
Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Assessment of Neonatal 25(OH)D3
2.4. Eczema Definitions
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Study Population
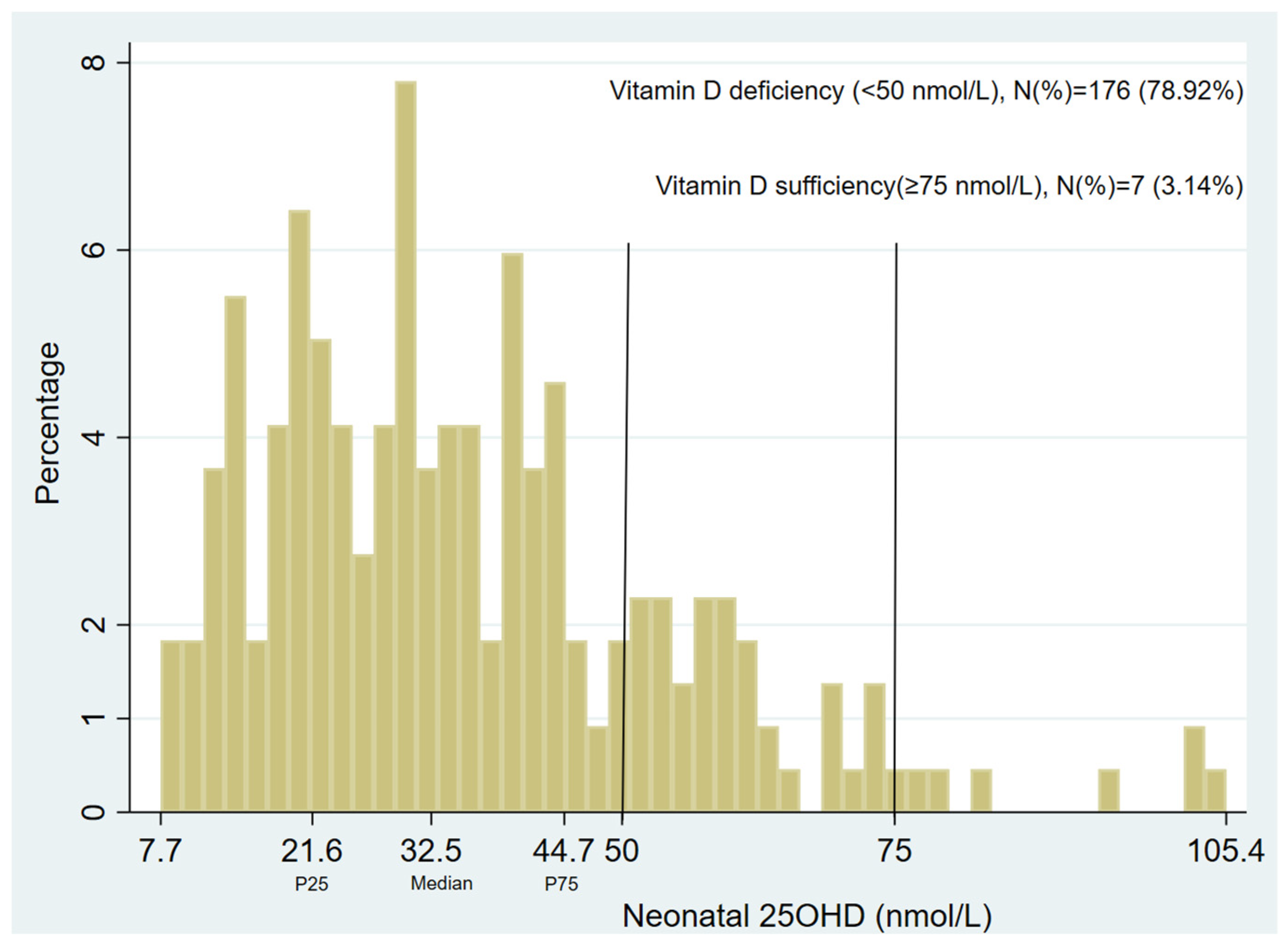
3.2. Neonatal Vitamin D Status
3.3. Neonatal Vitamin D Levels and 12-Month Prevalent Eczema at Age 1, 6, 12, 18, or 25 Years
3.4. Neonatal Vitamin D and Longitudinal Eczema Phenotypes up to 12 and 25 Years
3.5. Eczema/Sensitization Phenotypes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 25(OH)D3 | 25-hydroxyvitamin D3 |
| SPT | skin prick testing |
| aMOR | adjusted multinomial odds ratio |
| VDR | vitamin D receptors |
| MACS | Melbourne Atopy Cohort Study |
| DBS | dried blood spots |
| LC/MS | liquid chromatography–tandem mass spectrometry |
| BIC | Bayesian information criterion |
| GEE | generalized estimation equation |
| DAG | directed acyclic graph |
| VCGS | Victorian Clinical Genetics Services |
| SES | socio-economic status |
| HREC | Human Research Ethics Committee |
References
- Johansson, S.G.O.; Bieber, T.; Dahl, R.; Friedmann, P.S.; Lanier, B.Q.; Lockey, R.F.; Motala, R.; Ortega Martell, J.A.O.; Platts-Mills, T.A.E.; Ring, J.; et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J. Allergy Clin. Immunol. 2004, 113, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.J. Molecular mechanisms in atopic eczema: Insights gained from genetic studies. J. Pathol. 2017, 241, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Bieber, T. Atopic Dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Osborne, N.J.; Ukoumunne, O.C.; Wake, M.; Allen, K.J. Prevalence of eczema and food allergy is associated with latitude in Australia. J. Allergy Clin. Immunol. 2012, 129, 865–867. [Google Scholar] [CrossRef] [PubMed]
- Poole, A.; Song, Y.; Brown, H.; Hart, P.H.; Zhang, G. Cellular and molecular mechanisms of vitamin D in food allergy. J. Cell. Mol. Med. 2018, 22, 3270–3277. [Google Scholar] [CrossRef]
- Plum, L.A.; DeLuca, H.F. The Functional Metabolism and Molecular Biology of Vitamin D Action. Clin. Rev. Bone Miner. Metab. 2009, 7, 20–41. [Google Scholar] [CrossRef]
- Heine, G.; Niesner, U.; Chang, H.-D.; Steinmeyer, A.; Zugel, U.; Zuberbier, T.; Radbruch, A.; Worm, M. 1,25-dihydroxyvitamin D3 promotes IL-10 production in human B cells. Eur. J. Immunol. 2008, 38, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- Kay, J.; Gawkrodger, D.J.; Mortimer, M.J.; Jaron, A.G. The prevalence of childhood atopic eczema in a general population. J. Am. Acad. Dermatol. 1994, 30, 35–39. [Google Scholar] [CrossRef] [PubMed]
