Analysis of Dietary Pattern Impact on Weight Status for Personalised Nutrition through On-Line Advice: The Food4Me Spanish Cohort

 ,
,  ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Experimental Section
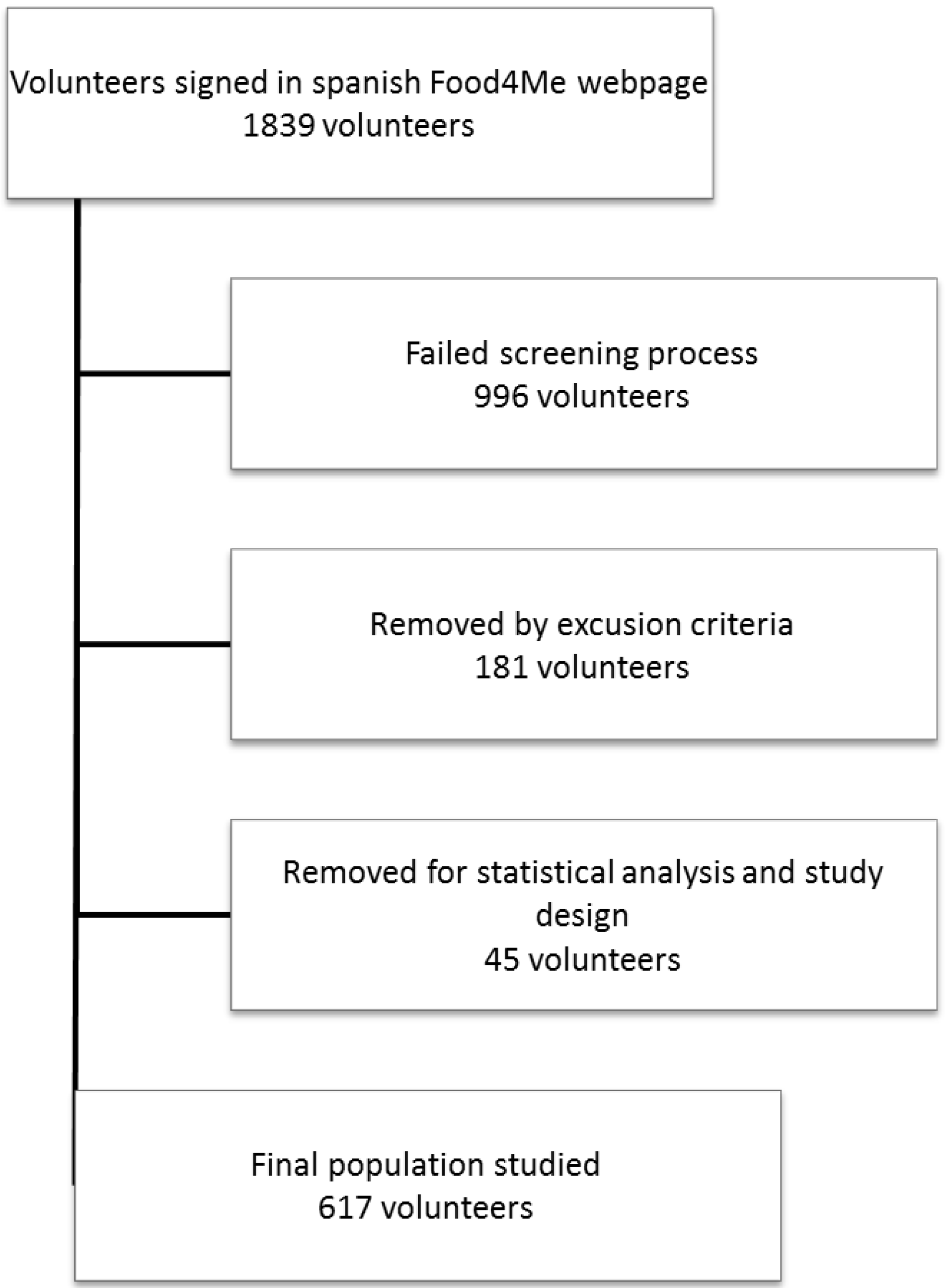
2.1. Study Population

2.2. Dietary Assessment
2.3. Anthropometric Measurements
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Categorized by Gender | Categorized by Age | |||||||||||
| Female | Male | p 1 | ≤37 years | ≤37 years | p 1 | |||||||
| n | 617 | 368 | 249 | - | 315 | 304 | - | |||||
| Age (years) | 38.3 ± 9.6 | 37.9 ± 9.5 | 38.9 ± 9.8 | 30.7 ± 4.5 | 46.1 ± 7.0 | - | ||||||
| BMI (kg/m2) | 25.8 ± 4.5 | 24.9 ± 4.7 | 27.1 ± 3.7 | *** | 24.7 ± 4.2 | 26.9 ± 4.4 | *** | |||||
| BMI status (% of n) | ||||||||||||
| Normal weight | 48.8% | 59.8% | 32.5% | *** 3 | 61.2% | 36.0% | *** 3 | |||||
| Overweight | 35.0% | 25.5% | 49.0% | 29.0% | 41.3% | |||||||
| Obese | 16.2% | 14.7% | 18.5% | 9.9% | 22.8% | |||||||
| Physical activity factor | 1.50 ± 4.47 | 1.48 ± 0.08 | 1.52 ± 0.11 | *** | 1.51 ± 0.10 | 1.48 ± 0.09 | ** | |||||
| Energy (kcal) | 2651 ± 796 | 2472 ± 759 | 2916 ± 777 | *** | 2632 ± 798 | 2670 ± 795 | ||||||
| EIR:BMR ratio 2 | 1.74 ± 0.50 | 1.82 ± 0.53 | 1.61 ± 0.42 | *** | 1.74 ± 0.50 | 1.73 ± 0.49 | ||||||
| Fat (% of energy) | 35.7 ± 6.4 | 36.3 ± 6.2 | 34.8 ± 6.6 | ** | 35.7 ± 6.0 | 35.7 ± 6.7 | ||||||
| Saturated fat (% of energy) | 13.1 ± 2.8 | 13.3 ± 2.7 | 12.8 ± 2.9 | * | 13.2 ± 2.8 | 13.0 ± 2.8 | ||||||
| Monounsaturated fat (% of energy) | 14.8 ± 3.7 | 15.2 ± 3.8 | 14.3 ± 3.4 | ** | 14.8 ± 3.5 | 14.9 ± 3.9 | ||||||
| Polyunsaturated fat (% of energy) | 5.3 ± 1.3 | 5.4 ± 1.4 | 5.2 ± 1.3 | 5.3 ± 1.3 | 5.3 ± 1.4 | |||||||
