Subclinical Cardiovascular Damage and Fat Utilization in Overweight/Obese Individuals Receiving the Same Dietary and Pharmacological Interventions

Abstract
:1. Introduction
2. Experimental Section
2.1. Blood Pressure Measurement
2.1.1. Biochemical Evaluation
2.1.2. Anthropometric and Nutritional Intake Measurements
2.2. Cardiovascular Assessment
2.2.1. Echocardiographic Evaluation
2.2.2. Left Ventricular Geometric Pattern and Systolic Function
2.3. Carotid Arteries Assessment
2.4. Statistical Analysis
3. Results

{kind=link}
| Variables | Normal Geometry | LVCR | p |
|---|---|---|---|
| Male sex (%) | 23.5 (4) | 26 (5) | 0.58 |
| Diabetes (%) | 5.9 | 5.9 | 0.75 |
| Hypertension (%) | 41.2 | 43.8 | 0.58 |
| Dyslipidemia (%) | 31.3 | 33.3 | 0.60 |
| Smoking (%) | 11.7 | 6.6 | 0.58 |
| Menopausal status (%) | 50 | 50 | 0.34 |
| Angiotensin-converting-enzyme inhibitor (%) | 53.8 | 46.2 | 0.61 |
| Diuretics (%) | 40 | 60 | 0.52 |
| Variables | Normal Geometry | LVCR | p |
|---|---|---|---|
| Age (years) | 50.06 ± 11 | 54.06 ± 10 | 0.297 |
| RMR (joule) | 5796 ± 715 | 6137 ± 1137 | 0.195 |
| RQ | 0.85 ± 0.05 | 0.89 ± 0.05 | 0.038 |
| BMI (kg/m2) | 32.56 ± 5 | 32.78 ± 7 | 0.924 |
| WC (cm) | 99.38 ± 10 | 102.87 ± 15 | 0.477 |
| HC (cm) | 105.97 ± 10 | 109.37 ± 11 | 0.274 |
| TBW (Lt) | 38.53 ± 7 | 40.06 ± 8 | 0.615 |
| ECW (Lt) | 17.04 ± 3 | 17.85 ± 3 | 0.514 |
| FFM (kg) | 52.09 ± 10 | 53.46 ± 12 | 0.755 |
| MM (kg) | 35.01 ± 7 | 36.22 ± 10 | 0.734 |
| FM (kg) | 28.47 ± 10 | 33.07 ± 12 | 0.297 |
| Glucose (mmol/L) | 5.12 ± 0.4 | 5.60 ± 1.3 | 0.177 |
| Creatinine (μmol/L) | 64.2 ± 8 | 66 ± 17 | 0.931 |
| T Cholesterol (mmol/L) | 5.89 ± 1.68 | 5.79 ± 1 | 0.835 |
| HDLCholest (mmol/L) | 1.43 ± 0.28 | 1.42 ± 0.41 | 0.956 |
| LDLCholest (mmol/L) | 3.91 ± 1.47 | 3.63 ± 0.98 | 0.521 |
| Triglycerides (mmol/L) | 1.21 ± 0.5 | 1.73 ± 1 | 0.083 |
| Calcium (mg/dL ) | 9.51 ± 0.39 | 9.42 ± 0.34 | 0.508 |
| Uric Acid (μmol/L) | 255.7 ± 59 | 296.2 ± 59 | 0.309 |
| SBP (mmHg) | 133.18 ± 14 | 128.41 ± 31 | 0.579 |
| DBP (mmHg) | 86.41 ± 8 | 80.82 ± 6 | 0.036 |
| HR (b/m) | 71.71 ± 7 | 73.06 ± 7 | 0.607 |
| Mean CIMT (mm) | 0.57 ± 0.11 | 0.80 ± 0.19 | 0.015 |
| LVMI (g/m2) | 72.51 ± 11 | 77.14 ± 11 | 0.243 |
| AR (mm) | 31.06 ± 3 | 32.06 ± 2 | 0.315 |
| LAD (mm) | 33.94 ± 3 | 34 ± 4 | 0.965 |
| LVend-dias diam(mm) | 47.35 ± 3 | 42.39 ± 5 | 0.004 |
| LV end-syst diam(mm) | 32.12 ± 3 | 27.94 ± 5 | 0.015 |
| Interventricular sept(mm) | 8.82 ± 0.78 | 11.63 ± 1.24 | <0.001 |
| LV Poster Wall(mm) | 8.49 ± 0.82 | 10.71 ± 0.90 | <0.001 |
| EF (%) | 60.12 ± 4 | 62.44 ± 4 | 0.147 |
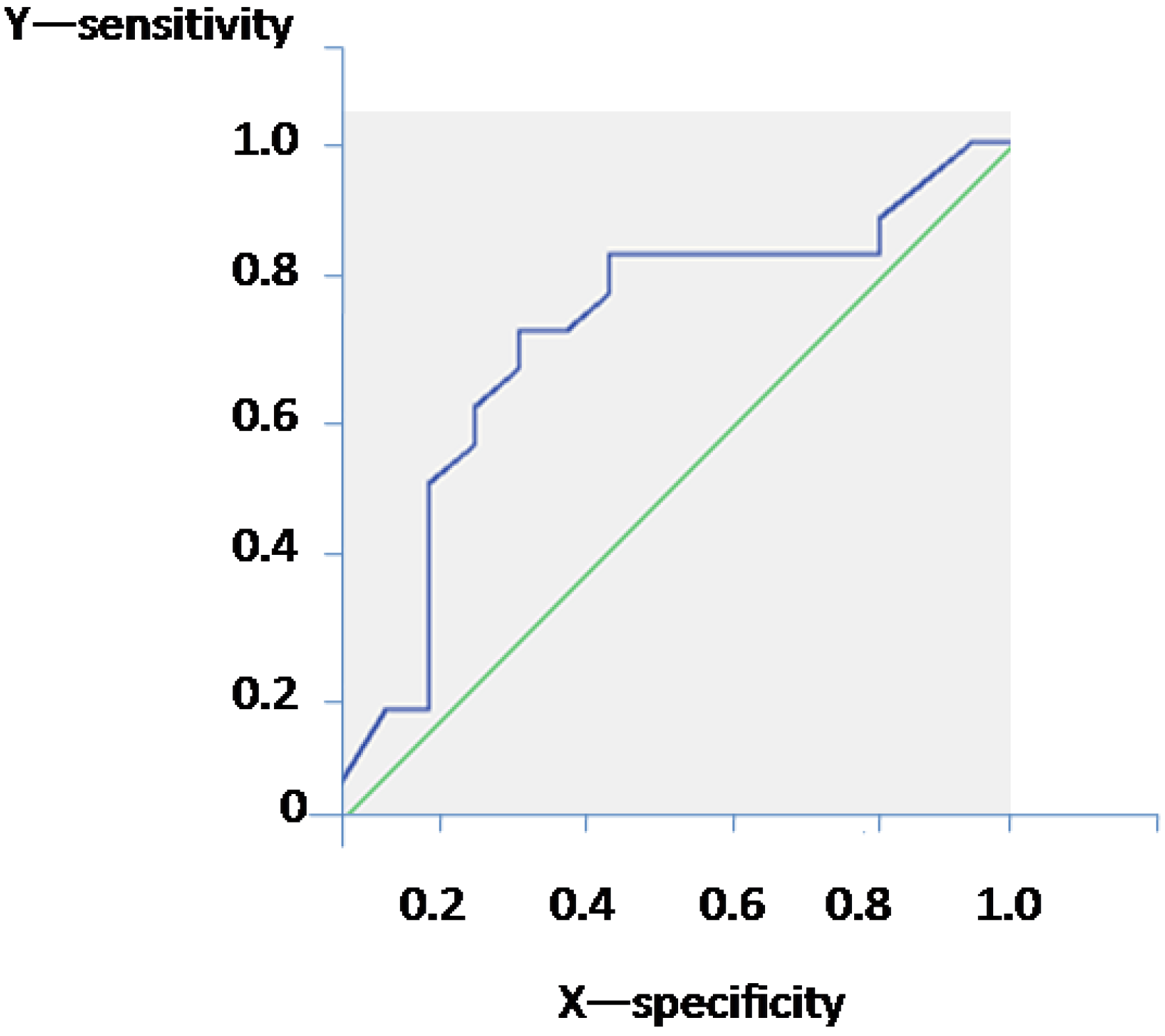
| Area | Standard Error | p | CI 95% | |
|---|---|---|---|---|
| Lower Limit | Higher Limit | |||
