Is Omega-3 Fatty Acids Enriched Nutrition Support Safe for Critical Ill Patients? A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Material and Method
2.1. Literature Search Strategy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Strategy |
|---|---|
| MEDLINE (Through PubMed) | (“Omega-3 fatty acids” [Title/Abstract] OR “fish oil” [Title/Abstract] OR “n-3 fatty acids” [Title/Abstract]” OR “eicosapentaenoic acid” [Title/Abstract] OR “docosahexaenoic acid” [Title/Abstract]) AND (“parenteral nutrition” [Title/Abstract] OR “TPN” [Title/Abstract] OR “PN” [Title/Abstract] OR “enteral nutrition” [Title/Abstract] OR “EN” [Title/Abstract]) AND (“critical” [Title/Abstract] OR “severe” [Title/Abstract] OR “intensive care” [Title/Abstract] OR “ICU”) |
| Cochrane Library | (“Omega-3 fatty acids” OR “fish oil” OR “n-3 fatty acids”) AND (“parenteral nutrition” OR “TPN” OR “PN” OR “enteral nutrition” OR “EN”) AND (“critical” OR “severe” OR “intensive care” OR “ICU”) |
| Chinese Biomedicine Database and CNKI | (“Yu You” OR “Omega-3” OR “Duo Bu Bao He Zhi Fang Suan”) AND (“Chang Wai Ying Yang” OR “TPN” OR “PN” OR “Chang Nei Ying Yang” OR “EN”) AND (“Wei Zhong Bing” OR “Wei Zhong Zheng” OR “ICU”) |
2.2. Study Selection
Inclusion and Exclusion Criteria
2.3. Methodological Quality Evaluation
| Items | Points | |
|---|---|---|
| Randomization | Appropriate | 2 |
| Did not describe the details of randomization | 1 | |
| Inappropriate | 0 | |
| Concealment | Appropriate | 2 |
| Did not describe the details of concealment | 1 | |
| Inappropriate or no concealment | 0 | |
| Blinded | Appropriate | 2 |
| Did not describe the details of blinded | 1 | |
| Inappropriate or not blinded | 0 | |
| Withdraw or drop-out | Described | 1 |
| Did not describe | 0 |
2.4. Measurements and Analytical Methods

3. Results
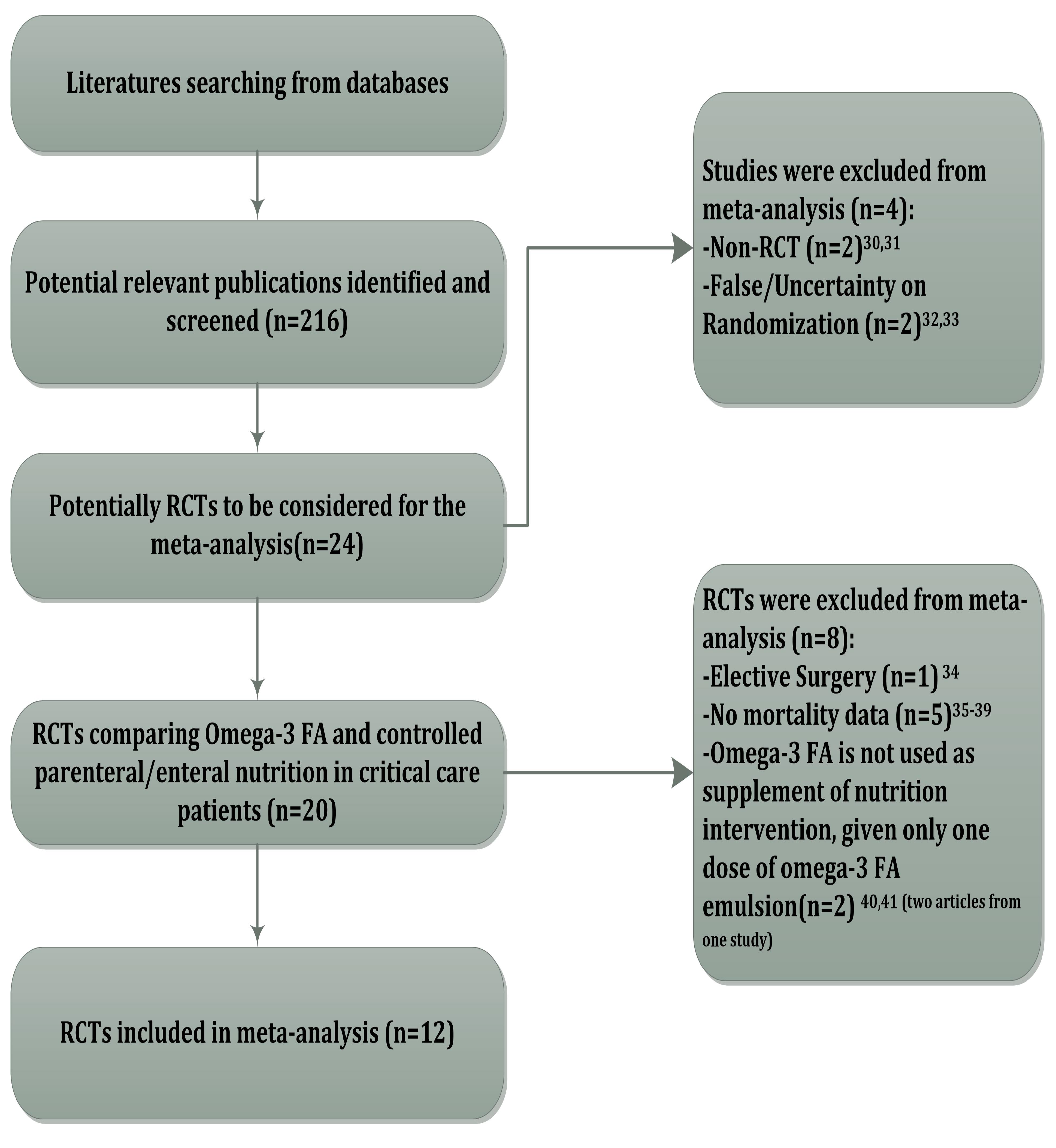
3.1. Study Identification and Selection

| Author, year | M.J.S | P.T. | N.O.P(ITT) | R.O.F | R.O.A. | Mortality n/N (ITT) | Calorie administered (kcal/day) | ||
|---|---|---|---|---|---|---|---|---|---|
| Omega-3 Group | Control Group | Omega-3 Group | Control Group | ||||||
| Gadek, J., 1999 [24] | 5 | ARDS | 146 | EN | EN | 11/70 | 19/76 | 1728 ± 74 | 1692 ± 60 |
| Grecu, I., 2003 [25] | 5 | Abdominal Sepsis | 54 | PN | PN | 2/28 | 2/26 | NR | NR |
