Oral Zinc Supplementation Decreases the Serum Iron Concentration in Healthy Schoolchildren: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Ethics Approval
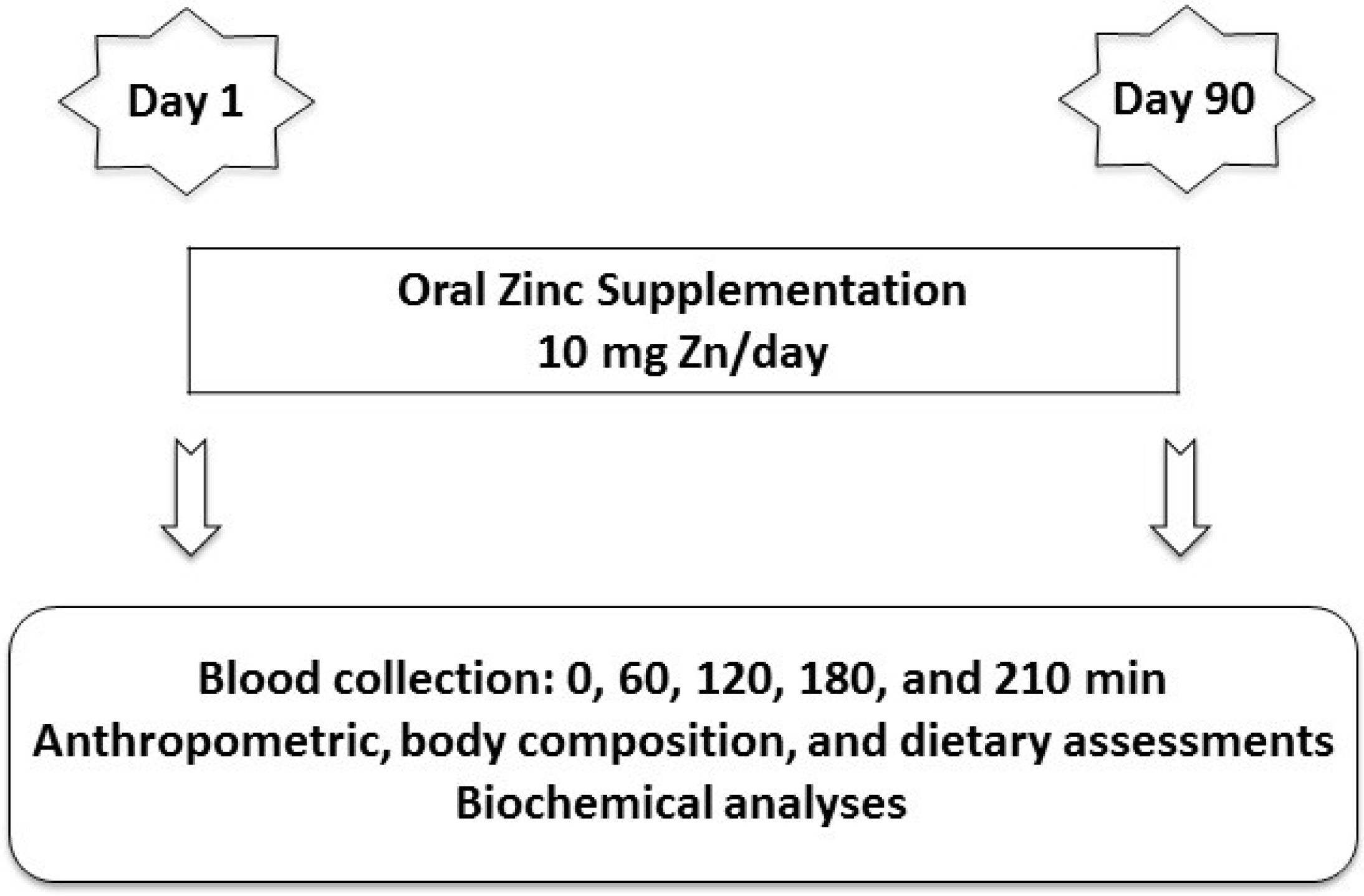
2.3. Experimental Design

2.4. Anthropometric and Body Composition Assessments
2.5. Dietetic Assessment
2.6. Oral Zinc Supplementation
2.7. Chemicals, Materials and Laboratory Procedures
2.8. Statistical Analyses
3. Results
3.1. Subjects
3.2. Anthropometric and Body Composition Assessments

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | Experimental | ||||
|---|---|---|---|---|---|---|
| Before | After | p Values | Before | After | p Values | |
| BMI (kg/m2) | 16.29 ± 0.40 | 16.60 ± 0.43 | 0.0424 * | 16.06 ± 0.45 | 16.30 ± 0.45 | 0.0243 * |
| Hemoglobin (g/dL) | 11.7 ± 0.18 | 11.7 ± 0.20 | 0.6829 | 11.6 ± 0.16 | 11.6 ± 0.17 | 0.7843 |
| MCV (fL) | 86.96 ± 0.99 | 84.88 ± 1.45 | 0.4973 | 85.55 ± 1.32 | 84.99 ± 1.06 | 0.7486 |
| Ferritin (ng/mL) | 29.9 ± 2.75 | 34.2 ± 3.53 | 0.3517 | 37.1 ± 3.25 | 34.0 ± 3.54 | 0.3415 |
| Transferrin (mg/dL) | 233 ± 7.22 | 238 ± 7.51 | 0.8904 | 229.1 ± 8.74 | 223.4 ± 6.22 | 0.2524 |
| Transferrin saturation (%) | 33.6 ± 1.12 | 32.6 ± 1.28 | 0.6224 | 34.7 ± 1.28 | 34.2 ± 1.36 | 0.7244 |
| Ceruloplasmin (mg/dL) | 31.2 ± 1.82 | 32.4 ± 1.53 | 0.5591 | 30.1 ± 1.58 | 27.6 ± 1.17 | 0.1367 |
| Total protein (g/dL) | 6.67 ± 0.26 | 6.49 ± 0.20 | 0.5511 | 6.54 ± 0.18 | 6.59 ± 0.18 | 0.8573 |
3.3. Dietetic Assessment
| Parameter | Before Supplementation | After Supplementation | p Values | Reference Values |
|---|---|---|---|---|
| Energy (kcal) | 6–9 years (boys): 1573–1978 kcal/day [16] 6–9 years (girls): 1428–1854 kcal/day [16] | |||
| Control group | 1562 ± 48.02 | 1566 ± 47.70 | 0.3090 | |
| Experimental group | 1617 ± 55.52 | 1796 ± 58.30 | 0.0002 ** | |
