To Legislate or Not to Legislate? A Comparison of the UK and South African Approaches to the Development and Implementation of Salt Reduction Programs



Abstract
:1. Introduction
2. The UK’s Voluntary Approach to Salt Reduction
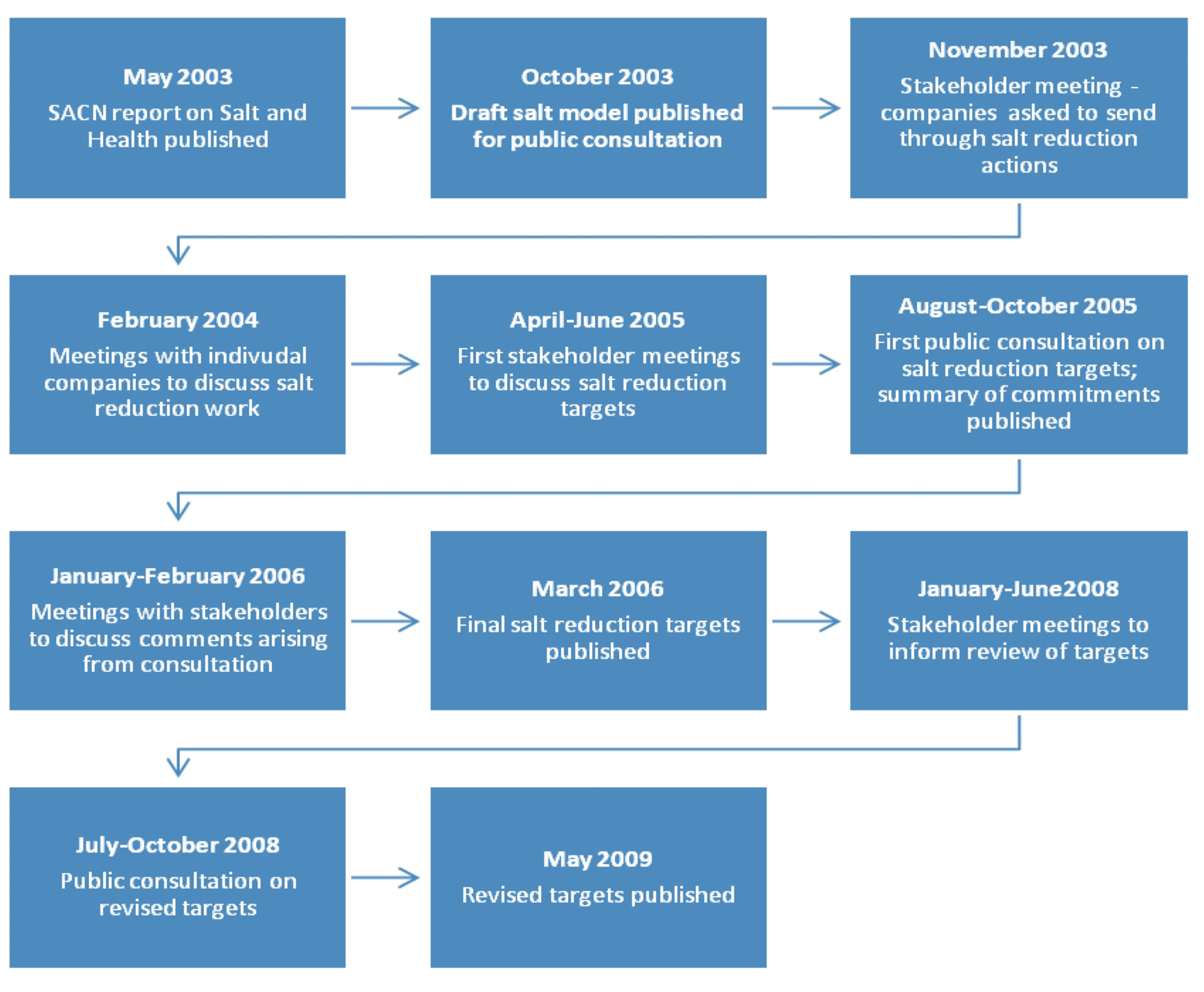
2.1. Overview of the United Kingdom’s Salt Reduction Target Process
2.1.1. Development of the Salt Model
2.1.2. Engaging the Food Industry
2.1.3. Stakeholder Forum and Industry Consultation

2.1.4. Cross-Sector Collaborations
2.1.5. Developing Targets for Salt Levels in Foods
2.1.6. Impact of the UK Salt Reduction Campaign
2.2. South Africa’s Legislative Approach to Salt Reduction
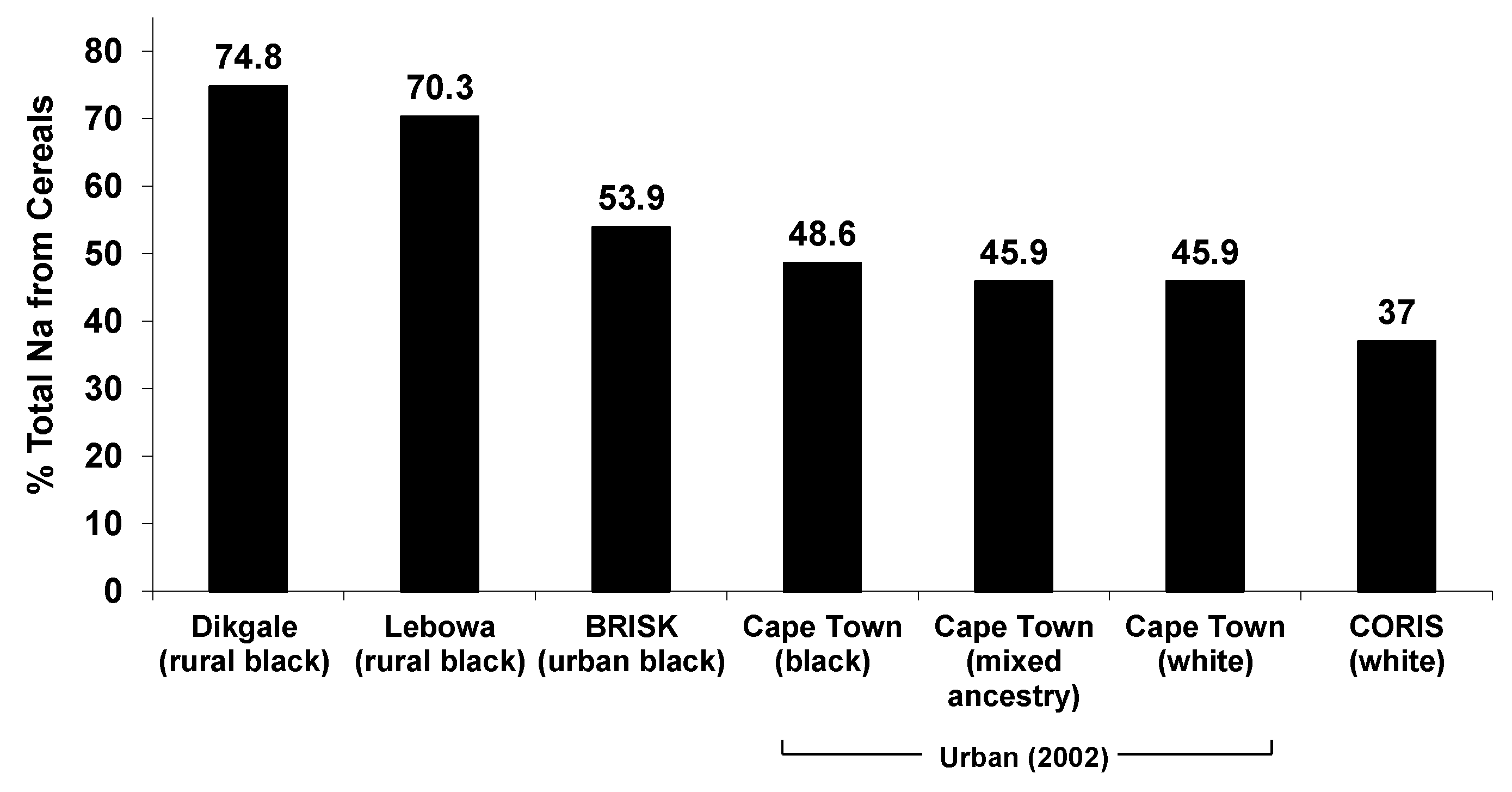
2.2.1. Estimating Salt Intake Levels
2.2.2. Identifying Contribution of Different Processed Foods to Salt in the Diet


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | Food item | % Total Na+ intake | ||
|---|---|---|---|---|
| Black n = 110 | Mixed ancestry n = 112 | White n = 103 | ||
| Bread, all types | 40.54 | 30.70 | 25.18 | |
| 1 | Bread/rolls, white | 22.26 | 22.03 | 15.24 |
| 2 | Bread/rolls, brown | 17.27 | 6.68 | 5.74 |
| Bread/rolls, whole wheat | 1.01 | 1.99 | 4.20 | |
| 3 | Beef sausage, boerewors | 4.15 | 6.62 | 2.43 |
| 4 | Steak and kidney pie (commercial) | 3.42 | 1.29 | 1.70 |
| 5 | Soup powder (reconstituted) | 2.93 | - | - |
| 6 | Margarine, brick/hard | 2.90 | 1.89 | 1.51 |
| 7 | Polony | 2.53 | 2.17 | - |
| 8 | Maas/sour milk | 2.44 | - | - |
| 9 | Potato chips/French fries | 2.21 | 1.65 | 1.55 |
| 10 | Milk, full cream, fresh | 2.12 | 1.90 | 1.56 |
| 11 | Potato crisps | 1.96 | 2.73 | 1.30 |
| 12 | Popcorn, plain | 1.41 | - | - |