| Mayer, K., 2003 [26] | 4 | sepsis | 21 | PN | PN | 5/10 | 3/11 | NR | NR |
| Pontes-Arruda, A., 2006 [27] | 5 | sepsis | 103 | EN | EN | 18/55 | 25/48 | 1621 ± 48 | 1647 ± 74 |
| Singer, P., 2006 [28] | 5 | ALI | 100 | EN | EN | 13/46 | 28/49 | 1624 ± 512 | 1420 ± 437 |
| Friesecke, S., 2008 [12] | 7 | Patients in medical ICU | 166 | PN + EN | PN | 18/83 | 22/82 | 22.2 ± 5.5 (kcal/kg/day) | 21.6 ± 5.6 (kcal/kg/day) |
| Wang, X., 2008 [11] | 4 | SAP | 56 | PN | PN | 0/28 | 2/28 | 27(kcal/kg/day) | 27 (kcal/kg/day) |
| Barbosa, V., 2010 [29] | 3 | sepsis | 23 | PN | PN | 2/13(5D), 4/13(28D) | 1/10(5D), 4/10(28D) | 2057 ± 418 | 1857 ± 255 |
| Grau-Carmona, T., 2011 [30] | 5 | sepsis | 132 | EN | EN | 11/61 | 11/71 | 1718 (1189–1956) | 1599 (1351–1976) |
| Gupta, A., 2011 [31] | 7 | ARDS | 61 | EN | PN | 7/31 | 13/30 | 1800 | 1800 |
| Stapleton, R.D., 2011 [32] | 5 | ALI | 90 | EN | EN | 9/41(14 days) 9/40(60 days) | 10/49(14 days) 11/45 (60 days) | NR | NR |
| Rice, T., 2011 [13] | 7 | ALI | 272 | EN | EN | 38/143 | 21/129 | 800–900 | 800–900 |
3.2. Primary Outcome: Mortality
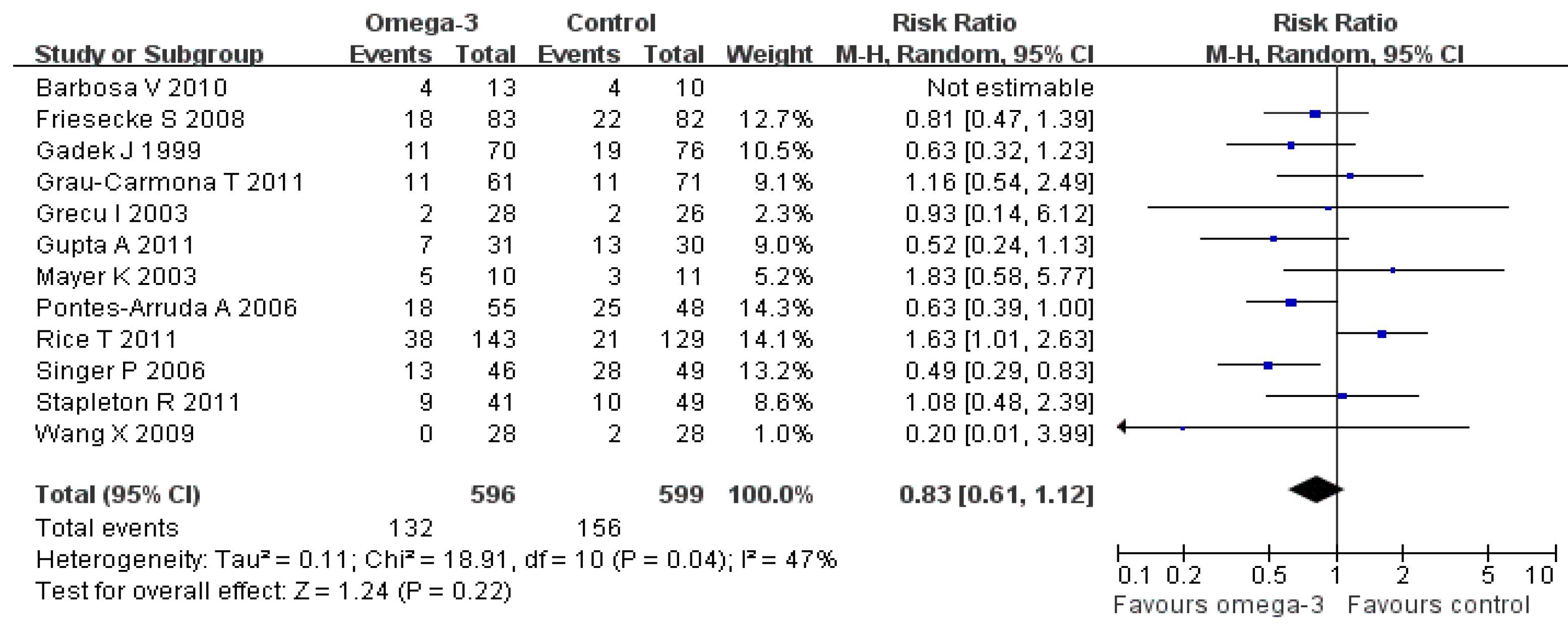
3.2.1 Overall Analysis

3.2.2. Sensitivity Analysis for All-Included Trials

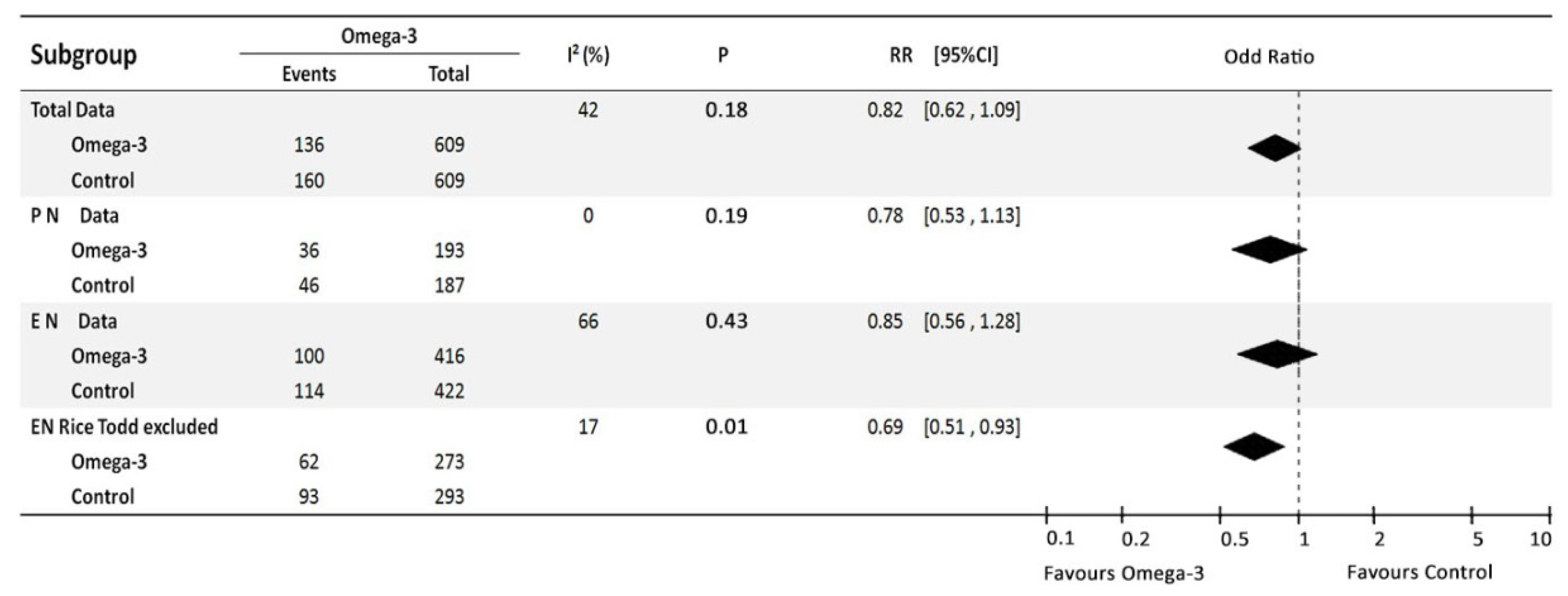
3.2.3. Sub-Group Analysis
3.2.3.1. Parenteral Omega-3 Studies
3.2.3.2. Sensitivity Analysis for PN Omega-3 Studies
3.2.3.3. Enteral Omega-3 Studies
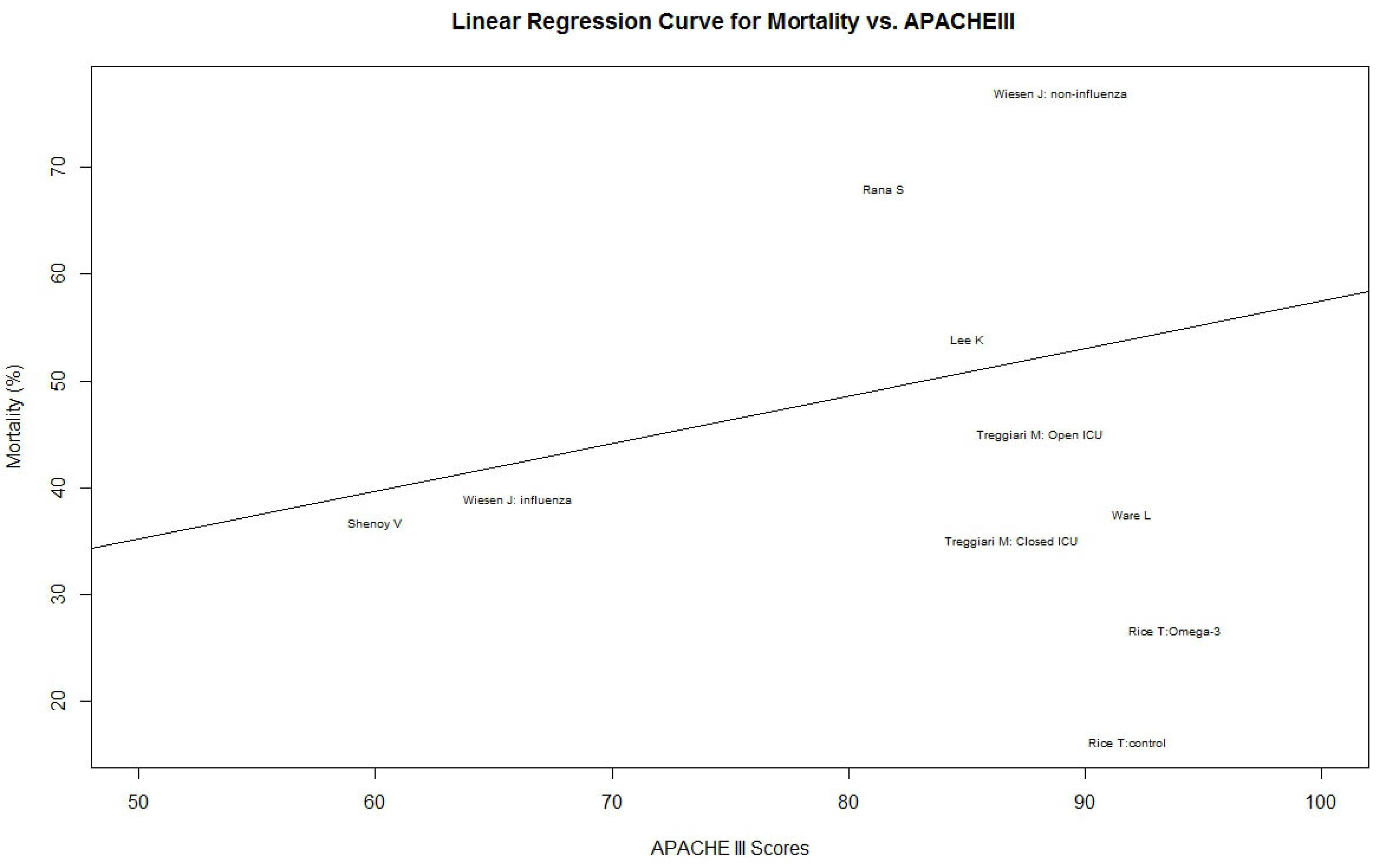
3.3. An Advanced Heterogeneity Test: O/E Ratio
| ALT Study | APACHE III | Sample size | Mortality (%) |
|---|---|---|---|
| Shenoy, V. [45] | 60 | 30 | 36.7 |
| Wiesen, J.: Influenza [46] | 66 | 23 | 39.0 |
| Wiesen, J.: Non-influenza [46] | 89 | 22 | 77.0 |
| Lee, K.[47] | 85 | 50 | 54.0 |
| Treggiari, M.: Open ICU [48] | 88.1 | 391 | 45.0 |
| Treggiari, M.: Closed ICU [48] | 86.9 | 684 | 35.0 |
| Rana, S.[49] | 81.5 | 38 | 68.0 |
| Ware, L.[50] | 92 | 528 | 37.5 |
| Rice, T.: Omega-3[13] | 93.8 | 143 | 26.6 |
| Rice, T.: Control [13] | 91.8 | 129 | 16.3 |


4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nestel, P.J. Fish oil and cardiovascular disease: Lipids and arterial function. Am. J. Clin. Nutr. 2000, 71, 228–231. [Google Scholar]