- de Lusignan, S.; Alexander, H.; Broderick, C.; Dennis, J.; McGovern, A.; Feeney, C.; Flohr, C. The epidemiology of eczema in children and adults in England: A population-based study using primary care data. Clin. Exp. Allergy 2021, 51, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J. Vitamin D and the Development of Atopic Eczema. J. Clin. Med. 2015, 4, 1036–1050. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, Á.; Hourihane, J.O.B.; Malvisi, L.; Irvine, A.D.; Kenny, L.C.; Murray, D.M.; Kiely, M.E. Antenatal vitamin D exposure and childhood eczema, food allergy, asthma and allergic rhinitis at 2 and 5 years of age in the atopic disease-specific Cork BASELINE Birth Cohort Study. Allergy 2018, 73, 2182–2191. [Google Scholar] [CrossRef] [PubMed]
- Baïz, N.; Dargent-Molina, P.; Wark, J.D.; Souberbielle, J.-C.; Annesi-Maesano, I. Cord serum 25-hydroxyvitamin D and risk of early childhood transient wheezing and atopic dermatitis. J. Allergy Clin. Immunol. 2014, 133, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.P.; Palmer, D.; Zhang, G.; Prescott, S.L. Cord blood 25-hydroxyvitamin D3 and allergic disease during infancy. Pediatrics 2012, 130, e1128–e1135. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J.; Sullivan, T.R.; Skeaff, C.M.; Smithers, L.G.; Makrides, M. Higher cord blood 25-hydroxyvitamin D concentrations reduce the risk of early childhood eczema: In children with a family history of allergic disease. World Allergy Organ. J. 2015, 8, 28. [Google Scholar] [CrossRef]
- Jones, A.P.; D‘Vaz, N.; Meldrum, S.; Palmer, D.J.; Zhang, G.; Prescott, S.L. 25-hydroxyvitamin D3 status is associated with developing adaptive and innate immune responses in the first 6 months of life. Clin. Exp. Allergy 2015, 45, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Chawes, B.L.; Bonnelykke, K.; Jensen, P.F.; Schoos, A.M.M.; Heickendorff, L.; Bisgaard, H. Cord blood 25(OH)-vitamin D deficiency and childhood asthma, allergy and eczema: The COPSAC2000 birth cohort study. PLoS ONE 2014, 9, e99856. [Google Scholar] [CrossRef] [PubMed]
- Zeng, R.; Li, Y.; Shen, S.; Qiu, X.; Chang, C.-L.; Koplin, J.J.; Perrett, K.P.; Dharmage, S.C.; Lodge, C.J.; Lowe, A.J. Is antenatal or early-life vitamin D associated with eczema or food allergy in childhood? A systematic review. Clin. Exp. Allergy 2023, 53, 511–525. [Google Scholar] [CrossRef]
- Rabbani, S.; Afaq, S.; Fazid, S.; Khattak, M.I.; Yousafzai, Y.M.; Habib, S.H.; Lowe, N.; Ul-Haq, Z. Correlation between maternal and neonatal blood Vitamin D level: Study from Pakistan. Matern. Child. Nutr. 2021, 17, e13028. [Google Scholar] [CrossRef] [PubMed]
- van der Pligt, P.F.; Ellery, S.J.; de Guingand, D.L.; Abbott, G.; Della Gatta, P.A.; Daly, R.M. Maternal plasma vitamin D levels across pregnancy are not associated with neonatal birthweight: Findings from an Australian cohort study of low-risk pregnant women. BMC Pregnancy Childbirth 2023, 23, 67. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Stubbs, B.J.; Mirzakhani, H.; O’Connor, G.T.; Sandel, M.; Beigelman, A.; Bachanier, L.B.; Zeiger, R.S.; et al. Six-Year Follow-up of a Trial of Antenatal Vitamin D for Asthma Reduction. N. Engl. J. Med. 2020, 382, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Chawes, B.L.; Bonnelykke, K.; Stokholm, J.; Vissing, N.H.; Bjarnadóttir, E.; Schoos, A.-M.M.; Wolsk, H.M.; Pedersen, T.M.; Vinding, R.K.; Thorsteinsdóttir, S.; et al. Effect of Vitamin D3 supplementation during pregnancy on risk of persistent wheeze in the offspring: A randomized clinical trial. JAMA J. Am. Med. Assoc. 2016, 315, 353–361. [Google Scholar] [CrossRef]
