: 1243. https://doi.org/10.3390/nu16081243