| Protein (g) | 4–8 years (both sexes): 0.76 g/kg/day [18] 9–13 years (both sexes): 0.76 g/kg/day [18] | |||
| Control group | 40.29 ± 0.55 | 40.56 ± 0.53 | 0.0292 * | |
| Experimental group | 41.13 ± 0.68 | 47.06 ± 0.61 | <0.0001 ** | |
| Fat (g) | ND [18] | |||
| Control group | 35.92 ± 0.62 | 36.11 ± 0.62 | 0.0145 * | |
| Experimental group | 36.46 ± 0.49 | 45.09 ± 2.44 | 0.0015 ** | |
| Carbohydrate (g) | 100 g/day [18] | |||
| Control group | 183 ± 2.61 | 183.4 ± 2.58 | 0.1232 | |
| Experimental group | 183.3 ± 4.56 | 180.8 ± 4.43 | <0.0001 ** | |
| Fiber (g) | 4–8 years (both sexes): 25 g/day [18] 9–13 years (girls): 26 g/day [18] 9–13 years (boys): 31 g/day [18] | |||
| Control group | 10.70 ± 0.28 | 11.09 ± 0.28 | <0.0001 * | |
| Experimental group | 10.56 ± 0.25 | 11.71 ± 0.25 | <0.0001 ** | |
| Calcium (mg) | 4–8 years (both sexes): 800 mg/day [19] 9–13 years (both sexes): 1100 mg/day [19] | |||
| Control group | 630.90 ± 28.29 | 628.40 ± 23.69 | 0.7377 | |
| Experimental group | 587.80 ± 17.13 | 648.10 ± 14.53 | <0.0001 ** | |
| Iron (mg) | 4–8 years (both sexes): 4.1 mg/day [17] 9–13 years (boys): 5.9 mg/day [17] 9–13 years (girls): 5.7 mg/day [17] | |||
| Control group | 8.69 ± 0.18 | 8.79 ± 0.13 | 0.1489 | |
| Experimental group | 8.76 ± 0.08 | 9.34 ± 0.09 | <0.0001 ** | |
| Zinc (mg) | 4–8 years (both sexes): 4 mg/day [17] 9–13 years (both sexes): 7 mg/day [17] | |||
| Control group | 6.24 ± 0.13 | 6.51 ± 0.12 | <0.0001 * | |
| Experimental group | 5.96 ± 0.11 | 6.50 ± 0.11 | <0.0001 ** |
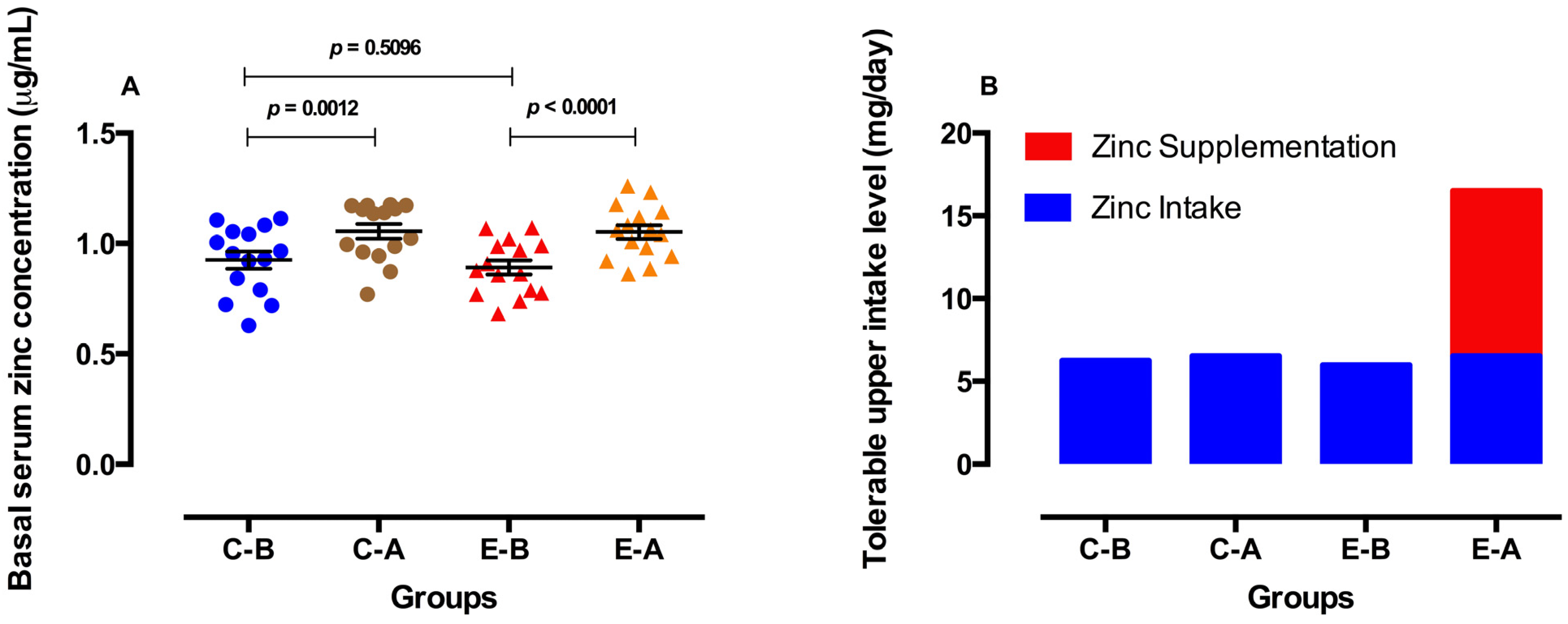
3.4. Zinc Parameters before and after Oral Zinc Supplementation

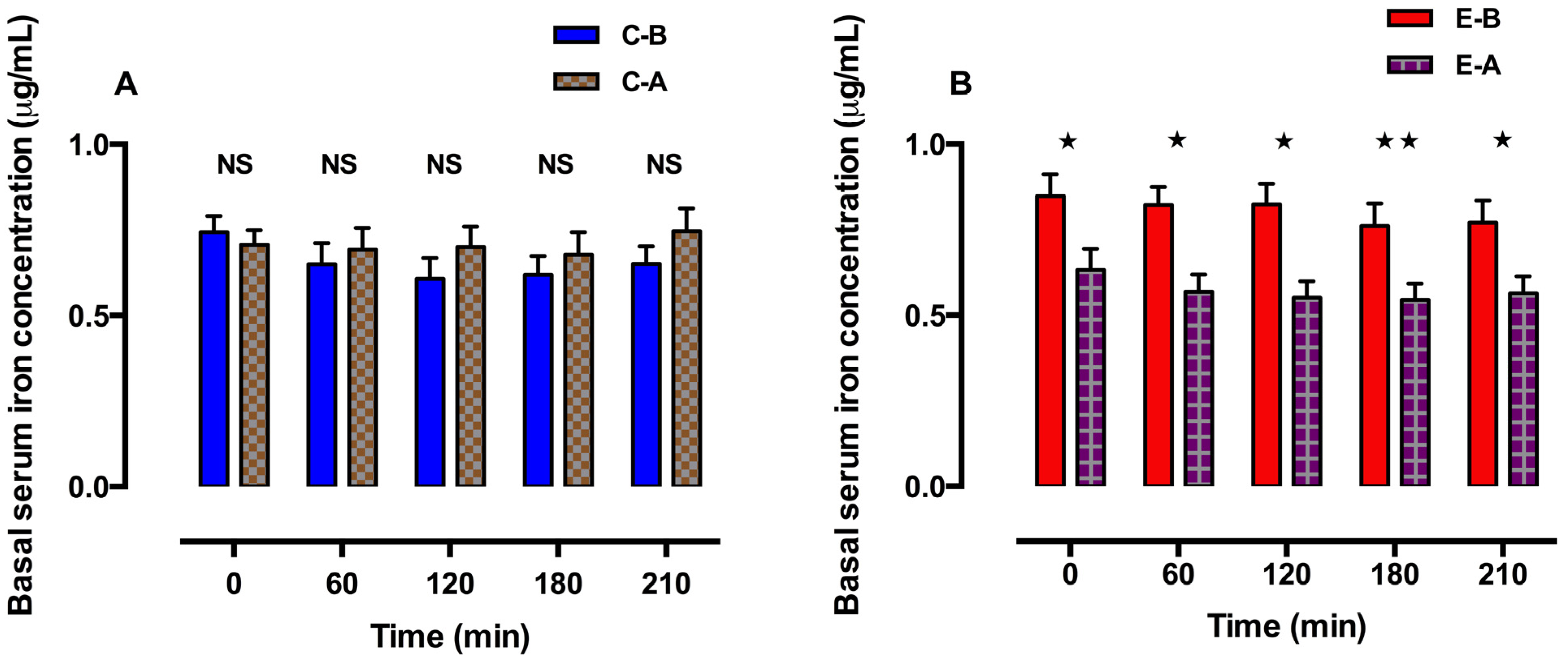
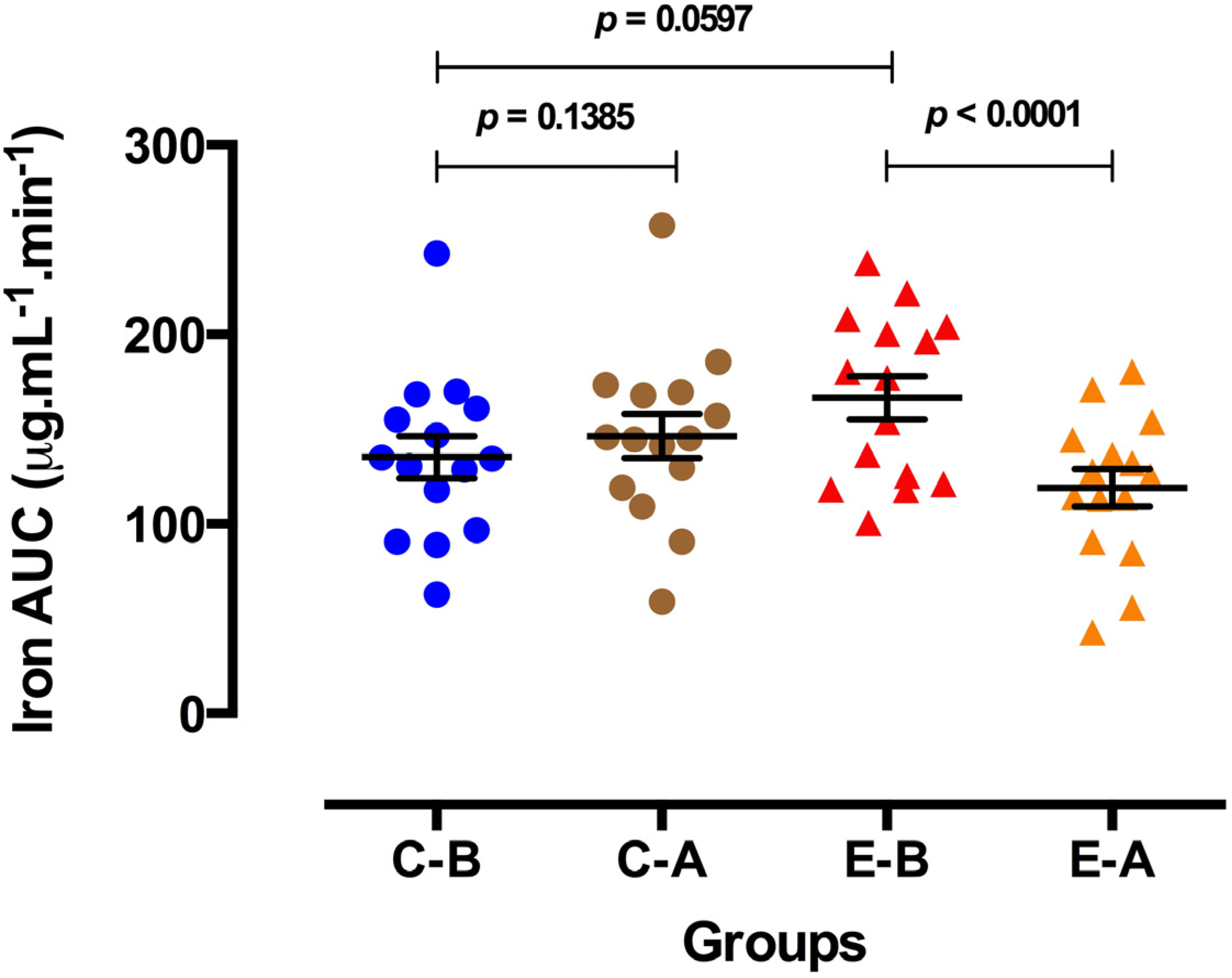
3.5. Iron Parameters before and after Oral Zinc Supplementation