- El-Heis, S.; D’Angelo, S.; Curtis, E.M.; Healy, E.; Moon, R.J.; Crozier, S.R.; Inskip, H.; Cooper, C.; Harvey, N.C.; Godfrey, K.M.; et al. Maternal antenatal vitamin D supplementation and offspring risk of atopic eczema in the first 4 years of life: Evidence from a randomized controlled trial. Br. J. Dermatol. 2022, 187, 659–666. [Google Scholar] [CrossRef]
- Goldring, S.T.; Griffiths, C.J.; Martineau, A.R.; Robinson, S.; Yu, C.; Poulton, S.; Kirby, J.C.; Stocks, J.; Hooper, R.; Shaheen, S.O.; et al. Prenatal vitamin d supplementation and child respiratory health: A randomised controlled trial. PLoS ONE 2013, 8, e66627. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Vitamin D Status. 2023. Available online: https://www.health.gov.au/resources/pregnancy-care-guidelines/part-g-targeted-maternal-health-tests/vitamin-d-status#references (accessed on 1 June 2023).
- ACOG Vitamin D: Screening and Supplementation during Pregnancy. The American College of Obstetricians and Gynecologists 2011. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2011/07/vitamin-d-screening-and-supplementation-during-pregnancy (accessed on 24 January 2023).
- WHO Guideline. Vitamin D Supplementation in Pregnant Women; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Haider, S.; Granell, R.; Curtin, J.A.; Holloway, J.W.; Fontanella, S.; Arshad, S.H.; Murray, C.S.; Cullinan, P.; Turner, S.; Roberts, G.; et al. Identification of eczema clusters and their association with filaggrin and atopic comorbidities: Analysis of five birth cohorts. Br. J. Dermatol. 2023, 190, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Lopez, D.J.; Lodge, C.J.; Bui, D.S.; Waidyatillake, N.T.; Abramson, M.J.; Perret, J.L.; Su, J.C.; Erbas, B.; Svanes, C.; Dharmage, S.C.; et al. Establishing subclasses of childhood eczema, their risk factors and prognosis. Clin. Exp. Allergy 2022, 52, 1079–1090. [Google Scholar] [CrossRef] [PubMed]
- Thacher, T.D.; Clarke, B.L. Vitamin D insufficiency. Mayo Clin. Proc. 2011, 86, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.J.; Lodge, C.J.; Allen, K.J.; Abramsin, M.J.; Matheson, M.C.; Thomas, P.S.; Barton, C.A.; Bennett, C.M.; Erbas, B.; Svanes, C.; et al. Cohort Profile: Melbourne Atopy Cohort study (MACS). Int. J. Epidemiol. 2017, 46, 25–26g. [Google Scholar] [CrossRef] [PubMed]
- VCGS Newborn Bloodspot Screening Test. Available online: https://www.vcgs.org.au/tests/newborn-bloodspot-screening (accessed on 11 May 2021).