| 13 | Salami, pork/beef (Russian) | 1.38 | 0.97 | - |
| 14 | Sausage roll (commercial) | 1.38 | 0.91 | 0.91 |
| 15 | Breakfast cereal, all-bran flakes | 1.22 | 1.51 | 4.19 |
| 16 | Soup, vegetable (canned) | 1.19 | - | 1.51 |
| 17 | Vienna sausage (canned) | 1.14 | 1.14 | 2.55 |
| 18 | Chicken pie (commercial) | 1.13 | 1.13 | - |
| 19 | Aromat | 1.13 | - | - |
| 20 b | Breakfast cereal, corn flakes | - | 2.90 | 3.06 |
| Cheese, cheddar | 1.92 | 1.88 | ||
| Savoury snack, corn chips | - | 1.53 | - | |
| Fish biltong (salted, dried cod) | - | 1.19 | - | |
| Baked beans | - | 1.01 | - | |
| Sausage, pork | - | - | 1.93 | |
| Pizza | - | - | 1.76 | |
| Ham (cooked/canned) | - | - | 1.32 | |
| ProVita crackers | - | - | 1.30 | |
| Bacon fried, lean | - | - | 1.27 | |
| Low fat spread, polyunsaturated | - | - | 1.19 | |
2.2.3. Cross-Sector Collaborative Research (Industry-Government-Academia)

2.2.4. Establishing the Maximum Salt Levels for the Legislation
2.2.5. Impact of the South Africa Salt Reduction Campaign

| South Africa food category | South Africa maximum sodium (mg) per 100 g foodstuff by 30 June 2016 and 2019 [18] | UK voluntary average and/or maximum sodium (mg) target per 100 g by 2017 [66] | |
|---|---|---|---|
| Bread | 400 (2016) 380 (2019) | 360 (average r) 450 (maximum) | |
| All breakfast cereals and porridges, whether ready-to-eat, instant or cook up, hot or cold | 500 (2016) 400 (2019) | 235 (average r) 400 (maximum) | |
| Spreads | Fat spread | 550 (2016) 450 (2019) | 425 (average r) 550 (maximum) |
| Butter spread | 550 (2016) 450 (2019) | Salted butters: 590 (average r) 670 (maximum) Lightly salted butters: 450 (average p) | |