| Omega 3 acids (% of energy) | 0.82 ± 0.24 | 0.84 ± 0.25 | 0.78 ± 0.23 | ** | 0.81 ± 0.24 | 0.82 ± 0.24 | ||||||
| Protein (% of energy) | 19.2 ± 4.0 | 19.4 ± 4.1 | 19.0 ± 3.7 | 19.5 ± 4.0 | 19.0 ± 3.9 | |||||||
| Carbohydrate (% of energy) | 44.7 ± 8.5 | 44.7 ± 8.4 | 44.7 ± 8.7 | 44.4 ± 7.8 | 45.0 ± 9.2 | |||||||
| Sugar (% of energy) | 21.2 ± 6.8 | 21.9 ± 7.1 | 20.1 ± 6.3 | ** | 21.2 ± 6.3 | 21.1 ± 7.4 | ||||||
| Alcohol (% of energy) | 3.0 ± 3.8 | 2.1 ± 2.6 | 4.2 ± 4.8 | *** | 2.8 ± 3.7 | 3.1 ± 3.9 | ||||||
| Salt (g) | 7.7 ± 3.0 | 7.1 ± 2.8 | 8.6 ± 3.2 | *** | 7.6 ± 3.0 | 7.8 ± 3.0 | ||||||
| Dietary fibre (g/1000 kcal) | 10.6 ± 3.7 | 11.0 ± 3.8 | 10.0 ± 3.3 | *** | 10.4 ± 3.6 | 10.8 ± 3.7 | ||||||
| Disease prevalence (% of n) 4 | 54.5% | 57.1% | 50.6% | 3 | 49.0% | 60.1% | ** 3 | |||||
| Prescribed medication (% of n) | 29.0% | 31.8% | 24.9% | 3 | 23.6% | 34.7% | ** 3 | |||||
| Supplement user (% of n) | 21.2% | 25.3% | 15.3% | ** 3 | 21.0% | 21.5% | 3 | |||||
| Smoke (% of n) | 16.9% | 16.6% | 17.3% | 3 | 20.4% | 13.2% | * 3 | |||||
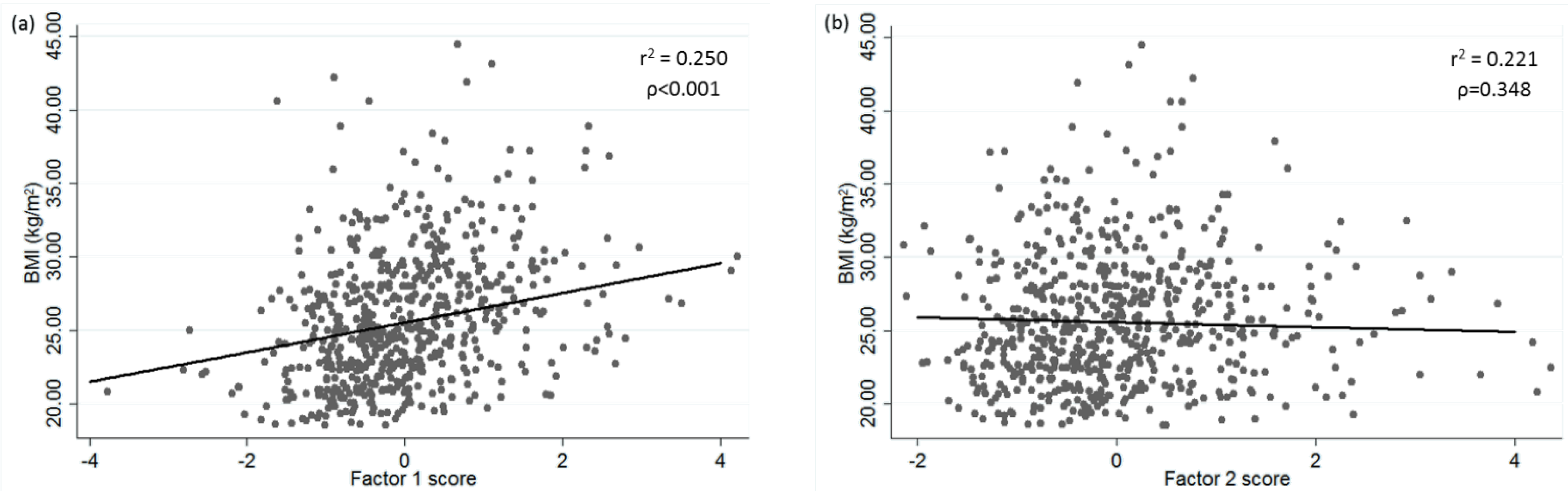
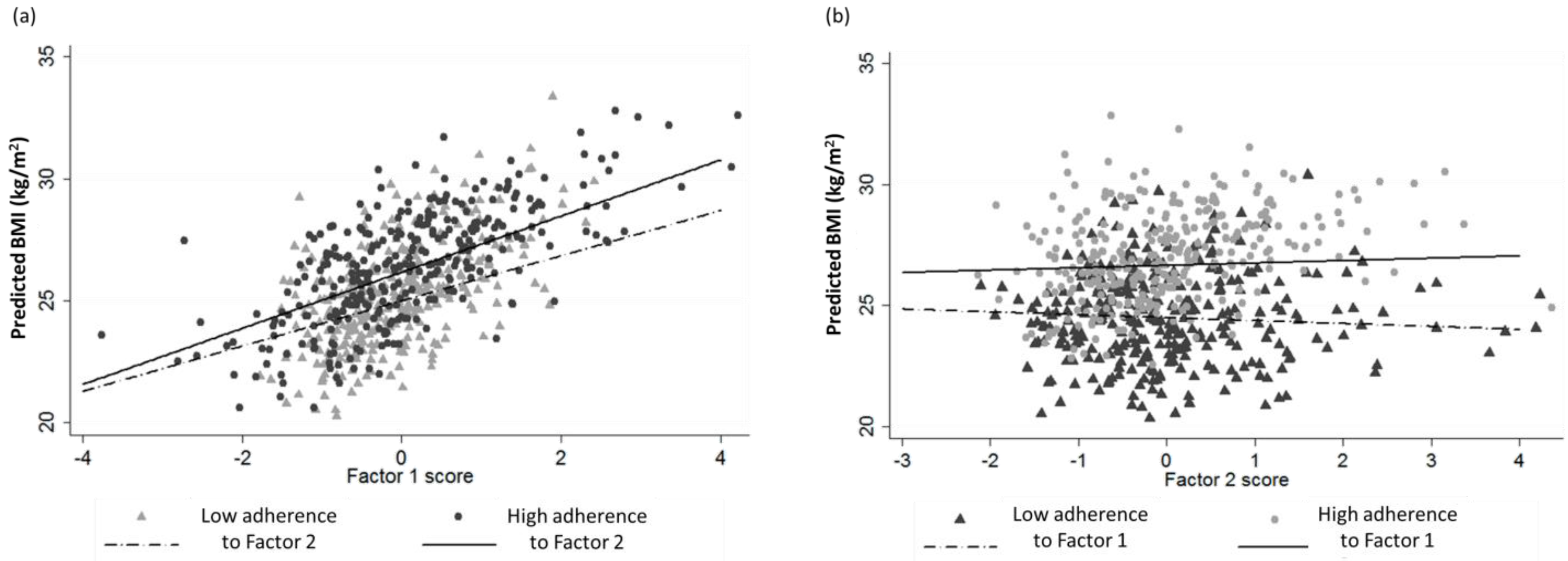
3.2. Factor Scores: Association and Effects with BMI
| Variable | Factor 1 | Factor 2 |
|---|---|---|
| Alcoholic beverages | ||
| Eggs | 0.3606 | |
| Fast and processed food | 0.6578 | |
| Fat and spreads | ||
| Fish products | 0.4804 | |
| Fruits | −0.3904 | |
| Full fat dairy products | ||
| High fat dairy products | ||
| Legumes | 0.458 | |
| Low calorie beverages | 0.3206 | |
| Nuts | 0.3022 | |
| Oils | 0.3305 | |
| Oily fruits | 0.5014 | |
| Potatoes | 0.3221 | |
| Red meat | 0.6336 | |
| Reduced fat dairy products | ||
| Refined grains | 0.4483 | |
| Snacks | 0.6094 | |
| Soup and sauces | ||
| Sweets | ||
| Sweets beverages | ||