- Kvaskoff, D.; Ko, P.; Simila, H.A.; Eyles, D.W. Distribution of 25-hydroxyvitamin D3 in dried blood spots and implications for its quantitation by tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2012, 901, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Muthén, B.; Muthén, L.K. Integrating Person-Centered and Variable-Centered Analyses: Growth Mixture Modeling With Latent Trajectory Classes. Alcohol. Clin. Exp. Res. 2000, 24, 882–891. [Google Scholar] [CrossRef]
- Smith, C.A.; Sun, C.; Pezic, A.; Rodda, C.; Cameron, F.; Allen, K.; Craig, M.E.; Carlin, J.; Dwyer, T.; Lucas, R.M.; et al. Determinants of Neonatal Vitamin D Levels as Measured on Neonatal Dried Blood Spot Samples. Neonatology 2017, 111, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W.; Morley, R.; Anderson, C.; Ko, P.; Burne, T.; Permezel, M.; Mortensen, P.B.; Norgaard-Pedersen, B.; Hougard, D.M.; McGarth, J.J. The utility of neonatal dried blood spots for the assessment of neonatal vitamin D status. Paediatr. Perinat. Epidemiol. 2010, 24, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Thorsen, S.U.; Collier, F.; Pezic, A.; O’Hely, M.; Clarke, M.; Tang, M.L.K.; Burgner, D.; Vuillermin, P.; Ponsoboy, A.-L.; Barwon Infant Study Investigator Group. Maternal and Cord Blood 25-Hydroxyvitamin D3 Are Associated with Increased Cord Blood and Naive and Activated Regulatory T Cells: The Barwon Infant Study. J. Immunol. 2021, 206, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Suaini, N.H.A.; Loo, E.X.-L.; Peters, R.L.; Yap, G.C.; Allen, K.J.; Van Bever, H.; Martino, D.J.; Neo Goh, A.E.; Dharmage, S.C.; Colega, M.T.; et al. Children of Asian ethnicity in Australia have higher risk of food allergy and early-onset eczema than those in Singapore. Allergy 2021, 76, 3171–3182. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.J.; Koplin, J.J.; Ponsonby, A.L.; Gurrin, L.C.; Wake, M.; Vuillermin, P.; Martin, P.; Matherson, M.; Lowe, A.; Robinson, M.; et al. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J. Allergy Clin. Immunol. 2013, 131, 1109–1116.e6. [Google Scholar] [CrossRef]
- Tanaka, K.; Miyake, Y.; Furukawa, S.; Arakawa, M. Pre- and Postnatal Smoking Exposure and Risk of Atopic Eczema in Young Japanese Children: A Prospective Prebirth Cohort Study. Nicotine Tob. Res. 2017, 19, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Susanto, N.H.; Lowe, A.J.; Salim, A.; Koplin, J.J.; Tang, M.L.K.; Suani, N.H.A.; Ponsonby, A.-L.; Allen, K.J.; Dharmage, S.C.; Erbas, B. Associations between grass pollen exposures in utero and in early life with food allergy in 12-month-old infants. Int. J. Env. Health Res. 2022, 32, 712–722. [Google Scholar] [CrossRef] [PubMed]
- Xepapadaki, P.; Papadopoulos, N.G. Viral infections and allergies. Immunobiology 2007, 212, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Renz, H.; Skevaki, C. Early life microbial exposures and allergy risks: Opportunities for prevention. Nat. Rev. Immunol. 2021, 21, 177–191. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Estimates | Prevalent Eczema Age | |||||
|---|---|---|---|---|---|---|
| 1 Year | 2 Years | 6 Years | 12 Years | 18 Years | 25 Years | |
| n/N † | 70/220 | 63/214 | 26/174 | 25/155 | 47/196 | 32/122 |