- Urakaze, M.; Hamazaki, T.; Makuta, M.; Ibuki, F.; Kobayashi, S.; Yano, S.; Kumagai, A. Infusion of fish oil emulsion: Effects on platelet aggregation and fatty acid composition in phospholipids of plasma, platelets, and red blood cell membranes in rabbits. Am. J. Clin. Nutr. 1987, 46, 936–942. [Google Scholar]
- Rizos, E.C.; Ntzani, E.E.; Bika, E.; Kostapanos, M.S.; Elisaf, M.S. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events a systematic review and meta-analysis. JAMA 2012, 308, 1024–1033. [Google Scholar] [CrossRef]
- Gerber, P.A.; Gouni-Berthold, I.; Kaspar, B. Omega-3 fatty acids: Role in metabolism and cardiovascular disease. Curr. Pharm. Des. 2013, 19, 3074–3093. [Google Scholar] [CrossRef]
- Poppitt, S.D.; Howe, C.A.; Lithander, F.E.; Silvers, K.M.; Lin, R.B.; Croft, J.; Ratnasabapathy, Y.; Gibson, R.A.; Anderson, C.S. Effects of moderate-dose omega-3 fish oil on cardiovascular risk factors and mood after ischemic stroke: A randomized, controlled trial. Stroke 2009, 40, 3485–3492. [Google Scholar] [CrossRef]
- Kremer, J.M. Effects of modulation of inflammatory and immune parameters in patients with rheumatic and inflammatory disease receiving dietary supplementation of n-3 and n-6 fatty acids. Lipids 1996, 31, 243–247. [Google Scholar] [CrossRef]
- Jiang, H.; Jiang, Z.M.; Luo, B.; Shuai, X.; Li, Y.P. Immunonutrition for clinical nutritional support: A systematic review based English and Chinese documents. Acta Acad. Med. Sin. 2002, 24, 554–558. [Google Scholar]
- Hayashi, N.; Tashiro, T.; Yamamori, H.; Takagi, K.; Morishima, Y.; Otsubo, Y. Effects of intravenous omega-3 and ω-6 fat emulsion on cytokine production and delayed type hypersensitivity in burned rats receiving total parenteral nutrition. JPEN 1998, 22, 363–367. [Google Scholar]
- Wei, C.; Hua, J.; Bin, C.; Karen, K. Impact of lipid emulsion containing fish oil on outcomes of surgical patients. Nutrition 2010, 26, 474–481. [Google Scholar] [CrossRef]
- Pacht, E.R.; DeMichele, S.J.; Nelson, J.L.; Hart, J.; Wennberg, A.K.; Gadek, J.E. Enteral nutrition with eicosapentaenoic acid, γ-linolenic acid, and antioxidants reduces alveolar inflammatory mediators and protein influx in patients with acute respiratory distress syndrome. Crit. Care Med. 2003, 31, 491–500. [Google Scholar] [CrossRef]