3.6. Hematologic and Biochemical Analyses
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Yanagisawa, H. Zinc deficiency and clinical practice—Validity of zinc preparation. Yakugaku Zasshi 2008, 128, 333–339. [Google Scholar] [CrossRef]
- Labbé, R.F.; Dewanji, A. Iron assessment tests: Transferrin receptor vis-à-vis zinc protoporphyrin. Clin. Biochem. 2004, 37, 165–174. [Google Scholar]
- Baqui, A.H.; Zaman, K.; Persson, L.A.; El Arifeen, S.; Yunus, M.; Begum, N.; Black, R.E. Simultaneous weekly supplementation of iron and zinc is associated with lower morbidity due to diarrhea and acute lower respiratory infection in Bangldeshi infants. J. Nutr. 2003, 133, 4150–4157. [Google Scholar]
- Alves, C.X.; Vale, S.H.L.; Dantas, M.M.G.; Maia, A.A.; França, M.C.; Marchini, J.S.; Leite, L.D.; Brandao-Neto, J. Positive effects of zinc supplementation on growth, GH, IGF1, and IGFBP3 in eutrophic children. J. Pediatr. Endocrinol. Metab. 2012, 25, 881–887. [Google Scholar]
- Lind, T.; Lonnerdal, B.; Stenlund, H.; Ismail, D.; Seswandhana, R.; Ekstrom, E.C.; Persson, L.Å. A community-based randomized controlled trial of iron and zinc supplementation in Indonesian infants: Interactions between iron and zinc. Am. J. Clin. Nutr. 2003, 77, 883–890. [Google Scholar]
- Troost, F.J.; Brummer, R.J.M.; Dainty, J.R.; Hoogewerff, J.A.; Bull, V.J.; Saris, W.H.M. Iron supplements inhibit zinc but not copper absorption in vivo in ileostomy subjects. Am. J. Clin. Nutr. 2003, 78, 1018–1023. [Google Scholar]
- Wieringa, F.T.; Berger, J.; Dijkhuizen, M.A.; Hidayat, A.; Ninh, N.X.; Utomo, B.; Wasantwisut, E.; Winichagoon, P. SEAMTIZI (South-East Asia Multi-country Trial on Iron and Zinc Supplementation in Infants) Study Group. Combined iron and zinc supplementation in infants improved iron and zinc status, but interactions reduced efficacy in a multi-country trial in Southeast Asia. J. Nutr. 2007, 137, 466–471. [Google Scholar]