| Vegetables | −0.3582 | 0.6345 |
| White meat | 0.4622 | 0.3023 |
| Whole grains |


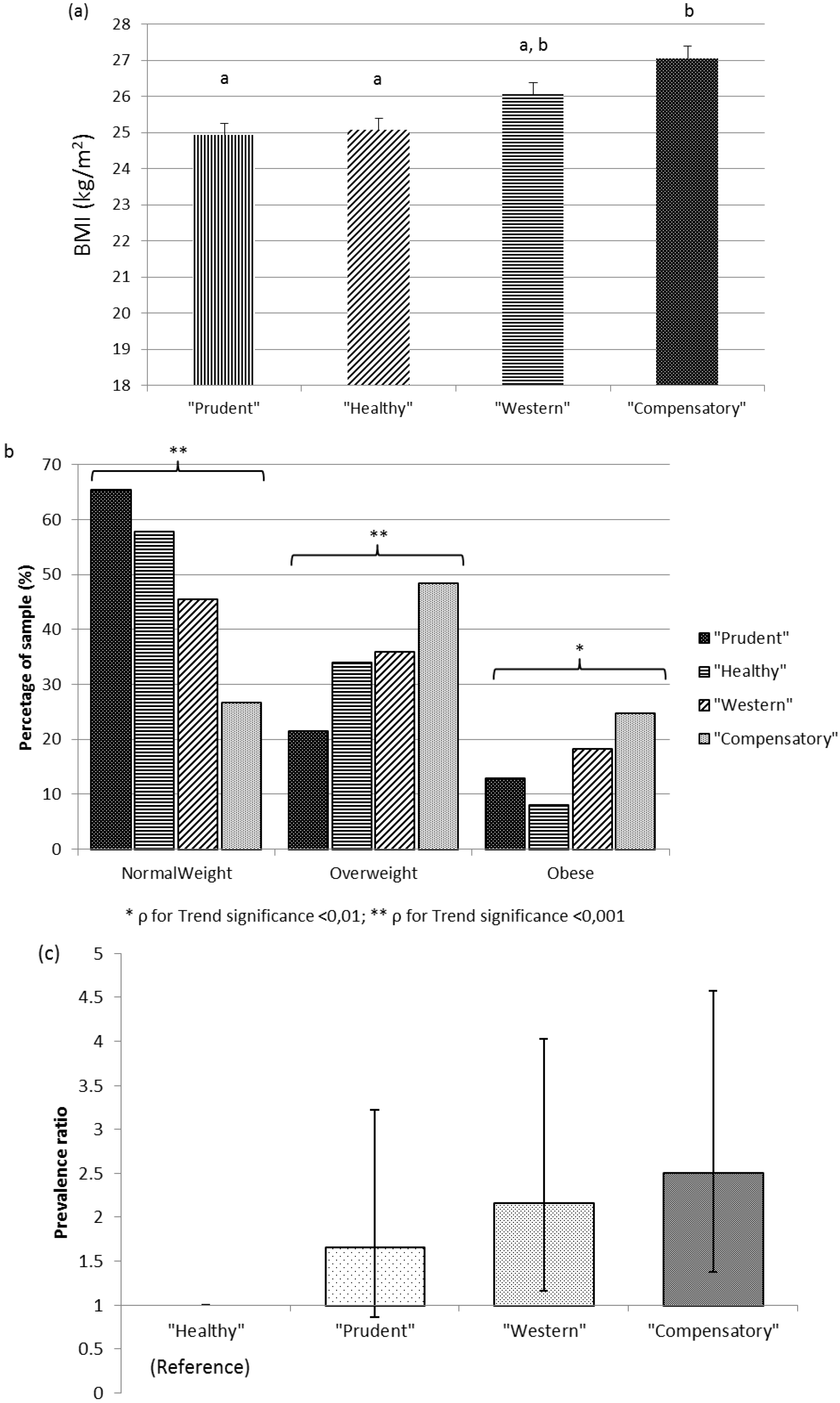
3.3. Dietary Patterns: Obesity Prevalence

3.4. Habits and Attitude towards Feeding
4. Discussion
4.1. Personalised Nutrition (PN) Seekers Status
4.2. Adherence to Dietary Patterns and Obesity
4.3. Tailoring the Advice Based on Prediction of Dietary Behaviours
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Margetts, B. Feedback on WHO/FAO global report on diet, nutrition and prevention of chronic diseases(NCD). Public Health Nutr. 2003, 6, 423–424. [Google Scholar] [CrossRef] [PubMed]
- Nishida, C.; Uauy, R.; Kumanyika, S.; Shetty, P. The joint WHO/FAO expert consultation on diet, nutrition and the prevention of chronic diseases: Process, product and policy implications. Public Health Nutr. 2004, 7, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Tonstad, S.; Malik, N.; Haddad, E. A high-fibre bean-rich diet versus a low-carbohydrate diet for obesity. J. Hum. Nutr. Diet. 2014, 27, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Barkoukis, H. Importance of understanding food consumption patterns. J. Am. Diet. Assoc. 2007, 107, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Jebb, S.A. Carbohydrates and obesity: From evidence to policy in the UK. Proc. Nutr. Soc. 2015, 74, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2013, 346, e7492. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, D.; Al-Badri, M.R.; Azar, S.T. Effect of mediterranean diet in diabetes control and cardiovascular risk modification: A systematic review. Front. Public Health 2015, 3, 69. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Xu, F.; Wang, Z.; Liang, Y.; Li, J. Dietary patterns and the incidence of hyperglyacemia in China. Public Health Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the healthy eating index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Kourisblazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef] [PubMed]