| Unadjusted associations | ||||||
| OR (95% CI) | 1.05 (0.90–1.22) | 0.86 (0.72–1.02) | 0.86 (0.67–1.10) | 0.89 (0.69–1.14) | 1.13 (0.99–1.28) | 1.04 (0.88–1.22) |
| p-value | 0.539 | 0.087 | 0.239 | 0.361 | 0.067 | 0.648 |
| Adjusted associations (Model 1) ‡ | ||||||
| OR (95% CI) | 1.06 (0.90–1.24) | 0.86 (0.72–1.03) | 0.87 (0.67–1.12) | 0.91 (0.71–1.17) | 1.03 (0.85–1.26) | 0.94 (0.74–1.20) |
| p-value | 0.489 | 0.091 | 0.275 | 0.484 | 0.741 | 0.623 |
| Additionally adjusted for the season of birth (Model 2) § | ||||||
| OR (95% CI) | 1.04 (0.87–1.24) | 0.80 (0.65–0.98) | 0.81 (0.60–1.08) | 0.86 (0.65–1.14) | 1.01 (0.81–1.27) | 0.87 (0.67–1.14) |
| p-value | 0.658 | 0.032 | 0.155 | 0.301 | 0.909 | 0.318 |
| Estimates | Longitudinal Eczema Subclasses | ||||
|---|---|---|---|---|---|
| Early-Onset Persistent | Early-Onset- Resolving | Mid-Onset Persistent | Mid-Onset- Resolving | Minimal/No Eczema | |
| n/N † | 22/223 | 18/223 | 25/223 | 4/223 | 154/223 |
| Unadjusted associations | |||||
| MOR (95% CI) | 0.75 (0.57–0.98) | 1.22 (0.98–1.52) | 0.98 (0.81–1.18) | 0.73 (0.40–1.31) | 1.00 (Reference) |
| p-value | 0.039 | 0.073 | 0.828 | 0.282 | - |
| Adjusted associations (Model 1) ‡ | |||||
| aMOR ¶ (95% CI) | 0.74 (0.56–0.98) | 1.30 (1.05–1.62) | 0.97 (0.79–1.19) | 0.66 (0.35–1.24) | 1.00 (Reference) |
| p-value | 0.036 | 0.016 | 0.787 | 0.196 | - |
| Additionally adjusted for the season of birth (Model 2) § | |||||
| aMOR (95% CI) | 0.75 (0.55–1.02) | 1.21 (0.93–1.56) | 0.89 (0.70–1.13) | 0.68 (0.38–1.23) | 1.00 (Reference) |
| p-value | 0.068 | 0.150 | 0.351 | 0.206 | - |
| Estimates | Longitudinal Eczema Subclass | |||
|---|---|---|---|---|
| Early-Onset Persistent | Early-Onset-Resolving | Mid-Onset Persistent | Minimal/No Eczema | |
| n/N † | 21/223 | 20/223 | 31/223 | 151/223 |
| Unadjusted associations | ||||
| MOR (95% CI) | 0.76 (0.58–1.01) | 1.13 (0.89–1.43) | 1.03 (0.85–1.24) | 1.00 (Reference) |
| p-value | 0.055 | 0.305 | 0.750 | - |
| Adjusted associations (Model 1) ‡ | ||||
| aMOR ¶ (95% CI) | 0.76 (0.58–1.01) | 1.18 (0.93–1.50) | 1.03 (0.84–1.25) | 1.00 (Reference) |
| p-value | 0.057 | 0.170 | 0.780 | - |
| Additionally adjusted for the season of birth (Model 2) § | ||||
| aMOR (95% CI) | 0.76 (0.55–1.04) | 1.05 (0.86–1.42) | 0.96 (0.75–1.22) | 1.00 (Reference) |
| p-value | 0.088 | 0.444 | 0.730 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, R.; Lodge, C.J.; Koplin, J.J.; Lopez, D.J.; Erbas, B.; Abramson, M.J.; Eyles, D.; Ponsonby, A.-L.; Wjst, M.; Allen, K.; et al. Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age. Nutrients 2024, 16, 1303. https://doi.org/10.3390/nu16091303
Zeng R, Lodge CJ, Koplin JJ, Lopez DJ, Erbas B, Abramson MJ, Eyles D, Ponsonby A-L, Wjst M, Allen K, et al. Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age. Nutrients. 2024; 16(9):1303. https://doi.org/10.3390/nu16091303
Chicago/Turabian StyleZeng, Rong, Caroline J. Lodge, Jennifer J. Koplin, Diego J. Lopez, Bircan Erbas, Michael J. Abramson, Darryl Eyles, Anne-Louise Ponsonby, Matthias Wjst, Katrina Allen, and et al. 2024. "Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age" Nutrients 16, no. 9: 1303. https://doi.org/10.3390/nu16091303