| 0.720 | 0.093 | 0.031 | 0.537 | 0.903 |

4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Stanley, W.C.; Recchia, F.A.; Lopaschuk, G.D. Review myocardial substrate metabolism in the normal and failing heart. Physiol. Rev. 2005, 85, 1093–1129. [Google Scholar] [CrossRef] [PubMed]
- Ussher, J.R.; Wang, W.; Gandhi, M.; Keung, W.; Samokhvalov, V.; Oka, T.; Wagg, C.S.; Jaswal, J.S.; Harris, R.A.; Clanachan, A.S.; et al. Stimulation of glucose oxidation protects against acute myocardial infarction and reperfusion injury. Cardiovasc. Res. 2012, 94, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Shrafian, H.; Frenneaux, M.P.; Opie, L.H. Metabolic mechanisms in heart failure. Circulation 2007, 116, 434–448. [Google Scholar] [CrossRef] [PubMed]
- Christe, M.E.; Rodgers, R.L. Altered glucose and fatty acid oxidation in hearts of the spontaneously hypertensive rat. J. Mol. Cell. Cardiol. 1994, 26, 1371–1374. [Google Scholar] [CrossRef] [PubMed]
- Zurlo, F.; Lillioja, S.; Esposito-Del Puente, A.; Nyomba, B.L.; Raz, I.; Saad, M.F.; Swinburn, B.A.; Knowler, W.C.; Bogardus, C.; Ravussin, E. Low ratio of fat to carbohydrate oxidation as predictor of weight gain: Study of 24-h RQ. Am. J. Physiol. 1990, 259, 650–657. [Google Scholar]
- Ferro, Y.; Gazzaruso, C.; Coppola, A.; Migliaccio, V.; Romeo, S.; Giustina, A.; Pujia, A.; Montalcini, T. Fat utilisationand arterial hypertension in overweight/obese subjects. J. Transl. Med. 2013, 11. [Google Scholar] [CrossRef]
- Montalcini, T.; Gazzaruso, C.; Ferro, Y.; Migliaccio, V.; Rotundo, S.; Castagna, A.; Pujia, A. Metabolic fuel utilisation and subclinical atherosclerosis in overweight/obese subjects. Endocrine. 2013, 44, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of clinical cardiovascular events with carotid intima-media thickness—A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Di Bello, V.; Carerj, S.; Perticone, F.; Benedetto, F.; Palombo, C.; Talini, E.; Giannini, D.; la Carrubba, S.; Antonini-Canterin, F.; di Salvo, G. Carotid intima-media thickness in asymptomatic patients with arterial hypertension without clinical cardiovascular disease: Relation with left ventricular geometry and mass and coexisting risk factors. Angiology 2009, 60, 705–713. [Google Scholar] [CrossRef] [PubMed]
- National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group Report on Hypertension in the Elderly. Hypertension 1994, 23, 275–285. [Google Scholar]
- Psaty, B.M.; Furberg, C.D.; Kuller, L.H.; Bild, D.E.; Rautaharju, P.M.; Polak, J.F.; Bovill, E.; Gottdiener, J.S. Traditional risk factors and subclinical disease measures as predictors of first myocardial infarction in older adults: The cardiovascular health study. Arch. Intern. Med. 1999, 59, 1339–1347. [Google Scholar] [CrossRef]