- Wang, X.; Li, W.; Li, N.; Li, J. Omega-3 fatty acids-supplemented parenteral nutrition decreases hyperinflammatory response and attenuates systemic disease sequelae in severe acute pancreatitis: A randomized and controlled study. JPEN 2008, 32, 236–241. [Google Scholar] [CrossRef]
- Friesecke, S.; Lotze, C.; Köhler, J.; Heinrich, A.; Felix, S.B.; Abel, P. Fish oil supplementation in the parenteral nutrition of critically ill medical patients: A randomized controlled trial. Intens. Care Med. 2008, 34, 1411–1420. [Google Scholar] [CrossRef]
- Rice, T.; Wheeler, A.P.; Thompson, B.T.; deBoisblanc, B.P.; Steingrub, J.; Pock, P. Enteral omega-3 fatty acid, -linolenic acid, and antioxidant supplementation in acute lung injury. JAMA 2011, 306, 1574–1581. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews for Interventions. version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available online: http://www.cochrane-handbook.org (accessed on 30 December,2013).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary. Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Jiang, H.; Sun, M.; Hefright, B.; Chen, W.; Lu, C.D.; Zeng, J. Efficacy of hypocaloric parenteral nutrition for surgical patients. Clin. Nutr. 2011, 30, 730–737. [Google Scholar] [CrossRef]
- Balasubramanian, S.P.; Wiener, M.; Alshameeri, Z.; Tiruvoipati, R.; Elbourne, D.; Reed, M.W. Standards of reporting of randomized controlled trials in general surgery. Ann. Surg. 2006, 244, 663–667. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Breslow, N.E.; Day, N.E. Statistical methods in cancer research: The design and analysis of cohort studies. IARC Sci. Publ. 1987, 82, 69. [Google Scholar]
- Shafi, S.; Ahn, C.; Parks, J.; Nathens, A.B.; Cryer, H.M.; Gentilello, L.M.; Hemmila, M.; Fildes, J.J. Quality of care within a trauma center is not altered by injury type. J. Trauma 2010, 68, 716–720. [Google Scholar]
- Cai, B.; Jiang, H.; Yang, H. Using Meta-regression algorithm to evaluate heterogeneity of systematic reviews of clinical nutrition support for burn. Chin. J. Burns 2013, 29, 344–348. [Google Scholar]
- Review Manager (RevMan) [Computer program]. version 5.2; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, 2012.
