Green Tea Consumption and Risk of Pancreatic Cancer: A Meta-analysis

Abstract
:1. Introduction
2. Experimental Section
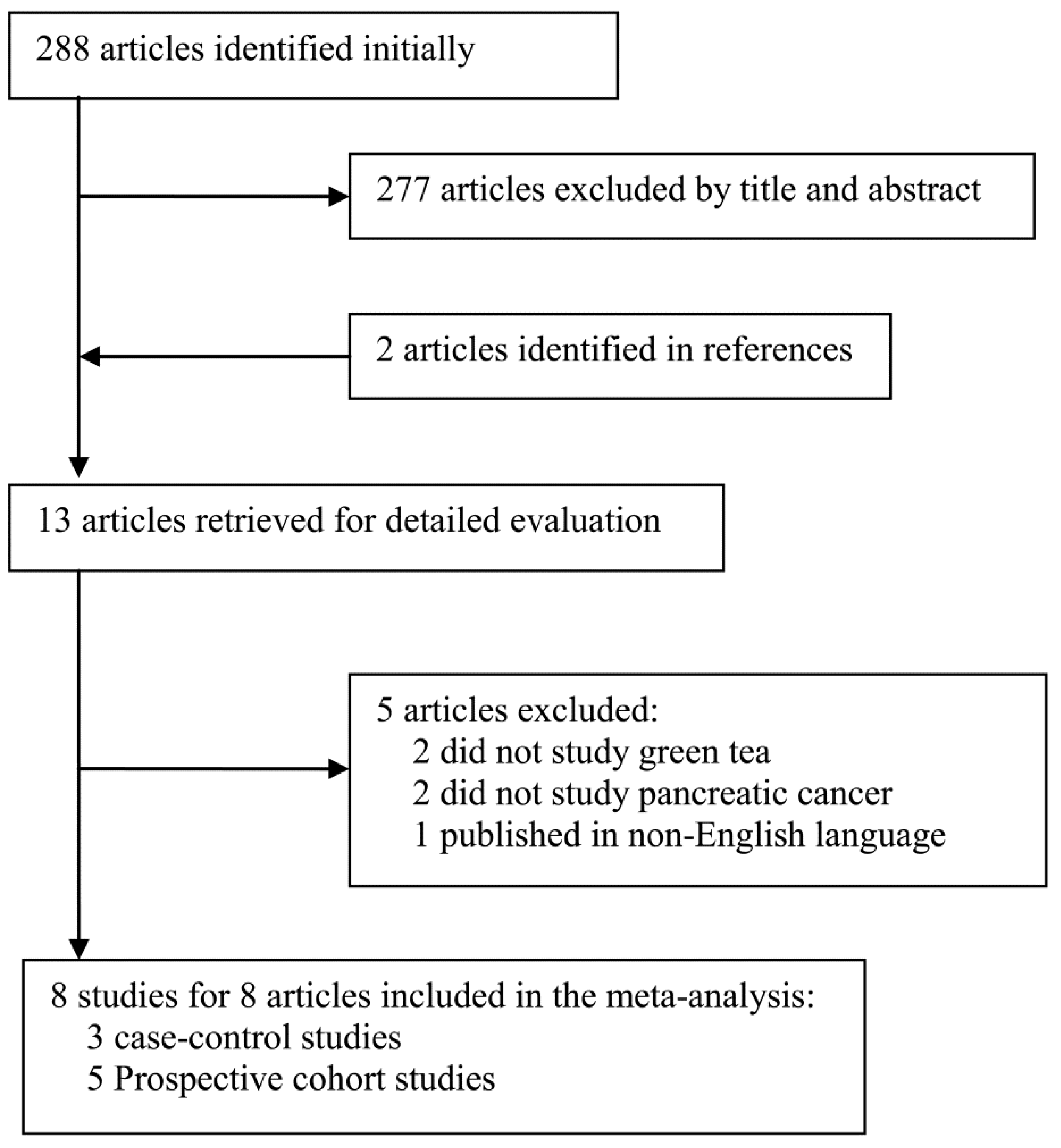
2.1. Literature Search and Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Study Characteristics
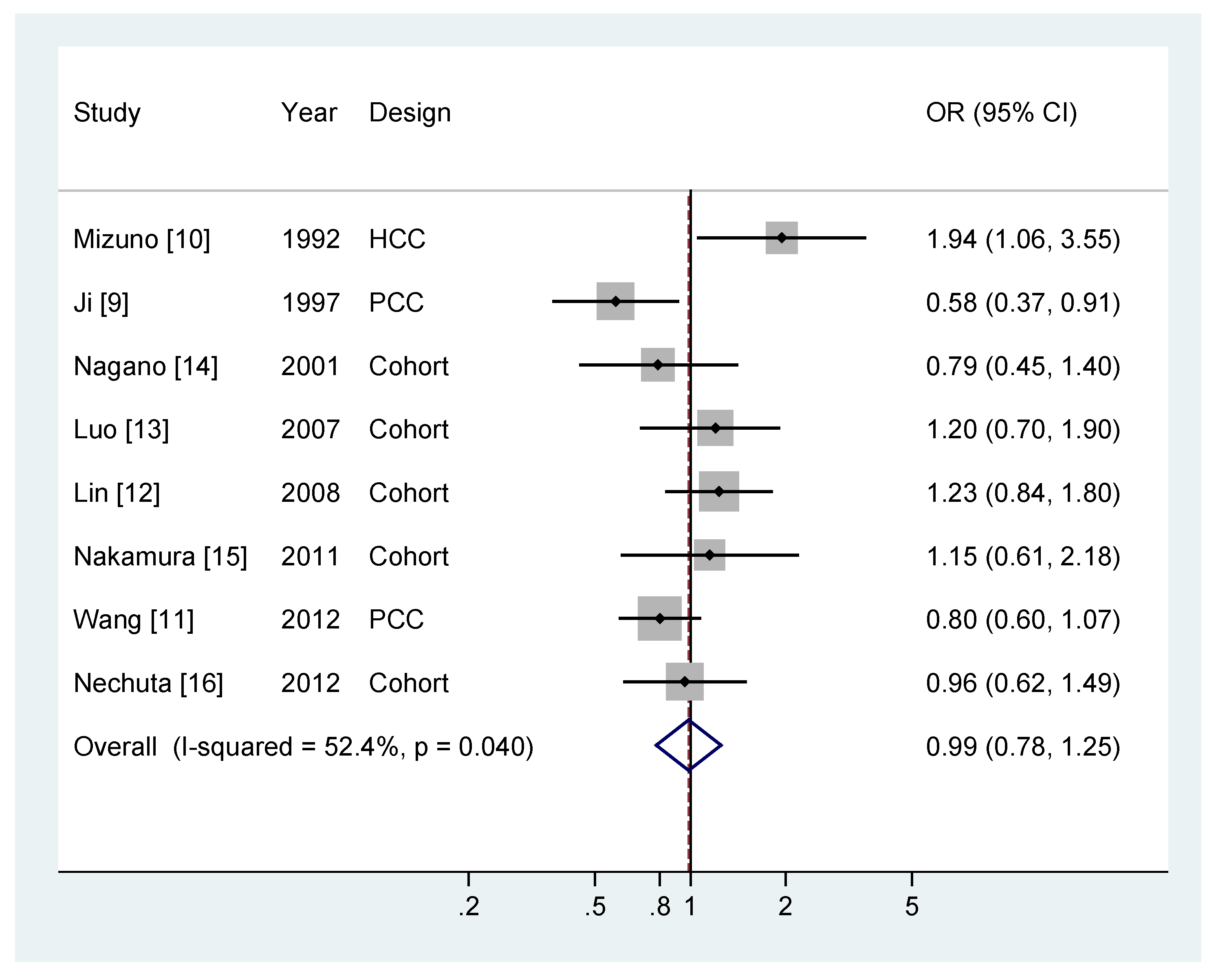
3.2. Meta-analysis


{kind=link}
{kind=link}
| Study | Country | Design | Sex | Cases/participants | Green tea consumption (highest vs. lowest) | OR/RR (95% CI) | Exposure assessment | Variables controlled for |
|---|---|---|---|---|---|---|---|---|
| Mizuno, 1992 [10] | Japan | HCC | M/F | 127/254 | ≥5 vs. <5 cups/day | 1.94 (1.06–3.55) | Interview | Age and sex. |
| Ji, 1997 [9] | China | PCC | M/F | 451/2003 | ≥300 vs. 0 g/month (M) ≥200 vs. 0 g/month (F) | 0.63 (0.34–1.17) (M) 0.53 (0.29–1.09) (F) | Interview | Age, income, education and smoking. |
| Nagano, 2001 [14] | Japan | Cohort | M/F | 122/3854 | ≥5 vs. 0–1 cups/day | 0.79 (0.45–1.40) | Self-report | Age, sex, BMI, radiation dose, drinking history, education and calendar time. |
| Luo, 2007 [13] | Japan | Cohort | M/F | 233/102137 | ≥ 5 vs. 0 cups/day | 1.20 (0.70–1.90) | Self-report | Age, sex, BMI, physical activity, smoking, history of diabetes or cholelithiasis, study area, and intakes of coffee and alcohol. |
| Lin, 2008 [12] | Japan | Cohort | M/F | 292/77850 | ≥7 vs. <1 cups/day | 1.23 (0.84–1.80) | Self-report | Age, sex, BMI, smoking, alcohol drinking, and history of diabetes or gallbladder diseases. |
| Nakamura, 2011 [15] | Japan | Cohort | M/F | 52/30826 | ≥1 vs. 0 cups/day | 1.77 (0.78–4.04) (M) 0.59 (0.21–1.61) (F) | Self-report | Age, BMI, smoking, and history of diabetes. |
| Wang, 2012 [11] | China | PCC | M/F | 908/1975 | ≥250 vs. 0 g/month (M) ≥150 vs. 0 g/month (F) | 0.91 (0.65–1.27) (M) 0.56 (0.32–0.98) (F) | Interview | Age, BMI, education, family history of cancer, smoking, history of type 2 diabetes, and additional adjustment for women included: menopausal status, oral contraceptives use, and menopausal hormone therapy. |