- Montalcini, T.; Gorgone, G.; Fava, A.; Romeo, S.; Gazzaruso, C.; Pujia, A. Carotid and brachial arterial enlargement in postmenopausal women with hypertension. Menopause 2012, 9, 145–149. [Google Scholar] [CrossRef]
- Montalcini, T.; Gorgone, G.; Garzaniti, A.; Gazzaruso, C.; Pujia, A. Artery remodelling and abdominal adiposity in nonobese postmenopausal women. Eur. J. Clin. Nutr. 2010, 64, 1022–1024. [Google Scholar] [CrossRef] [PubMed]
- Talluri, T.; Lietdke, R.J.; Evangelisti, A.; Talluri, J.; Maggia, G. Fat-free mass qualitative assessment with bioelectric impedance analysis (BIA). Ann. N. Y. Acad. Sci. 1999, 873, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Zemel, M.B.; Bruckbauer, A. Effects of a leucine and pyridoxine-containing nutraceutical on fat oxidation, and oxidative and inflammatory stress in overweight and obese subjects. Nutrients 2012, 4, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Sahn, D.J.; de Maria, A.; Kisslo, J.; Weyman, A. The committee on M-mode standardization of the American society of echocardiography: Recommendations regarding quantitation in M-mode echocardiography: Results of a survey of echocardiographic measurements. Circulation 1978, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Devereux, R.B.; Casale, P.N.; Kligfield, P.; Eisenberg, R.R.; Miller, D.; Campo, E.; Alonso, D.R. Performance of primary and derived M-mode echocardiographic measurements for detection of left ventricular hypertrophy in necropsied subjects and in patients with systemic hypertension, mitral regurgitation and dilated cardiomyopathy. Am. J. Cardiol. 1986, 57, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Valensise, H.; Novelli, G.P.; Vasapollo, B.; di Ruzza, G.; Romanini, M.E.; Marchei, M.; Larciprete, G.; Manfellotto, D.; Romanini, C.; Galante, A. Maternal diastolic dysfunction and left ventricular geometry in gestational hypertension. Hypertension 2001, 37, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Dubois, D.; Dubois, E.F. A formula to estimate the approximate surface area if height and weight be known. Arch. Intern. Med. 1916, 17, 863–871. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, E.; Foster, F.A.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.M.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Schillaci, G.; Borgioni, C.; Ciucci, A.; Battistelli, M.; Barroccini, C.; Santucci, A.; Santucci, C.; Reboldi, G.; Porcellati, C. Adverse prognostic significance of concentric remodelling of the left ventricle in hypertensive patients with normal left ventricular mass. J. Am. Coll. Cardiol. 1995, 25, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Ganau, A.; Devereux, R.B.; Roman, M.J.; de Simone, G.; Pickering, T.G.; Saba, P.S.; Vargiu, P.; Simongini, I.; Laragh, J.H. Patterns of left ventricular hypertrophy and geometric remodelling in essential hypertension. J. Am. Coll. Cardiol. 1992, 19, 1550–1558. [Google Scholar] [CrossRef] [PubMed]