- Wirfalt, A.K.; Jeffery, R.W. Using cluster analysis to examine dietary patterns: Nutrient intakes, gender, and weight status differ across food pattern clusters. J. Am. Diet. Assoc. 1997, 97, 272–279. [Google Scholar] [CrossRef]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.K.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary patterns: Challenges and opportunities in dietary patterns research an Experimental Biology workshop, April 1, 2006. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.; Livingstone, K.M.; Marsaux, C.F.; Forster, H.; O’Donovan, C.B.; Woolhead, C.; Macready, A.L.; Fallaize, R.; Navas-Carretero, S.; San-Cristobal, R.; et al. Design and baseline characteristics of the Food4Me study: A web-based randomised controlled trial of personalised nutrition in seven European countries. Genes Nutr. 2015, 10, 450. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E. Critical evaluation of energy intake using the goldberg cut-off for energy intake: Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Forster, H.; Fallaize, R.; Gallagher, C.; O’Donovan, C.B.; Woolhead, C.; Walsh, M.C.; Macready, A.L.; Lovegrove, J.A.; Mathers, J.C.; Gibney, M.J.; et al. Online dietary intake estimation: The Food4Me food frequency questionnaire. J. Med. Int. Res. 2014, 16, e150. [Google Scholar] [CrossRef] [PubMed]