- Espinoza, A.; Le Blanc, S.; Olivares, M.; Pizarro, F.; Ruz, M.; Arredondo, M. Iron, copper, and zinc transport: Inhibition of divalent metal transporter 1 (DMT1) and human copper transporter 1 (hCTR1) by shRNA. Biol. Trace Elem. Res. 2012, 146, 281–286. [Google Scholar] [CrossRef]
- Iyengar, V.; Pullakhandam, R.; Nair, K.M. Coordinate expression and localization of iron and zinc transporters explain iron–zinc interactions during uptake in Caco-2 cells: Implications for iron uptake at the enterocyte. J. Nutr. Biochem. 2012, 23, 1146–1154. [Google Scholar] [CrossRef]
- Olivares, M.; Pizarro, F.; Ruz, M. New insights about iron bioavailability inhibition by zinc. Nutrition 2007, 23, 292–295. [Google Scholar] [CrossRef]
- Antunes, M.F.R.; Leite, L.D.; Rocha, E.D.M.; Brito, N.J.N.; França, M.C.; Silva, C.A.B.; Almeida, M.G.; Rezende, A.A.; Marchini, J.S.; Brandão-Neto, J. Competitive interaction of zinc and iron after venous and oral zinc administration in eutrophic children. Trace Elem. Electrolytes 2010, 27, 185–191. [Google Scholar] [CrossRef]
- Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- WHO. Growth Reference Data for 5–19 Years. World Health Organization: Geneva, Switzerland, 2007. Available online: http://www.who.int/growthref/en/ (accessed on 15 October 2012).
- UNIFESP. Programa de Apoio à Nutrição. Universidade Federal de São Paulo: São Paulo, Brzazil, 2007. Available online: http://sourceforge.net/projects/nutwin/ (accessed on 12 June 2013).
- UNICAMP. Núcleo de Estudos e Pesquisas em Alimentação (NEPA): Tabela Brasileira de Composição de Alimentos (TACO); Universidade Estadual de Campinas, NEPA-UNICAMP: Campinas, Brazil, 2011. [Google Scholar]