- Teichholz, L.E.; Kreulen, T.; Herman, M.V.; Gorlin, R. Problems in echocardiographic volume determinants: Echocardiographic-angiographic correlations in the presence or absence of asynergy. Am. J. Cardiol. 1976, 37, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Pujia, A.; Gnasso, A.; Irace, C.; Colonna, A.; Mattioli, P.L. Common carotid arterial wall thickness in NIDDM subjects. Diabetes Care 1994, 17, 1330–1336. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Hung, C.L.; Shin, S.H.; Skali, H.; Verma, A.; Ghali, J.K.; Køber, L.; Velazquez, E.J.; Rouleau, J.L.; McMurray, J.J.; et al. Cardiac structure and function, remodeling, and clinical outcomes among patients with diabetes after myocardial infarction complicated by left ventricular systolic dysfunction, heart failure, or both. Am. Heart J. 2011, 162, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Muiesan, M.L.; Salvetti, M.; Monteduro, C.; Bonzi, B.; Paini, A.; Viola, S.; Poisa, P.; Rizzoni, D.; Castellano, M.; Agabiti-Rosei, E. Left ventricular concentric geometry during treatment adversely affects cardiovascular prognosis in hypertensive patients. Hypertension 2004, 43, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Burke, L.E.; Bray, G.A.; Blair, S.; Allison, D.B.; Pi-Sunyer, X.; Hong, Y.; Eckel, R.H. Clinical implications of obesity with specific focus on cardiovascular disease: A statement for professionals from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: Endorsed by the American College of Cardiology Foundation. Circulation 2004, 110, 2952–2967. [Google Scholar] [CrossRef] [PubMed]
- Antozzi, C.; Zeviani, M. Cardiomyopathies in disorders of oxidative metabolism. Cardiovasc. Res. 1997, 35, 184–199. [Google Scholar] [CrossRef] [PubMed]
- Jameel, M.N.; Zhang, J. Myocardial energetics in left ventricular hypertrophy. Curr. Cardiol. Rev. 2009, 5, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Dyck, J.R.; Lopaschuk, G.D. Malonyl CoA control of fatty acid oxidation in the ischemic heart. J. Mol. Cell. Cardiol. 2002, 34, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- El Alaoui-Talibi, Z.; Guendouz, A.; Moravec, M.; Moravec, J. Control of oxidative metabolism in volume-overloaded rat hearts: Effect of propionyl-l-carnitine. Am. J. Physiol. 1997, 272, 1615–1624. [Google Scholar]