| Nechuta, 2012 [16] | China | Cohort | F | 132/69310 | Regular vs. Never regular. | 0.96 (0.62–1.49) | Self-report | Age, BMI, marital status, education, occupation, exercise, intakes of fruit, vegetable and meat, history of diabetes, and family history of digestive system cancer. |

| N | OR (95% CI) | P for heterogeneity | I2 (%) | P for differences | |
|---|---|---|---|---|---|
| All studies | 8 | 0.99 (0.78–1.25) | 0.04 | 52.4 | |
| Design | |||||
| Cohort | 5 | 1.07 (0.87–1.33) | 0.72 | 0.0 | 0.52 |
| Case-control | 3 | 0.93 (0.53–1.63) | 0.006 | 80.2 | |
| Number of cases | |||||
| >200 | 4 | 0.90 (0.65–1.25) | 0.04 | 63.2 | 0.44 |
| <200 | 4 | 1.11 (0.78–1.60) | 0.17 | 41.0 | |
| Area | |||||
| China | 3 | 0.77 (0.60–0.99) | 0.23 | 21.7 | 0.04 |
| Japan | 5 | 1.21 (0.94–1.54) | 0.34 | 12.0 | |
| Sex | |||||
| Men | 5 | 0.98 (0.74–1.30) | 0.27 | 22.3 | 0.50 |
| Women | 6 | 0.84 (0.59–1.19) | 0.08 | 49.9 | Reference |
| Both sexes | 4 | 1.22 (0.89–1.65) | 0.21 | 33.6 | |
| Smoking status | |||||
| Smokers | 1 | 0.90 (0.45–1.80) | - | - | 0.84 |
| Non-smokers | 3 | 1.01 (0.65–1.57) | 0.13 | 50.7 |
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Michl, P.; Gress, T.M. Current concepts and novel targets in advanced pancreatic cancer. Gut 2013, 62, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, Y.; Hara, Y. Antimutagenic and anticarcinogenic activity of tea polyphenols. Mutat. Res. 1999, 436, 69–97. [Google Scholar] [CrossRef] [PubMed]
- Lyn-Cook, B.D.; Rogers, T.; Yan, Y.; Blann, E.B.; Kadlubar, F.F.; Hammons, G.J. Chemopreventive effects of tea extracts and various components on human pancreatic and prostate tumor cells in vitro. Nutr. Cancer 1999, 35, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Vu, H.A.; Beppu, Y.; Chi, H.T.; Sasaki, K.; Yamamoto, H.; Xinh, P.T.; Tanii, T.; Hara, Y.; Watanabe, T.; Sato, Y.; et al. Green tea epigallocatechin gallate exhibits anticancer effect in human pancreatic carcinoma cells via the inhibition of both focal adhesion kinase and insulin-like growth factor-I receptor. J. Biomed. Biotechnol. 2011, 2010. [Google Scholar] [CrossRef]