| Ready-to-eat savoury snacks, excluding salt-and-vinegar flavoured savoury snacks | 800 (2016) 700 (2019) | Extruded and sheeted snacks: 680 (average r) 800 (maximum) | |
| Flavoured potato crisps, excluding salt-and-vinegar flavoured potato crisps | 650 (2016) 550 (2019) | 525 (average r) 580 (maximum) | |
| Flavoured, ready-to-eat, savoury snacks and potato crisps salt-and-vinegar only | 1000 (2016) 850 (2019) | 750 (average r) 1000 (maximum) | |
| Processed meat (Classes 6, 12 or 14 of the South African National Standard SANS 885:2011), uncured | 850 (2016) 650 (2019) | Cooked uncured meat—whole muscle: 270 (maximum) Reformed whole muscle: 360 (maximum) Comminuted or chopped reformed meat: 540 (maximum) Burger and grill steaks: 300 (average r) 350 (maximum) Frankfurters, canned hot dogs, canned burgers: 550 (average r) 700 (maximum) Fresh chilled frankfurters: 600 (average r) 750 (maximum) | |
| Processed meat (Classes 6, 12 or 14 of the South African National Standard SANS 885:2011), cured | 950 (2016) 850 (2019) | Ham/other cured meats: 650 (average p) | |
| Raw-processed meat sausages (all types) and similar products | 800 (2016) 600 (2019) | Sausages—all fresh, chilled or frozen: 450 (average r) 550 (maximum) Cooked sausage and sausage meat products: 550 (average r) 680 (maximum) | |
| Dry soup powder (not the instant type) | 5500 (2016) 3500 (2019) | Wet and dried soups as consumed 210 (average r) 250 (maximum) | |
| Dry gravy powders and dry instant savoury sauces | 3500 (2016) 1500 (2019) | All gravy as consumed: 380 (average r) 450 (maximum) | |
| Dry savoury powders with dry instant noodles to be mixed with a liquid | 1500 (2016) 800 (2019) | Noodles, plain and flavoured as consumed: 200 (average r) 350 (maximum) | |