- David, M.; Alessandro, L.; Jennifer, T.; Douglas, G.A.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLOS. Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Gadek, J.E.; DeMichele, S.J.; Karlstad, M.D.; Pacht, E.R. Effect of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in patients with acute respiratory distress syndrome. Crit. Care Med. 1999, 27, 1409–1420. [Google Scholar] [CrossRef]
- Grecu, I.; Mirea, L.; Grintescu, I. Parenteral fish oil supplementation in patients with abdominal sepsis. Clin. Nutr. 2003, 22, 23S. [Google Scholar] [CrossRef]
- Mayer, K.; Gokorsch, S.; Fegbeutel, C. Parenteral nutrition with fish oil modulates cytokine response in patients with sepsis. Am. J. Respir. Crit. Care. Med. 2003, 167, 1321–1328. [Google Scholar] [CrossRef]
- Pontes-Arruda, A.; Aragão, A.M.; Albuquerque, J.D. Effects of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanically ventilated patients with severe sepsis and septic shock. Crit. Care. Med. 2006, 34, 2325–2333. [Google Scholar] [CrossRef]
- Singer, P.; Theilla, M.; Fisher, H.; Gibstein, L.; Grozovski, E.; Cohen, J. Benefit of an enteral diet enriched with eicosapentaenoic acid and gamma-linolenic acid in ventilated patients with acute lung injury. Crit. Care. Med. 2006, 34, 1033–1038. [Google Scholar] [CrossRef]
- Barbosa, V.M.; Miles, E.A.; Calhau, C.; Lafuente, E.; Calder, P.C. Effects of a fish oil containing lipid emulsion on plasma phospholipid fatty acids, inflammatory markers, and clinical outcomes in septic patients: A randomized, controlled clinical trial. Crit. Care 2010, 14, R5. [Google Scholar] [CrossRef]
- Grau-Carmona, T.; Morán-García, V.; García-de-Lorenzo, A.; Heras-de-la-Calle, G.; Quesada-Bellver, B.; López-Martínez, J. Effect of an enteral diet enriched with eicosapentaenoic acid, gamma-linolenic acid and anti-oxidants on the outcome of mechanically ventilated, critically ill septic patients. Clin. Nutr. 2011, 30, 578–584. [Google Scholar] [CrossRef]
- Gupta, A.; Govil, D.; Bhatnagar, S.; Gupta, S.; Goyal, J.; Patel, S. Efficacy and safety of parenteral omega 3 fatty acids in ventilated patients with acute lung injury. Indian. J. Crit. Care Med. 2011, 15, 108–113. [Google Scholar]
- Stapleton, R.D.; Martin, T.R.; Weiss, N.S.; Crowley, J.J.; Gundel, S.J.; Nathens, A.B. A phase II randomized placebo-controlled trial of omega-3 fatty acids for the treatment of acute lung injury. Crit. Care. Med. 2011, 39, 1655–1662. [Google Scholar] [CrossRef]