- Zhang, L.; Pang, E.; Loo, R.R.; Rao, J.; Go, V.L.; Loo, J.A.; Lu, Q.Y. Concomitant inhibition of HSP90, its mitochondrial localized homologue TRAP1 and HSP27 by green tea in pancreatic cancer HPAF-II cells. Proteomics 2011, 11, 4638–4647. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, C.; Artacho, R.; Gimenez, R. Beneficial effects of green tea—A review. J. Am. Coll. Nutr. 2006, 25, 79–99. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; World Cancer Research Fund/American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- Boehm, K.; Borrelli, F.; Ernst, E.; Habacher, G.; Hung, S.K.; Milazzo, S.; Horneber, M. Green tea (Camellia sinensis) for the prevention of cancer. Cochrane. Database Syst. Rev. 2009, 3. [Google Scholar] [CrossRef]
- Ji, B.T.; Chow, W.H.; Hsing, A.W.; McLaughlin, J.K.; Dai, Q.; Gao, Y.T.; Blot, W.J.; Fraumeni, J.F. Green tea consumption and the risk of pancreatic and colorectal cancers. Int. J. Cancer 1997, 70, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Watanabe, S.; Nakamura, K.; Omata, M.; Oguchi, H.; Ohashi, K.; Ohyanagi, H.; Fujiki, T.; Motojima, K. A multi-institute case-control study on the risk factors of developing pancreatic cancer. Jpn. J. Clin. Oncol. 1992, 22, 286–291. [Google Scholar] [PubMed]
- Wang, J.; Zhang, W.; Sun, L.; Yu, H.; Ni, Q.X.; Risch, H.A.; Gao, Y.T. Green tea drinking and risk of pancreatic cancer: A large-scale, population-based case-control study in urban Shanghai. Cancer Epidemiol. 2012, 36, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Kikuchi, S.; Tamakoshi, A.; Yagyu, K.; Obata, Y.; Kurosawa, M.; Inaba, Y.; Kawamura, T.; Motohashi, Y.; Ishibashi, T. Green tea consumption and the risk of pancreatic cancer in Japanese adults. Pancreas 2008, 37, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Inoue, M.; Iwasaki, M.; Sasazuki, S.; Otani, T.; Ye, W.; Tsugane, S. Green tea and coffee intake and risk of pancreatic cancer in a large-scale, population-based cohort study in Japan (JPHC study). Eur. J. Cancer Prev. 2007, 16, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Nagano, J.; Kono, S.; Preston, D.L.; Mabuchi, K. A prospective study of green tea consumption and cancer incidence, Hiroshima and Nagasaki (Japan). Cancer Causes Control 2001, 12, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Nagata, C.; Wada, K.; Tamai, Y.; Tsuji, M.; Takatsuka, N.; Shimizu, H. Cigarette smoking and other lifestyle factors in relation to the risk of pancreatic cancer death: A prospective cohort study in Japan. Jpn. J. Clin. Oncol. 