| Stock cubes, stock powders, stock granules, stock emulsions, stock pastes or stock jellies | 18000 (2016) 13000 (2019) | Stocks as consumed: 300 (average r) 380 (maximum) | |
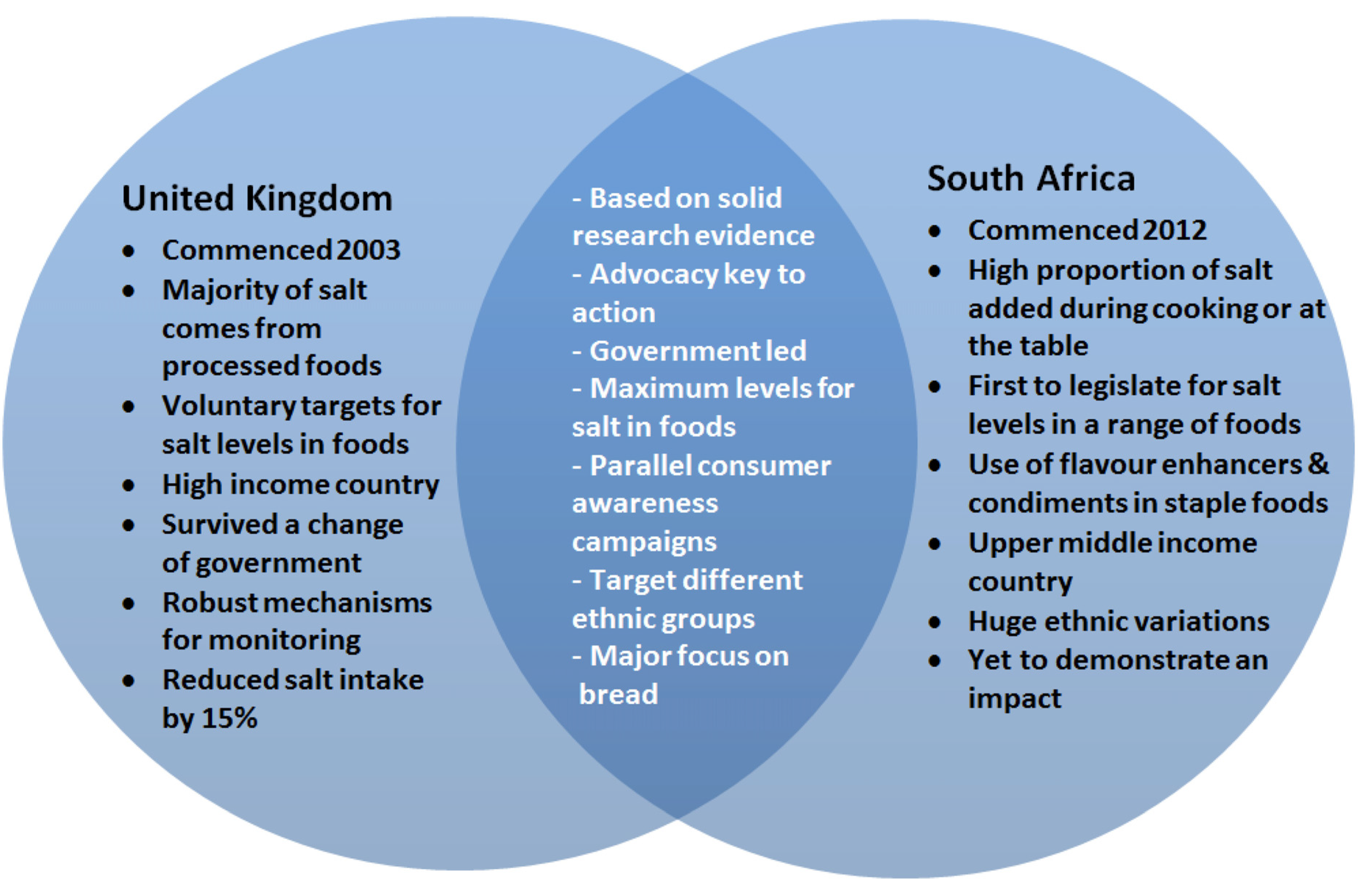
3. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Institute for Health Metrics and Evaluation (IHME). The Global Burden of Disease: Generating Evidence, Guiding Policy; University of Washington: Seattle, WA, USA, 2013. [Google Scholar]
- Murray, C.J.L.; Richards, M.A.; Newton, J.N.; Fenton, K.A.; Anderson, H.R.; Atkinson, C.; Bennett, D.; Bernabé, E.; Blencowe, H.; Bourne, R.; et al. UK health performance: Findings of the Global Burden of Disease Study 2010. Lancet 2013, 381, 997–1020. [Google Scholar] [CrossRef]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Chertow, G.M.; Coxson, P.G.; Moran, A.; Lightwood, J.M.; Pletcher, M.J.; Goldman, L. Projected effect of dietary salt reductions on future cardiovascular disease. N. Engl. J. Med. 2010, 362, 590–599. [Google Scholar] [CrossRef]
- World Health Organization. From burden to “best buys”: Reducing the economic impact of NCDs in low- and middle-income countries. World Economic Forum: Geneva, Switzerland, 2011. [Google Scholar]
- Asaria, P.; Chisholm, D.; Mathers, C.; Ezzati, M.; Beaglehole, R. Chronic disease prevention: Health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet 2007, 370, 2044–2053. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Sodium Intake for Adults and Children. Available online: http://www.who.int/nutrition/publications/guidelines/sodium_intake_printversion.pdf (accessed on 30 June 2014).