- Heller, A.R.; Rossler, S.; Litz, R.J.; Stehr, S.N.; Heller, S.C.; Koch, R. Omega-3 fatty acids improve the diagnosis-related clinical outcome. Crit. Care. Med. 2006, 34, 972–979. [Google Scholar] [CrossRef]
- Barros, K.V.; Cassulino, A.P.; Schalch, L.; Della, V.; Munhoz, E.; Manetta, J.A.; Noakes, P.S.; Miles, E.A.; Calder, P.C.; Flor Silveira, V.L. Supplemental intravenous n-3 fatty acids and n-3 fatty acid status and outcome in critically ill elderly patients in the ICU receiving enteral nutrition. Clin. Nutr. 2013, 32, 599–605. [Google Scholar] [CrossRef]
- Chen, J.; Guo, K.; Wang, H.; Lin, W. An applied study of lipid emulsion containing fish oil in nutrition support for ventilated patients. J. Clin. Pulmon. Chin. 2011, 16, 1251–1252. [Google Scholar]
- Zhang, W.; Yang, L.; Sun, Q. Efficacy of lipid emulsion containing fish oil on parenteral nutrition of acute severe pancreatitis. Shan Xi Med. J. Chin. 2012, 41, 367–369. [Google Scholar]
- Han, Y.Y.; Lai, S.L.; Ko, W.J.; Choi, C.H.; Lai, S.H. Effects of fish oil on inflammatory modulation in surgical intensive care unit patients. JPEN 2012, 27, 91–98. [Google Scholar]
- Theilla, M.; Singer, P.; Cohen, J.; Dekeyser, F. A diet enriched in eicosapentanoic acid, gamma-linolenic acid and antioxidants in the prevention of new pressure ulcer formation in critically ill patients with acute lung injury: A randomized, prospective, controlled study. Clin. Nutr. 2007, 26, 752–757. [Google Scholar] [CrossRef]
- Zhang, J.; Liang, H.; Zhang, L. Effects of fish oil parenteral nutrition on serum CRP and MIF levels in multiple trauma patients. J. Trauma Surg. Chin. 2009, 11, 144–146. [Google Scholar]
- Xiong, J.; Zhu, S.; Zhou, Y.; Wu, H.; Wang, C. Regulation of omega-3 fish oil emulsion on the SIRS during the initial stage of severe acute pancreatitis. J. Huazhong Univ. Sci. Technol. Med. Sci. 2009, 29, 35–38. [Google Scholar] [CrossRef]
- Sungurtekin, H.; Değirmenci, S.; Sungurtekin, U.; Oguz, B.E.; Sabir, N.; Kaptanoglu, B. Comparison of the effects of different intravenous fat emulsions in patients with systemic inflammatory response syndrome and sepsis. Nutr. Clin. Pract. 2011, 26, 665–671. [Google Scholar] [CrossRef]