- Fallaize, R.; Forster, H.; Macready, A.L.; Walsh, M.C.; Mathers, J.C.; Brennan, L.; Gibney, E.R.; Gibney, M.J.; Lovegrove, J.A. Online dietary intake estimation: Reproducibility and validity of the Food4Me food frequency questionnaire against a 4-day weighed food record. J. Med. Internet Res. 2014, 16, e190. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.; Livingstone, K.; Woolhead, C.; Forster, H.; O’Donovan, C.; Macready, A.; Fallaize, R.; Marsaux, C.M.; Tsirigoti, L.; Efstathopoulou, E.; et al. How reliable is internet-based self-reported identity, socio-demographic and obesity measures in european adults? Genes Nutr. 2015, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Svensson, M.; Hult, M.; van der Mark, M.; Grotta, A.; Jonasson, J.; von Hausswolff-Juhlin, Y.; Rossner, S.; Lagerros, Y.T. The change in eating behaviors in a web-based weight loss program: A longitudinal analysis of study completers. J. Med. Internet Res. 2014, 16, e234. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Morgan, P.J.; Hutchesson, M.J.; Callister, R. Efficacy of standard versus enhanced features in a Web-based commercial weight-loss program for obese adults, part 2: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e140. [Google Scholar] [CrossRef] [PubMed]
- Brindal, E.; Freyne, J.; Saunders, I.; Berkovsky, S.; Smith, G.; Noakes, M. Features predicting weight loss in overweight or obese participants in a web-based intervention: Randomized trial. J. Med. Internet Res. 2012, 14, e173. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.M.; Hutchesson, M.J.; Jensen, M.; Morgan, P.; Callister, R.; Collins, C.E. Participants in an online weight loss program can improve diet quality during weight loss: A randomized controlled trial. Nutr. J. 2014, 13, 82. [Google Scholar] [CrossRef] [PubMed]