- World Health Organization. Follow-up to the Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases. Available online: http://apps.who.int/gb/ebwha/pdf_files/WHA66/A66_R10-en.pdf (accessed on 12 August 2014).
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef]
- Webster, J.L.; Dunford, E.K.; Hawkes, C.; Neal, B.C. Salt reduction initiatives around the world. J. Hypertens. 2011, 29, 1043–1050. [Google Scholar] [CrossRef]
- He, F.J.; Brinsden, H.C.; MacGregor, G.A. Salt reduction in the United Kingdom: A successful experiment in public health. J. Hum. Hypertens. 2014, 28, 345–352. [Google Scholar] [CrossRef]
- Hofman, K.J.; Tollman, S.M. Population health in South Africa: A view from the salt mines. Lancet Glob. Health 2013, 1, 66–67. [Google Scholar] [CrossRef]
- He, F.J.; Pombo-Rodrigues, S.; Macgregor, G.A. Salt reduction in England from 2003 to 2011: Its relationship to blood pressure, stroke and ischaemic heart disease mortality. BMJ Open 2014, 4, e004549. [Google Scholar] [CrossRef]
- Charlton, K.E.; Steyn, K.; Levitt, N.S.; Zulu, J.V.; Jonathan, D.; Veldman, F.J.; Nel, J.H. Ethnic differences in intake and excretion of sodium, potassium, calcium and magnesium in South Africans. Eur. J. Cardiovasc. Prev. Rehabil. 2005, 12, 355–362. [Google Scholar] [CrossRef]
- Webster, J.; Trieu, K.; Dunford, E.; Hawkes, C. Target Salt 2025: A Global Overview of National Programs to Encourage the Food Industry to Reduce Salt in Foods. Nutrients 2014, 6, 3274–3287. [Google Scholar] [CrossRef]
- Campbell, N.; Legowski, B.; Legetic, B.; Ferrante, D.; Nilson, E.; Campbell, C.; L’Abbé, M. Targets and Timelines for Reducing Salt in Processed Food in the Americas. J. Clin. Hypertens. 2014, in press. [Google Scholar] [CrossRef]
- Government, S.A. Government Gazette: No.R.214, under section 15(1) of the Foodstuffs, Cosmetics and Disinfectants Act 1972 (Act 54 of 1972). 2013. Available online: http://www.heartfoundation.co.za/sites/default/files/articles/South%20Africa%20salt%20legislation.pdf (accessed on 1 July 2014).
- Department of Health and Social Security. Committee on Medical Aspects of Food Policy Report on Health and Social Subjects; HM Stationery Office: London, UK, 1974. [Google Scholar]
- MacGregor, G.A.; De Wardener, H.E. Salt, Diet and Health: Neptune’s Poisoned Chalice: The Origins of High Blood Pressure; Cambridge University Press: Cambridge, UK, 1998. [Google Scholar]
- Health Education Council. National Advisory Committee on Nutrition Education Discussion Paper on Proposals for Nutritional Guidelines for Health Education in Britain; HM Stationery Office: London, UK, 1983. [Google Scholar]
- MacGregor, G.A.; Sever, P.S. Salt—Overwhelming evidence but still no action: Can a consensus be reached with the food industry? CASH (Consensus Action on Salt and Hypertension). BMJ 1996, 312, 1287–1289. [Google Scholar] [CrossRef]
- Vines, G. Taking Dissent with a Pinch of Salt; NewScientist: London, UK, 1986; Volume 9, p. 16. [Google Scholar]
- Department of Health. Committee on Medical Aspects of Food Policy Report on Nutritional Aspects of Cardiovascular Disease; HM Stationery Office: London, UK, 1994. [Google Scholar]
- Great Britain Department of Health. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom: Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy; HMSO: London, UK, 1991. [Google Scholar]
- Great Britain Department of Health. The Health of the Nation: A strategy for Health in England; HMSO: London, UK, 1996. [Google Scholar]
- Godlee, F. The food industry fights for salt. BMJ 1996, 312, 1239–1240. [Google Scholar] [CrossRef]
- Great Britain Department of Health. A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition; Department of Health: London, UK, 1996. [Google Scholar]
- Feng, J.; MacGregor, G. Effect of modest salt reduction on blood pressure. A meta-analysis of randomised trials: Implications for Public Health. J. Hum. Hypertens. 2002, 16, 761–770. [Google Scholar] [CrossRef]
- Nakagawa, H.; Morikawa, Y.; Okayama, A.; Fujita, Y.; Yoshida, Y.; Mikawa, K.; Sakata, K.; Ishizaki, M.; Miura, K.; Naruse, Y.; et al. Trends in blood pressure and urinary sodium and potassium excretion in Japan: Reinvestigation in the 8th year after the Intersalt Study. J. Hum. Hypertens. 1999, 13, 735–741. [Google Scholar]
- Graudal, N.A.; Galloe, A.M.; Garred, P. Effects of sodium restriction on blood pressure, renin, aldosterone, catecholamines, cholesterols and triglyceride: A meta-analysis. JAMA 1998, 279, 1383–1391. [Google Scholar] [CrossRef]
- Scientific Advisory Committee on Nutrition. Salt and Health. Available online: www.sacn.gov.uk/pdfs/sacn_salt_final.pdf (accessed on 25 June 2014).