- Khor, B.S.; Liaw, S.J.; Shih, H.C.; Wang, L.S. Randomized, double blind, placebo-controlled trial of fish-oil-based lipid emulsion infusion for treatment of critically ill patients with severe sepsis. Asian J. Surg. 2011, 34, 1–10. [Google Scholar] [CrossRef]
- Sabater, J.; Masclans, J.R.; Sacanell, J.; Chacon, P.; Sabin, P.; Planas, M. Effects of an omega-3 fatty acid-enriched lipid emulsion on eicosanoid synthesis in acute respiratory distress syndrome (ARDS): A prospective, randomized, double-blind, parallel group study. Nutr. Metab. (Lond.) 2011, 8, 22. [Google Scholar] [CrossRef]
- Sabater, J.; Masclans, J.R.; Sacanell, J.; Chacon, P.; Sabin, P.; Planas, M. Effects on hemodynamics and gas exchange of omega-3 fatty acid-enriched lipid emulsion in acute respiratory distress syndrome (ARDS): A prospective, randomized, double-blind, parallel group study. Lipids Health Dis. 2008, 7, 39. [Google Scholar] [CrossRef]
- Shenoy, V.V.; Nagar, V.S.; Chowdhury, A.A.; Bhalgat, P.S.; Juvale, N.I. Pulmonary leptospirosis: An excellent response to bolus methylprednisolone. Postgrad. Med. J. 2006, 82, 602–606. [Google Scholar] [CrossRef]
- Wiesen, J.; Komara, J.J.; Walker, E.; Wiedemann, H.P.; Guzman, J.A. Relative cost and outcomes in the intensive care unit of acute lung injury (ALI) due to pandemic influenza compared with other etiologies: A single-center study. Ann. Intens. Care 2012, 2, 41. [Google Scholar] [CrossRef]
- Lee, K.A.; Gong, M.N. Pre-B-cell colony-enhancing factor and its clinical correlates with acute lung injury and sepsis. Chest 2011, 140, 382–390. [Google Scholar] [CrossRef]
- Treggiari, M.M.; Martin, D.P.; Yanez, N.D.; Caldwell, E.; Hudson, L.D.; Rubenfeld, G.D. Effect of intensive care unit organizational model and structure on outcomes in patients with acute lung injury. Am. J. Respir. Crit. Care. Med. 2007, 176, 685–690. [Google Scholar] [CrossRef]
- Rana, S.; Jenad, H.; Gay, P.C.; Buck, C.F.; Hubmayr, R.D.; Gajic, O. Failure of non-invasive ventilation in patients with acute lung injury: Observational cohort study. Crit. Care 2006, 10, R79. [Google Scholar] [CrossRef]
- Ware, L.B.; Koyama, T.; Billheimer, D.D.; Wu, W.; Bernard, G.R.; Thompson, B.T. Prognostic and pathogenetic value of combining clinical and biochemical indices in patients with acute lung injury. Chest 2010, 137, 288–296. [Google Scholar] [CrossRef]