- Postrach, E.; Aspalter, R.; Elbelt, U.; Koller, M.; Longin, R.; Schulzke, J.D.; Valentini, L. Determinants of successful weight loss after using a commercial web-based weight reduction program for six months: Cohort study. J. Med. Internet Res. 2013, 15, e219. [Google Scholar] [CrossRef] [PubMed]
- Kaipainen, K.; Payne, C.R.; Wansink, B. Mindless eating challenge: Retention, weight outcomes, and barriers for changes in a public web-based healthy eating and weight loss program. J. Med. Internet Res. 2012, 14, e168. [Google Scholar] [CrossRef] [PubMed]
- Springvloet, L.; Lechner, L.; de Vries, H.; Oenema, A. Long-term efficacy of a Web-based computer-tailored nutrition education intervention for adults including cognitive and environmental feedback: A randomized controlled trial. BMC Public Health 2015, 15, 372. [Google Scholar] [CrossRef] [PubMed]
- Ashwell, M.; Howarth, E.; Chesters, D.; Allan, P.; Hoyland, A.; Walton, J. A web-based weight loss programme including breakfast cereals results in greater loss of body mass than a standardised web-based programme in a randomised controlled trial. Obes. Facts 2014, 7, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Spittaels, H.; de Bourdeaudhuij, I.; Brug, J.; Vandelanotte, C. Effectiveness of an online computer-tailored physical activity intervention in a real-life setting. Health Educ. Res. 2007, 22, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Hutchesson, M.J.; Collins, C.E.; Morgan, P.J.; Watson, J.F.; Guest, M.; Callister, R. Changes to dietary intake during a 12-week commercial web-based weight loss program: A randomized controlled trial. Eur. J. Clin. Nutr. 2014, 68, 64–70. [Google Scholar] [CrossRef] [PubMed]
- De Sanidad, S.; Estadística, S.E. Encuesta Nacional de Salud 2011–2012. Available online: http://www.ine.es/prensa/np770.pdf (accessed on 10 November 2015).