- Food Standards Agency. Industry Support for Salt Campaign. Available online: http://www.food.gov.uk/healthiereating/salt/support/industry (accessed on 1 August 2010).
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef]
- Food Standards Agency. Salt Timeline of Key Events. Available online: http://www.food.gov.uk/healthiereating/salt/salttimeline (accessed on 16 August 2010).
- Food Standards Agency. Industry Activity. Available online: http://www.food.gov.uk/healthiereating/salt/industry (accessed on 4 August 2010).
- Food Standards Agency. Working with the Catering Business for Healthier Choices. Available online: http://www.food.gov.uk/healthiereating/healthycatering/cateringbusiness/ (accessed on 25 June 2014).
- Association of Cereal Food Manufacturers. Breakfast Salt Slashed Again. Available online: http://www.breakfastcereal.org/News/Breakfast-Salt-Slashed-Again.html (accessed on 14 July 2014).
- UK Food and Drink Federation. Salt: Industry’s Efforts Make a Difference. Available online: https://www.fdf.org.uk/resources/salt-thefactsfinal1.pdf (accessed on 16 August 2010).
- Food Standards Agency. Processed Food Databank: Sampling Round Two: February 2007–September 2007. Available online: http://www.food.gov.uk/science/surveillance/fsisbranch2008/fsis0108 (accessed on 12 August 2014).
- UK Department of Health. Responsibility Deal Food Network—New Salt Targets: F9 Salt Reduction 2017 pledge & F10 out of Home Salt Reduction Pledge. Available online: https://responsibilitydeal.dh.gov.uk/responsibility-deal-food-network-new-salt-targets-f9-salt-reduction-2017-pledge-f10-out-of-home-salt-reduction-pledge/ (accessed on 20 June 2014).
- Shankar, B.; Brambila-Macias, J.; Traill, B.; Mazzocchi, M.; Capacci, S. An evaluation of the UK Food Standards Agency’s salt campaign. Health Econ. 2013, 22, 243–250. [Google Scholar] [CrossRef]
- Wyness, L.A.; Butriss, J.L.; Stanner, S.A. Reducing the population’s sodium intake: The UK Food Standards Agency’s salt reduction programme. Public Health Nutr. 2012, 15, 254–261. [Google Scholar] [CrossRef]
- Smith-Spangler, C.M.; Juusola, J.L.; Enns, E.A.; Owens, D.K.; Garber, A.M. Population Strategies to Decrease Sodium Intake and the Burden of Cardiovascular Disease. Ann. Intern. Med. 2010, 152, 481–487. [Google Scholar] [CrossRef]
- Department of Health. Assessment of Dietary Sodium Levels among Adults (aged 19–64) in England, 2011. Available online: http://transparency.dh.gov.uk/2012/06/21/sodium-levels-among-adults (accessed on 25 June 2012).
- Charlton, K.E.; Steyn, K.; Levitt, N.S. Dietary Intervention Lowers Blood Pressure in South Africas with Hypertension. Available online: http://www.mrc.ac.za/policybriefs/saltpolicy.pdf (accessed on 30 June 2014).
- Charlton, K.E.; Steyn, K.; Levitt, N.S.; Peer, N.; Jonathan, D.; Gogela, T.; Rossouw, K.; Gwebushe, N.; Lombard, C.J. A food-based dietary strategy lowers blood pressure in a low socio-economic setting: A randomised study in South Africa. Public Health Nutr. 2008, 11, 1397–1406. [Google Scholar] [CrossRef]
- Bertram, M.Y.; Steyn, K.; Wentzel-Viljoen, E.; Tollman, S.; Hofman, K.J. Reducing the sodium content of high-salt foods: Effect on cardiovascular disease in South Africa. S. Afr. Med. J. 2012, 102, 743–745. [Google Scholar]
- South Africa Government. Government Gazette No.35509, Government Notice No. R 533, 11 July 2012. Available online: http://www.pmg.org.za/files/doc/2012/foodstuffregs.pdf (accessed on 1 July 2014).