- Rice, T.; Vanderbilt University School of Medicine, Nashville, TN, USA. Personnel Communication, May 2013.
- Villet, S.; Chiolero, R.L.; Bollmann, M.D. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef]
- Faisy, C.; Lerolle, N.; Dachraoui, F.; Savard, J.F.; Abboud, I.; Tadie, J.M.; Fagon, J.Y. Impact of energy deficit calculated by a predictive method on outcome in medical patients requiring prolonged acute mechanical ventilation. Br. J. Nutr. 2009, 101, 1079–1087. [Google Scholar] [CrossRef]
- Singera, P.; Pichardb, C.; Heideggerb, C.P.; Wernermanc, J. Considering energy deficit in the intensive care unit. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 170–176. [Google Scholar] [CrossRef]
- Heidegger, C.P.; Berger, M.M.; Graf, S.; Zingg, W.; Darmon, P.; Costanza, M.C.; Thibault, R.; Pichard, C. Optimisation of energy provision with supplemental parenteral nutrition in critically ill patients: A randomised controlled clinical trial. Lancet 2013, 381, 385–393. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chen, W.; Jiang, H.; Zhou, Z.-Y.; Tao, Y.-X.; Cai, B.; Liu, J.; Yang, H.; Lu, C.D.; Zeng, J. Is Omega-3 Fatty Acids Enriched Nutrition Support Safe for Critical Ill Patients? A Systematic Review and Meta-Analysis. Nutrients 2014, 6, 2148-2164. https://doi.org/10.3390/nu6062148
Chen W, Jiang H, Zhou Z-Y, Tao Y-X, Cai B, Liu J, Yang H, Lu CD, Zeng J. Is Omega-3 Fatty Acids Enriched Nutrition Support Safe for Critical Ill Patients? A Systematic Review and Meta-Analysis. Nutrients. 2014; 6(6):2148-2164. https://doi.org/10.3390/nu6062148
Chicago/Turabian StyleChen, Wei, Hua Jiang, Zhi-Yuan Zhou, Ye-Xuan Tao, Bin Cai, Jie Liu, Hao Yang, Charles Damien Lu, and Jun Zeng. 2014. "Is Omega-3 Fatty Acids Enriched Nutrition Support Safe for Critical Ill Patients? A Systematic Review and Meta-Analysis" Nutrients 6, no. 6: 2148-2164. https://doi.org/10.3390/nu6062148
APA StyleChen, W., Jiang, H., Zhou, Z.-Y., Tao, Y.-X., Cai, B., Liu, J., Yang, H., Lu, C. D., & Zeng, J. (2014). Is Omega-3 Fatty Acids Enriched Nutrition Support Safe for Critical Ill Patients? A Systematic Review and Meta-Analysis. Nutrients, 6(6), 2148-2164. https://doi.org/10.3390/nu6062148