2011, 41, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Nechuta, S.; Shu, X.O.; Li, H.L.; Yang, G.; Ji, B.T.; Xiang, Y.B.; Cai, H.; Chow, W.H.; Gao, Y.T.; Zheng, W. Prospective cohort study of tea consumption and risk of digestive system cancers: Results from the Shanghai Women’s Health Study. Am. J. Clin. Nutr. 2012, 96, 1056–1063. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [PubMed]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose-respose data. Stata J. 2006, 6, 40–57. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey, S.G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Mena, S.; Ortega, A.; Estrela, J.M. Oxidative stress in environmental-induced carcinogenesis. Mutat. Res. 2009, 674, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Takada, M.; Nakamura, Y.; Koizumi, T.; Toyama, H.; Kamigaki, T.; Suzuki, Y.; Takeyama, Y.; Kuroda, Y. Suppression of human pancreatic carcinoma cell growth and invasion by epigallocatechin-3-gallate. Pancreas 2002, 25, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Majima, T.; Tsutsumi, M.; Nishino, H.; Tsunoda, T.; Konishi, Y. Inhibitory effects of beta-carotene, palm carotene, and green tea polyphenols on pancreatic carcinogenesis initiated by N-nitorsobis(2-oxopropyl)amine in Syrian golden hamsters. Pancreas 1998, 16, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Hiura, A.; Tsutsumi, M.; Satake, K. Inhibitory effect of green tea extract on the process of pancreatic carcinogenesis induced by N-nitrosobis-(2-oxypropyl)amine (BOP) and on tumor promotion after transplantation of N-nitrosobis-(2-hydroxypropyl)amine (BHP)-induced pancreatic cancer in Syrian hamsters. Pancreas 1997, 15, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Maliakal, P.; Chen, L.; Meng, X.; Bondoc, F.Y.; Prabhu, S.; Lambert, G.; Mohr, S.; Yang, C.S. Pharmacokinetics of tea catechins after ingestion of green tea and (−)-epigallocatechin-3-gallate by humans: Formation of different metabolites and individual variability. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1025–1032. [Google Scholar]