- Popkin, B.M. The nutrition transition and obesity in the developing world. J. Nutr. 2001, 131, 871–873. [Google Scholar]
- Badenhorst, C.; Steyn, N.; Jooste, P.; Nel, J.; Kruger, M.; POelofse, A.; Barnard, C. Nutritional status of Pedi schoolchildren aged 6–14 years in two rural areas of Lebowa: a comprehensive nutritional survey of dietary intake, anthropometric, biochemical, haematological and clinical measurements. S. Afr. J. Food Sci. Nutr. 1993, 5, 112–119. [Google Scholar]
- Bourne, L.T.; Langenhoven, M.L.; Steyn, K.; Jooste, P.L.; Laubscher, J.A.; Van der Vyver, E. Nutrient intake in the urban African population of the Cape Peninsula, South Africa. The Brisk study. Cent. Afr. J. Med. 1993, 39, 238–247. [Google Scholar]
- Steyn, N.; Burger, S.; Monyeki, K.; Alberts, M.; Nthangeni, G. Dietary Intake of the Adult Population of Dikgale; University of the North: Sovenga, 1998. [Google Scholar]
- Steyn, N.; Burger, S.; Monyeki, K.; Alberts, M.; Nthangeni, G. Seasonal variation in dietary intake of the adult population of Dikgale. S. Afr. J. Clin. Nutr. 2001, 14, 140–145. [Google Scholar]
- Wolmarans, P.; Langenhoven, M.L.; van Eck, M.; Swanepoel, A.S. The contribution of different food groups to the energy, fat and fibre intake of the Coronary Risk Factor Study (CORIS) population. S. Afr. Med. J. 1989, 75, 167–171. [Google Scholar]
- Charlton, K.E.; Steyn, K.; Levitt, N.S.; Zulu, J.V.; Jonathan, D.; Veldman, F.J.; Nel, J.H. Diet and blood pressure in South Africa: Intake of foods containing sodium, potassium, calcium, and magnesium in three ethnic groups. Nutrition 2005, 21, 39–50. [Google Scholar] [CrossRef]
- Charlton, K.E.; MacGregor, E.; Vorster, N.H.; Levitt, N.S.; Steyn, K. Partial replacement of NaCl can be achieved with potassium, magnesium and calcium salts in brown bread. Int. J. Food Sci. Nutr. 2007, 58, 508–521. [Google Scholar] [CrossRef]
- Charlton, K. The Development of a Dietary Intervention to Modify Cation Content of Foods and the Evaluation of Its Effects on Blood Pressure in Hypertensive Black South Africans. Ph.D. Thesis, University of Cape Town, Cape Town, South Africa, 2006. [Google Scholar]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Svetkey, L.P.; Simons-Morton, D.; Vollmer, W.M.; Appel, L.J.; Conlin, P.R.; Ryan, D.H.; Ard, J.; Kennedy, B.M. Effects of dietary patterns on blood pressure: Subgroup analysis of the Dietary Approaches to Stop Hypertension (DASH) randomized clinical trial. Arch. Intern. Med. 1999, 159, 285–293. [Google Scholar] [CrossRef]
- Food & Beverage Reporter. Recipe reformulations and capital investments required. Available online: http://www.fbreporter.com/54--sp-961/-sp-283/26300-recipe-reformulations-and-capital-investments-required (accessed on 12 August 2014).
- The Heart and Stroke Foundation South Africa. Salt Is Killing South Africans and It Is Time to Take Action. Available online: http://www.heartfoundation.co.za/media-releases/salt-killing-south-africans-and-it-time-take-action (accessed on 1 July 2014).
- Heart and Stroke Fondation of South Africa. Salt Watch. Available online: http://www.heartfoundation.co.za/salt-watch (accessed on 2 September 2014).
- Phaswana-Mafuya, N.; Peltzer, K.; Schneider, M.; Makiwane, M.; Zuma, K.; Ramlagan, S.; Tabane, C.; Davids, A.; Mbelle, N.; Matseke, G.; et al. Study on Global Ageing and Adult Health (SAGE), South Africa 2007–2008; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- WHO/PAHO Regional Expert Group for Cardiovascular Disease. Prevention through Population—Wide Dietary Salt Reduction. Protocol for Population Level Sodium Determination in 24-Hour Urine Samples. Available online: http://new.paho.org/hq/dmdocuments/2010/pahosaltprotocol.pdf (accessed on 30 June 2014).
- Food Standards Agency. 2017 UK Salt Reduction Targets. Available online: http://multimedia. food.gov.uk/multimedia/spreadsheets/salttargets2017.xls (accessed on 4 July 2014).