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [PubMed]
- Northstone, K.; Ness, A.R.; Emmett, P.M.; Rogers, I.S. Adjusting for energy intake in dietary pattern investigations using principal components analysis. Eur. J. Clin. Nutr. 2008, 62, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Judd, S.E.; Letter, A.J.; Shikany, J.M.; Roth, D.L.; Newby, P.K. Dietary patterns derived using exploratory and confirmatory factor analysis are stable and generalizable across race, region, and gender subgroups in the regards study. Front. Nutr. 2014, 1, 29. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Emmett, P.M.; Newby, P.K.; Northstone, K. Dietary patterns obtained through principal components analysis: The effect of input variable quantification. Br. J. Nutr. 2013, 109, 1881–1891. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Devlin, U.M.; McNulty, B.A.; Nugent, A.P.; Gibney, M.J. The use of cluster analysis to derive dietary patterns: Methodological considerations, reproducibility, validity and the effect of energy mis-reporting. Proc. Nutr. Soc. 2012, 71, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Buys, N.J.; Hills, A.P. Dietary pattern and its association with the prevalence of obesity, hypertension and other cardiovascular risk factors among chinese older adults. Int. J. Environ. Res. Public Health 2014, 11, 3956–3971. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Muller, D.; Hallfrisch, J.; Qiao, N.; Andres, R.; Tucker, K.L. Dietary patterns and changes in body mass index and waist circumference in adults. Am. J. Clin. Nutr. 2003, 77, 1417–1425. [Google Scholar] [PubMed]
- Flores, M.; Macias, N.; Rivera, M.; Lozada, A.; Barquera, S.; Rivera-Dommarco, J.; Tucker, K.L. Dietary patterns in mexican adults are associated with risk of being overweight or obese. J. Nutr. 2010, 140, 1869–1873. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.S.; Black, K.E.; Wong, J.E.; Parnell, W.R.; Skidmore, P.M. Dieting status influences associations between dietary patterns and body composition in adolescents: A cross-sectional study. Nutr. J. 2013, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L. Childhood dietary patterns and later obesity: A review of the evidence. Proc. Nutr. Soc. 2014, 73, 137–146. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, Y.; Lai, J.; Wang, D.; Zhang, J.; Fu, P.; Yang, X.; Qi, L. Dietary patterns as compared with physical activity in relation to metabolic syndrome among chinese adults. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Song, Y.; Lee, K.H.; Lee, H.S.; Lee, M.; Jee, S.H.; Joung, H. A fruit and dairy dietary pattern is associated with a reduced risk of metabolic syndrome. Metabolism 2012, 61, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Garduno-Diaz, S.D.; Khokhar, S. South asian dietary patterns and their association with risk factors for the metabolic syndrome. J. Hum. Nutr. Diet. 2013, 26, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Spiegelman, D.; Willett, W.C. Prospective study of major dietary patterns and risk of coronary heart disease in men. Am. J. Clin. Nutr. 2000, 72, 912–921. [Google Scholar] [PubMed]
- Mente, A.; de Koning, L.; Shannon, H.S.; Anand, S.S. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch. Intern. Med. 2009, 169, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Varela-Moreiras, G.; Avila, J.M.; Cuadrado, C.; del Pozo, S.; Ruiz, E.; Moreiras, O. Evaluation of food consumption and dietary patterns in spain by the food consumption survey: Updated information. Eur. J. Clin. Nutr. 2010, 64, S37–S43. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.; Bach-Faig, A.; Raido Quintana, B.; Buckland, G.; vaz de Almeida, M.D.; Serra-Majem, L. Worldwide variation of adherence to the mediterranean diet, in 1961–1965 and 2000–2003. Public Health Nutr. 2009, 12, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Kyriacou, A.; Evans, J.M.; Economides, N. Adherence to the Mediterranean diet by the Greek and Cypriot population: A systematic review. Eur. J. Public Health 2015. [Google Scholar] [CrossRef]