- Human Energy Requirements. Available online: http://www.fao.org/docrep/007/y5686e/y5686e00.htm (accessed on 10 June 2013).
- Food and Nutrition Board; Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; The National Academies Press: Washington, DC, USA, 2003. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes (DRIs) for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Food and Nutrition Board; Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Lowe, N.M.; Fekete, K.; Decsi, T. Methods of assessment of zinc status in humans: A systematic Review. Am. J. Clin. Nutr. 2009, 89, S2040–S2051. [Google Scholar] [CrossRef]
- Sandström, B. Micronutrient interactions: Effects on absorption and bioavailability. Br. J. Nutr. 2001, 85, S181–S185. [Google Scholar]
- Olivares, M.; Pizarro, F.; Ruz, M.; López de Romaña, D. Acute inhibition of iron bioavailability by zinc: Studies in humans. Biometals 2012, 25, 657–664. [Google Scholar] [CrossRef]
- Olivares, M.; Pizarro, F.; Ruz, M. Zinc inhibits nonheme iron bioavailability in humans. Biol. Trace Elem. Res. 2007, 117, 7–14. [Google Scholar] [CrossRef]
- Iyengar, V.; Pullakhandam, R.; Nair, K.M. Dietary ligands as determinants of iron–zinc interactions at the absorptive enterocyte. J. Food Sci. 2010, 75, H260–H264. [Google Scholar] [CrossRef]
- Zaman, K.; McArthur, J.O.; Abboud, M.N.; Ahmad, Z.I.; Garg, M.L.; Petocz, P.; Samman, S. Iron supplementation decreases plasma zinc but has no effect on plasma fatty acids in non-anemic women. Nutr. Res. 2013, 33, 272–278. [Google Scholar] [CrossRef]
- Rossander-Hultén, L.; Brune, M.; Sandstroöm, B.; Loönnerdal, B.; Hallberg, L. Competitive inhibition of iron absorption by manganese and zinc in humans. Am. J. Clin. Nutr. 1991, 54, 152–156. [Google Scholar]