- Kelly, D.P.; Mendelsohn, N.J.; Sobel, B.E.; Bergmann, S.R. Detection and assessment by positron emission tomography of a genetically determined defect in myocardial fatty acid utilisation (long-chain acyl-CoA dehydrogenase deficiency). Am. J. Cardiol. 1993, 71, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Elia, M. Organ and tissue contribution to metabolic rate. In Energy Metabolism, Tissue Determinants and Cellular Corollaries; Kinney, J., Tucker, H., Eds.; Raven Press: New York, NY, USA, 1992; pp. 61–80. [Google Scholar]
- He, Q.; Heshka, S.; Albu, J.; Boxt, L.; Krasnow, N.; Elia, M.; Gallagher, D. Smaller organ mass with greater age, except for heart. J. Appl. Physiol. 2009, 106, 1780–1784. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Adachi-Akahane, S. Inter-organ communication in the regulation of lipid metabolism: Focusing on the network between the liver, intestine, and heart. J. Pharmacol. Sci. 2013, 123, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Panchal, S.K.; Ward, L.; Brown, L. Ellagic acid attenuates high-carbohydrate, high-fat diet-induced metabolic syndrome in rats. Eur. J. Nutr. 2013, 52, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Diwan, V.; Poudyal, H.; Brown, L. Piperine attenuates cardiovascular, liver and metabolic changes in high carbohydrate, high fat-fed rats. Cell Biochem. Biophys. 2013, 67, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Guallar, E.; Linton, J.A.; Lee, D.C.; Jang, Y.; Son, D.K.; Han, E.J.; Baek, S.J.; Yun, Y.D.; Jee, S.H.; et al. Fasting glucose level and the risk of incident atherosclerotic cardiovascular diseases. Diabetes Care 2013, 36, 1988–1993. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, D.H.; Black, M.A.; Pyke, K.E.; Padilla, J.; Atkinson, G.; Harris, R.A.; Parker, B.; Widlansky, M.E.; Tschakovsky, M.E.; Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, 2–12. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montalcini, T.; Lamprinoudi, T.; Gorgone, G.; Ferro, Y.; Romeo, S.; Pujia, A. Subclinical Cardiovascular Damage and Fat Utilization in Overweight/Obese Individuals Receiving the Same Dietary and Pharmacological Interventions. Nutrients 2014, 6, 5560-5571. https://doi.org/10.3390/nu6125560
Montalcini T, Lamprinoudi T, Gorgone G, Ferro Y, Romeo S, Pujia A. Subclinical Cardiovascular Damage and Fat Utilization in Overweight/Obese Individuals Receiving the Same Dietary and Pharmacological Interventions. Nutrients. 2014; 6(12):5560-5571. https://doi.org/10.3390/nu6125560
Chicago/Turabian StyleMontalcini, Tiziana, Theodora Lamprinoudi, Gaetano Gorgone, Yvelise Ferro, Stefano Romeo, and Arturo Pujia. 2014. "Subclinical Cardiovascular Damage and Fat Utilization in Overweight/Obese Individuals Receiving the Same Dietary and Pharmacological Interventions" Nutrients 6, no. 12: 5560-5571. https://doi.org/10.3390/nu6125560