- Dernini, S.; Berry, E.M. Mediterranean diet: From a healthy diet to a sustainable dietary pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- De Vet, E.; de Wit, J.B.; Luszczynska, A.; Stok, F.M.; Gaspar, T.; Pratt, M.; Wardle, J.; de Ridder, D.T. Access to excess: How do adolescents deal with unhealthy foods in their environment? Eur. J. Public Health 2013, 23, 752–756. [Google Scholar] [CrossRef] [PubMed]
- De Graaf, C. Effects of snacks on energy intake: An evolutionary perspective. Appetite 2006, 47, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Barnes, T.L.; French, S.A.; Harnack, L.J.; Mitchell, N.R.; Wolfson, J. Snacking behaviors, diet quality, and body mass index in a community sample of working adults. J. Acad. Nutr. Diet. 2015, 115, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Berteus Forslund, H.; Torgerson, J.S.; Sjostrom, L.; Lindroos, A.K. Snacking frequency in relation to energy intake and food choices in obese men and women compared to a reference population. Int. J. Obes. 2005, 29, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F. Meals and snacking, diet quality and energy balance. Physiol. Behav. 2014, 134, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Chapelot, D. The role of snacking in energy balance: A biobehavioral approach. J. Nutr. 2011, 141, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Soriguer, F.; Garcia-Escobar, E.; Morcillo, S.; Garcia-Fuentes, E.; de Fonseca, F.; Olveira, G.; Rojo-Martinez, G. Mediterranean diet and the spanish paradox. A hypothesis. Med. Hypotheses 2013, 80, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Chrysohoou, C.; Pitsavos, C.; Stefanadis, C. Association between the prevalence of obesity and adherence to the mediterranean diet: The ATTICA study. Nutrition 2006, 22, 449–456. [Google Scholar] [CrossRef] [PubMed]
- San-Cristobal, R.; Milagro, F.I.; Martinez, J.A. Future challenges and present ethical considerations in the use of personalized nutrition based on genetic advice. J. Acad. Nutr. Diet. 2013, 113, 1447–1454. [Google Scholar] [CrossRef] [PubMed]
- Stewart-Knox, B.; Kuznesof, S.; Robinson, J.; Rankin, A.; Orr, K.; Duffy, M.; Poinhos, R.; de Almeida, M.D.; Macready, A.; Gallagher, C.; et al. Factors influencing european consumer uptake of personalised nutrition. Results of a qualitative analysis. Appetite 2013, 66, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.A.; Navas-Carretero, S.; Saris, W.H.; Astrup, A. Personalized weight loss strategies-the role of macronutrient distribution. Nat. Rev. Endocrinol. 2014, 10, 749–760. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.A.; Milagro, F.I. Genetics of weight loss: A basis for personalized obesity management. Trends Food Sci. Technol. 2015, 42, 97–115. [Google Scholar] [CrossRef]
- Milagro, F.I.; Mansego, M.L.; de Miguel, C.; Martinez, J.A. Dietary factors, epigenetic modifications and obesity outcomes: Progresses and perspectives. Mol. Aspects Med. 2013, 34, 782–812. [Google Scholar] [CrossRef] [PubMed]
- Friedl, K.E.; Rowe, S.; Bellows, L.L.; Johnson, S.L.; Hetherington, M.M.; de Froidmont-Gortz, I.; Lammens, V.; Hubbard, V.S. Report of an EU-US symposium on understanding nutrition-related consumer behavior: Strategies to promote a lifetime of healthy food choices. J. Nutr. Educ. Behav. 2014, 46, 445–450. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
San-Cristobal, R.; Navas-Carretero, S.; Celis-Morales, C.; Brennan, L.; Walsh, M.; Lovegrove, J.A.; Daniel, H.; Saris, W.H.M.; Traczyk, I.; Manios, Y.; et al. Analysis of Dietary Pattern Impact on Weight Status for Personalised Nutrition through On-Line Advice: The Food4Me Spanish Cohort. Nutrients 2015, 7, 9523-9537. https://doi.org/10.3390/nu7115482
San-Cristobal R, Navas-Carretero S, Celis-Morales C, Brennan L, Walsh M, Lovegrove JA, Daniel H, Saris WHM, Traczyk I, Manios Y, et al. Analysis of Dietary Pattern Impact on Weight Status for Personalised Nutrition through On-Line Advice: The Food4Me Spanish Cohort. Nutrients. 2015; 7(11):9523-9537. https://doi.org/10.3390/nu7115482
Chicago/Turabian StyleSan-Cristobal, Rodrigo, Santiago Navas-Carretero, Carlos Celis-Morales, Lorraine Brennan, Marianne Walsh, Julie A. Lovegrove, Hannelore Daniel, Wim H. M. Saris, Iwonna Traczyk, Yannis Manios, and et al. 2015. "Analysis of Dietary Pattern Impact on Weight Status for Personalised Nutrition through On-Line Advice: The Food4Me Spanish Cohort" Nutrients 7, no. 11: 9523-9537. https://doi.org/10.3390/nu7115482