- Davidsson, L.; Almgren, A.; Sandström, B.; Hurrell, R.F. Zinc absorption in adult humans: The effect of iron fortification. Br. J. Nutr. 1995, 74, 417–425. [Google Scholar] [CrossRef]
- Oliveira, K.J.F.; Donangelo, C.M.; Oliveira, A.V., Jr.; Silveira, C.L.P.; Koury, J.C. Effect of zinc supplementation on the antioxidant, copper, and iron status of physically active adolescents. Cell Biochem. Funct. 2009, 27, 162–166. [Google Scholar]
- Herman, S.; Griffin, I.J.; Suwarti, S.; Ernawati, F.; Permaesih, D.; Pambudi, D.; Abrams, S.A. Cofortification of iron-fortified flour with zinc sulfate, but not zinc oxide, decreases iron absorption in Indonesian children. Am. J. Clin. Nutr. 2002, 76, 813–817. [Google Scholar]
- Kordas, K.; Stoltzfus, R.J. New evidence of iron and zinc interplay at the enterocyte and neural tissues. J. Nutr. 2004, 134, 1295–1298. [Google Scholar]
- Garrick, M.D.; Singleton, S.T.; Vargas, F.; Kuo, K.C.; Zhao, L.; Knopfel, M.; Davidson, T.; Costa, M.; Paradkar, P.; Roth, J.A.; et al. DMT1: Which metals does it transport? Biol. Res. 2006, 39, 79–85. [Google Scholar]
- Pinilla-Tenas, J.J.; Sparkman, B.K.; Shawki, A.; Illing, A.C.; Mitchell, C.J.; Zhao, N.; Liuzzi, J.P.; Cousins, R.J.; Knutson, M.D.; Mackenzie, B. Zip14 is a complex broad-scope metal-ion transporter whose functional properties support roles in the cellular uptake of zinc and nontransferrin-bound iron. Am. J. Physiol. Cell Physiol. 2011, 301, C862–C871. [Google Scholar]
- Dekker, L.H.; Villamor, E. Zinc supplementation in children is not associated with decreases in hemoglobin concentrations. J. Nutr. 2010, 140, 1035–1040. [Google Scholar] [CrossRef]