- Bloom, D.E.; Cafiero, E.T.; Jane-Llopis, E.; Abrahams-Gessel, S.; Bloom, L.R.; Fathima, S.; Feigl, A.B.; Gaziano, T.; Mowafi, M.; Pandya, A.; et al. The Global Economic Burden on Noncommunicable Diseases; World Economic Forum: Geneva, Switzerland, 2011. [Google Scholar]
- Cutler, J.; Follmann, D.; Allender, P. Randomized trials of sodium reduction: An overview. Am. J. Clin. Nutr. 1997, 65, 643–651. [Google Scholar]
- Hooper, L.; Bartlett, C.; Smith, G.D.; Ebrahim, S. Systematic review of long term effects of advice to reduce dietary salt in adults. BMJ 2002, 325, 628–634. [Google Scholar] [CrossRef]
- Midgley, J.; Matthew, A.; Greenwood, C.; Logan, A. Effect of reduced dietary sodium on blood pressure. JAMA 1996, 275, 1590–1597. [Google Scholar] [CrossRef]
- He, F.; MacGregor, G. Effect of longer-term modest salt reduction on blood pressure. Cochrane Database Syst. Rev. 2004, 3. [Google Scholar] [CrossRef]
- Hooper, L.; Bartlett, C.; Smith, G.D.; Ebrahim, S. Advice to reduce dietary salt for prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2004, 1. [Google Scholar] [CrossRef]
- World Health Organization. Report of the Formal Meeting of Member States to Conclude the Work on the Comprehensive Global Monitoring Framework, Including Indicators, and a Set of Voluntary Global Targets for the Prevention and Control of Noncommunicable Diseases. Available online: http://apps.who.int/gb/NCDs/pdf/A_NCD_2-en.pdf (accessed on 30 June 2014).
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Nguyen, Q.N.; Pham, S.T.; Do, L.D.; Nguyen, V.L.; Wall, S.; Weinehall, L.; Bonita, R.; Byass, P. Cardiovascular disease risk factor patterns and their implications for intervention strategies in Vietnam. Int. J. Hyptens. 2012. [Google Scholar] [CrossRef]
- World Health Organization. WHO CVD-Risk Management Package for Low- and Medium-Resource Settings; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Rose, G.; Khaw, K.-T.; Marmot, M. Rose’s Strategy of Preventive Medicine; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Mendis, S. Challenges for the management of hypertension in low-resource settings. Ethn. Dis. 2003, 13, 67–70. [Google Scholar]
- Wentzel-Viljoen, E.; Steyn, K.; Ketterer, E.; Charlton, K.E. "Use salt and foods high in salt sparingly”: A food-based dietary guideline for South Africa. S. Afr. J. Clin. Nutr. 2013, 26, 105–113. [Google Scholar]
- Elliott, T.; Trevena, H.; Sacks, G.; Dunford, E.; Martin, J.; Webster, J.; Swinburn, B.; Moodie, A.R.; Neal, B.C. A systematic interim assessment of the Australian Government’s Food and Health Dialogue. Med. J. Aust. 2014, 200, 92–95. [Google Scholar] [CrossRef]
- Mayosi, B.M.; Flisher, A.J.; Lalloo, U.G.; Sitas, F.; Tollman, S.M.; Bradshaw, D. The burden of non-communicable diseases in South Africa. Lancet 2009, 374, 934–947. [Google Scholar] [CrossRef]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Vander Hoorn, S.; Murray, C.J. Selected major risk factors and global and regional burden of disease. Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef]
- Jooste, P.L.; Weight, M.J.; Lombard, C.J. Iodine Concentration in Household Salt in South Africa. Available online: http://www.who.int/bulletin/archives/79(6)534.pdf (accessed on 14 July 2014).
- Charlton, K.E.; Jooste, P.L.; Steyn, K.; Levitt, N.S.; Ghosh, A. A lowered salt intake does not compromise iodine status in Cape Town, South Africa, where salt iodization is mandatory. Nutrition 2013, 29, 630–634. [Google Scholar] [CrossRef]
- Vanderpump, M.P.; Lazarus, J.H.; Smyth, P.P.; Laurberg, P.; Holder, R.L.; Boelaert, K.; Franklyn, J.A. Iodine status of UK schoolgirls: A cross-sectional survey. Lancet 2011, 377, 2007–2012. [Google Scholar] [CrossRef]
- World Health Organization. Salt Reduction and Iodine Fortification Strategies in Public Health: Report of a Joint Technical Meeting. Available online: http://apps.who.int/iris/bitstream/10665/101509/1/9789241506694_eng.pdf?ua=1 (accessed on 30 June 2014).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Charlton, K.; Webster, J.; Kowal, P. To Legislate or Not to Legislate? A Comparison of the UK and South African Approaches to the Development and Implementation of Salt Reduction Programs. Nutrients 2014, 6, 3672-3695. https://doi.org/10.3390/nu6093672
Charlton K, Webster J, Kowal P. To Legislate or Not to Legislate? A Comparison of the UK and South African Approaches to the Development and Implementation of Salt Reduction Programs. Nutrients. 2014; 6(9):3672-3695. https://doi.org/10.3390/nu6093672
Chicago/Turabian StyleCharlton, Karen, Jacqui Webster, and Paul Kowal. 2014. "To Legislate or Not to Legislate? A Comparison of the UK and South African Approaches to the Development and Implementation of Salt Reduction Programs" Nutrients 6, no. 9: 3672-3695. https://doi.org/10.3390/nu6093672