- Henning, S.M.; Niu, Y.; Liu, Y.; Lee, N.H.; Hara, Y.; Thames, G.D.; Minutti, R.R.; Carpenter, C.L.; Wang, H.; Heber, D. Bioavailability and antioxidant effect of epigallocatechin gallate administered in purified form versus as green tea extract in healthy individuals. J. Nutr. Biochem. 2005, 16, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.H.; Gao, Q.Y.; Fang, J.Y. Green tea and incidence of colorectal cancer: Evidence from prospective cohort studies. Nutr. Cancer 2012, 64, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Rha, S.Y.; Oh, K.W.; Nam, C.M. Green tea consumption and stomach cancer risk: A meta-analysis. Epidemiol. Health 2010, 32. [Google Scholar] [CrossRef]
- Gao, Y.T.; McLaughlin, J.K.; Blot, W.J.; Ji, B.T.; Dai, Q.; Fraumeni, J.F. Reduced risk of esophageal cancer associated with green tea consumption. J. Natl. Cancer Inst. 1994, 86, 855–858. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Sasazuki, S.; Wakai, K.; Suzuki, T.; Matsuo, K.; Shimazu, T.; Tsuji, I.; Tanaka, K.; Mizoue, T.; Nagata, C.; et al. Green tea consumption and gastric cancer in Japanese: A pooled analysis of six cohort studies. Gut 2009, 58, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Zheng, W.; Xiang, Y.B.; Gao, J.; Li, H.L.; Zhang, X.; Gao, Y.T.; Shu, X.O. Green tea consumption and colorectal cancer risk: A report from the Shanghai Men’s Health Study. Carcinogenesis 2011, 32, 1684–1688. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, J.-L.; Li, Z.-H.; Wang, Z.-C.; Zhang, H.-L. Green Tea Consumption and Risk of Pancreatic Cancer: A Meta-analysis. Nutrients 2014, 6, 4640-4650. https://doi.org/10.3390/nu6114640
Zeng J-L, Li Z-H, Wang Z-C, Zhang H-L. Green Tea Consumption and Risk of Pancreatic Cancer: A Meta-analysis. Nutrients. 2014; 6(11):4640-4650. https://doi.org/10.3390/nu6114640
Chicago/Turabian StyleZeng, Jin-Long, Zhi-Hua Li, Zhi-Chao Wang, and Hai-Liang Zhang. 2014. "Green Tea Consumption and Risk of Pancreatic Cancer: A Meta-analysis" Nutrients 6, no. 11: 4640-4650. https://doi.org/10.3390/nu6114640