- Fahmida, U.; Rumawas, J.S.; Utomo, B.; Patmonodewo, S.; Schultink, W. Zinc-iron, but not zinc-alone supplementation, increased linear growth of stunted infants with low haemoglobin. Asia Pac. J. Clin. Nutr. 2007, 16, 301–309. [Google Scholar]
- Donangelo, C.M.; Woodhouse, L.R.; King, S.M.; Viteri, F.E.; King, J.C. Supplemental zinc lowers measures of iron status in young women with low iron reserves. J. Nutr. 2002, 132, 1860–1864. [Google Scholar]
- Purchase, R. The treatment of Wilson’s disease, a rare genetic disorder of copper metabolism. Sci. Prog. 2013, 96, 19–32. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
De Brito, N.J.N.; Rocha, É.D.; De Araújo Silva, A.; Costa, J.B.S.; França, M.C.; Das Graças Almeida, M.; Brandão-Neto, J. Oral Zinc Supplementation Decreases the Serum Iron Concentration in Healthy Schoolchildren: A Pilot Study. Nutrients 2014, 6, 3460-3473. https://doi.org/10.3390/nu6093460
De Brito NJN, Rocha ÉD, De Araújo Silva A, Costa JBS, França MC, Das Graças Almeida M, Brandão-Neto J. Oral Zinc Supplementation Decreases the Serum Iron Concentration in Healthy Schoolchildren: A Pilot Study. Nutrients. 2014; 6(9):3460-3473. https://doi.org/10.3390/nu6093460
Chicago/Turabian StyleDe Brito, Naira Josele Neves, Érika Dantas Rocha, Alfredo De Araújo Silva, João Batista Sousa Costa, Mardone Cavalcante França, Maria Das Graças Almeida, and José Brandão-Neto. 2014. "Oral Zinc Supplementation Decreases the Serum Iron Concentration in Healthy Schoolchildren: A Pilot Study" Nutrients 6, no. 9: 3460-3473. https://doi.org/10.3390/nu6093460
APA StyleDe Brito, N. J. N., Rocha, É. D., De Araújo Silva, A., Costa, J. B. S., França, M. C., Das Graças Almeida, M., & Brandão-Neto, J. (2014). Oral Zinc Supplementation Decreases the Serum Iron Concentration in Healthy Schoolchildren: A Pilot Study. Nutrients, 6(9), 3460-3473. https://doi.org/10.3390/nu6093460